Personality, Behavior Characteristics, and Life Quality Impact of Children with Dyslexia



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Instruments
2.3. Statistical Methods
3. Results
3.1. General Characteristics of the Participated Children
3.2. Family Environment, Parenting Education and Children’s Dyslexia
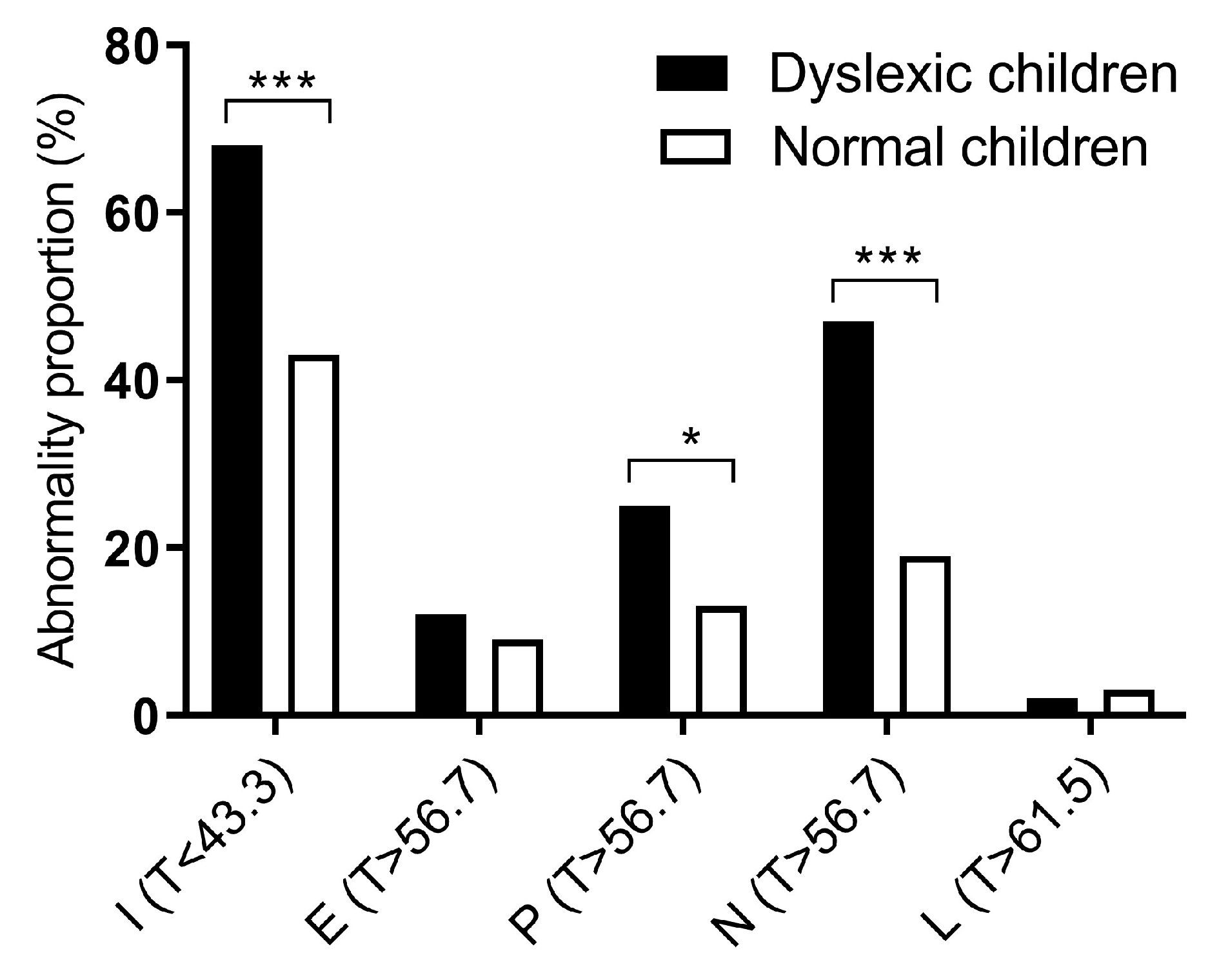
3.3. Personality Characteristics of Children with Dyslexia
3.4. Behavioral Characteristics of Children with Dyslexia
3.5. Life Quality of Children with Dyslexia
4. Discussion
4.1. Family Environment, Parenting Factors and Dyslexia
4.2. Children with Dyslexia and Their Personality and Behavior Characteristics
4.3. Children with Dyslexia and Their Life Quality
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- APA. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Goswami, U.; Wang, H.L.; Cruz, A.; Fosker, T.; Mead, N.; Huss, M. Language-universal sensory deficits in developmental dyslexia: English, Spanish, and Chinese. J. Cogn. Neurosci. 2011, 23, 325–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habib, M.; Giraud, K. Dyslexia. Handb. Clin. Neurol. 2012, 111, 229–235. [Google Scholar]
- Cai, L.; Chen, Y.; Hu, X.; Guo, Y.; Zhao, X.; Sun, T.; Wu, Y.; Li, X. An Epidemiological Study on the Children with Chinese Developmental Dyslexia. J. Dev. Behav. Pediatrics JDBP 2019. [Google Scholar] [CrossRef] [PubMed]
- Pennington, B.F. From single to multiple deficit models of developmental disorders. Cognition 2006, 101, 385–413. [Google Scholar] [CrossRef]
- Rüsseler, J.; Ye, Z.; Gerth, I.; Szycik, G.R.; Münte, T.F. Audio-visual speech perception in adult readers with dyslexia: An fMRI study. Brain Imaging Behav. 2018, 12, 357–368. [Google Scholar] [CrossRef]
- Wallace, M.T.; Stevenson, R.A. The construct of the multisensory temporal binding window and its dysregulation in developmental disabilities. Neuropsychologia 2014, 64, 105–123. [Google Scholar] [CrossRef] [Green Version]
- Marchandkrynski, M.; Bélanger, A.M.; Morinmoncet, O.; Beauchamp, M.H.; Leonard, G. Cognitive predictors of sequential motor impairments in children with dyslexia and/or attention deficit/hyperactivity disorder. Dev. Neuropsychol. 2018, 43, 430–453. [Google Scholar] [CrossRef]
- Mammarella, I.C.; Chiara, M.; Francesca, P.; Filippo, G.; Claudia, G.; Cesare, C. Representation of survey and route spatial descriptions in children with nonverbal (visuospatial) learning disabilities. Brain Cogn. 2009, 71, 173–179. [Google Scholar] [CrossRef]
- Rodriguez, E.T.; Tamis-LeMonda, C.S. Trajectories of the home learning environment across the first 5 years: Associations with children’s vocabulary and literacy skills at prekindergarten. Child Dev. 2011, 82, 1058–1075. [Google Scholar] [CrossRef]
- Karande, S.; Bhosrekar, K.M. Health-related quality of life of children with newly diagnosed specific learning disability. J. Trop. Pediatrics 2009, 55, 160–169. [Google Scholar] [CrossRef] [Green Version]
- Karande, S.; Venkataraman, R. Self-perceived health-related quality of life of Indian children with specific learning disability. J. Postgrad. Med. 2012, 58, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Smolik, F.; Málková, G. Validity of language sample measures taken from structured elicitation procedures in Czech. Ceskoslovenská Psychol. 2011, 55, 451–461. [Google Scholar]
- Furnes, B.; Samuelsson, S. Phonological awareness and rapid automatized naming predicting early development in reading and spelling: Results from a cross-linguistic longitudinal study. Learn. Individ. Differ. 2011, 21, 85–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Einat, T.; Einat, A. Learning disabilities and delinquency: A study of Israeli prison inmates. Int. J. Offender Ther. Comp. Criminol. 2008, 52, 416–434. [Google Scholar] [CrossRef] [PubMed]
- Kumagami, T.; Kumagai, K. Measuring adjustment in Japanese juvenile delinquents with learning disabilities using Japanese version of Kaufman Assessment Battery for Children II. Psychiatry Clin. Neurosci. 2014, 68, 768–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karande, S.; Venkataraman, R. Impact of co-morbid attention-deficit/hyperactivity disorder on self-perceived health-related quality-of-life of children with specific learning disability. Indian J. Psychiatry 2013, 55, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Tam, I.O.L.; Leung, C. Evaluation of the effectiveness of a literacy intervention programme on enhancing learning outcomes for secondary students with dyslexia in Hong Kong. Dyslexia 2019, 25, 296–317. [Google Scholar] [CrossRef]
- Tilanus, E.A.T.; Segers, E.; Verhoeven, L. Predicting responsiveness to a sustained reading and spelling intervention in children with dyslexia. Dyslexia 2019, 25, 190–206. [Google Scholar] [CrossRef]
- Huang, Y.; Xu, C.; He, M.; Huang, W.; Wu, K. Saliva cortisol, melatonin levels and circadian rhythm alterations in Chinese primary school children with dyslexia. Medicine 2020, 99, e19098. [Google Scholar] [CrossRef]
- Gong, Y. Eysenck Personality Questionnaire; Hunan Medical College: Changsha, China, 1986. [Google Scholar]
- Chen, L.; Wu, H.; Mai, J. Comparison of Quality of Life among Primary and Secondary School Students between Urban and Rural in Beijing and Guangzhou. Chin. J. Soc. Med. 2007, 24, 268–270. [Google Scholar]
- Zhang, Y.; Li, H.; Zou, S. Association between Cognitive Distortion, Type D Personality, Family Environment, and Depression in Chinese Adolescents. Depress. Res. Treat. 2011, 2011, 143045. [Google Scholar] [CrossRef] [PubMed]
- Coplan, R.J.; Armer, M. Talking Yourself out of Being Shy: Shyness, Expressive Vocabulary, and Socioemotional Adjustment in Preschool. Merrill Palmer Q. 2005, 51, 20–41. [Google Scholar] [CrossRef]
- Van Roy, B.; Groholt, B.; Heyerdahl, S.; Clench-Aas, J. Understanding discrepancies in parent-child reporting of emotional and behavioural problems: Effects of relational and socio-demographic factors. BMC Psychiatry 2010, 10, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagan, M.J.; Roubinov, D.S.; Adler, N.E.; Boyce, W.T.; Bush, N.R. Socioeconomic Adversity, Negativity in the Parent Child-Relationship, and Physiological Reactivity: An Examination of Pathways and Interactive Processes Affecting Young Children’s Physical Health. Psychosom. Med. 2016, 78, 998–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, B.Y.; Xian, D.X. The influence of maternal prenatal education on behavior problems in preschool children. Chin. J. New Clin. Med. 2019, 12, 311–314. [Google Scholar]
- Ruan, Z.L.; Liu, L.; Strodl, E.; Fan, L.J.; Yin, X.N.; Wen, G.M.; Sun, D.L.; Xian, D.X.; Jiang, H.; Jing, J.; et al. Antenatal Training with Music and Maternal Talk Concurrently May Reduce Autistic-Like Behaviors at around 3 Years of Age. Front. Psychiatry 2017, 8, 305. [Google Scholar] [CrossRef] [Green Version]
- Justice, L.; Logan, J.; Kaderavek, J.; Schmitt, M.B.; Tompkins, V.; Bartlett, C. Empirically Based Profiles of the Early Literacy Skills of Children with Language Impairment in Early Childhood Special Education. J. Learn. Disabil. 2015, 48, 482–494. [Google Scholar] [CrossRef]
- Bleses, D.; Jensen, P.; Hojen, A.; Dale, P.S. An educator-administered measure of language development in young children. Infant Behav. Dev. 2018, 52, 104–113. [Google Scholar] [CrossRef]
- Ying, L.; Zhou, H.; Yu, S.; Chen, C.; Jia, X. Parent-child communication and self-esteem mediate the relationship between interparental conflict and children’s depressive symptoms. Child Care Health Dev. 2018, 44, 908–915. [Google Scholar] [CrossRef]
- Xu, W.; Yan, N.; Chen, G.; Zhang, X.; Feng, T. Parent-child separation: The relationship between separation and psychological adjustment among Chinese rural children. Qual. Life Res. 2018, 27, 913–921. [Google Scholar] [CrossRef]
- Noel, M.; Peterson, C.; Jesso, B. The relationship of parenting stress and child temperament to language development among economically disadvantaged preschoolers. J. Child Lang. 2008, 35, 823–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gass, S.M.; Varonis, E.M. Input, Interaction, and Second Language Production. Stud. Second Lang. Acquis. 1994, 16, 283–302. [Google Scholar] [CrossRef] [Green Version]
- Crozier, W.R.; Badawood, A. Shyness, Vocabulary and Children’s Reticence in Saudi Arabian Preschools. Infant Child Dev. 2010, 18, 255–270. [Google Scholar] [CrossRef]
- Salley, B.J.; Dixon, W.E. Temperamental and Joint Attentional Predictors of Language Development. Merrill Palmer Q. 2007, 53, 131–154. [Google Scholar]
- Coplan, R.J.; Weeks, M. Shy and soft-spoken: Shyness, pragmatic language, and socio-emotional adjustment in early childhood. Infant Child Dev. 2010, 18, 238–254. [Google Scholar] [CrossRef]
- Blum, R.W.; Kelly, A.; Ireland, M. Health-risk behaviors and protective factors among adolescents with mobility impairments and learning and emotional disabilities. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2001, 28, 481–490. [Google Scholar] [CrossRef]
- Dahle, A.E.; Knivsberg, A.M.; Andreassen, A.B. Coexisting problem behaviour in severe dyslexia. J. Res. Spec. Educ. Needs 2011, 11, 162–170. [Google Scholar] [CrossRef]
- Poon, K.; Ho, C.S. Contrasting deficits on executive functions in Chinese delinquent adolescents with attention deficit and hyperactivity disorder symptoms and/or reading disability. Res. Dev. Disabil. 2014, 35, 3046–3056. [Google Scholar] [CrossRef]
- Humphrey, N.; Mullins, P.M. Self-concept and self-esteem in developmental dyslexia. J. Res. Spec. Educ. Needs 2010, 2. [Google Scholar] [CrossRef]
- Macdonald, S.J. Biographical pathways into criminality: Understanding the relationship between dyslexia and educational disengagement. Disabil. Soc. 2012, 27, 427–440. [Google Scholar] [CrossRef]
- Terras, M.M.; Thompson, L.C.; Minnis, H. Dyslexia and psycho-social functioning: An exploratory study of the role of self-esteem and understanding. Dyslexia 2010, 15, 304–327. [Google Scholar] [CrossRef] [PubMed]
- Felder-Puig, R.; Baumgartner, M.R.; Gadner, H.; Formann, A. Health-related quality of life in Austrian elementary school children. Med Care 2008, 46, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Karande, S.; Kulkarni, M. Specific learning disability: The invisible handicap. Indian Pediatrics 2005, 42, 315–319. [Google Scholar] [PubMed]
- Humphrey, N. Teacher and pupil ratings of self-esteem in developmental dyslexia. Br. J. Spec. Educ. 2002, 29, 29–36. [Google Scholar] [CrossRef]
- Humphrey, N. Facilitating a positive sense of self in pupils with dyslexia: The role of teachers and peers. Support Learn. 2010, 18, 130–136. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Dyslexia Group (n = 60) | Control Group (n = 180) | χ2/t | p |
|---|---|---|---|---|
| Age (Mean ± SD) | 9.93 ± 1.01 | 10.02 ± 0.78 | −0.716 | 0.475 |
| Gender, n (%) | ||||
| Male | 40(66.7) | 117(65.0) | 0.055 | 0.814 |
| Female | 20(33.3) | 63(35.0) | ||
| Only child family | 10(16.7) | 41(22.8) | 1.004 | 0.316 |
| Single parent family | 3(5.0) | 15(8.3) | 0.721 | 0.396 |
| Residence | ||||
| Urban | 52(86.7) | 138(76.7) | 2.728 | 0.092 |
| Rural | 8(13.3) | 42(23.3) | ||
| Antenatal training Preschool education before 3 years | 10(16.7) 21(35.0) | 64(35.6) 60(33.3) | 7.528 0.056 | 0.006 0.813 |
| Family member also suffer from dyslexia | 13(21.7) | 4(2.2) | 22.981 | <0.001 |
| Parent-child relationship | ||||
| Good | 44(73.3) | 147(81.7) | 6.142 | 0.046 |
| General | 12(20.0) | 31(17.2) | ||
| Bad | 4(6.7) | 2(1.1) | ||
| Communication between parents and children | ||||
| Every day | 41(63.3) | 123(68.3) | 14.631 | 0.002 |
| 33–34 times a week | 4(6.7) | 29(16.1) | ||
| 1–2 times a week | 9(20.0) | 26(14.5) | ||
| <1 time a week | 6(10.0) | 2(1.1) | ||
| Time to start speaking | ||||
| 0.5–2.5 years old | 50(83.3) | 154(85.6) | 0.193 | 0.908 |
| 2.5–4 years old | 9(15.0) | 23(12.8) | ||
| More than 4 years old | 1(1.7) | 3(1.6) | ||
| Father’s occupation | ||||
| Farmer | 12(20.0) | 11(6.1) | 12.911 | 0.005 |
| Worker | 22(36.7) | 56(31.1) | ||
| Businessman/service providers | 18(30.0) | 69(38.3) | ||
| Professionals/public official | 8(13.3) | 44(24.5) | ||
| Mother’s occupation | ||||
| Farmer | 11(18.3) | 9(5.0) | 14.383 | 0.002 |
| Worker | 23(38.3) | 61(33.9) | ||
| Businessman/service providers | 24(40.0) | 87(48.3) | ||
| Professionals/public official | 2(3.4) | 23(12.8) | ||
| Father’s education level | ||||
| Elementary school or below | 17(28.3) | 23(12.8) | 9.526 | 0.023 |
| Junior high school | 12(20.0) | 61(33.9) | ||
| Senior high school | 17(28.3) | 56(31.1) | ||
| College and above | 14(23.4) | 40(22.2) | ||
| Mother’s education level | ||||
| Elementary school or below | 11(18.3) | 25(13.9) | 8.353 | 0.039 |
| Junior high school | 26(43.3) | 48(26.7) | ||
| Senior high school | 12(20.0) | 55(30.6) | ||
| College and above | 11(18.3) | 52(28.9) | ||
| Household income (monthly) | ||||
| <3000 | 5(8.3) | 14(7.8) | 8.677 | 0.034 |
| 3000–5000 | 35(58.3) | 70(38.9) | ||
| 5000–10,000 | 16(26.7) | 64(35.6) | ||
| ≥10,000 | 4(6.7) | 32(17.8) |
| Investigated Factors | β | SE | Wald | p | OR (95% CI) |
|---|---|---|---|---|---|
| Antenatal training | −1.015 | 0.380 | 7.138 | 0.008 | 0.36(0.17–0.76) |
| Family member also suffer from dyslexia | 2.499 | 0.595 | 17.647 | <0.001 | 12.17(3.79–39.05) |
| Parent-child relationship | |||||
| Good | 1.00 (Ref) | ||||
| General | 0.257 | 0.381 | 0.456 | 0.500 | 1.29(0.61–2.73) |
| Bad | 1.899 | 0.883 | 4.628 | 0.031 | 6.68(1.18–37.71) |
| Communication frequency between parents and children | |||||
| Every day | 1.00 (Ref) | ||||
| 3–4 times a week | −0.806 | 0.565 | 2.039 | 0.153 | 0.45(1.15–1.35) |
| 1–2 times a week | 0.401 | 0.395 | 1.031 | 0.310 | 1.49(0.69–3.24) |
| <1 time a week | 2.273 | 0.837 | 7.370 | 0.007 | 9.71(1.88–50.12) |
| Father’s occupation | |||||
| Farmer | 1.00 (Ref) | ||||
| Worker | −0.934 | 0.252 | 13.788 | <0.001 | 0.39 (0.24–0.64) |
| Businessman/service providers | −1.344 | 0.265 | 25.777 | <0.001 | 0.26 (0.16–0.44) |
| Professionals/public official | −1.705 | 0.384 | 19.673 | <0.001 | 0.18 (0.09–0.39) |
| Mother’s occupation | |||||
| Farmer | 1.00 (Ref) | ||||
| Worker | −0.975 | 0.245 | 15.890 | <0.001 | 0.38(0.23–0.61) |
| Businessman/service providers | −1.288 | 0.231 | 31.199 | <0.001 | 0.28(0.18–0.43) |
| Professionals/public official | −2.442 | 0.737 | 10.976 | 0.001 | 0.09(0.02–0.37) |
| Father’s education level | |||||
| Elementary school or below | 1.00 (Ref) | ||||
| Junior high school | −1.626 | 0.316 | 26.510 | <0.001 | 0.20(0.11–0.37) |
| Senior high school | −1.192 | 0.277 | 18.534 | <0.001 | 0.31(0.18–0.52) |
| College and above | −1.050 | 0311 | 11.429 | 0.001 | 0.35(0.19–0.64) |
| Mother’s education level | |||||
| Elementary school or below | 1.00 (Ref) | ||||
| Junior high school | −0.613 | 0.244 | 6.339 | 0.012 | 0.54(0.34–0.87) |
| Senior high school | −1.522 | 0.319 | 22.832 | <0.001 | 0.22(0.12–0.41) |
| College and above | −1.533 | 0.332 | 21.908 | <0.001 | 0.21(0.11–0.41) |
| Household income | |||||
| <3000 | 1.00 (Ref) | ||||
| 3000–5000 | −0.693 | 0.207 | 11.211 | 0.001 | 0.50(0.33–0.75) |
| 5000–10,000 | −1.386 | 0.280 | 24.599 | <0.001 | 0.25(0.15–0.43) |
| ≥10,000 | −2.079 | 0.530 | 15.374 | <0.001 | 0.13(0.04–0.35) |
| Personality | Dyslexia Group (n = 60) | Control Group (n = 180) | t | p |
|---|---|---|---|---|
| Psychoticism | 50.25 ± 12.90 | 46.33 ± 10.00 | 2.28 | 0.040 |
| Extroversion/Introversion | 40.42 ± 12.53 | 44.50 ± 11.05 | −2.26 | 0.025 |
| Neuroticism | 54.08 ± 11.33 | 49.65 ± 10.24 | 2.68 | 0.008 |
| Dissimulation | 48.17 ± 9.78 | 52.15 ± 7.68 | −2.28 | 0.007 |
| Dimensions | Dyslexia Group (n = 60) | Control Group (n = 180) | t | p |
|---|---|---|---|---|
| Psychosocial function (21 items) | 2.56 ± 0.47 | 2.84 ± 0.48 | −3.96 | <0.001 |
| Teacher-student relationship | 2.58 ± 0.69 | 2.92 ± 0.63 | −3.449 | 0.001 |
| Peer relation | 2.83 ± 0.61 | 3.21 ± 0.61 | −4.154 | <0.001 |
| Parent-child relationship | 2.84 ± 0.73 | 3.05 ± 0.68 | −2.035 | 0.043 |
| Learning ability and attitude | 2.27 ± 0.76 | 2.64 ± 0.70 | −3.347 | 0.001 |
| Self-concept | 2.27 ± 0.64 | 2.37 ± 0.65 | −1.029 | 0.305 |
| Physical & mental health (12 items) | 2.74 ± 0.45 | 2.99 ± 0.45 | −3.751 | <0.001 |
| Somatic sensation | 2.70 ± 0.47 | 2.91 ± 0.45 | −3.115 | 0.020 |
| Negative emotion | 2.77 ± 0.61 | 2.79 ± 0.63 | −0.271 | 0.784 |
| Attitude of homework | 2.75 ± 0.80 | 3.28 ± 0.62 | −5.135 | <0.001 |
| Living environment (8 items) | 2.70 ± 0.50 | 2.72 ± 0.54 | 0.098 | 0.922 |
| Life convenience | 3.01 ± 0.75 | 3.23 ± 0.73 | −1.984 | 0.049 |
| Extracurricular activities | 2.55 ± 0.76 | 2.28 ± 0.71 | 2.439 | 0.016 |
| Athletic ability | 2.55 ± 0.76 | 2.65 ± 0.75 | −0.856 | 0.393 |
| Satisfaction of living quality (8 items) | 2.84 ± 0.59 | 2.96 ± 0.51 | −1.429 | 0.155 |
| Self-satisfaction | 2.94 ± 0.69 | 3.17 ± 0.56 | −2.480 | 0.014 |
| Others | 2.75 ± 0.80 | 2.75 ± 0.72 | −0.066 | 0.947 |
| Total score (49 items) | 131.52 ± 18.05 | 141.64 ± 18.13 | −3.670 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.; He, M.; Li, A.; Lin, Y.; Zhang, X.; Wu, K. Personality, Behavior Characteristics, and Life Quality Impact of Children with Dyslexia. Int. J. Environ. Res. Public Health 2020, 17, 1415. https://doi.org/10.3390/ijerph17041415
Huang Y, He M, Li A, Lin Y, Zhang X, Wu K. Personality, Behavior Characteristics, and Life Quality Impact of Children with Dyslexia. International Journal of Environmental Research and Public Health. 2020; 17(4):1415. https://doi.org/10.3390/ijerph17041415
Chicago/Turabian StyleHuang, Yanhong, Meirong He, Anna Li, Yuhang Lin, Xuanzhi Zhang, and Kusheng Wu. 2020. "Personality, Behavior Characteristics, and Life Quality Impact of Children with Dyslexia" International Journal of Environmental Research and Public Health 17, no. 4: 1415. https://doi.org/10.3390/ijerph17041415
APA StyleHuang, Y., He, M., Li, A., Lin, Y., Zhang, X., & Wu, K. (2020). Personality, Behavior Characteristics, and Life Quality Impact of Children with Dyslexia. International Journal of Environmental Research and Public Health, 17(4), 1415. https://doi.org/10.3390/ijerph17041415