Heart Rate Variability in Women with Systemic Lupus Erythematosus: Association with Health-Related Parameters and Effects of Aerobic Exercise

 , , ,
, , , 


Abstract
:1. Introduction
2. Materials and Methods
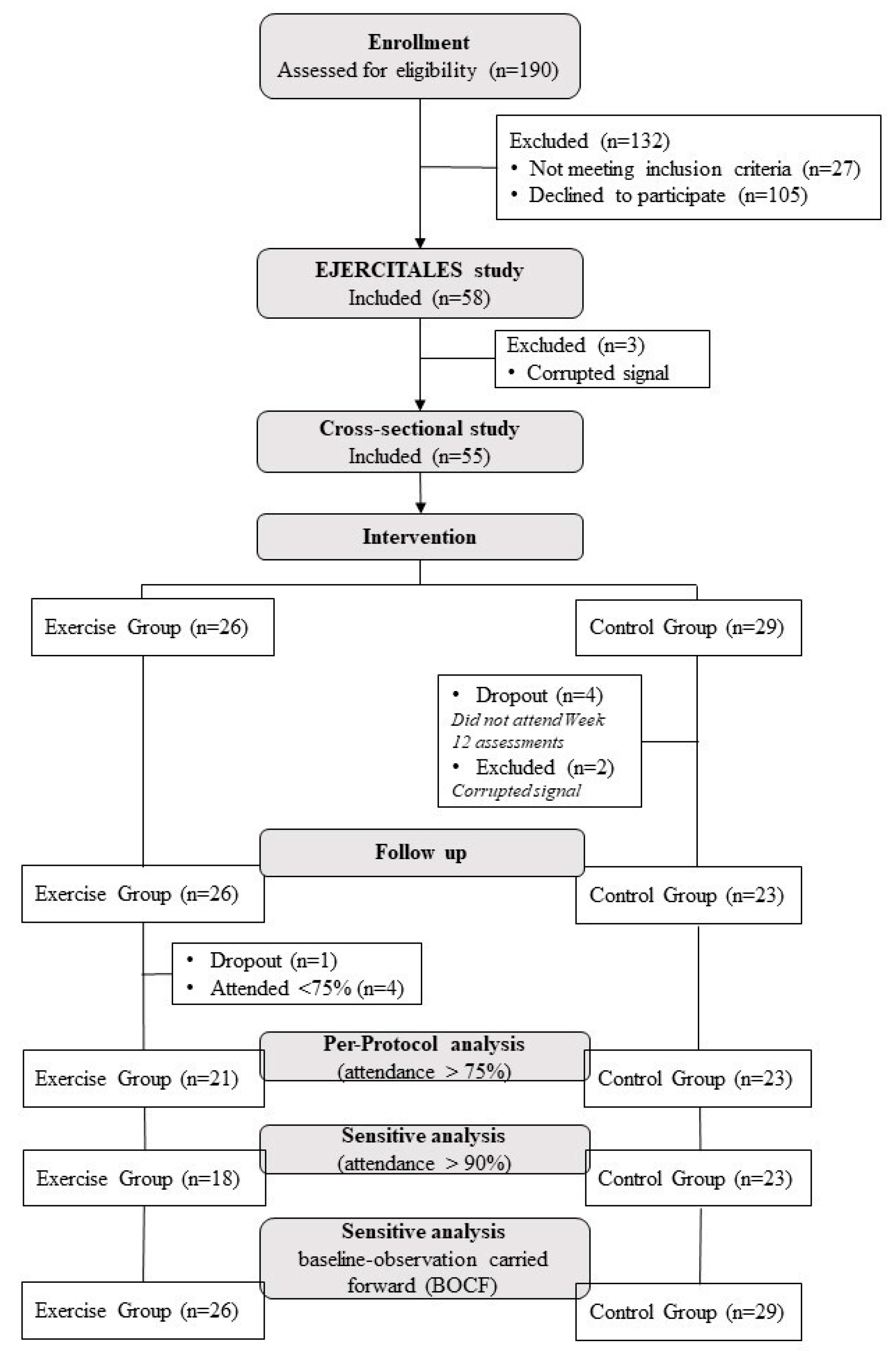
2.1. Study Design and Participants
2.2. Intervention
2.2.1. Exercise Group
2.2.2. Control Group
2.3. Heart Rate Variability
2.4. Patient-Reported Outcomes
2.5. Inflammatory and Oxidative Stress Markers
2.6. Other Measurements
2.7. Classification of Responders, Non-Responders, and Adverse Responders
2.8. Treatment Allocation and Blinding
2.9. Statistical Analysis
3. Results
3.1. Associations of HRV with Inflammatory, Oxidative Stress Markers, and PROs (Aim 1)
3.2. Effects of the Exercise Intervention on HRV-Derived Parameters (Aim 2)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Margery-Muir, A.A.; Bundell, C.; Nelson, D.; Groth, D.M.; Wetherall, J.D. Gender balance in patients with systemic lupus erythematosus. Autoimmun. Rev. 2017, 16, 258–268. [Google Scholar] [CrossRef] [PubMed]
- Lisnevskaia, L.; Murphy, G.; Isenberg, D. Systemic lupus erythematosus. Lancet 2014, 384, 1878–1888. [Google Scholar] [CrossRef]
- Stojan, G.; Petri, M. Epidemiology of systemic lupus erythematosus: An update. Curr. Opin. Rheumatol. 2018, 30, 144–150. [Google Scholar] [CrossRef]
- Ocampo-Piraquive, V.; Nieto-Aristizábal, I.; Cañas, C.A.; Tobón, G.J. Mortality in systemic lupus erythematosus: Causes, predictors and interventions. Expert Rev. Clin. Immunol. 2018, 14, 1043–1053. [Google Scholar] [CrossRef]
- Liu, Y.; Kaplan, M.J. Cardiovascular disease in systemic lupus erythematosus: An update. Curr. Opin. Rheumatol. 2018, 30, 441–448. [Google Scholar] [CrossRef]
- Freeman, J.V.; Dewey, F.E.; Hadley, D.M.; Myers, J.; Froelicher, V.F. Autonomic Nervous System Interaction With the Cardiovascular System During Exercise. Prog. Cardiovasc. Dis. 2006, 48, 342–362. [Google Scholar] [CrossRef]
- Lahiri, M.K.; Kannankeril, P.J.; Goldberger, J.J. Assessment of Autonomic Function in Cardiovascular Disease. Physiological Basis and Prognostic Implications. J. Am. Coll. Cardiol. 2008, 51, 1725–1733. [Google Scholar] [CrossRef] [Green Version]
- Marsland, A.L.; Gianaros, P.J.; Prather, A.A.; Jennings, J.R.; Neumann, S.A.; Manuck, S.B. Stimulated production of proinflammatory cytokines covaries inversely with heart rate variability. Psychosom. Med. 2007, 69, 709–716. [Google Scholar] [CrossRef]
- Task Force Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur. Heart J. 1996, 17, 354–381. Available online: https://www.escardio.org/static-file/Escardio/Guidelines/Scientific-Statements/guidelines-Heart-Rate-Variability-FT-1996.pdf (accessed on 14 December 2020). [CrossRef] [Green Version]
- Singh, N.; Moneghetti, K.J.; Christle, J.W.; Hadley, D.; Plews, D.; Froelicher, V.; Plews, D. Heart Rate Variability: An Old Metric with New Meaning in the Era of using mHealth Technologies for Health and Exercise Training Guidance. Part One: Physiology and Methods. Arrhythmia Electrophysiol. Rev. 2018, 7, 193–198. [Google Scholar] [CrossRef] [Green Version]
- Stojanovich, L. Autonomic dysfunction in autoimmune rheumatic disease. Autoimmun. Rev. 2009, 8, 569–572. [Google Scholar] [CrossRef] [PubMed]
- Laversuch, C.J.; Seo, H.; Modarres, H.; Collins, D.A.; McKenna, W.; Bourke, B.E. Reduction in heart rate variability in patients with systemic lupus erythematosus. J. Rheumatol. 1997, 24, 1540–1544. [Google Scholar] [PubMed]
- Aydemir, M.; Yazisiz, V.; Basarici, I.; Avci, A.; Erbasan, F.; Belgi, A.; Terzioglu, E. Cardiac autonomic profile in rheumatoid arthritis and systemic lupus erythematosus. Lupus 2010, 19, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Thanou, A.; Stavrakis, S.; Dyer, J.W.; Munroe, M.E.; James, J.A.; Merrill, J.T. Impact of heart rate variability, a marker for cardiac health, on lupus disease activity. Arthritis Res. Ther. 2016, 18, 197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matusik, P.S.; Matusik, P.T.; Stein, P.K. Heart rate variability in patients with systemic lupus erythematosus: A systematic review and methodological considerations. Lupus 2018, 27, 1225–1239. [Google Scholar] [CrossRef]
- Tselios, K.; Gladman, D.D.; Harvey, P.; Su, J.; Urowitz, M.B. Severe brady-arrhythmias in systemic lupus erythematosus: Prevalence, etiology and associated factors. Lupus 2018, 27, 1415–1423. [Google Scholar] [CrossRef]
- Whelton, S.P.; Narla, V.; Blaha, M.J.; Nasir, K.; Blumenthal, R.S.; Jenny, N.S.; Al-Mallah, M.H.; Michos, E.D. Association between resting heart rate and inflammatory biomarkers (high-sensitivity C-reactive protein, interleukin-6, and fibrinogen) (from the Multi-Ethnic Study of Atherosclerosis). Am. J. Cardiol. 2014, 113, 644–649. [Google Scholar] [CrossRef] [Green Version]
- O’Dwyer, T.; Durcan, L.; Wilson, F. Exercise and physical activity in systemic lupus erythematosus: A systematic review with meta-analyses. Semin. Arthritis Rheum. 2017, 47, 204–215. [Google Scholar] [CrossRef]
- Soriano-Maldonado, A.; Morillas-de-Laguno, P.; Sabio, J.M.; Gavilán-Carrera, B.; Rosales-Castillo, A.; Montalbán-Méndez, C.; Sáez-Urán, L.M.; Callejas-Rubio, J.L.; Vargas-Hitos, J.A. Effects of 12-week Aerobic Exercise on Arterial Stiffness, Inflammation, and Cardiorespiratory Fitness in Women with Systemic LUPUS Erythematosus: Non-Randomized Controlled Trial. J. Clin. Med. 2018, 7, 477. [Google Scholar] [CrossRef] [Green Version]
- Gavilán-Carrera, B.; Vargas-Hitos, J.A.; Morillas-de-laguno, P.; Rosales-Castillo, A.; Sola-Rodríguez, S.; Callejas-Rubio, L.; Sabio, M.; Soriano-Maldonado, A. Effects of 12-week aerobic exercise on patient-reported outcomes in women with systemic lupus erythematosus. Disabil. Rehabil. 2020, 1–9. [Google Scholar] [CrossRef]
- Sloan, R.A.; Sawada, S.S.; Martin, C.K.; Church, T.; Blair, S.N. Associations between cardiorespiratory fitness and health-related quality of life. Health Qual. Life Outcomes 2009, 7, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myers, J.; McAuley, P.; Lavie, C.J.; Despres, J.-P.; Arena, R.; Kokkinos, P. Physical Activity and Cardiorespiratory Fitness as Major Markers of Cardiovascular Risk: Their Independent and Interwoven Importance to Health Status. Prog. Cardiovasc. Dis. 2015, 57, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Fanouriakis, A.; Kostopoulou, M.; Alunno, A.; Aringer, M.; Bajema, I.; Boletis, J.N.; Cervera, R.; Doria, A.; Gordon, C.; Govoni, M.; et al. 2019 Update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 736–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benatti, F.B.; Pedersen, B.K. Exercise as an anti-inflammatory therapy for rheumatic diseases-myokine regulation. Nat. Rev. Rheumatol. 2015, 11, 86–97. [Google Scholar] [CrossRef]
- Lavie, C.J.; Ozemek, C.; Carbone, S.; Katzmarzyk, P.T.; Blair, S.N. Sedentary Behavior, Exercise, and Cardiovascular Health. Circ. Res. 2019, 124, 799–815. [Google Scholar] [CrossRef]
- Anderson, L.; Thompson, D.R.; Oldridge, N.; Zwisler, A.-D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2016, 67, 1–12. [Google Scholar]
- Speck, R.M.; Courneya, K.S.; Mâsse, L.C.; Duval, S.; Schmitz, K.H. An update of controlled physical activity trials in cancer survivors: A systematic review and meta-analysis. J. Cancer Surviv. 2010, 4, 87–100. [Google Scholar] [CrossRef]
- Yorgun, H.; Canpolat, U.; Aytemir, K.; Ateş, A.; Kaya, E.; Akdoğan, A.; Sunman, H.; Canpolat, A.G.; Çalgüneri, M.; Kabakçı, G.; et al. Evaluation of cardiac autonomic functions in patients with systemic lupus erythematosus. Lupus 2012, 21, 373–379. [Google Scholar] [CrossRef]
- Bienias, P.; Ciurzyński, M.; Chrzanowska, A.; Dudzik-Niewiadomska, I.; Irzyk, K.; Oleszek, K.; Kalińska-Bienias, A.; Kisiel, B.; Tłustochowicz, W.; Pruszczyk, P. Attenuated post-exercise heart rate recovery in patients with systemic lupus erythematosus: The role of disease severity and beta-blocker treatment. Lupus 2018, 27, 217–224. [Google Scholar] [CrossRef]
- Slade, S.C.; Dionne, C.E.; Underwood, M.; Buchbinder, R.; Beck, B.; Bennell, K.; Brosseau, L.; Costa, L.; Cramp, F.; Cup, E.; et al. Consensus on Exercise Reporting Template (CERT): Modified Delphi Study. Phys. Ther. 2016, 96, 1514–1524. [Google Scholar] [CrossRef]
- Giles, D.; Draper, N.; Neil, W. Validity of the Polar V800 heart rate monitor to measure RR intervals at rest. Eur. J. Appl. Physiol. 2016, 116, 563–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarvainen, M.P.; Lipponen, J.; Niskanen, J.-P.; Ranta-aho, P.O. User’s Guide HRV. 2017. Available online: https://www.kubios.com/downloads/Kubios_HRV_Users_Guide.pdf (accessed on 14 December 2020).
- Alonso, J.; Prieto, L.; Anto, J.M. The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): An instrument for measuring clinical results. Med. Clin. 1995, 104, 771–776. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Smets, E.M.A.; Garssen, B.; Bonke, B.; De Haes, J.C.J.M. The multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J. Psychosom. Res. 1995, 39, 315–325. [Google Scholar] [CrossRef] [Green Version]
- Weiss, W.; Gohlisch, C.; Harsch-Gladisch, C.; Tölle, M.; Zidek, W.; van der Giet, M. Oscillometric estimation of central blood pressure: Validation of the Mobil-O-Graph in comparison with the SphygmoCor device. Blood Press. Monit. 2012, 17, 128–131. [Google Scholar] [CrossRef] [Green Version]
- Petri, M. Disease activity assessment in SLE: Do we have the right instruments? Ann. Rheum. Dis. 2007, 66, 61–64. [Google Scholar] [CrossRef] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, W.G. Measures of Reliability in Sports Medicine and Science. Curr. Opin. Sport. Med. 2000, 30, 1–15. [Google Scholar]
- Riemann, B.L.; Lininger, M.R. Statistical Primer for Athletic Trainers: The Essentials of Understanding Measures of Reliability and Minimal Important Change. J. Athl. Train. 2018, 53, 98. [Google Scholar] [CrossRef] [Green Version]
- Ndrepepa, G. Myeloperoxidase—A bridge linking inflammation and oxidative stress with cardiovascular disease. Clin. Chim. Acta 2019, 493, 36–51. [Google Scholar] [CrossRef]
- Heslop, C.L.; Frohlich, J.J.; Hill, J.S. Myeloperoxidase and C-Reactive Protein Have Combined Utility for Long-Term Prediction of Cardiovascular Mortality After Coronary Angiography. J. Am. Coll. Cardiol. 2010, 55, 1102–1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aeschbacher, S.; Schoen, T.; Dörig, L.; Kreuzmann, R.; Neuhauser, C.; Schmidt-Trucksäss, A.; Probst-Hensch, N.M.; Risch, M.; Risch, L.; Conen, D. Heart rate, heart rate variability and inflammatory biomarkers among young and healthy adults. Ann. Med. 2017, 49, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, A.L.; Peng, C.K.; Lipsitz, L.A. What is physiologic complexity and how does it change with aging and disease? Neurobiol. Aging 2002, 23, 23–26. [Google Scholar] [CrossRef]
- Haensel, A.; Mills, P.J.; Nelesen, R.A.; Ziegler, M.G.; Dimsdale, J.E. The relationship between heart rate variability and inflammatory markers in cardiovascular diseases. Psychoneuroendocrinology 2012, 76, 211–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiweck, C.; Piette, D.; Berckmans, D.; Claes, S.; Vrieze, E. Heart rate and high frequency heart rate variability during stress as biomarker for clinical depression. A systematic review. Psychol. Med. 2019, 49, 200–211. [Google Scholar] [CrossRef]
- Crosswell, A.D.; Lockwood, K.G.; Ganz, P.A.; Bower, J.E. Low heart rate variability and cancer-related fatigue in breast cancer survivors. Psychoneuroendocrinology 2014, 45, 58. [Google Scholar] [CrossRef] [Green Version]
- Pagani, M.; Lucini, D. Chronic fatigue syndrome: A hypothesis focusing on the autonomic nervous system. Clin. Sci. 1999, 96, 117–125. [Google Scholar] [CrossRef] [Green Version]
- Balsamo, S.; Santos-Neto, L. dos Fatigue in systemic lupus erythematosus: An association with reduced physical fitness. Autoimmun. Rev. 2011, 10, 514–518. [Google Scholar] [CrossRef]
- Rivera-López, R.; Jiménez-Jáimez, J.; Sabio, J.M.; Zamora-Pasadas, M.; Vargas-Hitos, J.A.; Martínez-Bordonado, J.; Navarrete-Navarrete, N.; Fernández, R.R.; Sanchez-Cantalejo, E.; Jiménez-Alonso, J. Relationship between QT Interval Length and Arterial Stiffness in Systemic Lupus Erythematosus (SLE): A Cross-Sectional Case-Control Study. PLoS ONE 2016, 11, e0152291. [Google Scholar] [CrossRef] [Green Version]
- Vesterinen, V.; Nummela, A.; Heikura, I.; Laine, T.; Hynynen, E.; Botella, J.; Häkkinen, K. Individual Endurance Training Prescription with Heart Rate Variability. Med. Sci. Sports Exerc. 2016, 48, 1347–1354. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| All (n = 55) | Exercise (n = 26) | Control (n = 29) | p | |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | ||
| Age, years | 43.5 (14.0) | 42.9 (15.1) | 43.9 (13.3) | 0.808 |
| BMI, kg/m2 | 25.4 (4.8) | 25.9 (3.4) | 25.0 (5.8) | 0.491 |
| SBP, mm/Hg | 117.5 (10.3) | 116.8 (9.9) | 118.1 (10.6) | 0.653 |
| DBP, mm/Hg | 75.3 (9.4) | 75.5 (8.7) | 75.1 (10.01) | 0.843 |
| MBP, mm/Hg | 94.6 (8.7) | 94.5 (8.3) | 94.7 (9.2) | 0.937 |
| Mean HR, bpm | 76.70 (10.71) | 79.11 (9.76) | 74.54 (11.23) | 0.112 |
| hsCRP, mg/L (median, IQR) | 1.6 (2.6–6.5) | 2.2 (1.9–7.6) | 1.2 (1.5–7.1) | 0.218 |
| IL-6, pg/mL (median, IQR) | 10.5 (9.4–12.3) | 8.2 (7.1–11.7) | 11.3 (10.3–14.0) | 0.018 |
| TNF-α, pg/mL (median, IQR) | 15.6 (15.7–19.8) | 16.5 (15.4–21.1) | 14.8 (14.3–20.4) | 0.385 |
| MPO, ng/mL (median, IQR) | 69.6 (79.1–119.6) | 60.1 (62.4–126.9) | 75.7 (76.3–130.9) | 0.385 |
| Smoke (%) | 23.6 | 15.4 | 31.0 | 0.237 |
| Menopause (%) | 38.2 | 38.5 | 37.9 | 0.968 |
| Dyslipidemia (%) | 16.4 | 19.2 | 13.8 | 0.586 |
| Statins (%) | 16.4 | 23.1 | 10.3 | 0.203 |
| Immunosuppressants (%) | 45.5 | 46.1 | 44.8 | 0.921 |
| Current corticosteroid intake (mg/day) | 3.86 (5.1) | 4.08 (6.1) | 3.70 (4.2) | 0.789 |
| Disease duration, years | 15.1 (10.1) | 14.54 (10.4) | 15.6 (9.9) | 0.704 |
| Total PA, min/week | 94.8 (92.6) | 97.5 (95.9) | 92.4 (91.1) | 0.660 |
| SLEDAI | 0.16 (0.764) | 0.04 (0.196) | 0.28 (1.0) | 0.254 |
| SDI | 0.42 (1.1) | 0.19 (0.63) | 0.62 (1.3) | 0.145 |
| Psychological Stress (PSS; 0–56; median, IQR) | 31.0 (28.9–32.1) | 30.0 (27.7–31.6) | 31.0 (28.7–33.9) | 0.303 |
| Depressive symptoms (BDI-II; 0–63) | 12.8 (9.2) | 8.0 (6.4–12.7) | 17.0 (12.2–19.3) | 0.011 |
| Fatigue (MFI-S; 0–20) | ||||
| General Fatigue (median, IQR) | 15.0 (12.9–15.1) | 14.5 (12.1–15.3) | 16.0 (12.5–15.9) | 0.498 |
| Physical fatigue | 12.8 (4.7) | 12.4 (4.8) | 13.1 (4.7) | 0.577 |
| Reduced Activity (median, IQR) | 10.0 (8.7–11.5) | 8.0 (7.8–11.5) | 11.0 (8.4–12.6) | 0.741 |
| Reduced Motivation | 9.4 (3.7) | 8.5 (3.4) | 10.1 (3.9) | 0.112 |
| Mental Fatigue | 12.2 (2.8) | 12.04 (3.0) | 12.3 (2.6) | 0.720 |
| Health-related quality of life (SF-36; 0–00) * | ||||
| Physical Component Summary | 43.0 (8.2) | 45.5 (8.5) | 40.6 (7.8) | 0.034 |
| Mental Component Summary | 44.9 (11.0) | 47.5 (11.7) | 40.4 (11.0) | 0.106 |
| All (n = 55) | Exercise (n = 26) | Control (n = 29) | p | |
|---|---|---|---|---|
| Median (IQR) | Median (IQR) | Median (IQR) | ||
| SDNN, ms | 19.59 (13.30–25.80) | 15.87 (11.34–25.24) | 21.42 (14.55–26.36) | 0.376 |
| RMSSD, ms | 16.20 (11.55–25.07) | 14.82 (8.86–24.86) | 17.33 (13.61–26.75) | 0.292 |
| pNN50 (%) | 0.57 (0.21–3.17) | 0.42 (0.22–2.78) | 0.70 (0.22–3.48) | 0.715 |
| LF, ms2 | 164.12 (76.51–340.51) | 157.23 (76.51–345.26) | 198.18 (76.51–345.26) | 0.607 |
| HF, ms2 | 97.20 (39.31–299.42) | 93.65 (29.92–334.81) | 100.37 (59.40–216.69) | 0.607 |
| LFHF | 1.57 (0.93–2.81) | 1.31 (0.83–3.29) | 1.82 (1.08–2.55) | 0.980 |
| SD1, ms | 11.48 (8.18–17.75) | 10.49 (6.27–17.60) | 12.27 (9.64–17.60) | 0.292 |
| SD2, ms | 25.30 (15.54–30.46) | 20.86 (18.28–30.42) | 25.80 (18.29–30.42) | 0.423 |
| SampEn, au | 1.70 (1.55–1.83) | 1.70 (1.60–1.82) | 1.70 (1.51–1.83) | 0.692 |
| hsCRP | IL-6 | TNF-α | MPO | SLEDAI | SDI | PSS | BDI | MFI-General Fatigue | MFI-Physical Fatigue | MFI-Reduce Activity | MFI-Reduce Motivation | MFI-Mental Fatigue | SF-36 Physical Component | SF-36 Mental Component | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SDNN | −0.05 | −0.11 | −0.21 | 0.04 | −0.21 | −0.14 | 0.16 | −0.11 | 0.05 | −0.14 | −0.10 | −0.08 | −0.06 | −0.03 | −0.01 |
| RMSSD | −0.09 | −0.14 | −0.17 | −0.01 | −0.19 | −0.03 | 0.04 | −0.04 | 0.06 | −0.09 | 0.03 | 0.03 | 0.04 | 0.05 | −0.05 |
| pNN50 | −0.06 | −0.14 | −0.14 | 0.05 | −0.09 | −0.06 | 0.16 | −0.06 | 0.10 | −0.09 | 0.05 | −0.02 | 0.04 | 0.07 | −0.04 |
| LF | −0.03 | −0.08 | −0.23 | −0.08 | −0.16 | −0.17 | 0.17 | −0.13 | 0.10 | −0.08 | −0.10 | −0.13 | −0.05 | −0.03 | 0.01 |
| HF | −0.07 | −0.20 | −0.23 | −0.08 | −0.25 | −0.15 | 0.05 | −0.14 | −0.05 | −0.25 | −0.13 | −0.03 | −0.03 | 0.03 | −0.07 |
| LFHF | 0.05 | 0.32 * | 0.17 | 0.20 | 0.17 | 0.03 | 0.08 | 0.12 | 0.14 | 0.30 * | −0.13 | −0.05 | −0.05 | −0.11 | 0.17 |
| SD1 | −0.09 | −0.14 | −0.17 | −0.01 | −0.19 | −0.03 | 0.04 | −0.04 | 0.06 | −0.09 | −0.03 | 0.04 | 0.04 | 0.05 | −0.05 |
| SD2 | −0.03 | −0.09 | −0.21 | 0.09 | −0.20 | −0.17 | 0.18 | −0.14 | 0.06 | −0.14 | 0.03 | −0.09 | −0.09 | −0.05 | 0.00 |
| SampEn | −0.35 ** | −0.16 | −0.16 | −0.32 * | −0.03 | −0.05 | −0.19 | 0.15 | 0.05 | 0.04 | −0.12 | 0.23 | 0.23 | 0.14 | 0.14 |
| B | SE | CI 95% | p | ||
|---|---|---|---|---|---|
| LFHF | |||||
| IL-6 | 0.48 | 0.39 | −0.31 | 1.27 | 0.231 |
| MFI-Physical Fatigue | 0.89 | 0.37 | 0.15 | 1.62 | 0.019 |
| SampEn | |||||
| hsCRP | −4.82 | 1.89 | −8.62 | −1.03 | 0.014 |
| MPO | −106.51 | 37.85 | −182.54 | −30.50 | 0.007 |
| Change from Baseline at Week 12 | Exercise (n = 21) | Control (n = 23) | Median Difference (95% CI) | p |
|---|---|---|---|---|
| Median (SE) | Median (SE) | |||
| SDNN | 2.70 (2.36) | 4.18 (2.91) | −1.48 (−12.00 to 6.37) | 0.539 |
| RMSSD | 2.03 (3.52) | 2.75 (4.33) | −0.72 (−12.05 to 9.74) | 0.831 |
| pNN50 | 0.21 (1.93) | 0.28 (2.96) | −0.07 (−5.87 to 6.16) | 0.960 |
| LF (ms) | 2.50 (81.86) | −22.31 (57.00) | 24.81 (−142.07 to 169.88) | 0.858 |
| HF (ms) | 4.76 (98.31) | 6.91 (73.40) | −2.15 (−140.79 to 129.24) | 0.932 |
| LFHF | −0.12 (1.30) | 0.05 (1.01) | −0.17 (−01.45 to 2.30) | 0.652 |
| SD1 | 1.44 (2.49) | 1.95 (3.07) | −0.51 (−8.53 to 6.90) | 0.831 |
| SD2 | 3.10 (2.51) | 5.22 (3.04) | −2.45 (−11.91 to 6.33) | 0.539 |
| SampEn | 0.02 (0.07) | 0.01 (0.08) | 0.01 (−0.31 to 0.23) | 0.741 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Rosales, E.; Sola-Rodríguez, S.; Vargas-Hitos, J.A.; Gavilán-Carrera, B.; Rosales-Castillo, A.; Hernández-Martínez, A.; Artero, E.G.; Sabio, J.M.; Soriano-Maldonado, A. Heart Rate Variability in Women with Systemic Lupus Erythematosus: Association with Health-Related Parameters and Effects of Aerobic Exercise. Int. J. Environ. Res. Public Health 2020, 17, 9501. https://doi.org/10.3390/ijerph17249501
Martínez-Rosales E, Sola-Rodríguez S, Vargas-Hitos JA, Gavilán-Carrera B, Rosales-Castillo A, Hernández-Martínez A, Artero EG, Sabio JM, Soriano-Maldonado A. Heart Rate Variability in Women with Systemic Lupus Erythematosus: Association with Health-Related Parameters and Effects of Aerobic Exercise. International Journal of Environmental Research and Public Health. 2020; 17(24):9501. https://doi.org/10.3390/ijerph17249501
Chicago/Turabian StyleMartínez-Rosales, Elena, Sergio Sola-Rodríguez, José Antonio Vargas-Hitos, Blanca Gavilán-Carrera, Antonio Rosales-Castillo, Alba Hernández-Martínez, Enrique G. Artero, José Mario Sabio, and Alberto Soriano-Maldonado. 2020. "Heart Rate Variability in Women with Systemic Lupus Erythematosus: Association with Health-Related Parameters and Effects of Aerobic Exercise" International Journal of Environmental Research and Public Health 17, no. 24: 9501. https://doi.org/10.3390/ijerph17249501
APA StyleMartínez-Rosales, E., Sola-Rodríguez, S., Vargas-Hitos, J. A., Gavilán-Carrera, B., Rosales-Castillo, A., Hernández-Martínez, A., Artero, E. G., Sabio, J. M., & Soriano-Maldonado, A. (2020). Heart Rate Variability in Women with Systemic Lupus Erythematosus: Association with Health-Related Parameters and Effects of Aerobic Exercise. International Journal of Environmental Research and Public Health, 17(24), 9501. https://doi.org/10.3390/ijerph17249501