A Transdisciplinary Analysis of COVID-19 in Italy: The Most Affected Country in Europe


Abstract
:1. Introduction
2. Case Presentation
2.1. Geographic, Climatic, Demographic, Economic and Political Characteristics of the Country
2.2. The Italian Health Care System: Characteristics and Ranking
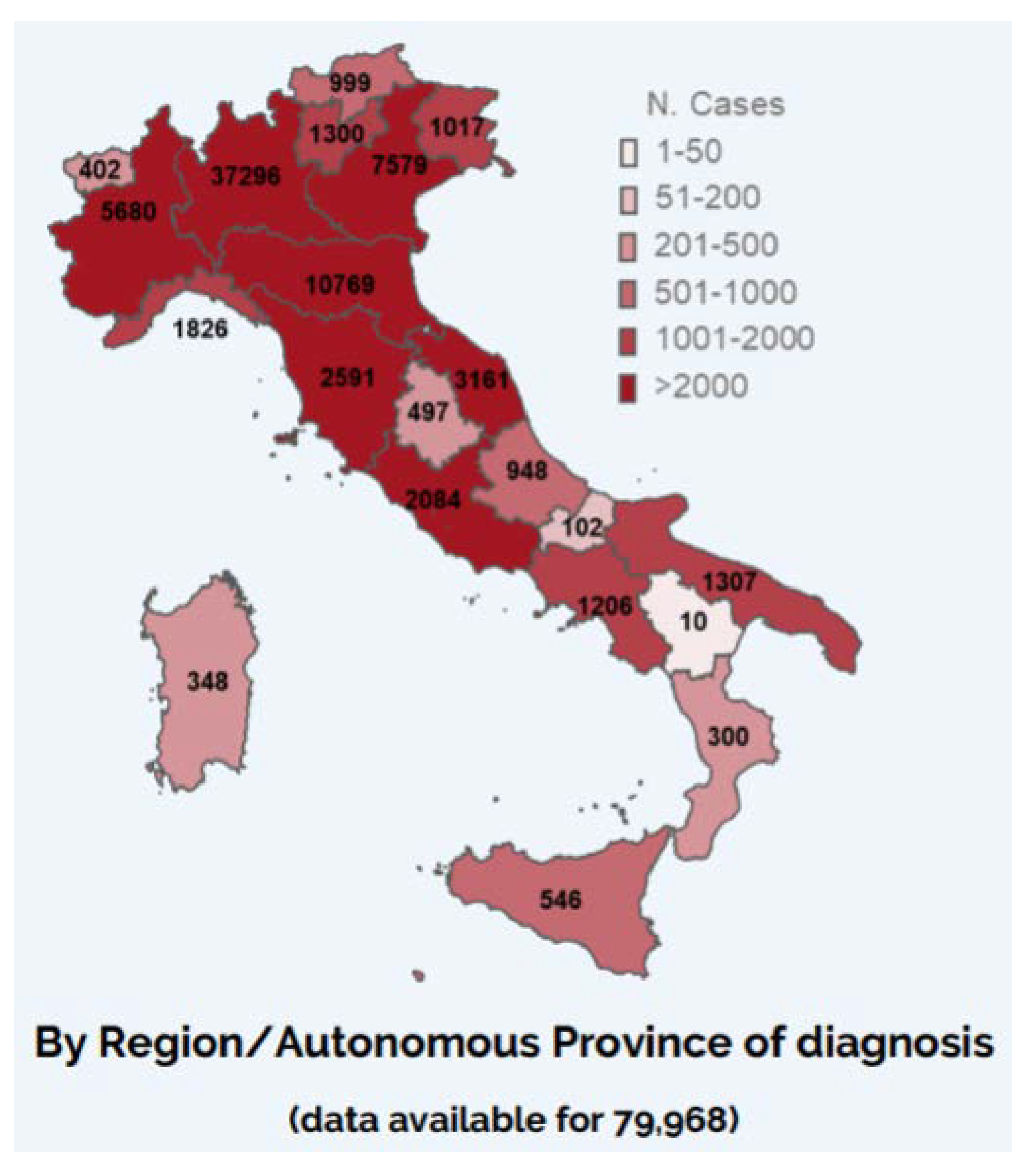
2.3. The Italian Epidemiological Situation Regarding COVID-19
3. Management and Outcome
3.1. Non-Pharmaceutical Intervention Measures Taken by Italian Authorities
3.2. Economic Impact and Mathematical Modelling Predictions
3.3. Impact on Society and Implications of the Media and Social Media
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Statista Research Department: Coronavirus (COVID-19) in Italy–Statistics & Facts. Available online: https://www.statista.com/topics/6061/coronavirus-covid-19-in-italy/ (accessed on 1 December 2020).
- Worldometers: COVID-19, Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/#countries (accessed on 27 March 2020).
- Bloomberg (23/03/2020): “The Lessons from Italy’s COVID-19 Mistakes”. Available online: https://www.bloomberg.com/opinion/articles/2020-03-23/italy-s-covid-19-trial-and-error-and-lessons-for-france-and-u-k (accessed on 27 March 2020).
- Bontempi, E. The Europe Second Wave of COVID-19 Infection and the Italy "Strange" Situation. Environ. Res. 2020, 110476. [Google Scholar] [CrossRef]
- Worldatlas: Italy. Available online: https://www.worldatlas.com/webimage/countrys/europe/it.htm#page (accessed on 27 March 2020).
- Worldometers: Italy Demographics. Available online: https://www.worldometers.info/demographics/italy-demographics/ (accessed on 27 March 2020).
- Macrotrends: Countries—Italy. Available online: https://www.macrotrends.net/countries/ITA/italy/population (accessed on 27 March 2020).
- UN Data: Italy—Country Profile. Available online: http://data.un.org/en/iso/it.html (accessed on 27 March 2020).
- OECD Data: Italy. Available online: https://data.oecd.org/italy.htm (accessed on 27 March 2020).
- The Italian Government. Available online: http://www.governo.it/it (accessed on 27 March 2020).
- OECD and European Observatory on Health Systems and Policies. Italy: Country Health Profile 2019, State of Health in the EU. Available online: http://www.euro.who.int/__data/assets/pdf_file/0010/419464/Country-Health-Profile-2019-Italy.pdf?ua=1 (accessed on 17 December 2020).
- European Observatory on Health Systems and Policies and WHO Regional Office for Europe. Italy. In Organization and Financing of Public Health Services in Europe: Country Reports; Rechel, B., Maresso, A., Sagan, A., Hernandez-Quevedo, C., Williams, G., Richardson, E., Jakubowski, E., Nolte, E., Eds.; European Observatory on Health Systems and Policies: Copenhagen, Denmark, 2018; pp. 49–65. [Google Scholar]
- QuiFinanza (2019): Sanità, I Paesi Dove Funziona Meglio: Come L’italia Si È Conquistata Un Posto In Classifica (Health Care, the Countries Where it Works Best: How Italy Won A Place in the Rankings). Available online: https://quifinanza.it/info-utili/sanita-paesi-dove-funziona-meglio-italia-posto-classifica/313244/ (accessed on 27 March 2020).
- COVID-19 Task Force of the Department of Infectious Diseases and IT Service, Istituto Superiore di Sanità (ISS). COVID-19 Epidemic, National Update: 19 March 2020. Available online: https://www.epicentro.iss.it/coronavirus/bollettino/Bollettino%20sorveglianza%20integrata%20COVID-19_19-marzo%202020.pdf (accessed on 2 December 2020).
- COVID-19 Task Force of the Department of Infectious Diseases and IT Service, Istituto Superiore di Sanità (ISS). Integrated Surveillance of COVID-19 in Italy, Update: 27 March 2020. Available online: https://www.epicentro.iss.it/coronavirus/bollettino/Infografica_27marzo%20ENG.pdf (accessed on 17 December 2020).
- Civil Protection Department. Chronology of Main Steps and Legal Acts Taken by the Italian Government for the Containment of the COVID-19 Epidemiological Emergency, Updated at 12 of March 2020. Available online: http://www.protezionecivile.gov.it/documents/20182/1227694/Summary+of+measures+taken+against+the+spread+of+C-19/c16459ad-4e52-4e90-90f3-c6a2b30c17eb (accessed on 17 December 2020).
- National Institute of Health (ISS) (08/11/2020): ISS for COVID-19—How to Behave Outdoors. Available online: https://www.iss.it/fuori-casa-come-comportarsi?p_p_id=com_liferay_asset_publisher_web_portlet_AssetPublisherPortlet_INSTANCE_yX1afjCDBkWH&p_p_lifecycle=0&p_p_state=normal&p_p_mode=view&_com_liferay_asset_publisher_web_portlet_AssetPublisherPortlet_INSTANCE_yX1afjCDBkWH_cur=0&p_r_p_resetCur=false&_com_liferay_asset_publisher_web_portlet_AssetPublisherPortlet_INSTANCE_yX1afjCDBkWH_assetEntryId=5513418#5513418 (accessed on 1 December 2020).
- Ministry of Health. Circular n. 32850 issued on the 12 October 2020, COVID19—Directions for the Duration and Ending of Isolation and Quarantine. Available online: https://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2020&codLeg=76613&parte=1%20&serie=null (accessed on 17 December 2020).
- Ministry of Health: FAQ—COVID-19, Questions and Answers. Available online: http://www.salute.gov.it/portale/nuovocoronavirus/dettaglioFaqNuovoCoronavirus.jsp?lingua=italiano&id=228#11 (accessed on 27 March 2020).
- The Italian Government: Press Release of the Council of the Ministers n. 38 (24/03/20). Available online: http://www.governo.it/it/articolo/comunicato-stampa-del-consiglio-dei-ministri-n-38/14376 (accessed on 27 March 2020).
- National Research Council (Cnr) (17/03/2020): Mathematical Models for Predicting the Spread of the COVID-19 Epidemic. Available online: https://www.cnr.it/it/nota-stampa/n-9287/modelli-matematici-per-la-previsione-della-diffusione-dell-epidemia-covid-19 (accessed on 27 March 2020).
- Reply (09/03/20): Preliminary Report on COVID-19 and Its Implications—Coronavirus: The Impact on Consumers and Enterprises. Available online: https://www.reply.com/it/covid-19-report (accessed on 27 March 2020).
- IFRC, UNICEF and WHO. Social Stigma Associated with COVID-19: A Guide to Preventing and Addressing Social Stigma, 24/02/20. Available online: https://www.unicef.org/media/65931/file/Social%20stigma%20associated%20with%20the%20coronavirus%20disease%202019%20(COVID-19).pdf (accessed on 17 December 2020).
- Agenzia Italia (AGI) (24/03/2020): Coronavirus on Social Media, the Most Shared Words. Available online: https://www.agi.it/cronaca/news/2020-03-25/multe-coronavirus-social-discussioni-7843700/ (accessed on 27 March 2020).
- Díaz-Pachón, D.A.; Rao, J.S. A Simple Correction for Covid-19 Testing Bias. Available online: https://arxiv.org/abs/2007.07426 (accessed on 17 December 2020).
- Castro, R.; Luz, P.M.; Wakimoto, M.D.; Veloso, V.G.; Grinsztejn, B.; Perazzo, H. COVID-19: A meta-analysis of diagnostic test accuracy of commercial assays registered in Brazil. Braz. J. Infect. Dis. 2020, 24, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Auriemma, V.; Iannaccone, C. COVID-19 Pandemic: Socio-Economic Consequences of Social Distancing Measures in Italy. Front. Sociol. 2020, 5. [Google Scholar] [CrossRef]
- UNCTAD: Services Sector Vital to COVID-19 Economic Recovery. Available online: https://unctad.org/news/services-sector-vital-covid-19-economic-recovery (accessed on 1 December 2020).
- Italian Government. Il Decreto Ristori. Available online: http://www.governo.it/it/approfondimento/il-decreto-ristori/15550 (accessed on 1 December 2020).
- Italian Ministry of Foreign Affairs: COVID-19: DPCM 24 OTTOBRE 2020, NOVITÀ. Available online: https://consbasilea.esteri.it/consolato_basilea/it/la_comunicazione/dal_consolato/covid-19-dpcm-24-ottobre-2020-novita.html (accessed on 1 December 2020).
- Paterlini, M. Covid:19: Italy Has Wasted the Sacrifices of the First Wave, Say Experts. Available online: https://www.bmj.com/content/371/bmj.m4279 (accessed on 1 December 2020).



{kind=link}
{kind=link}
{kind=link}
| Age Group | Male | Female | Total | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N. Cases | % Cases by Sex | N. Deaths | % Deaths by Sex | % CFR | N. Cases | % Cases by Sex | N. Deaths | % Deaths by Sex | % CFR | N. Cases | % Cases by Age Group | N. Deaths | % Deaths by Age Group | % CFR | |
| 0–9 | 324 | 55.5 | 0 | 0.0 | 0.0 | 260 | 44.5 | 0 | 0.0 | 0.0 | 589 | 0.6 | 0 | 0.0 | 0.0 |
| 10–19 | 392 | 51.4 | 0 | 0.0 | 0.0 | 371 | 48.6 | 0 | 0.0 | 0.0 | 766 | 0.8 | 0 | 0.0 | 0.0 |
| 20–29 | 1631 | 43.3 | 1 | 50.0 | 0.1 | 2132 | 56.7 | 1 | 50.0 | 0.0 | 3830 | 4.1 | 2 | 0.0 | 0.1 |
| 30–39 | 3105 | 48.1 | 18 | 90.0 | 0.6 | 3352 | 51.9 | 2 | 10.0 | 0.1 | 6523 | 6.9 | 20 | 0.2 | 0.3 |
| 40–49 | 5802 | 48.4 | 66 | 74.2 | 1.1 | 6198 | 51.6 | 23 | 25.8 | 0.4 | 12,084 | 12.8 | 89 | 0.9 | 0.7 |
| 50–59 | 10,068 | 54.2 | 294 | 79.9 | 2.9 | 8495 | 45.8 | 74 | 20.1 | 0.9 | 18,678 | 19.8 | 369 | 3.7 | 2.0 |
| 60–69 | 10,744 | 65.8 | 923 | 79.6 | 8.6 | 5584 | 34.2 | 236 | 20.4 | 4.2 | 16,395 | 17.4 | 1162 | 11.6 | 7.1 |
| 70–79 | 11,236 | 64.7 | 2597 | 75.3 | 23.1 | 6142 | 35.3 | 854 | 24.7 | 13.9 | 17,464 | 18.5 | 3456 | 34.5 | 19.8 |
| 80–89 | 7630 | 54.0 | 2603 | 65.4 | 34.1 | 6504 | 46.0 | 1378 | 34.6 | 21.2 | 14,186 | 15.0 | 3984 | 39.7 | 28.1 |
| >90 | 1160 | 32.5 | 424 | 45.2 | 36.6 | 2404 | 67.5 | 514 | 54.8 | 21.4 | 3573 | 3.8 | 939 | 9.4 | 26.3 |
| Unknown | 114 | 51.6 | 4 | 80.0 | 3.5 | 107 | 48.4 | 1 | 20.0 | 0.9 | 224 | 0.2 | 5 | 0.0 | 2.2 |
| Total | 52,206 | 6930 | 13.3 | 41,549 | 3083 | 7.4 | 94,312 | 10,026 | 10.6 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortenzi, F.; Albanese, E.; Fadda, M. A Transdisciplinary Analysis of COVID-19 in Italy: The Most Affected Country in Europe. Int. J. Environ. Res. Public Health 2020, 17, 9488. https://doi.org/10.3390/ijerph17249488
Ortenzi F, Albanese E, Fadda M. A Transdisciplinary Analysis of COVID-19 in Italy: The Most Affected Country in Europe. International Journal of Environmental Research and Public Health. 2020; 17(24):9488. https://doi.org/10.3390/ijerph17249488
Chicago/Turabian StyleOrtenzi, Flaminia, Emiliano Albanese, and Marta Fadda. 2020. "A Transdisciplinary Analysis of COVID-19 in Italy: The Most Affected Country in Europe" International Journal of Environmental Research and Public Health 17, no. 24: 9488. https://doi.org/10.3390/ijerph17249488
APA StyleOrtenzi, F., Albanese, E., & Fadda, M. (2020). A Transdisciplinary Analysis of COVID-19 in Italy: The Most Affected Country in Europe. International Journal of Environmental Research and Public Health, 17(24), 9488. https://doi.org/10.3390/ijerph17249488