Assessing Health Impacts of Conventional Centralized and Emerging Resource Recovery-Oriented Decentralized Water Systems

Abstract
:1. Introduction
2. Method
2.1. Description of Evaluated Water and Wastewater Systems
2.2. Life Cycle Health Impact Assessment
2.2.1. Goal and Scope
2.2.2. Life Cycle Inventory
2.2.3. Life Cycle Impact Assessment
2.2.4. Life Cycle Interpretation
2.3. QMRA
2.3.1. Hazard Identification
2.3.2. Exposure and Dose Response Assessment
2.3.3. Risk Characterization
2.4. Integration of LCA and QMRA
3. Results
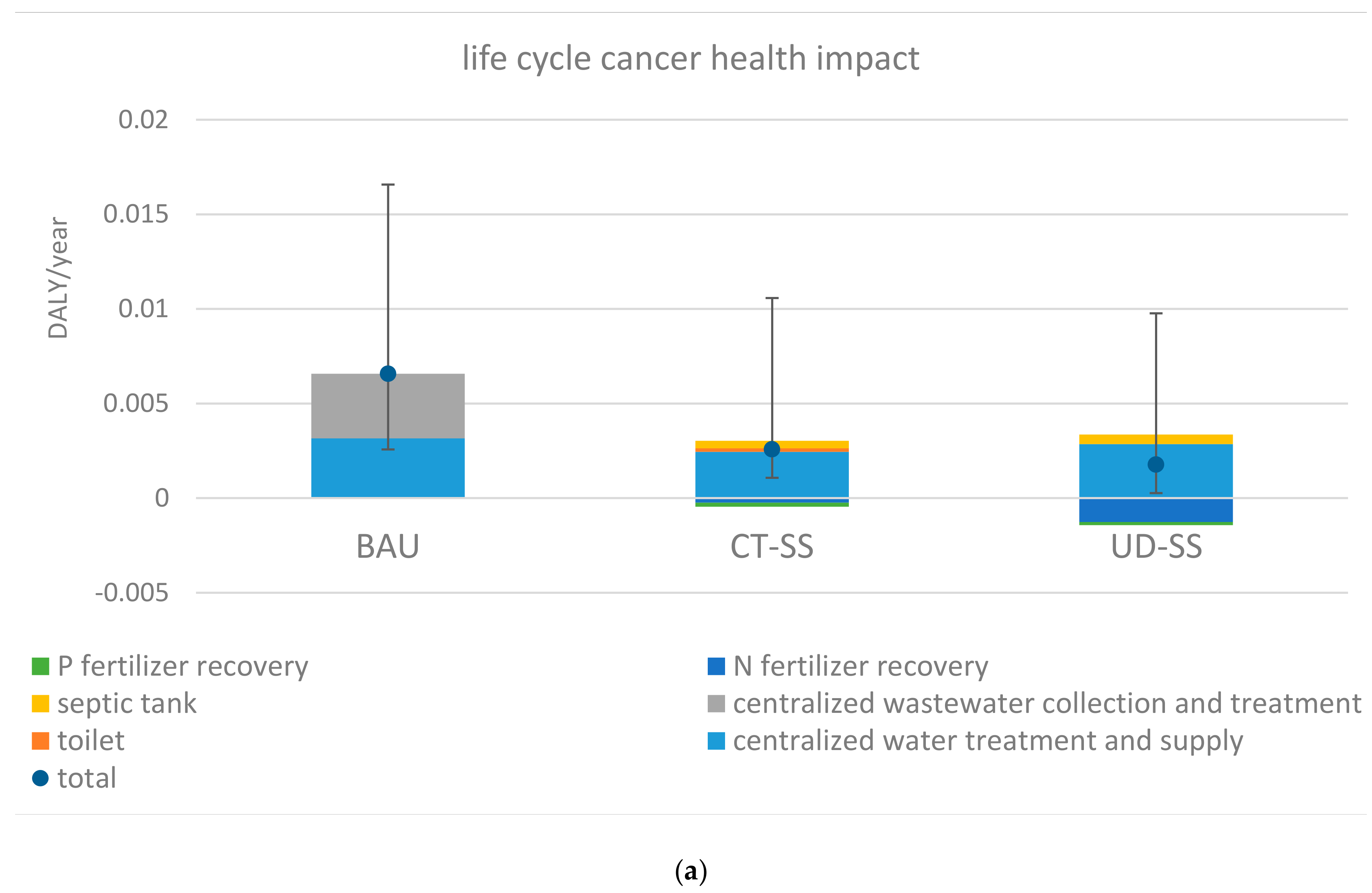
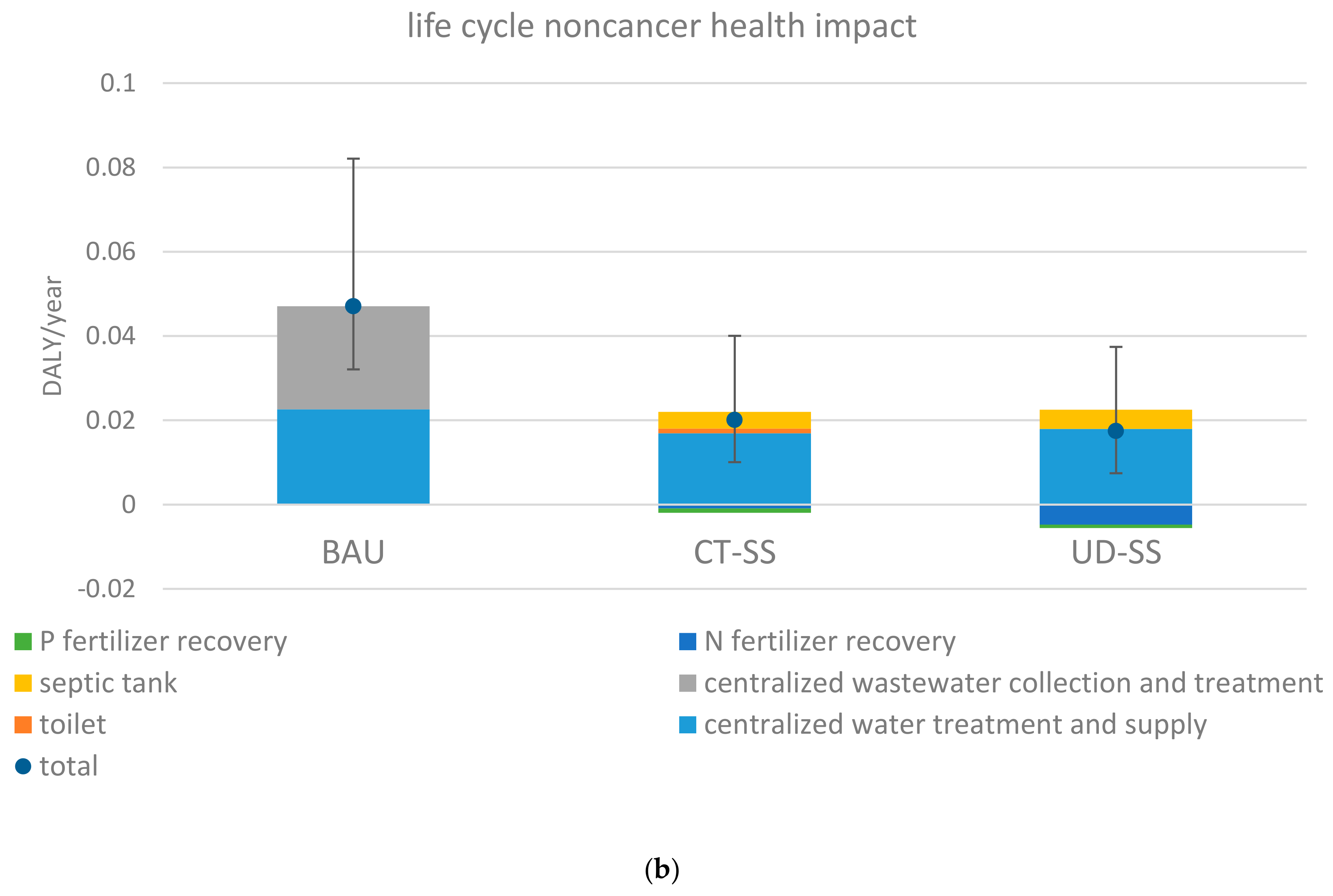
3.1. Magnitudes of Life Cycle Health Impacts
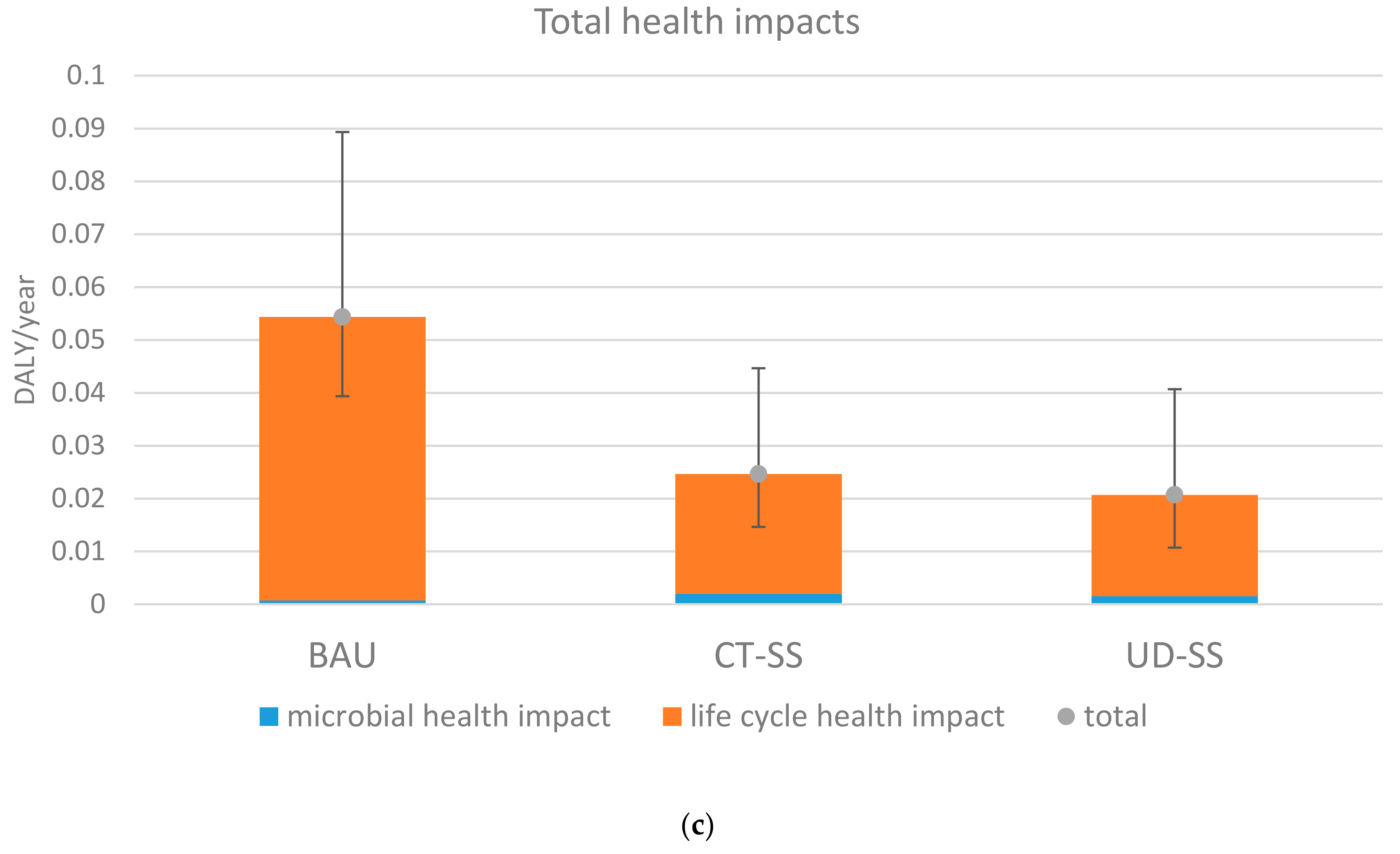
3.2. Relative Contributions of Life Cycle Health Impacts and Microbial Health Risks
3.3. Variability and Uncertainty Analyses
4. Discussion
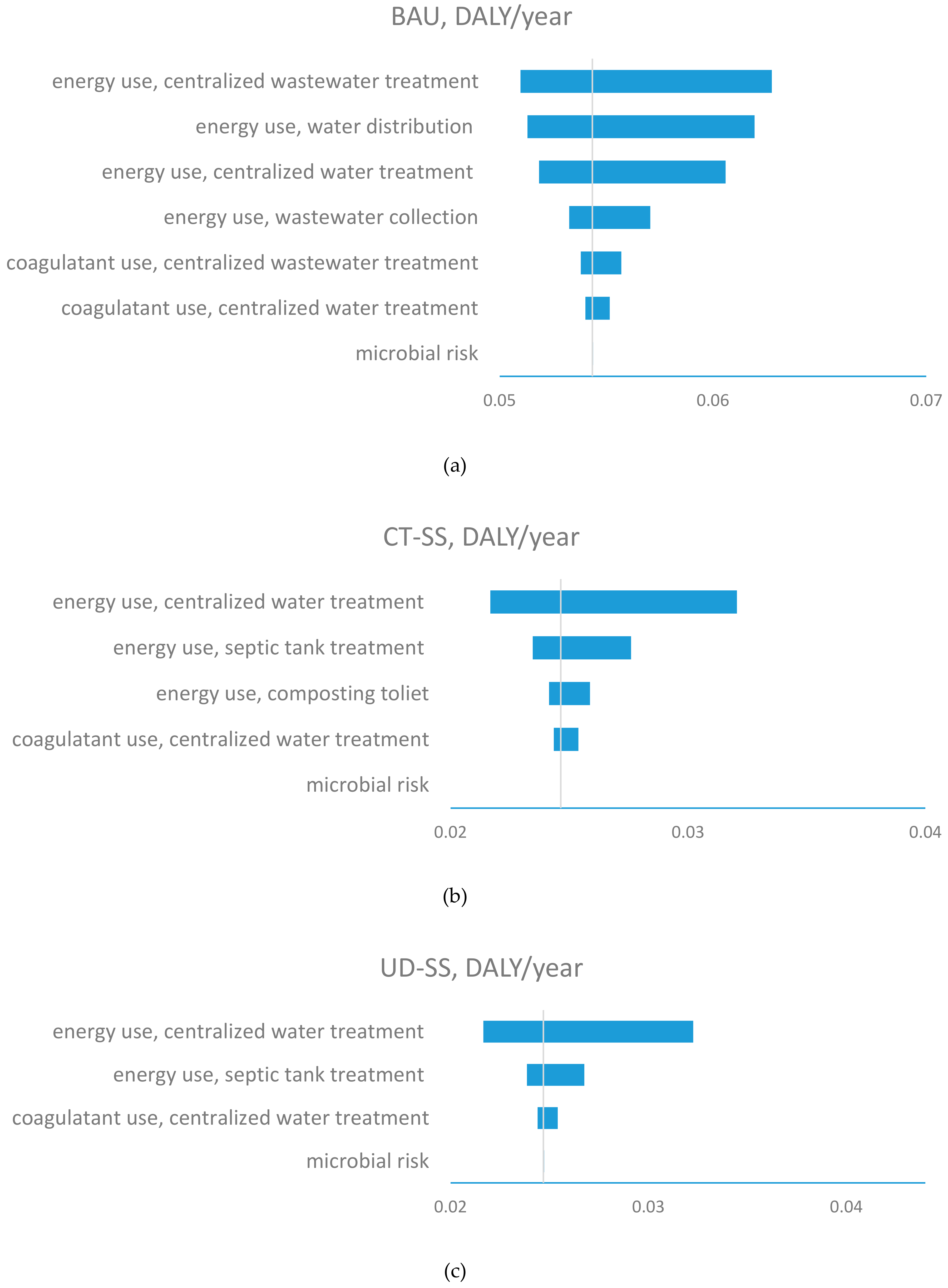
4.1. Sensitivity Assessment
4.2. Implications for Infrastructure Management and Policy Development
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Xue, X.; Cashman, S.; Gaglione, A.; Mosley, J.; Weiss, L.; Ma, X.; Cashdollar, J.; Garland, J. Holistic Analysis of Urban Water Systems in the Greater Cincinnati Region: (1) Life Cycle Assessment and Cost Implications. Water Res. 2019, 2, 100015. [Google Scholar] [CrossRef]
- Xue, X.; Hawkins, T.R.; Schoen, M.E.; Garland, J.; Ashbolt, N.J. Comparing the Life Cycle Energy Consumption, Global Warming and Eutrophication Potentials of Several Water and Waste Service Options. Water 2016, 8, 154. [Google Scholar] [CrossRef] [Green Version]
- Xue, X.; Schoen, M.E.; Ma, X.; Hawkins, T.R.; Ashbolt, N.J.; Cashdollar, J.; Garland, J. Critical insights for a sustainability framework to address integrated community water services: Technical metrics and approaches. Water Res. 2015, 77, 155–159. [Google Scholar] [CrossRef]
- Schoen, M.E.; Xue, X.; Wood, A.; Hawkins, T.R.; Garland, J.; Ashbolt, N.J. Cost, energy, global warming, eutrophication and local human health impacts of community water and sanitation service options. Water Res. 2017, 109, 186–195. [Google Scholar] [CrossRef] [PubMed]
- ISO 14040:2006. Environmental Management—Life Cycle Assessment—Principles and Framework. Available online: https://www.iso.org/standard/37456.html (accessed on 2 February 2020).
- Romeiko, X.X. Comprehensive water footprint assessment of conventional and four alternative resource recovery based wastewater service options. Resour. Conserv. Recycl. 2019, 151, 104458. [Google Scholar] [CrossRef]
- Cashman, S.; Gaglione, A.; Mosley, J.; Weiss, L.; Hawkins, T.R.; Ashbolt, N.J.; Cashdollar, J.; Xue, X.; Ma, X.; Arden, S. Environmental and Cost Life Cycle Assessment of Disinfection Options for Municipal Wastewater Treatment; Office of Research and Development, National Homeland Security Research Center: Cincinnati, OH, USA, 2014. [Google Scholar]
- Cashman, S.; Gaglione, A.; Mosley, J.; Weiss, L.; Hawkins, T.R.; Ashbolt, N.J.; Cashdollar, J.; Xue, X.; Ma, X.; Arden, S. Environmental and Cost Life Cycle Assessment of Disinfection Options for Municipal Drinking Water Treatment; Office of Research and Development, US Environmental Protection Agency: Cincinnati, OH, USA, 2014. [Google Scholar]
- Jeong, H.; Minne, E.; Crittenden, J.C. Life cycle assessment of the city of Atlanta, Georgia’s centralized water system. Int. J. Life Cycle Assess. 2015, 20, 880–891. [Google Scholar] [CrossRef]
- Lane, J.L.; de Haas, D.W.; Lant, P.A. The Diverse Environmental Burden of City-scale Urban Water Systems. Water Res. 2015, 81, 398–415. [Google Scholar] [CrossRef] [PubMed]
- Schoen, M.E.; Xue, X.; Hawkins, T.R.; Garland, J. Comparative human health risk analysis of coastal community water and waste service options. Environ. Sci. Technol. 2014, 48, 9728–9736. [Google Scholar] [CrossRef]
- Anastasopoulou, A.; Kolios, A.; Somorin, T.; Sowale, A.; Jiang, Y.; Fidalgo, B.; Parker, A.; Williams, L.; Collins, M.; McAdam, E.; et al. Conceptual environmental impact assessment of a novel self-sustained sanitation system incorporating a quantitative microbial risk assessment approach. Sci. Total Environ. 2018, 639, 657–672. [Google Scholar] [CrossRef]
- Harder, R.; Heimersson, S.; Svanström, M.; Peters, G.M. Including pathogen risk in life cycle assessment of wastewater management. 1. Estimating the burden of disease associated with pathogens. Environ. Sci. Technol. 2014, 48, 9438–9445. [Google Scholar] [CrossRef] [Green Version]
- Harder, R.; Peters, G.M.; Molander, S.; Ashbolt, N.J.; Svanström, M. Including pathogen risk in life cycle assessment: The effect of modelling choices in the context of sewage sludge management. Iint. J. Life Cycle Assess. 2016, 21, 60–69. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, Y.; Peters, G.M.; Ashbolt, N.J.; Heimersson, S.; Svanström, M.; Khan, S.J. Global and local health burden trade-off through the hybridisation of quantitative microbial risk assessment and life cycle assessment to aid water management. Water Res. 2015, 79, 26–38. [Google Scholar] [CrossRef] [PubMed]
- US Census Bureau. Population. Available online: https://www.census.gov/topics/population.html (accessed on 15 January 2020).
- Falmouth Department of Water. Water Treatment and Distribution. Available online: http://www.falmouthmass.us/depart.php?depkey=water (accessed on 2 February 2020).
- Brown, V.; Jackson, D.W.; Khalifé, M. 2009 Melbourne metropolitan sewerage strategy: A portfolio of decentralised and on-site concept designs. Water Sci. Technol. 2010, 62, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Wang, X.C. Cost-benefit evaluation of a decentralized water system for wastewater reuse and environmental protection. Water Sci. Technol. 2009, 59, 1515–1522. [Google Scholar] [CrossRef] [PubMed]
- Gikas, P.; Tchobanoglous, G. The role of satellite and decentralized strategies in water resources management. J. Environ. Manage. 2012, 2009, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Kinstedt, K. Optimization of the Collection and Transport of Blackwater in Source-Separated Wastewater Systems; Technical University Hamburg: Hamburg, Germany, 2012. [Google Scholar]
- Malisie, A.F.; Prihandrijanti, M.; Otterpohl, R. The potential of nutrient reuse from a source-separated domestic wastewater system in Indonesia—Case study: Ecological sanitation pilot plant in Surabaya. Water Sci. Technol. 2007, 56, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Otterpohl, R.; Braun, U.; Oldenburg, M. Innovative technologies for decentralised water-, wastewater and biowaste management in urban and peri-urban areas. Water Sci. Technol. 2003, 48, 23–32. [Google Scholar] [CrossRef]
- Peter-Fröhlich, A.; Pawlowski, L.; Bonhomme, A.; Oldenburg, M. EU demonstration project for separate discharge and treatment of urine, faeces and greywater—Part I: Results. Water Sci. Technol. 2007, 56, 239–249. [Google Scholar] [CrossRef]
- Sharma, A.; Burn, S.; Gardner, T.; Gregory, A. Role of decentralised systems in the transition of urban water systems. Water Sci. Technol. 2010, 10, 577. [Google Scholar] [CrossRef]
- Ishii, S.K.; Boyer, T.H. Life cycle comparison of centralized wastewater treatment and urine source separation with struvite precipitation: Focus on urine nutrient management. Water Res. 2015, 79, 88–103. [Google Scholar] [CrossRef]
- Tervahauta, T.; van der Weijden, R.D.; Flemming, R.L.; Hernández Leal, L.; Zeeman, G.; Buisman, C.J. Calcium phosphate granulation in anaerobic treatment of black water: A new approach to phosphorus recovery. Water Res. 2014, 48, 632–642. [Google Scholar] [CrossRef]
- Villarroel Walker, R.; Beck, M.B.; Hall, J.W.; Dawson, R.J.; Heidrich, O. The energy-water-food nexus: Strategic analysis of technologies for transforming the urban metabolism. J. Environ. Manage. 2014, 141, 104–115. [Google Scholar] [CrossRef] [PubMed]
- Loubet, P.; Roux, P.; Loiseau, E.; Bellon-Maurel, V. Life Cycle Assessment of Urban water Systems: A Comparative Analysis of Selected peer-Reviewed Literature. Water Res. 2014, 67, 187–202. [Google Scholar] [CrossRef] [PubMed]
- Cape Cod Water Protection Colloborative. Comparison of Costs for Wastewater Management Systems Applicable to Cape Cod. Available online: http://www.ccwpc.org/index.php/component/content/article/36-wastewater-reports/78-comparison-of-costs-for-wastewater-management-systems-applicable-to-cape-cod (accessed on 2 February 2020).
- US EPA. Indoor Water Use in the United States. Available online: http://www.epa.gov/WaterSense/pubs/indoor.html (accessed on 2 February 2020).
- US EPA. Water & Energy Efficiency. Available online: http://water.epa.gov/infrastructure/sustain/waterefficiency.cfm (accessed on 2 February 2020).
- U.S. Environmental Protection Agency. Evaluation of Energy Conservation Measures for Wastewater Treatment Facilities; U.S. Environmental Protection Agency: Washington, DC, USA, 2010. [Google Scholar]
- Memon, F.A.; Zheng, Z.; Bulter, D.; Shirley-Smith, C.; Lui, S.; Makropoulos, C.; Avery, L. Life Cycle Impact Assessment of Greywater Recycling Technologies for New Developments. Envion. Monit. Assess. 2007, 129, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Cape Cod Eco-Toilet Center. Urine-Diverting, Flush Toilet. Available online: http://capecodecotoiletcenter.com/types-of-eco-toilets/urine-diverting-toilets/ud-flush-toilets/ (accessed on 2 February 2020).
- Meinzinger, F.; Oldenburg, M. Characteristics of Source-separated Household Wastewater flows—A statistical assessment. Water Sci. Technol. 2009, 59, 1785–1791. [Google Scholar] [CrossRef] [PubMed]
- Resource Efficiency of Urban Sanitation Systems: A Comparative Assessment Using Material and Energy Flow Analysis. Available online: https://pdfs.semanticscholar.org/7dbb/7300a22ea727c4f23065e52a70a2ecef02f8.pdf (accessed on 2 February 2020).
- US EPA. NONROAD Model (Nonroad Engines, Equipment, and Vehicles). Available online: https://19january2017snapshot.epa.gov/moves/nonroad-model-nonroad-engines-equipment-and-vehicles_.html (accessed on 18 October 2016).
- The ecoinvent Organisation. The ecoinvent Database. Available online: https://www.ecoinvent.org/database/database.html (accessed on 2 February 2020).
- Green Delta. The openLCA Software. Available online: http://www.openlca.org/openlca/new/ (accessed on 2 February 2020).
- United States Goverment Accountability Office. Amount of Energy Needed to Supply, Use, and Treat Water is Location-Specific and can be Reduced by Certain Technologies and Approaches; United States Government Accountability Office: Washington, DC, USA, 2011; p. 10.
- Electric Power Research Institute. Water and Sustainability: U.S. Electricity Consumption for Water Supply & Treatment—TheNext Half Century; EPRI: Palo Alto, CA, USA, 2002. [Google Scholar]
- Schulz, M.; Short, M.D.; Peters, G.M. A streamlined sustainability assessment tool for improved decision making in the urban water industry. Integr. Environ. Assess. Manag. 2012, 8, 183–193. [Google Scholar] [CrossRef] [Green Version]
- Hallmann, M.; Grant, T.; Alsop, N. Life Cycle Assessment and Life Cycle Costing of Water Tanks as a Supplement to Mains Water Supply for Yarra Valley Water; Center for Design at RMIT University: Melbourne, Australia, 2003. [Google Scholar]
- Soller, J.A.; Schoen, M.E.; Bartrand, T.; Ravenscroft, J.E.; Ashbolt, N.J. Estimated human health risks from exposure to recreational waters impacted by human and non-human sources of faecal contamination. Water Res. 2010, 44, 4674–4691. [Google Scholar] [CrossRef]
- Gaulke, L.S.; Weiyang, X.; Scanlon, A.; Henck, A.; Hinckley, T. Evaluation criteria for implementation of a sustainable sanitation and wastewater treatment system at Jiuzhaigou National Park, Sichuan Province. China. Environ. Manag 2010, 45, 93–104. [Google Scholar] [CrossRef]
- Makaya, J.M.; Savadogo, A.; Somda, M.K.; Bour, J.; Barro, N.; Traoré, A.S. Quality of human urine used as fertilizer: Case of an ecological sanitation system in Ouagadougou peri-urban areas-Burkina Faso. J. Environ. Prot. 2014, 5, 464–474. [Google Scholar] [CrossRef] [Green Version]
- Dufour, A.P.; Evans, O.; Behymer, T.D.; Cantú, R. Water ingestion during swimming activities in a pool: A pilot study. J. Water Health 2006, 4, 425–430. [Google Scholar] [CrossRef] [Green Version]
- Charles, K.J. Quantitative Microbial Risk Assessment: A Catchment Management Tool to Delineate Buffer Distances for On-Site Sewage Treatment and Disposal Systems in Sydney’s Drinking Water Catchments; University of New South Wales: Sydney, New South Wales, Australia, 2009. [Google Scholar]
- Bales, R.C.; Li, S.; Maguire, K.M.; Yahya, M.T.; Gerba, C.P.; Harvey, R.W. Virus and bacteria transport in a sandy aquifer, Cape Cod, MA. Ground Water 1995, 33, 653–661. [Google Scholar] [CrossRef]
- US-EPA. Exposure Factors Handbook; Office of Research and Development, United States Environmental Protection Agency: Washington, DC, USA, 1997; Volume EPA/600/P-95/002Fa. [Google Scholar]
- Teunis, P.F.M.; Xu, M.; Fleming, K.K.; Yang, J.; Moe, C.L.; LeChevallier, M.W. Enteric Virus Infection Risk from Intrusion of Sewage into a Drinking Water Distribution Network. Environ. Sci. Technol. 2010, 44, 8561–8566. [Google Scholar] [CrossRef]
- Medema, G.J.; Teunis, P.F.M.; Havelaar, A.H.; Haas, C.N. Assessment of the dose-response relationship of Campylobacter jejuni. Int. J. Food Micro. 1996, 30, 101–111. [Google Scholar] [CrossRef]
- Teunis, P.F.M.; van der Hiejden, O.G.; van der Giessen, J.W.B.; Havelaar, A.H. The Dose-Response Relation in Human Volunteers for Gastro-Intestinal Pathogens; Rijksinstituut voor Volksgezondheid en Milieu RIVM: Bilthofen, The Netherlands, 1996. [Google Scholar]
- US-EPA. Economic Analysis for the Final Long Term 2 Enhanced Surface Water Treatment Rule. EPA 815-R-06-001; U.S. Environmental Protection Agency: Washington, DC, USA, 2005. [Google Scholar]
- Teunis, P.F.; Ogden, I.D.; Strachan, N.J. Hierarchical dose response of E. coli O157:H7 from human outbreaks incorporating heterogeneity in exposure. Epidemiol. Infect. 2008, 136, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Teunis, P.F.M.; Moe, C.L.; Liu, P.; Miller, S.E.; Lindesmith, L.; Baric, R.S.; Pendu, J.L.; Calderon, R.L. Norwalk virus: How infectious is it? J. Med. Virol. 2008, 80, 1468–1476. [Google Scholar] [CrossRef] [PubMed]
- Havelaar, A.H.; Melse, J.M. Quantifying Public Health Risk in the WHO Guidelines for Drinking-Water Quality, a Burden of Disease Approach, RIVM Report 734301022; RIVM: Bilthoven, The Netherlands, 2003; p. 49. [Google Scholar]
- Vijgen, S.; Mangen, M.; Kortbeek, L.; van Duijnhoven, Y.; Havelaar, A. Disease Burden and Related Costs of Cryptosporidiosis and Giardiasis in the Netherlands; RIVM: Bilthoven, The Netherlands, 2007. [Google Scholar]
- Havelaar, A.H.; van Duynhoven, Y.T.H.P.; Nauta, M.J.; Bouwknegt, M.; Heuvelink, A.E.; de Wit, G.A.; Nieuwenhuizen, M.G.M.; van de Kar, N.C.A. Disease Burden in the Netherlands due to Infections with Shiga-Toxin Producing Escherichia coli O157. RIVM Report 284550008; RIVM: Bilthoven, The Netherlands, 2003; p. 85. [Google Scholar]
- Howard, G.; Ahmed, M.F.; Teunis, P.; Mahmud, S.G.; Davison, A.; Deere, D. Disease burden estimation to support policy decision-making and research prioritization for arsenic mitigation. J. Water Health 2007, 5, 67–81. [Google Scholar] [CrossRef]
- Huijbregts, M.A.J.; Rombouts, L.J.A.; Ragas, A.M.J.; Meent, D.v.d. Human–Toxicological Effect and Damage Factors of Carcinogenic and Noncarcinogenic Chemicals for Life Cycle Impact Assessment. Integr. Environ. Assess. Manag. 2005, 1, 181–244. [Google Scholar] [CrossRef]
- Xue, X.; Hawkins, T.R.; Ingwersen, W.W.; Smith, R.L. Demonstrating an approach for including pesticide use in life-cycle assessment: Estimating human and ecosystem toxicity of pesticide use in Midwest corn farming. Int. J. Life Cycle Assess. 2015, 20, 1117–1126. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Input Parameter | Input Statistic | Range for the Sensitivity Analysis | References | |
|---|---|---|---|---|
| Distribution + | Low (5th Percentile) | High (95th Percentile) | ||
| Coagulant input of water treatment, kg·m−3 treated water | Triangular (0.016, 0.019, 0.028) | 0.017 | 0.026 | [1,41,42] |
| Energy use of water treatment, MJ·m−3 water | Normal (1.27, 0.43) | 0.56 | 1.98 | [1,41,42] |
| Energy use of water distribution, MJ·m−3 water | Normal (0.95, 0.41) | 0.28 | 1.62 | [1,41,42] |
| Energy use of wastewater collection for BAU, MJ·m−3 wastewater | Normal (0.47, 0.24) | 0.08 | 0.86 | [1,41,42] |
| Coagulant input of centralized wastewater treatment plant for BAU, kg·m−3 wastewater | Triangular (0.008, 0.010, 0.012) | 0.09 | 0.011 | [1,33] |
| Energy use of centralized wastewater treatment plant for BAU, MJ·m−3 wastewater | Normal (2.34, 0.6) | 1.35 | 3.33 | [1,41,42] |
| Energy use of septic treatment for CT-SS and UD-SS, MJ·m−3 wastewater | Normal (0.18,0.03) | 0.13 | 0.23 | [34,43,44] |
| Energy use of transporting compost for CT-SS, MJ·(household·year)−1 | Normal (440, 30) | 391 | 489 | [36,37] |
| Energy use of transporting urine for UD-SS, MJ·(household·year)−1 | Normal (1280, 100) | 1116 | 1445 | [36,37] |
| Reference Hazard | Dose-Response Model | Parameters | ID50 | Pill | Inf |
|---|---|---|---|---|
| Campylobacter jejuni | Beta-Poisson [53,54] | 0.145; 7.59 | 800 cfu | 0.33 |
| Cryptosporidium spp. | Exponential [55] | 0.09 | 8 oocysts | 0.71 |
| E. coli O157:H7 | Beta-Poisson [56] | 0.4, 45.9 | 207 cfu | 0.28 |
| Norovirus | Hypergeometric [57] | 0.04, 0.055 | 26 genome copies | 0.7 |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romeiko, X.X. Assessing Health Impacts of Conventional Centralized and Emerging Resource Recovery-Oriented Decentralized Water Systems. Int. J. Environ. Res. Public Health 2020, 17, 973. https://doi.org/10.3390/ijerph17030973
Romeiko XX. Assessing Health Impacts of Conventional Centralized and Emerging Resource Recovery-Oriented Decentralized Water Systems. International Journal of Environmental Research and Public Health. 2020; 17(3):973. https://doi.org/10.3390/ijerph17030973
Chicago/Turabian StyleRomeiko, Xiaobo Xue. 2020. "Assessing Health Impacts of Conventional Centralized and Emerging Resource Recovery-Oriented Decentralized Water Systems" International Journal of Environmental Research and Public Health 17, no. 3: 973. https://doi.org/10.3390/ijerph17030973