Comparison of Liquid Chromatography Mass Spectrometry and Enzyme-Linked Immunosorbent Assay Methods to Measure Salivary Cotinine Levels in Ill Children

 ,
, 
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects and Biological Samples
2.2. Measures
2.3. Chemical Analyses
2.4. Statistical Analyses
2.4.1. Mixed Model
2.4.2. Paired Sample t-Test
2.4.3. Linear Regression Models
3. Results
3.1. Demographics and TSE Patterns
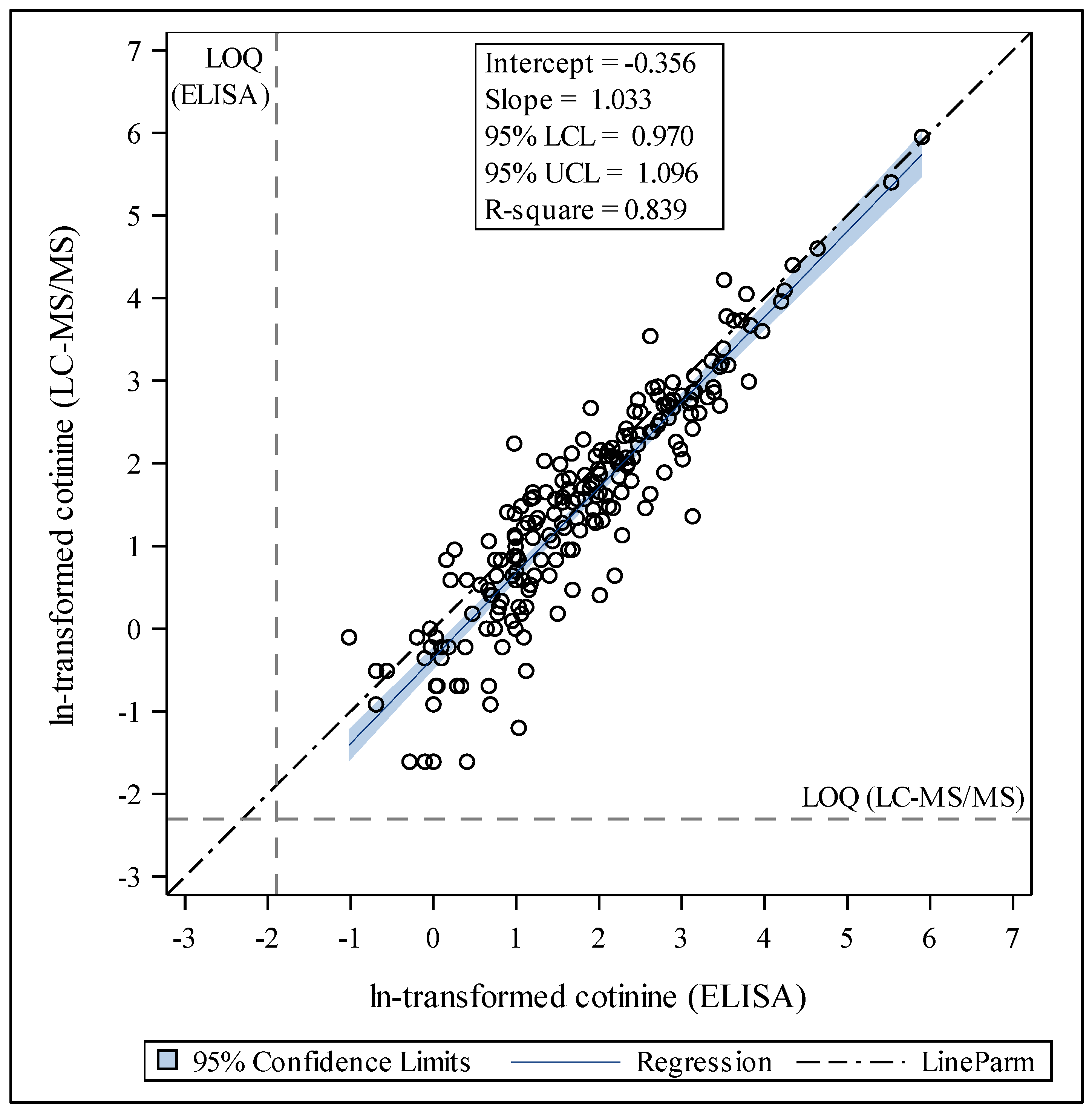
3.2. Cotinine Measurements and Comparisons of Analyses by LC-MS/MS and ELISA Distribution of Cotinine by LC-MS/MS Compared to ELISA
3.3. Internal Consistency of LC-MS/MS and ELISA
3.4. Differences in Cotinine Results by Demographics, TSE, and Home Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Avila-Tang, E.; Al-Delaimy, W.K.; Ashley, D.L.; Benowitz, N.; Bernert, J.T.; Kim, S.; Samet, J.M.; Hecht, S.S. Assessing secondhand smoke using biological markers. Tob. Control 2013, 22, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Torres, S.; Merino, C.; Paton, B.; Correig, X.; Ramirez, N. Biomarkers of Exposure to Secondhand and Thirdhand Tobacco Smoke: Recent Advances and Future Perspectives. Int. J. Environ. Res. Public Health 2018, 15, 2693. [Google Scholar] [CrossRef] [PubMed]
- Fang, S.C.; Chen, S.; Trachtenberg, F.; Rokicki, S.; Adamkiewicz, G.; Levy, D.E. Validity of Self-Reported Tobacco Smoke Exposure among Non-Smoking Adult Public Housing Residents. PLoS ONE 2016, 11, e0155024. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.M.; Cheng, Y.C.; Cho, T.M.; Mishina, E.V.; Del Valle-Pinero, A.Y.; van Bemmel, D.M.; Hatsukami, D.K. Biomarkers of Potential Harm: Summary of an FDA-Sponsored Public Workshop. Nicotine Tob. Res. 2019, 21, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.M.; Edwards, S.H.; Arab, A.; Del Valle-Pinero, A.Y.; Yang, L.; Hatsukami, D.K. Biomarkers of Tobacco Exposure: Summary of an FDA-Sponsored Public Workshop. Cancer Epidemiol. Biomarkers Prev. 2017, 26, 291–302. [Google Scholar] [CrossRef]
- Benowitz, N.L.; Bernert, J.T.; Foulds, J.; Hecht, S.S.; Jacob, P.; Jarvis, M.J.; Joseph, A.; Oncken, C.; Piper, M.E. Biochemical Verification of Tobacco Use and Abstinence: 2019 Update. Nicotine Tob. Res. 2019. [Google Scholar] [CrossRef]
- Jacob, P., 3rd; Benowitz, N.L.; Destaillats, H.; Gundel, L.; Hang, B.; Martins-Green, M.; Matt, G.E.; Quintana, P.J.; Samet, J.M.; Schick, S.F.; et al. Thirdhand Smoke: New Evidence, Challenges, and Future Directions. Chem. Res. Toxicol. 2017, 30, 270–294. [Google Scholar] [CrossRef]
- Benowitz, N.L.; Hukkanen, J.; Jacob, P., 3rd. Nicotine chemistry, metabolism, kinetics and biomarkers. Handb. Exp. Pharmacol. 2009, 192, 29–60. [Google Scholar] [CrossRef]
- Benowitz, N.L. Cotinine as a biomarker of environmental tobacco smoke exposure. Epidemiol. Rev. 1996, 18, 188–204. [Google Scholar] [CrossRef]
- Leong, J.W.; Dore, N.D.; Shelley, K.; Holt, E.J.; Laing, I.A.; Palmer, L.J.; LeSouef, P.N. The elimination half-life of urinary cotinine in children of tobacco-smoking mothers. Pulm. Pharmacol. Ther. 1998, 11, 287–290. [Google Scholar] [CrossRef]
- Dempsey, D.A.; Sambol, N.C.; Jacob, P., 3rd; Hoffmann, E.; Tyndale, R.F.; Fuentes-Afflick, E.; Benowitz, N.L. CYP2A6 genotype but not age determines cotinine half-life in infants and children. Clin. Pharmacol. Ther. 2013, 94, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, A.; Ino, T.; Ohta, M.; Otani, T.; Hanada, S.; Sakuraoka, A.; Matsumoto, A.; Ichiba, M.; Hara, M. Enzyme-linked immunosorbent assay of nicotine metabolites. Environ. Health Prev. Med. 2010, 15, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Irvine, L.; Crombie, I.K.; Clark, R.A.; Slane, P.W.; Feyerabend, C.; Goodman, K.E.; Cater, J.I. Advising parents of asthmatic children on passive smoking: Randomised controlled trial. BMJ 1999, 318, 1456–1459. [Google Scholar] [CrossRef] [PubMed]
- Behbod, B.; Sharma, M.; Baxi, R.; Roseby, R.; Webster, P. Family and carer smoking control programmes for reducing children’s exposure to environmental tobacco smoke. Cochrane Database Syst. Rev. 2018, 1, CD001746. [Google Scholar] [CrossRef] [PubMed]
- Collins, B.N.; Nair, U.S.; Hovell, M.F.; DiSantis, K.I.; Jaffe, K.; Tolley, N.M.; Wileyto, E.P.; Audrain-McGovern, J. Reducing Underserved Children’s Exposure to Tobacco Smoke: A Randomized Counseling Trial With Maternal Smokers. Am. J. Prev. Med. 2015, 49, 534–544. [Google Scholar] [CrossRef]
- Lepore, S.J.; Collins, B.N.; Coffman, D.L.; Winickoff, J.P.; Nair, U.S.; Moughan, B.; Bryant-Stephens, T.; Taylor, D.; Fleece, D.; Godfrey, M. Kids Safe and Smokefree (KiSS) Multilevel Intervention to Reduce Child Tobacco Smoke Exposure: Long-Term Results of a Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2018, 15, 1239. [Google Scholar] [CrossRef]
- Blaakman, S.W.; Borrelli, B.; Wiesenthal, E.N.; Fagnano, M.; Tremblay, P.J.; Stevens, T.P.; Halterman, J.S. Secondhand Smoke Exposure Reduction After NICU Discharge: Results of a Randomized Trial. Acad. Pediatr. 2015, 15, 605–612. [Google Scholar] [CrossRef]
- Halterman, J.S.; Szilagyi, P.G.; Fisher, S.G.; Fagnano, M.; Tremblay, P.; Conn, K.M.; Wang, H.; Borrelli, B. Randomized controlled trial to improve care for urban children with asthma: Results of the School-Based Asthma Therapy trial. Arch. Pediatr. Adolesc. Med. 2011, 165, 262–268. [Google Scholar] [CrossRef]
- Schoedel, K.A.; Hoffmann, E.B.; Rao, Y.; Sellers, E.M.; Tyndale, R.F. Ethnic variation in CYP2A6 and association of genetically slow nicotine metabolism and smoking in adult Caucasians. Pharmacogenetics 2004, 14, 615–626. [Google Scholar] [CrossRef]
- Matt, G.E.; Quintana, P.J.; Liles, S.; Hovell, M.F.; Zakarian, J.M.; Jacob, P., 3rd; Benowitz, N.L. Evaluation of urinary trans-3’-hydroxycotinine as a biomarker of children’s environmental tobacco smoke exposure. Biomarkers 2006, 11, 507–523. [Google Scholar] [CrossRef]
- Hukkanen, J.; Jacob, P., 3rd; Benowitz, N.L. Metabolism and disposition kinetics of nicotine. Pharmacol. Rev. 2005, 57, 79–115. [Google Scholar] [CrossRef]
- Matt, G.E.; Quintana, P.J.; Hovell, M.F.; Bernert, J.T.; Song, S.; Novianti, N.; Juarez, T.; Floro, J.; Gehrman, C.; Garcia, M.; et al. Households contaminated by environmental tobacco smoke: Sources of infant exposures. Tob. Control 2004, 13, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Matt, G.E.; Quintana, P.J.; Destaillats, H.; Gundel, L.A.; Sleiman, M.; Singer, B.C.; Jacob, P.; Benowitz, N.; Winickoff, J.P.; Rehan, V.; et al. Thirdhand tobacco smoke: Emerging evidence and arguments for a multidisciplinary research agenda. Environ. Health Perspect. 2011, 119, 1218–1226. [Google Scholar] [CrossRef] [PubMed]
- Mahabee-Gittens, E.M.; Merianos, A.L.; Hoh, E.; Quintana, P.J.; Matt, G.E. Nicotine on Children’s Hands: Limited Protection of Smoking Bans and Initial Clinical Findings. Tob. Use Insights 2019, 12. [Google Scholar] [CrossRef] [PubMed]
- Mahabee-Gittens, E.M.; Merianos, A.L.; Matt, G.E. Preliminary evidence that high levels of nicotine on children’s hands may contribute to overall tobacco smoke exposure. Tob. Control 2018, 27, 217–219. [Google Scholar] [CrossRef] [PubMed]
- Matt, G.E.; Quintana, P.J.; Zakarian, J.M.; Fortmann, A.L.; Chatfield, D.A.; Hoh, E.; Uribe, A.M.; Hovell, M.F. When smokers move out and non-smokers move in: Residential thirdhand smoke pollution and exposure. Tob. Control 2011, 20, e1. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, D.A.; Meyers, M.J.; Oh, S.S.; Nguyen, E.A.; Fuentes-Afflick, E.; Wu, A.H.; Jacob, P.; Benowitz, N.L. Determination of tobacco smoke exposure by plasma cotinine levels in infants and children attending urban public hospital clinics. Arch. Pediatr. Adolesc. Med. 2012, 166, 851–856. [Google Scholar] [CrossRef]
- Kalkbrenner, A.E.; Hornung, R.W.; Bernert, J.T.; Hammond, S.K.; Braun, J.M.; Lanphear, B.P. Determinants of serum cotinine and hair cotinine as biomarkers of childhood secondhand smoke exposure. J. Expo. Sci. Environ. Epidemiol. 2010, 20, 615–624. [Google Scholar] [CrossRef]
- Benowitz, N.L.; Perez-Stable, E.J.; Fong, I.; Modin, G.; Herrera, B.; Jacob, P., 3rd. Ethnic differences in N-glucuronidation of nicotine and cotinine. J. Pharmacol. Exp. Ther. 1999, 291, 1196–1203. [Google Scholar]
- Wilson, S.E.; Kahn, R.S.; Khoury, J.; Lanphear, B.P. Racial differences in exposure to environmental tobacco smoke among children. Environ. Health Perspect. 2005, 113, 362–367. [Google Scholar] [CrossRef]
- Mahabee-Gittens, E.M.; Gordon, J.S.; Krugh, M.E.; Henry, B.; Leonard, A.C. A smoking cessation intervention plus proactive quitline referral in the pediatric emergency department: A pilot study. Nicotine Tob. Res. 2008, 10, 1745–1751. [Google Scholar] [CrossRef] [PubMed]
- High Sensitivity Salivary Cotinine Quantitative Enzyme Immunoassay Kit; Salimetrics, LLC: State College, PA, USA, 2015.
- Murphy, S.E.; Wickham, K.M.; Lindgren, B.R.; Spector, L.G.; Joseph, A. Cotinine and trans 3’-hydroxycotinine in dried blood spots as biomarkers of tobacco exposure and nicotine metabolism. J. Expo. Sci. Environ. Epidemiol. 2013, 23, 513–518. [Google Scholar] [CrossRef]
- Data Quality Assessment and Data Usability Evaluation Technical Guidance; New Jersey Department of Environmental Protection: Trenton, NJ, USA, 2014; pp. 1–132.
- Mahabee-Gittens, E.M.; Merianos, A.L.; Gordon, J.S.; Stone, L.; Semenova, O.; Matt, G.E. Electronic Health Record Classification of Tobacco Smoke Exposure and Cotinine Levels in Hospitalized Pediatric Patients. Hosp. Pediatr. 2019, 9, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Merianos, A.L.; Jandarov, R.A.; Choi, K.; Mahabee-Gittens, E.M. Tobacco smoke exposure disparities persist in U.S. children: NHANES 1999–2014. Prev. Med. 2019, 123, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Mahabee-Gittens, E.M.; Merianos, A.L.; Stone, L.; Tabangin, M.E.; Khoury, J.C.; Gordon, J.S. Tobacco Use Behaviors and Perceptions of Parental Smokers in the Emergency Department Setting. Tob. Use Insights 2019, 12, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Shenassa, E.D.; Rossen, L.M.; Cohen, J.; Morello-Frosch, R.; Payne-Sturges, D.C. Income Inequality and US Children’s Secondhand Smoke Exposure: Distinct Associations by Race-Ethnicity. Nicotine Tob. Res. 2017, 19, 1292–1299. [Google Scholar] [CrossRef]
- Tsai, J.; Homa, D.M.; Gentzke, A.S.; Mahoney, M.; Sharapova, S.R.; Sosnoff, C.S.; Caron, K.T.; Wang, L.; Melstrom, P.C.; Trivers, K.F. Exposure to Secondhand Smoke Among Nonsmokers—United States, 1988–2014. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 1342–1346. [Google Scholar] [CrossRef]
- Howrylak, J.A.; Spanier, A.J.; Huang, B.; Peake, R.W.; Kellogg, M.D.; Sauers, H.; Kahn, R.S. Cotinine in children admitted for asthma and readmission. Pediatrics 2014, 133, e355–e362. [Google Scholar] [CrossRef]
- Murphy, S.E. Nicotine Metabolism and Smoking: Ethnic Differences in the Role of P450 2A6. Chem. Res. Toxicol. 2017, 30, 410–419. [Google Scholar] [CrossRef]
- Parzynski, C.S.; Jaszyna-Gasior, M.; Franken, F.H.; Moolchan, E.T. Measuring nicotine intake among highly-dependent adolescent smokers: Comparability of saliva and plasma cotinine concentrations. Pharmacol. Biochem. Behav. 2008, 89, 145–149. [Google Scholar] [CrossRef][Green Version]
- Jarvis, M.J.; Primatesta, P.; Erens, B.; Feyerabend, C.; Bryant, A. Measuring nicotine intake in population surveys: Comparability of saliva cotinine and plasma cotinine estimates. Nicotine Tob. Res. 2003, 5, 349–355. [Google Scholar] [CrossRef] [PubMed]
- SRNT Subcommittee on Biochemical Verification, Biochemical verification of tobacco use and cessation. Nicotine Tob. Res. 2002, 4, 149–159. [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Analyte | Method | Total Samples Analyzed | Total Samples Detected | Percent Detected | LOQ | GeoM | Geometric SD | Min | P25 | P50 | P75 | P95 | Max |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cotinine (ng/mL) | LC-MS/MS | 218 | 211 | 97% | 0.10 | 4.1 | 4.1 | <LOQ | 1.3 | 4.3 | 10.3 | 41.5 | 382 |
| ELISA | 218 | 208 | 95% | 0.15 | 5.7 | 3.5 | <LOQ | 2.2 | 5.1 | 12.2 | 41.2 | 364 |
| Internal ELISA (N = 55) | Internal LC-MS/MS (N = 20) | |||||
|---|---|---|---|---|---|---|
| Across methods (N = 203) | ICC | Median RPD * | ICC | Median RPD | ||
| Overall | 0.884 | 0.993 | 0.113 | 0.991 | 0.061 | |
| Age | 0–6 yrs (n = 122) | 0.899 | 0.992 | 0.118 | 0.996 | 0.057 |
| 7–17 yrs (n = 81) | 0.824 | 0.994 | 0.099 | 0.983 | 0.073 | |
| Sex | Male (n = 100) | 0.890 | 0.993 | 0.087 | 0.995 | 0.056 |
| Female (n = 103) | 0.869 | 0.993 | 0.156 | 0.985 | 0.073 | |
| LC-MS/MS Based Cotinine | ELISA Based Cotinine | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Parameter | % of Cohort | 95% LCL | 95% UCL | p-Value | 95% LCL | 95% UCL | p-Value | ||
| Age of child | N/A | −0.11 | −0.15 | −0.08 | < 0.0001 | −0.09 | −0.13 | −0.06 | < 0.0001 |
| # cigarettes/day smoked-caregiver | N/A | 0.09 | 0.05 | 0.12 | < 0.0001 | 0.07 | 0.04 | 0.11 | < 0.0001 |
| # cigarettes/day smoked around child | N/A | 0.01 | −0.00 | 0.02 | 0.17 | 0.01 | −0.01 | 0.02 | 0.34 |
| Sex of child | |||||||||
| Female | 51.3% | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Male | 48.7% | 0.38 | 0.02 | 0.75 | 0.04 | 0.30 | −0.06 | 0.65 | 0.10 |
| Race/ethnicity | |||||||||
| Non-Hispanic White | 36.6% | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Non-Hispanic Black | 54.3% | 0.52 | 0.10 | 0.95 | 0.04 | 0.38 | −0.03 | 0.80 | 0.16 |
| Other | 9.1% | 0.07 | −0.61 | 0.75 | 0.04 | 0.06 | −0.61 | 0.73 | 0.16 |
| Caregiver’s Annual Income | |||||||||
| Less than $5,000 | 35.5% | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| $5,001 to $15,000 | 26.9% | 0.10 | −0.35 | 0.55 | 0.01 | 0.04 | −0.40 | 0.47 | 0.02 |
| $15,001 to $30,000 | 21.3% | −0.44 | −0.93 | 0.05 | 0.01 | −0.49 | −0.97 | −0.01 | 0.02 |
| $30,001 to $50,000 | 9.1% | −1.07 | −1.74 | −0.41 | 0.01 | −0.91 | −1.56 | −0.27 | 0.02 |
| $50,001 to $75,000 | 5.6% | −0.48 | −1.29 | 0.34 | 0.01 | −0.43 | −1.23 | 0.36 | 0.02 |
| More than $75,000 | 1.5% | −0.98 | −2.50 | 0.55 | 0.01 | −1.55 | −3.04 | −0.06 | 0.02 |
| Type of home | |||||||||
| Single family house | 48.2% | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Multi-family house | 20.3% | 0.49 | 0.02 | 0.96 | 0.06 | 0.22 | −0.24 | 0.68 | 0.19 |
| Apartment | 30.0% | 0.53 | 0.10 | 0.97 | 0.06 | 0.45 | 0.02 | 0.87 | 0.19 |
| Other | 1.5% | 0.66 | −0.82 | 2.14 | 0.06 | −0.37 | −1.81 | 1.08 | 0.19 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahabee-Gittens, E.M.; Mazzella, M.J.; Doucette, J.T.; Merianos, A.L.; Stone, L.; Wullenweber, C.A.; A. Busgang, S.; Matt, G.E. Comparison of Liquid Chromatography Mass Spectrometry and Enzyme-Linked Immunosorbent Assay Methods to Measure Salivary Cotinine Levels in Ill Children. Int. J. Environ. Res. Public Health 2020, 17, 1157. https://doi.org/10.3390/ijerph17041157
Mahabee-Gittens EM, Mazzella MJ, Doucette JT, Merianos AL, Stone L, Wullenweber CA, A. Busgang S, Matt GE. Comparison of Liquid Chromatography Mass Spectrometry and Enzyme-Linked Immunosorbent Assay Methods to Measure Salivary Cotinine Levels in Ill Children. International Journal of Environmental Research and Public Health. 2020; 17(4):1157. https://doi.org/10.3390/ijerph17041157
Chicago/Turabian StyleMahabee-Gittens, E. Melinda, Matthew J. Mazzella, John T. Doucette, Ashley L. Merianos, Lara Stone, Chase A. Wullenweber, Stefanie A. Busgang, and Georg E. Matt. 2020. "Comparison of Liquid Chromatography Mass Spectrometry and Enzyme-Linked Immunosorbent Assay Methods to Measure Salivary Cotinine Levels in Ill Children" International Journal of Environmental Research and Public Health 17, no. 4: 1157. https://doi.org/10.3390/ijerph17041157
APA StyleMahabee-Gittens, E. M., Mazzella, M. J., Doucette, J. T., Merianos, A. L., Stone, L., Wullenweber, C. A., A. Busgang, S., & Matt, G. E. (2020). Comparison of Liquid Chromatography Mass Spectrometry and Enzyme-Linked Immunosorbent Assay Methods to Measure Salivary Cotinine Levels in Ill Children. International Journal of Environmental Research and Public Health, 17(4), 1157. https://doi.org/10.3390/ijerph17041157