1. Introduction
Air pollution has been a worldwide environmental problem and major risk to human health. Fine particular matter pollution (PM2.5) and its detrimental health effects have raised great public health concerns around the world, not only in China. According to the International Agency for Research on Cancer Monographs on the Evaluation of Carcinogenic Risks to Humans, PM2.5 has become a carcinogenic factor for lung cancer [
1,
2]. It has been estimated that outdoor air pollution including PM2.5 has caused 4.2 million premature deaths per year in the world, with the greatest number in South-East Asia and the Western Pacific regions and with 6% of deaths caused by lung cancer [
3]. Currently, trachea, bronchus and lung cancers represent the majority of cancer incidences in China, with the age-adjusted incidence rate of 36.54 per 100,000 in 2014 [
4]. However, despite some efforts examining PM2.5 or PM10 effects on lung cancer mortality [
5,
6,
7,
8], the associations between exposure to PM2.5 and lung cancer incidence were not well and comprehensively understood in China.
Most research on PM2.5-associated lung cancer incidence were conducted in developed countries, where health outcome data are more readily available. As published in the International Agency for Research on Cancer Monographs (volume 109) on the Evaluation of Carcinogenic Risks to Humans, biologically, the exposure to outdoor air pollution, which includes the ambient particulate matter, would lead to increased cancer risks in humans through the elevations in genetic damage, such as cytogenetic abnormalities, altered gene expression and mutations in both somatic and germ cells [
1,
2]. Empirically, the substantial body of studies in developed countries suggested a significant and positive association between PM2.5 exposure and lung cancer incidence. In particular, the 17 prospective European cohort studies that were performed in 12 European areas (one of the largest and most informative studies) suggested that a 5 μg/m
3 increment in annual exposure to PM2.5 was correlated with the elevation of hazard ratio of lung cancer incidence by 1.18 [
9]. Even restricting the study population to those who had never smoked, long-term exposure to PM2.5 was still statistically and positively associated with the risk of lung cancer mortality [
10]. Other nationwide studies in western countries further enhance the evidence of significant effects of PM2.5 exposure on lung cancer incidence [
11,
12,
13]. However, these nationwide or multisite long-term estimations from developed countries might not be applicable to China. There are significant differences in the air pollution level between China and Western countries. More specifically, the annual medium concentration of PM2.5 in China was 54 μg/m
3, which is more than four times higher than that in Western countries (e.g., 12 μg/m
3 for the United Kingdom, 8 μg/m
3 for the United States) [
3], which highlights the significance of examining the association between PM2.5 and lung cancer incidence in other places, such as China.
In comparison, studies that estimate PM2.5 effects on lung cancer incidence in developing countries are quite limited. Overall, these limited studies indicated a significant and adverse effect of PM2.5 exposure on lung cancer incidence. One of the representative studies is a nationwide time-series study with lung cancer incidence data from 75 Chinese cancer registries from 1990 to 2009. Using the spatial age-period-cohort model, the authors found that there were positive associations between 2 year average PM2.5 exposure and lung cancer incidence for both males and females [
14]. Similarly, as suggested in a multisite study of 72 Chinese cities, both the concurrent and previous 8 year annual PM2.5 concentrations were significantly associated with male lung cancer incidence [
15]. However, these multisite or nationwide studies that estimate PM2.5 effects on lung cancer incidence are still quite limited in developing countries. In addition, to have an in-depth understanding of particulate matter effects on lung cancer outcome, especially for lung cancer incidence, further research is needed according to previous study findings. First, these studies either focused on single site [
16] or only urban areas in China [
7,
15,
17], which highlights the necessity for nationwide examinations that include both the urban and rural areas in China. Second, there are relatively few studies examining the long-term effects of particulate matter [
6,
7,
18], especially for the long-term lag response of lung cancer incidence to PM2.5. Third, most of these studies paid attention to the examination of PM2.5-associated lung cancer mortalities [
5,
7,
8,
19], while PM2.5-associated lung cancer incidences were not well and comprehensively examined.
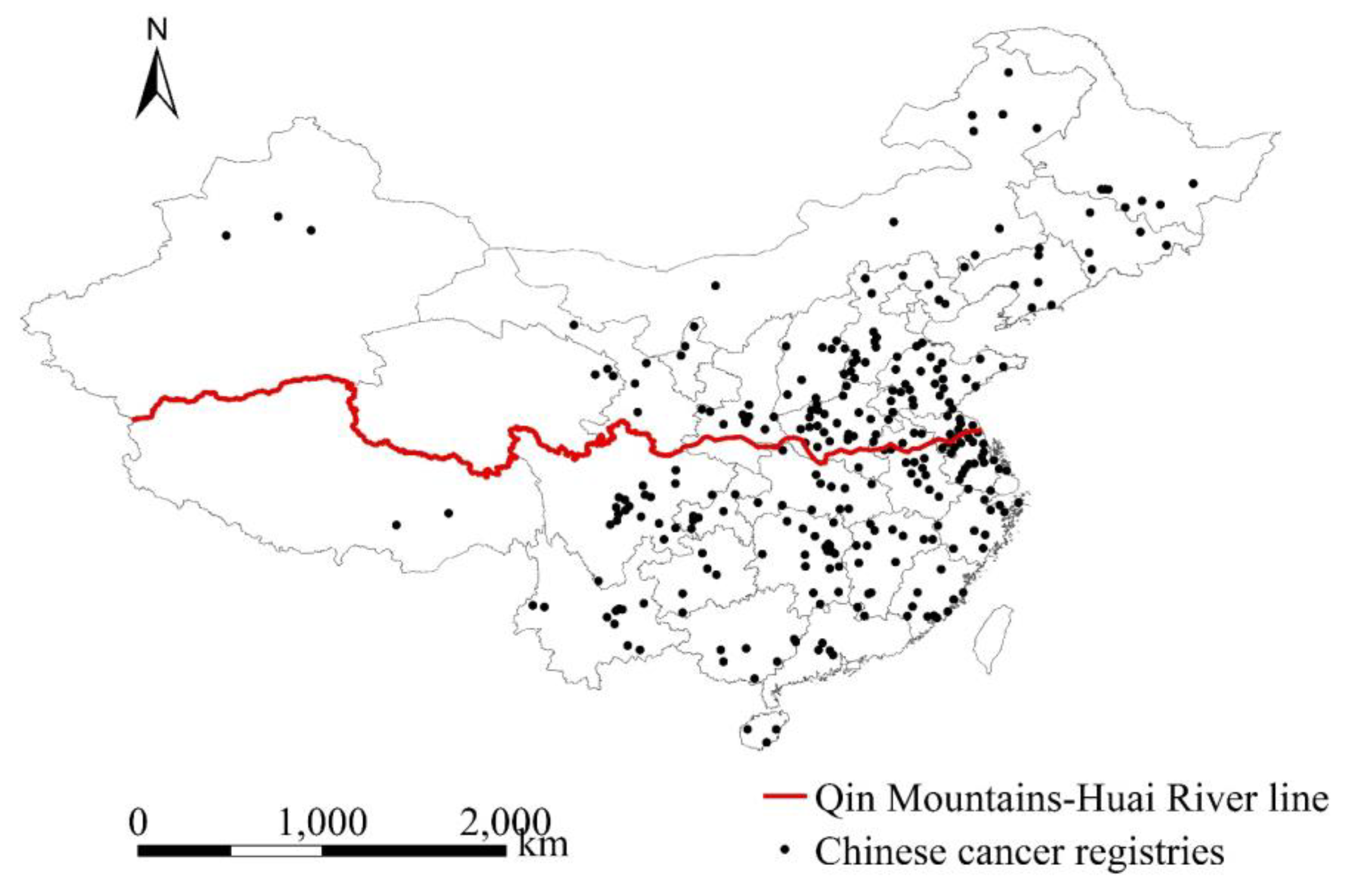
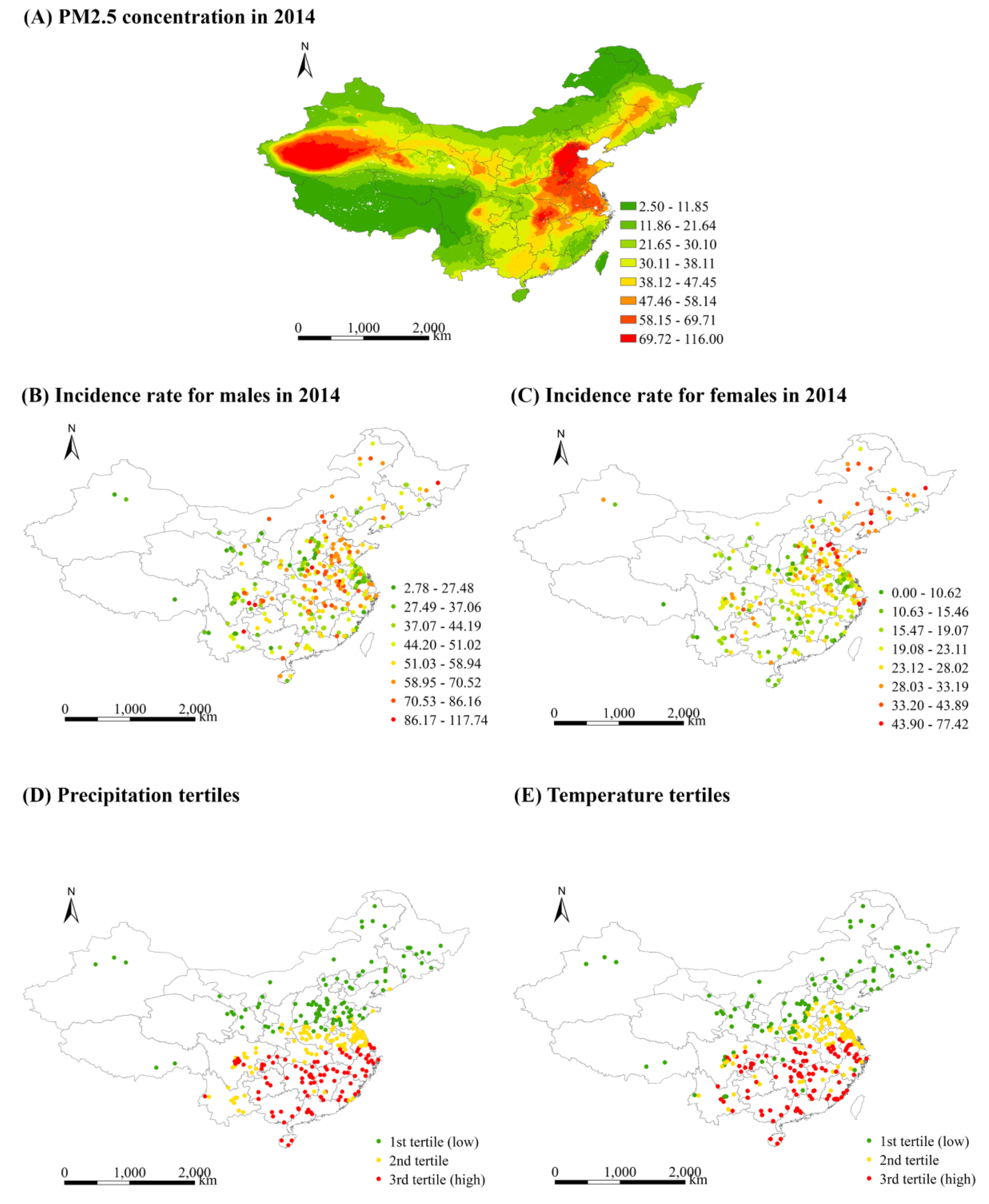
To fill the gaps above, we conducted a nationwide study to estimate the effects of PM2.5 exposure on annual incidence rates of trachea, bronchus and lung cancers in China, using the population-based health outcome data collected from 295 Chinese cancer registries from 2006 to 2014. We determined the estimates using two regression models with controls for location, time and socioeconomic characteristics. We further investigated whether the effects were modified according to the region, temperature and precipitation.
4. Discussion
It is essential to systematically examine air pollution-associated health effects in developing countries where the air pollution level is considerably higher than that in developed countries. However, studies that estimate the effect of PM2.5 on lung cancer incidence in developing countries are still quite limited. In addition, cross-sectional studies that show PM2.5 effects which might not be visible in the individual or cohort studies are also quite limited. Cross-sectional studies, in combination with cohort studies, would contribute to an in-depth understanding of PM2.5 effects on lung cancer incidences.
To our knowledge, this is one of the few nationwide studies that showed positive associations between long-term exposure to PM2.5 and annual incidence rates of lung cancer for both males and females in China. We determined the long-term lag effects of PM2.5 on the incidence rates for both Chinese males and females. Our estimate of the PM2.5 effect was robust to not only the control socioeconomic characteristics, but also the further adjustments of health and behaviour covariates. More fundamentally, we found some evidence of effect modification by temperature.
This study estimated that if PM2.5 changes by 10 μg/m
3, then the incidence rates of lung cancer relative to its mean (for comparison, the mean value was used as baseline) changes by 3.57% and 2.71% for males and females, respectively, which might be considerably lower than those reported in developed countries. In particular, a multisite study of 100 counties in North Carolina indicated that a 10 μg/m
3 change in PM2.5 was positively associated with a 17.28% change in the incidence rate of lung cancer relative to its mean [
39], which is considerably higher than our estimates. The lower effect size of PM2.5 found in our long-term study was also found in the short-term studies in China. As suggested in a time-series study conducted in 272 representative Chinese cities from 2013 to 2015, the effect of short-term exposure to PM2.5 on cardiopulmonary-caused mortality in China was lower than those reported in developed counties [
19]. However, since cross-sectional studies using the incidence rate of lung cancer as the health outcome are still quite limited and it is also hard to compare our estimates with those from cohort studies because of the difference in study design and estimation method [
9,
30], more studies are required to confirm the lower PM2.5 effect found in our study. One possible explanation for a lower PM2.5 effect in China might come from the difference in PM2.5 composition. PM2.5 composition in China has a high proportion of crustal materials and dust [
40], which are less toxic than the fossil-combustion-associated PM2.5 component [
41,
42]. The second explanation might be the tremendous difference in aging situation between China and Western Countries. Despite a rapid aging process in China at the present, the proportion of ageing people (people aged 65 and over) in China was 8.2% in 2010, which is still significantly lower than 13.6% and 20.60% in the US and Germany [
43], making Chinese people less sensitive to exposure to PM2.5.
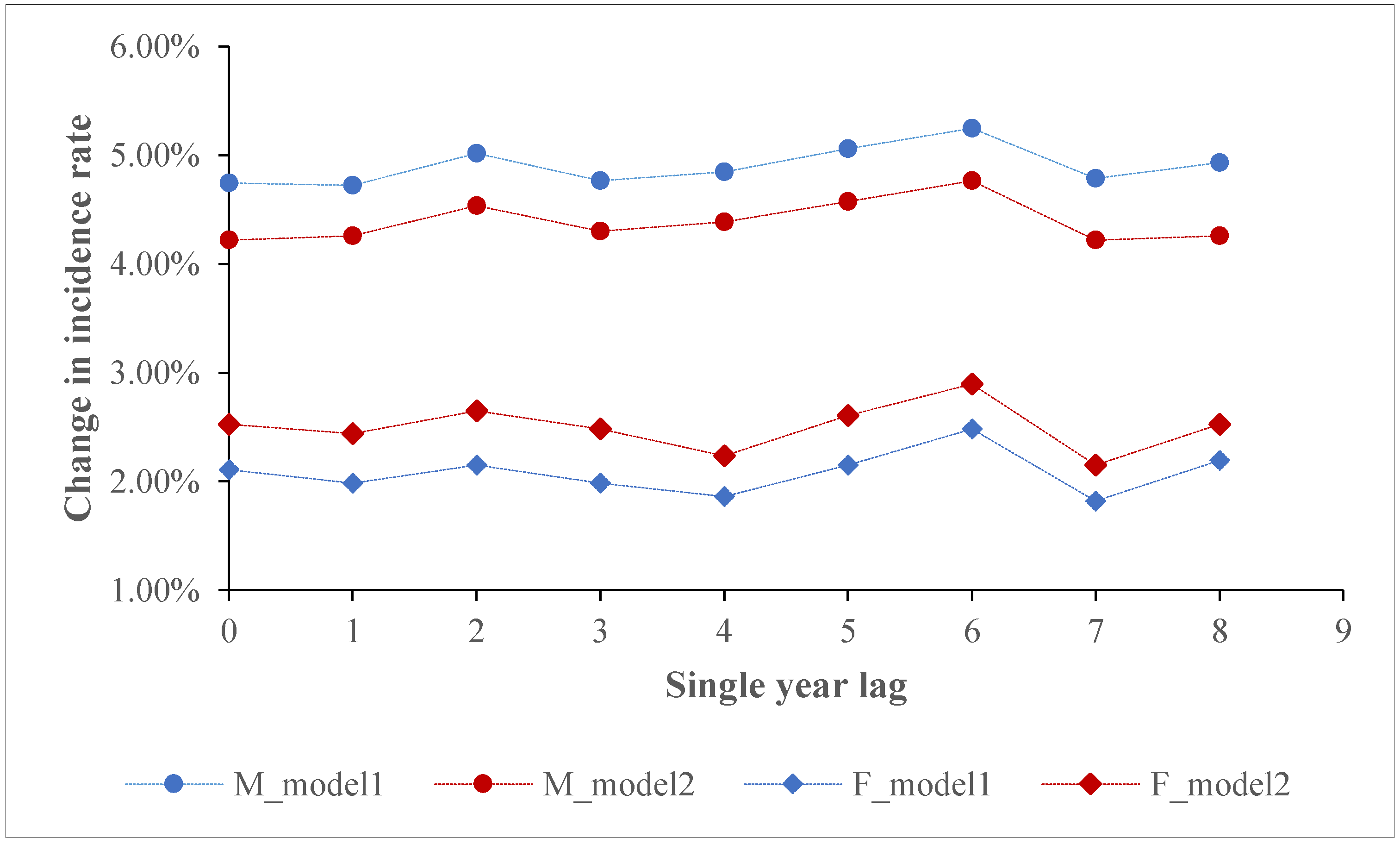
We found the long-term lag effects of PM2.5 on lung cancer incidences, which was seldom reported in previous studies. In the present study, PM2.5 with different single year lags (lag0 to lag8) or moving average year lags ((lag0–1) to (lag0–8)) were all significantly associated with the incidence rate of lung cancer for both males and females. This finding was consistent with that from similar studies. For example, a multisite study of 72 Chinese cities indicated that both the concurrent and previous 8 year annual PM2.5 concentrations were correlated with lung cancer incidence for males [
15]. A nationwide population-based multigenerational panel study from 1990 to 2014 in the US suggested that prenatal and early postnatal exposure to PM2.5 was positively correlated with Childhood Asthma [
44]. Findings from other similar studies further enhanced the evidence of long-term lag effects of air pollution in China [
45,
46] as well as western countries [
30].
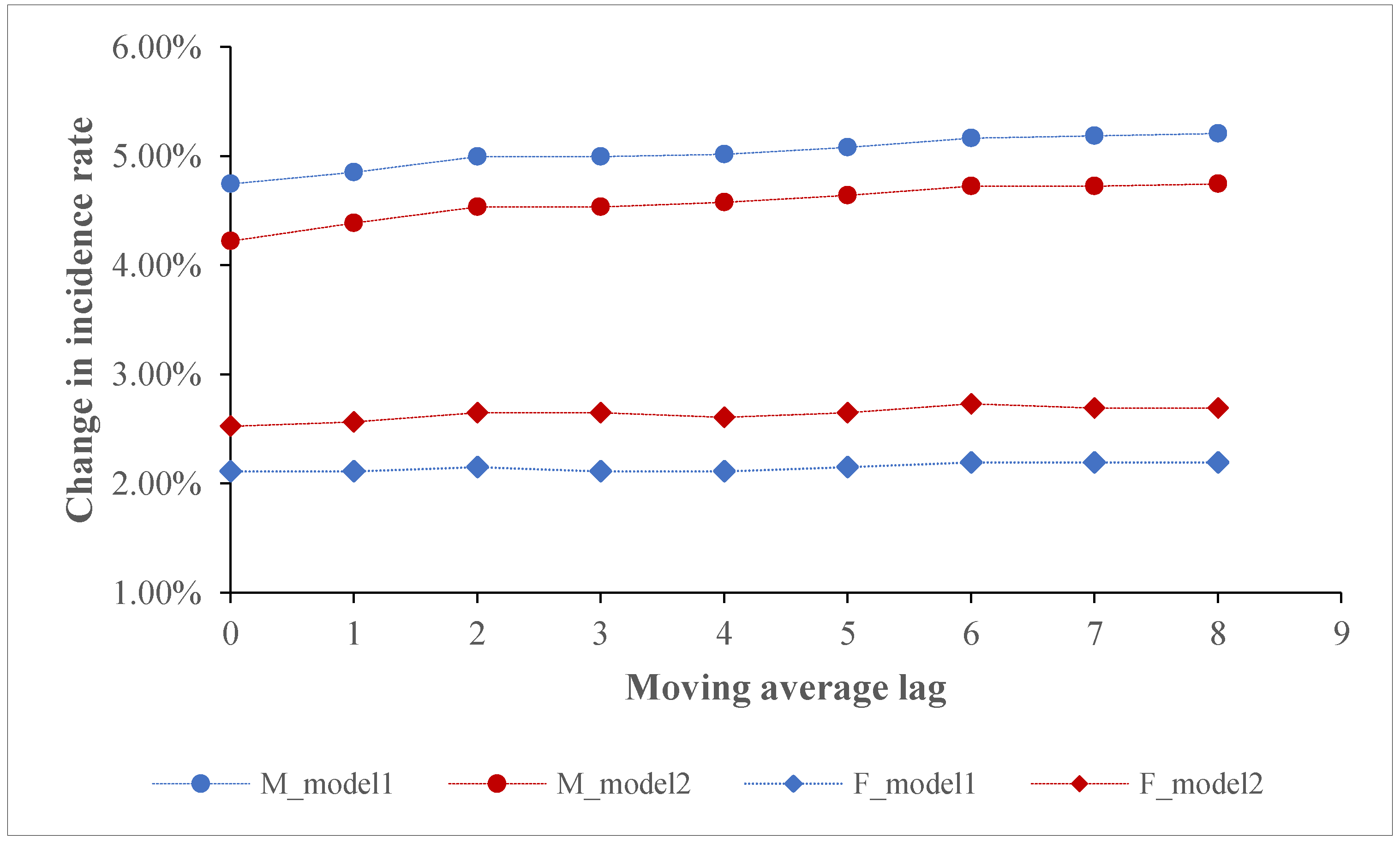
We found that with an elevation of moving average-year lags, PM2.5 effects on the incidence rate of lung cancer for males increased but finally levelled off. The stronger effects that occurred before the level-off point might stem from the fact that with long-term exposure to PM2.5, people tend to intake a low dose of PM2.5; the low intake then causes a slow and subtle change in human lung function, which increasingly leads to a stronger impact on lung cancer incidence. Empirically, the increasingly stronger lag effects could be also found in both the short-term and long-term studies. In particular, a recent time-series study in Shanghai indicated that with an elevation of PM2.5 moving average-day lags (lag01–lag05), the size of PM2.5 effect on daily outpatient visits increased [
47]. Similarly, a time-series study performed in Saudi Arabia also found that a larger PM2.5 moving average-day lag was associated with a greater cardiovascular visits risk for males, females and the combined groups [
48]. Another short-term study that examined the effect of PM2.5 with different lags on respiratory hospital admissions further enhanced the evidence of PM2.5 lag effects [
49]. In addition, a long-term study suggested that compared with the concurrent PM exposure, the second and third-year exposures to PM after birth (i.e., PM1, PM2.5 and PM10) exerted stronger effects on autism spectrum disorder for children [
50]. The findings in the present study highlight that lung cancer incidence is correlated with not only current PM2.5 exposure, but also the previous exposure to PM2.5. Moreover, the estimates by exclusively relying on concurrent PM2.5 exposure might underestimate the actual PM2.5-associated health effects.
We found a positive effect modification by temperature. Despite a recent increasing interest in examining the modification effect of temperature, the findings are mixed. While some short-term studies suggested that the higher temperature was correlated with a strong relationship between air pollution and health outcomes [
51,
52], others found a negative effect modification by temperature [
53,
54]. Our findings support the former argument. The mechanisms of how temperature modifies the association between PM2.5 and health outcomes remain unclear. One possible explanation might be the changed exposure to PM2.5. Temperature can exert effects on the surface air quality by way of affecting the ventilation and dilution of air pollution and the response in atmospheric chemistry [
55]. A cold climate may result in restricted outdoor activities and less efficient penetration of PM2.5 from outdoors to indoors, thus leading to larger measurement errors in colder regions than in warmer regions when using the outdoor fixed-site monitoring data.
Several limitations and future work should be discussed in our study. First, with respect to the sensitivity analysis of PM2.5 effects adjusted by health and behaviour covariates, we attributed the same health-related covariates to counties (districts) that are located in the same prefecture-level city, which might ignore the behaviour variation between these counties. Second, as in many studies that examined the concurrent, 2, 3 or 8 year lag effects of PM2.5 on lung cancer [
14,
15,
56], the 8 year lag (both single and moving average) employed in the present study might be still too short to account for the potential long-latency of lung cancer. We hope to address this limitation in the future if PM2.5 data prior to 1998 become available. Third, as in most previous ecological studies, there are inevitable errors in exposure measurement in our study (i.e., the mean PM2.5 concentration in a county to proxy exposure), because both air pollution variation and the pattern of daily human activity could affect actual human exposure [
57,
58]. Fourth, cohort studies which can relate individual health outcome to PM2.5 exposure are highly required in the future to test our findings because of the ecological nature in the present study.







{kind=link}
{kind=link}
{kind=link}
{kind=link}