Anthropometric, Body Composition, and Morphological Lower Limb Asymmetries in Elite Soccer Players: A Prospective Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Subjects
2.3. Data Collection
2.4. Statistical Analysis
3. Results
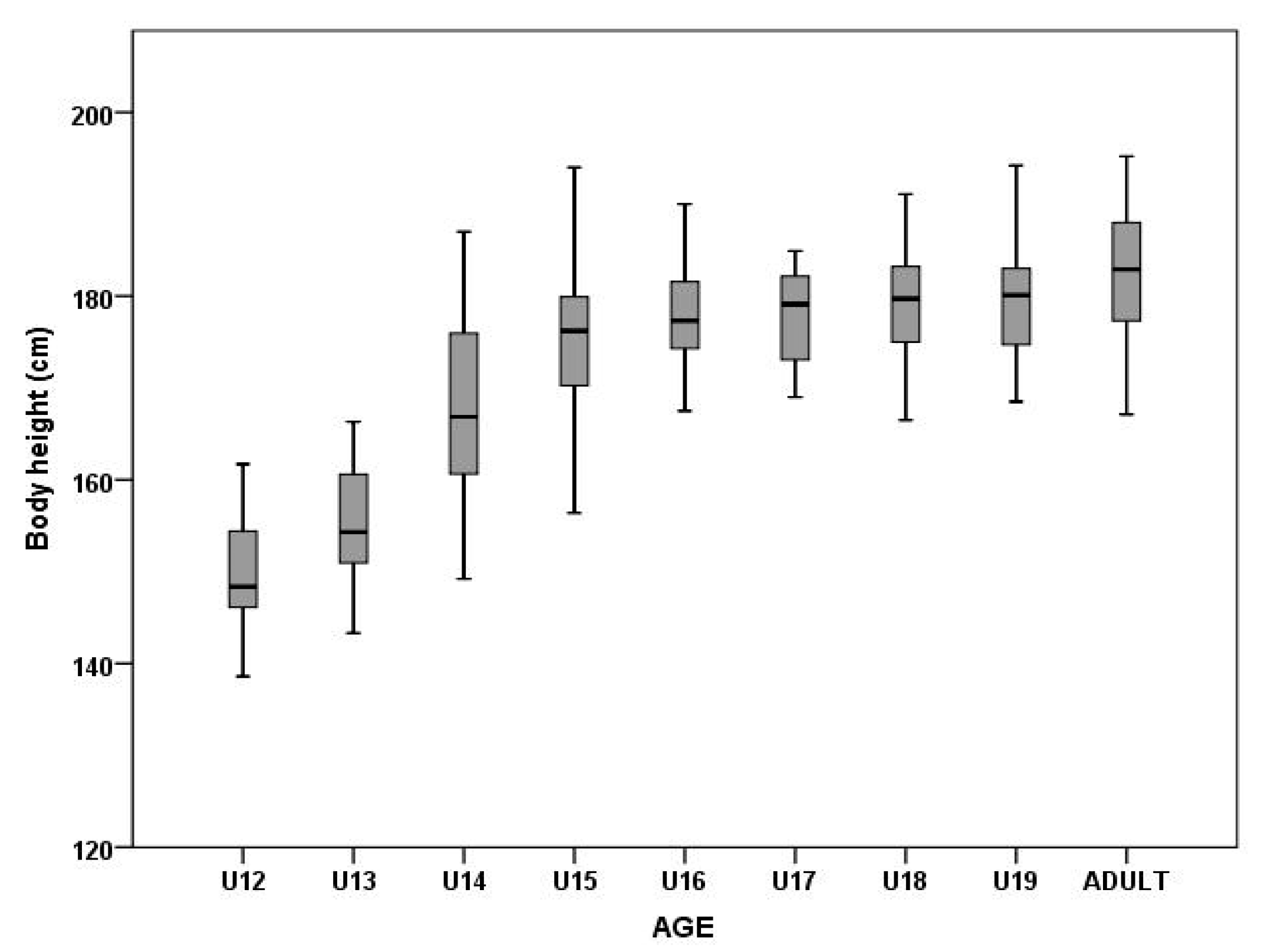
3.1. Body Height and Body Mass
3.2. Fat Mass and Fat-Free Mass
3.3. Segmental Comparison of Muscle Mass in Upper and Lower Extremities
4. Discussion
4.1. Anthropometric Parameters
4.2. Body composition
4.3. Segmental Comparison of Upper and Lower Extremity Muscle Mass
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mala, L.; Zahalka, F.; Maly, T. Bioimpedance for Analysis of Body Composition in Sports. In Bioimpedance in Biomedical Applications and Research; Springer: Cham, Switzerland, 2018; pp. 243–256. [Google Scholar] [CrossRef]
- Figueiredo, A.J.; Gonçalves, C.E.; Coelho, E.; Silva, M.J.; Malina, R.M. Youth soccer players, 11–14 years: Maturity, size, function, skill and goal orientation. Ann. Hum. Biol. 2009, 36, 60–73. [Google Scholar] [CrossRef] [Green Version]
- Leão, C.; Camões, M.; Clemente, F.M.; Nikolaidis, P.T.; Lima, R.; Bezerra, P.; Rosemann, T.; Knechtle, B. Anthropometric profile of soccer players as a determinant of position specificity and methodological issues of body composition estimation. Int. J. Environ. Res. Public Health 2019, 16, 2386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mala, L.; Maly, T.; Camilleri, R.; Dornowsk, M.; Zahalka, F.; Petr, M.; Hrasky, P.; Bujnovsky, D. Gender differences in strength lateral asymmetries, limbs morphology and body composition in adolescent judo athletes. Arch. Budo 2017, 13, 377–385. [Google Scholar]
- Milsom, J.; Naughton, R.; O’Boyle, A.; Iqbal, Z.; Morgans, R.; Drust, B. Body composition assessment of English Premier League soccer players: A comparative DXA analysis of first team, U21 and U18 squads. J. Sports Sci. 2015, 33, 1799–1806. [Google Scholar] [CrossRef] [PubMed]
- Carling, C.; Le Gall, F.; Reilly, T.; Williams, A.M. Do anthropometric and fitness characteristics vary according to birth date distribution in elite youth academy soccer players? Scand. J. Med. Sci. Sports 2009, 19, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M.; Mendez-Villanueva, A. Reliability and stability of anthropometric and performance measures in highly-trained young soccer players: Effect of age and maturation. J. Sports Sci. 2013, 31, 1332–1343. [Google Scholar] [CrossRef] [PubMed]
- Deprez, D.; Buchheit, M.; Fransen, J.; Pion, J.; Lenoir, M.; Philippaerts, R.M.; Vaeyens, R. A longitudinal study investigating the stability of anthropometry and soccer-specific endurance in pubertal high-level youth soccer players. J. Sport. Sci. Med. 2015, 14, 418. [Google Scholar]
- Bujnovsky, D.; Maly, T.; Ford, K.R.; Sugimoto, D.; Kunzmann, E.; Hank, M.; Zahalka, F. Physical Fitness Characteristics of High-level Youth Football Players: Influence of Playing Position. Sports 2019, 7, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ducher, G.; Courteix, D.; Meme, S.; Magni, C.; Viala, J.; Benhamou, C. Bone geometry in response to long-term tennis playing and its relationship with muscle volume: A quantitative magnetic resonance imaging study in tennis players. Bone 2005, 37, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Maly, T.; Mala, L.; Bujnovsky, D.; Hank, M.; Zahalka, F. Morphological and isokinetic strength differences: Bilateral and ipsilateral variation by different sport activity. Open Med. 2019, 14, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Maly, T.; Sugimoto, D.; Izovska, J.; Zahalka, F.; Mala, L. Effect of muscular strength, asymmetries and fatigue on kicking performance in soccer players. Int. J. Sports Med. 2018, 39, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Garrett, W.E.; Moorman, C.T.; Yu, B. Injury rate, mechanism, and risk factors of hamstring strain injuries in sports: A review of the literature. J. Sport Health Sci. 2012, 1, 92–101. [Google Scholar] [CrossRef] [Green Version]
- Fousekis, K.; Tsepis, E.; Vagenas, G. Lower limb strength in professional soccer players: Profile, asymmetry, and training age. J. Sports Sci. Med. 2010, 9, 364. [Google Scholar] [PubMed]
- Murphy, D.F.; Connolly, D.A.J.; Beynnon, B.D. Risk factors for lower extremity injury: A review of the literature. Br. J. Sports Med. 2003, 37, 13–29. [Google Scholar] [CrossRef] [Green Version]
- Croisier, J.L.; Ganteaume, S.; Binet, J.; Genty, M.; Ferret, J.M. Strength imbalances and prevention of hamstring injury in professional soccer players: A prospective study. Am. J. Sports Med. 2008, 36, 1469–1475. [Google Scholar] [CrossRef] [PubMed]
- Menzel, H.J.; Chagas, M.H.; Szmuchrowski, L.A.; Araujo, S.R.; de Andrade, A.G.; de Jesus-Moraleida, F.R. Analysis of lower limb asymmetries by isokinetic and vertical jump tests in soccer players. J. Strength Cond. Res. 2013, 27, 1370–1377. [Google Scholar] [CrossRef]
- Read, P.J.; Oliver, J.L.; Myer, G.D.; Croix, M.B.D.S.; Lloyd, R.S. The effects of maturation on measures of asymmetry during neuromuscular control tests in elite male youth soccer players. Pediatr. Exerc. Sci. 2018, 30, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Dittmar, M. Reliability and variability of bioimpedance measures in normal adults: Effects of age, gender, and body mass. Am. J. Phys. Anthropol. Am. J. Phys. Anthropol. 2003, 122, 361–370. [Google Scholar] [CrossRef]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M. Bioelectrical impedance analysis—Part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef]
- Gil, S.M.; Badiola, A.; Bidaurrazaga-Letona, I.; Zabala-Lili, J.; Gravina, L.; Santos-Concejero, J.; Lekue, J.A.; Granados, C. Relationship between the relative age effect and anthropometry, maturity and performance in young soccer players. J. Sports Sci. 2014, 32, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Stratton, G.; Reilly, T.; Williams, A.M.; Richardson, D. Youth Soccer: From Science to Performance; Routledge: London, UK, 2004. [Google Scholar] [CrossRef]
- Neyzi, O.; Bundak, R.; Gökçay, G.; Günöz, H.; Furman, A.; Darendeliler, F.; Baş, F. Reference values for weight, height, head circumference, and body mass index in Turkish children. J. Clin. Res. Pediatr. Endocrinol. 2015, 7, 280. [Google Scholar] [CrossRef]
- Júlíusson, P.B.; Roelants, M.; Nordal, E.; Furevik, L.; Eide, G.E.; Moster, D.; Bjerknes, R. Growth references for 0–19 year-old Norwegian children for length/height, weight, body mass index and head circumference. Ann. Hum. Biol. 2013, 40, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Malina, R.M.; Eisenmann, J.C.; Cumming, S.P.; Ribeiro, B.; Aroso, J. Maturity-associated variation in the growth and functional capacities of youth football (soccer) players 13–15 years. Eur. J. Appl. Physiol. 2004, 91, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Vaeyens, R.; Malina, R.M.; Janssens, M.; Van Renterghem, B.; Bourgois, J.; Vrijens, J.; Philippaerts, R.M. A multidisciplinary selection model for youth soccer: The Ghent Youth Soccer Project. Br. J. Sports Med. 2006, 40, 928–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, C.H.; Wheatley, C.M.; Behnia, M.; Johnson, B.D. The effect of aging on relationships between lean body mass and VO2max in rowers. PLoS ONE 2016, 11. [Google Scholar] [CrossRef] [Green Version]
- De Ste Croix, M.; Armstrong, N.; Welsman, J.; Sharpe, P. Longitudinal changes in isokinetic leg strength in 10-14-year-olds. Ann. Hum. Biol. 2002, 29, 50–62. [Google Scholar] [CrossRef]
- Degache, F.; Richard, R.; Edouard, P.; Oullion, R.; Calmels, P. The relationship between muscle strength and physiological age: A cross-sectional study in boys aged from 11 to 15. Ann. Phys. Rehabil. Med. 2010, 53, 180–188. [Google Scholar] [CrossRef] [Green Version]
- Reilly, T.; Bangsbo, J.; Franks, A. Anthropometric and physiological predispositions for elite soccer. J. Sports Sci. 2000, 18, 669–683. [Google Scholar] [CrossRef]
- Lloyd, R.S.; Oliver, J.L. The Youth Physical Development Model: A New Approach to Long-Term Athletic Development. Strength Cond. J. 2012, 34, 61–72. [Google Scholar] [CrossRef] [Green Version]
- Milanese, C.; Cavedon, V.; Corradini, G.; De Vita, F.; Zancanaro, C. Seasonal DXA-measured body composition changes in professional male soccer players. J. Sports Sci. 2015, 33, 1219–1228. [Google Scholar] [CrossRef]
- Perez-Gomez, J.; Olmedillas, H.; Delgado-Guerra, S.; Royo, I.A.; Vicente-Rodriguez, G.; Ortiz, R.A.; Calbet, J.A. Effects of weight lifting training combined with plyometric exercises on physical fitness, body composition, and knee extension velocity during kicking in football. Appl. Physiol. Nutr. Metab. 2008, 33, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Milsom, J.; Barreira, P.; Burgess, D.J.; Iqbal, Z.; Morton, J.P. Case study: Muscle atrophy and hypertrophy in a premier league soccer player during rehabilitation from ACL injury. Int. J. Sport Nutr. Exerc. Metab. 2014, 24, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Sedano, S.; Vaeyens, R.; Philippaerts, R.; Redondo, J.C.; Cuadrado, G. Anthropometric and anaerobic fitness profile of elite and non-elite female soccer players. J. Sport. Med. Phys. Fit. 2009, 49, 387. [Google Scholar]
- Simenko, J.; Ipavec, M.; Vodicar, J.; Rauter, S. Body symmetry/asymmetry in youth judokas in the under 73 kg category. Ido Mov. Cult. J. Martial Arts Anthropol. 2017, 17, 51–55. [Google Scholar] [CrossRef]
- Maly, T.; Zahalka, F.; Mala, L. Unilateral and Ipsilateral Strength Asymmetries in Elite Youth Soccer Players with Respect to Muscle Group and Limb Dominance. Int. J. Morphol. 2016, 34. [Google Scholar] [CrossRef] [Green Version]
- Tsolakis, C.; Bogdanis, G.; Vagenas, G. Anthropometric profile and limb asymmetries in young male and female fencers. J. Hum. Mov. Stud. 2006, 50, 201–215. [Google Scholar]
- Calbet, J.A.L.; Moysi, J.S.; Dorado, C.; Rodriguez, L.P. Bone mineral content and density in professional tennis players. Calcif. Tissue Int. 1998, 62, 491–496. [Google Scholar] [CrossRef]
- Sanchis-Moysi, J.; Idoate, F.; Olmedillas, H.; Guadalupe-Grau, A.; Alayon, S.; Carreras, A.; Calbet, J.A.L. The upper extremity of the professional tennis player: Muscle volumes, fiber-type distribution and muscle strength. Scand. J. Med. Sci. Sports 2010, 20, 524–534. [Google Scholar] [CrossRef]
- Sanchis-Moysi, J.; Serrano-Sánchez, J.A.; González-Henríquez, J.J.; Lopez-Calbet, J.A.; Dorado, C. Greater reduction in abdominal than in upper arms subcutaneous fat volume in 10-to 12-year-old tennis players: A volumetric MRI study. Front. Pediatr. 2019, 7, 345. [Google Scholar] [CrossRef] [Green Version]
- Sanchis-Moysi, J.; Idoate, F.; Izquierdo, M.; Calbet, J.A.; Dorado, C. Iliopsoas and gluteal muscles are asymmetric in tennis players but not in soccer players. PLoS ONE 2011, 6. [Google Scholar] [CrossRef] [Green Version]
- Malina, R.M.; Cumming, S.P.; Rogol, A.D.; Coelho-e-Silva, M.J.; Figueiredo, A.J.; Konarski, J.M.; Kozieł, S.M. Bio-banding in youth sports: Background, concept, and application. Sports Med. 2019, 49, 1671–1685. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Team | n | Age (years) | Field-BasedTraining | ResistanceTraining | Match |
|---|---|---|---|---|---|
| Adult | 69 | 23.1 ± 2.6 | 6–7 × (60–90 min) | 1 × 45 min | 2 × 45 min |
| U19 | 33 | 18.8 ± 0.6 | 5–6 × (60–90 min) | 1 × 45 min | 2 × 45 min |
| U18 | 41 | 17.6 ± 0.4 | 5–6 × (60–90 min) | 1 × 45 min | 2 × 45 min |
| U17 | 28 | 16.6 ± 0.5 | 5–6 × (60–90 min) | 1 × 30 min | 2 × 40 min |
| U16 | 71 | 15.6 ± 0.6 | 5–6 × (60–90 min) | 1 × 30 min | 2 × 40 min |
| U15 | 47 | 15.7 ± 0.3 | 5 × (60–90 min) | 2 × 35 min | |
| U14 | 32 | 13.7 ± 0.4 | 5 × (60–90 min) | 2 × 35 min | |
| U13 | 16 | 12.5 ± 0.6 | 4 × (60–120 min) | 3 × 30 min | |
| U12 | 18 | 11.8 ± 0.2 | 4 × (60–120 min) | 2 × 35 min |
| U12 | U13 | U14 | U15 | U16 | U17 | U18 | U19 | ADULT | |
|---|---|---|---|---|---|---|---|---|---|
| U12 | n.s. | U12 < U14 | U12 < U15 | U12 < U16 | U12 < U17 | U12 < U18 | U12 < U19 | U12 < AD | |
| U13 | n.s. | U13 < U14 | U13 < U15 | U13 < U16 | U13 < U17 | U13 < U18 | U13 < U19 | U13 < AD | |
| U14 | U12 < U14 | U13 < U14 | U14 < U15 | U14 < U16 | U14 < U17 | U14 < U18 | U14 < U19 | U14 < AD | |
| U15 | U12 < U15 | U13 < U15 | n.s. | n.s. | n.s. | n.s. | n.s. | U15 < AD | |
| U16 | U12 < U16 | U13 < U16 | U14 < U16 | U15 < 16 | n.s. | n.s. | n.s. | U16 < AD | |
| U17 | U12 < U17 | U13 < U17 | U14 < U17 | U15 < 17 | n.s. | n.s. | n.s. | n.s. | |
| U18 | U12 < U18 | U13 < U18 | U14 < U18 | U15 < 18 | n.s. | n.s. | n.s. | n.s. | |
| U19 | U12 < U19 | U13 < U19 | U14 < U19 | U15 < 19 | U16 < 19 | n.s. | n.s. | n.s. | |
| ADULT | U12 < AD | U13 < AD | U14 < AD | U15 < AD | U16 < AD | U17 < AD | U18 < AD | n.s. |
| U12 | U13 | U14 | U15 | U16 | U17 | U18 | U19 | ADULT | |
|---|---|---|---|---|---|---|---|---|---|
| U12 | n.s. | n.s. | n.s. | U12 > U16 | U12 > U17 | U12 > U18 | U12 > U19 | U12 > AD | |
| U13 | n.s. | U13 > U14 | n.s. | U13 > U16 | U13 > U17 | U13 > U18 | U13 > U19 | U13 > AD | |
| U14 | n.s. | U13 < U14 | n.s. | n.s. | n.s. | U14 > U18 | n.s. | n.s. | |
| U15 | n.s. | n.s. | n.s. | U15 > U16 | U15 > U17 | U15 > U18 | U15 > U19 | U15 > AD | |
| U16 | U12 < U16 | U13 < U16 | n.s. | U15 < 16 | n.s. | n.s. | n.s. | n.s. | |
| U17 | U12 < U17 | U13 < U17 | n.s. | U15 < 17 | n.s. | n.s. | n.s. | n.s. | |
| U18 | U12 < U18 | U13 < U18 | U14 < U18 | U15 < 18 | n.s. | n.s. | n.s. | n.s. | |
| U19 | U12 < U19 | U13 < U19 | n.s. | U15 < 19 | n.s. | n.s. | n.s. | n.s. | |
| ADULT | U12 < AD | U13 < AD | n.s. | U15 < AD | n.s. | n.s. | n.s. | n.s. |
| Compared variables | Type III Sum of Squares | Mean Square | F | Sig. | Partial Eta Squared |
|---|---|---|---|---|---|
| Muscle Mass PL (%) | 142.43 | 17.80 | 21.36 | 0.00 | 0.33 |
| Muscle Mass NL (%) | 206.98 | 25.87 | 38.93 | 0.00 | 0.47 |
| Age Category | Preferred Limb | Non-Preferred Limb | t | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| U12 | 13.79 | 0.76 | 13.61 | 0.83 | −0.91 |
| U13 | 14.02 | 1.33 | 13.89 | 1.35 | 0.02 |
| U14 | 14.61 | 1.16 | 14.49 | 1.13 | 0.37 |
| U15 | 14.90 | 1.02 | 14.71 | 1.00 | −0.38 |
| U16 | 15.07 | 0.85 | 14.55 | 0.79 | 1.37 |
| U17 | 15.26 | 0.89 | 14.73 | 0.83 | 2.77 * |
| U18 | 15.50 | 0.88 | 15.12 | 0.47 | −0.39 |
| U19 | 15.74 | 0.78 | 15.32 | 0.59 | 0.33 |
| Adults | 16.09 | 0.77 | 15.91 | 0.66 | 5.02 ** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mala, L.; Maly, T.; Cabell, L.; Hank, M.; Bujnovsky, D.; Zahalka, F. Anthropometric, Body Composition, and Morphological Lower Limb Asymmetries in Elite Soccer Players: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 1140. https://doi.org/10.3390/ijerph17041140
Mala L, Maly T, Cabell L, Hank M, Bujnovsky D, Zahalka F. Anthropometric, Body Composition, and Morphological Lower Limb Asymmetries in Elite Soccer Players: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(4):1140. https://doi.org/10.3390/ijerph17041140
Chicago/Turabian StyleMala, Lucia, Tomas Maly, Lee Cabell, Mikulas Hank, David Bujnovsky, and Frantisek Zahalka. 2020. "Anthropometric, Body Composition, and Morphological Lower Limb Asymmetries in Elite Soccer Players: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 17, no. 4: 1140. https://doi.org/10.3390/ijerph17041140