2.4. Measures
Demographic data. The participants were asked to specify their gender, age, whether they were a student of the university or college, study program, and their year of study. Demographic questions were taken from the Health Behavior among Lithuanian Adult Population questionnaire, approved for the national survey [
28].
BMI was calculated as body mass (kg) divided by height squared (m
2) from students’ self-reported height and weight. According to the World Health Organization, students’ BMIs were classified into four categories: underweight (<18.5 kg/m
2), normal weight (18.5–24.9 kg/m
2), overweight (25.0–29.9 kg/m
2), and obese (≥30.0 kg/m
2) [
29]. The BMIs ranged from 14.0 to 47.3 (mean = 22.7, SD = 3.7) kg/m². The results showed that majority of the students were of normal body weight; however, 21.9% of men and 12.8% of women were overweight, and 3.9% and 4.2%, respectively, were obese.
The Lithuanian version of the
Multidimensional Body–Self Relations Questionnaire–Appearance Scales (MBSRQ-AS) [
30] was used to assess the appearance-related elements of the body image construct. This instrument comprises five subscales, with responses captured on a 5-point Likert scale ranging from 1 (completely disagree) to 5 (completely agree). The appearance evaluation subscale assesses perceptions of physical attractiveness, with higher scores reflecting a higher attractiveness evaluation; the appearance orientation subscale reveals the degree of investment in one’s appearance, with higher scores indicating a greater investment; the overweight preoccupation subscale evaluates weight vigilance, dieting, fat anxiety, and eating restraint, with higher scores reflecting a greater preoccupation with being overweight; and the body area satisfaction subscale assesses satisfaction or dissatisfaction with particular areas of the body, with higher scores indicating greater body area satisfaction. The Lithuanian version of the MBSRQ-AS (LT-MBSRQ-AS) has demonstrated good validity and reliability in a student population sample [
31]. In the present study, the Cronbach’s alpha values for the appearance evaluation, appearance orientation, overweight preoccupation, and body area satisfaction subscales were 0.83, 0.79, 0.73 and 0.88, respectively.
The Lithuanian version of the
Eating Disorder Examination Questionnaire 6.0 (EDE-Q 6.0) [
32] is a 28-item self-report questionnaire designed to evaluate the essential behavioral characteristics of eating disorders and eating disordered behavior. The EDE-Q 6.0 concentrates on the 28 days prior to the questionnaire and establishes two data models. First, the six open-ended questions yield frequency data on the essential behavioral characteristics of eating disorders (in terms of the number of episodes of the behavior or number of days on which the action occurred): objective binge eating, self-induced vomiting, laxative use, and excessive exercise. Second, 22 attitudinal questions across four subscales produce subscale scores that reflect the severity of the eating disorder characteristics. The responses are recorded on a 7-point Likert scale from 0 (no days) to 6 (every day), with higher scores reflecting a greater severity or higher frequency. The Lithuanian version of the EDE-Q 6.0 (LT-EDE-Q 6.0) has demonstrated good validity and reliability in a student population sample [
33]. In the present study, Cronbach’s alpha for the LT-EDE-Q 6.0 was good, namely 0.94.
We used the
Drive for Muscularity Scale (DMS) [
34] to examine behaviors that reflect preoccupation with muscularity. The scale assesses individuals’ perceptions of not being muscular enough and needing to add bulk to their body frame in the form of muscle mass (irrespective of their percentage of actual muscle mass or body fat). It consists of 15 items rated a on 6-point Likert scale ranging from 1 (never) to 6 (always). Higher scores indicate more muscle development behaviors. The Lithuanian version of the DMS showed good psychometric properties [
35]. In the present study, the internal consistency of the scale was good (Cronbach’s alpha = 0.89).
The Lithuanian version of
Rosenberg’s Self-Esteem Scale (
RSES) [
36] was used to assess self-esteem and general feelings of self-worth. The scale is composed of 10 items scored on a 4-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree). Higher scores denote higher self-esteem. The RSES is the most widely used measure of global self-esteem. The tool demonstrated good internal consistency in the present study, with a Cronbach’s alpha of 0.89.
The Lithuanian version of
The World Health Organization Quality of Life-BREF Questionnaire (WHOQOL-BREF) [
37,
38] is an abbreviated version of the World Health Organization Quality of Life-100 (WHOQOL-100) [
39] self-report questionnaire. It contains 26 items and was used to assess the QoL. Two questions of the overall QoL perception and the overall understanding of health were evaluated separately. The remaining 24 items of the questionnaire comprise four domains. The 7-item (3, 4, 10, 15, 16, 17, and 18) physical health domain includes questions about dependence on medicinal substances and medical aids, pain and discomfort, activities of daily living, energy and fatigue, mobility, sleep, and rest and work capacity. The 6-item (5, 6, 7, 11, 19, and 26) psychological health domain includes questions about self-esteem, body image and appearance, negative and positive feelings, spirituality-religion, personal beliefs, and concentration. The social relations domain assesses personal relationships, social support, and sexual activity; it comprises 3 items (from 20 to 22). The 8-item (8, 9, 12, 13, 14, 23, 24 and 25) environment domain reveals information about one’s financial resources, physical safety, home environment, the possibility for recreation, opportunities for obtaining new skills and knowledge, health and social care, physical environment, and transportation satisfaction. The responses can range from 1 (very dissatisfied) to 5 (very satisfied). The scores are transformed into a scale between 0 and 100, with 0 being very poor and 100 being very good. The reliability and validity of the Lithuanian version of the WHOQOL-BREF (LT-WHOQOL-BREF) in a student population sample have been demonstrated [
40]. The questionnaire was obtained from the official site of the World Health Organization [
39]. The internal consistency of the domains of physical health, psychological health, social relations and the environment was 0.80, 0.85, 0.80, and 0.89, respectively. The Cronbach’s alpha for the LT-WHOQOL-BREF general scale was 0.94.
Leisure time physical activity was assessed using the
Leisure Time Exercise Questionnaire (LTEQ) [
41]. This instrument measures mild, moderate, and strenuous physical activity over one week. The number of bouts of mild exercise is multiplied by 3, moderate exercise by 5, and strenuous exercise by 9, all of which results in a final score of physical activity that provides a total metabolic equivalent by each intensity level. A higher score indicates higher physical activity in each of the three levels. An additional question is used to assess the frequency of vigorous exercise (rarely/never, sometimes, or often).
Self-rated health was evaluated using a single question: “How would you describe your general health during the last 12 months?” There was a 4-point response scale: 1 = “poor”, 2 = “average”, 3 = “good”, and 4 = “excellent”).
Nutrition habits were evaluated using a food frequency questionnaire that contains 19 groups of different foods from the national survey of Health Behavior among Lithuanian Adult Population, 2014 [
28]. After principal component analysis (PCA), six nutrition factors were extracted: fruits, berries, and veggies, unhealthy snacks (sweets and fast food), red meat, chicken and rice, fish, and dairy/porridge. The six factors together explained 51.48% of the total variance Kaiser-Meyer-Olkin (KMO) test = 0.72. Factor loadings from the PCA are presented in
Appendix A,
Table A1. In this study, only the first factor encompassing fresh vegetables, fruits, and berries consumption was used. In addition, a 5-item scale was used to evaluate unhealthy nutrition habits, such as eating while watching TV, eating in a rush, overeating, having unhealthy snacks, and eating late at night, less than 2 h before sleep. The provided response options were from “never” up to “always”. The sum of the answers for each study participant was defined as an unhealthy nutrition score and employed for further analyses as a continuous variable. The higher score indicated a higher frequency of unhealthy eating behaviors.
Smoking and alcohol consumption items were taken from the national survey of Health Behavior among Lithuanian Adult Population 2014 [
28]. Smoking levels were assessed using a single item: “At this moment, how often do you smoke?”. The responses options were: “I have never smoked”, “I smoked some time before, but I quit”, “I occasionally smoke”, or “I smoke at least one cigarette a day.” The answers were dichotomized into yes (yes and sometimes) and no. Alcohol consumption was assessed using two items: “How often do you have a drink containing alcohol?” and “How often do you consume six standard alcohol units per one occasion?”, with the following examples of the most popular alcoholic drinks standard units. In this study, only the information about binge drinking was used. Answers were dichotomized into per cent values for less than once per month and at least once per month.
Single questions were used to indicate average sleep duration and browsing the internet times for non-educational purposes.
2.5. Statistical Analysis
Descriptive statistics were calculated for demographic data and each of the behaviors. The chi-square test and independent samples t test were performed to note any significant differences for each study variable between genders. For the comparison of nonnormally distributed data, the Mann Whitney U test was used. The internal consistency of the scales was tested using Cronbach’s alpha.
Exploratory factor analysis was performed for food frequency items using the extraction method of principal component analysis with the rotation method of varimax with Kaiser normalization. A series of simultaneous multiple linear regression analyses were conducted using age, BMI, lifestyle-related factors, body image scores, and disordered eating scores as the independent variables, and measures of psychological, physical, social, and environmental QoL domains as the dependent variables. Statistical analyses were conducted using IBM SPSS Statistics 26 (IBM Corp., Armonk, NY, USA).
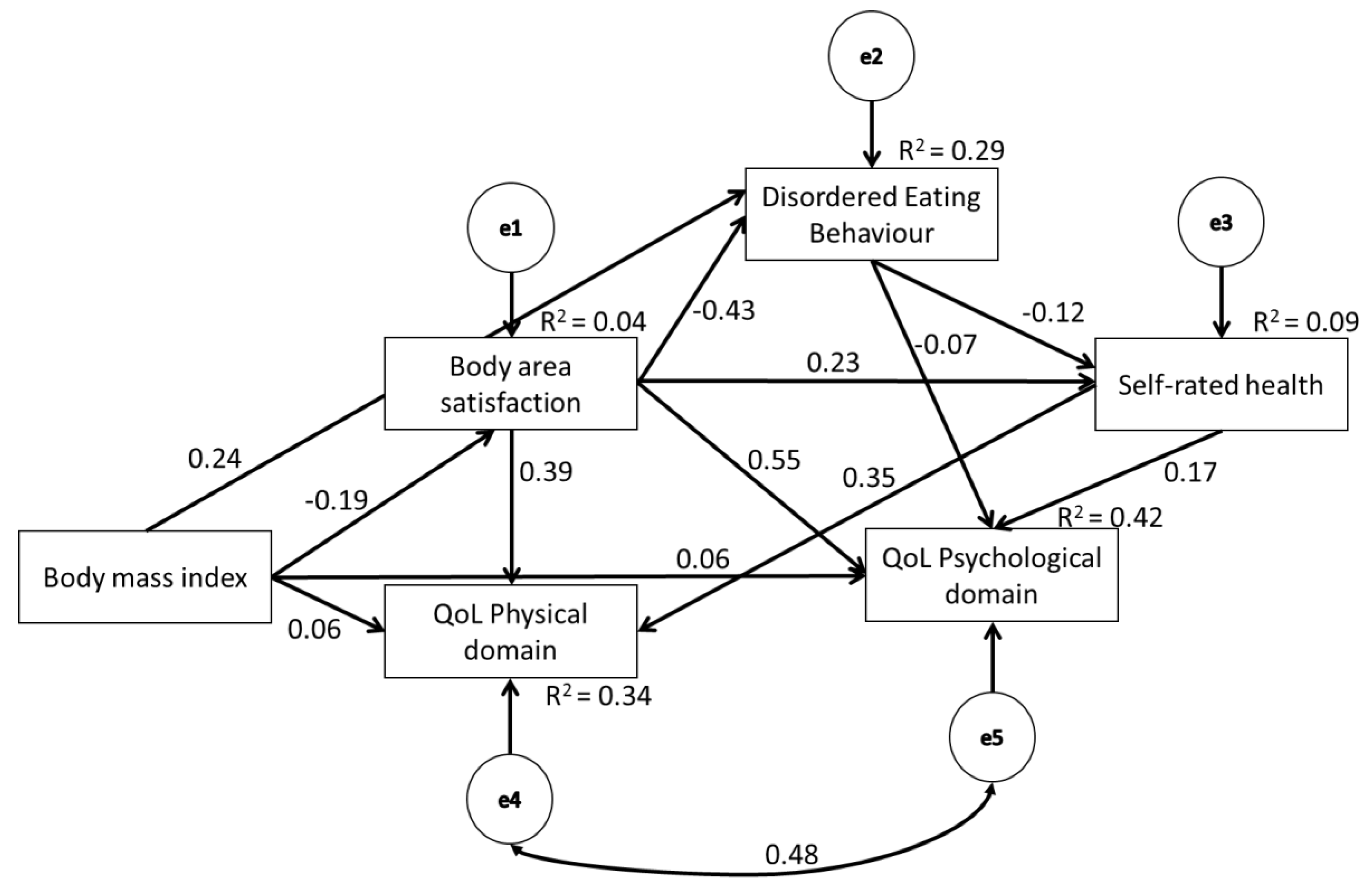
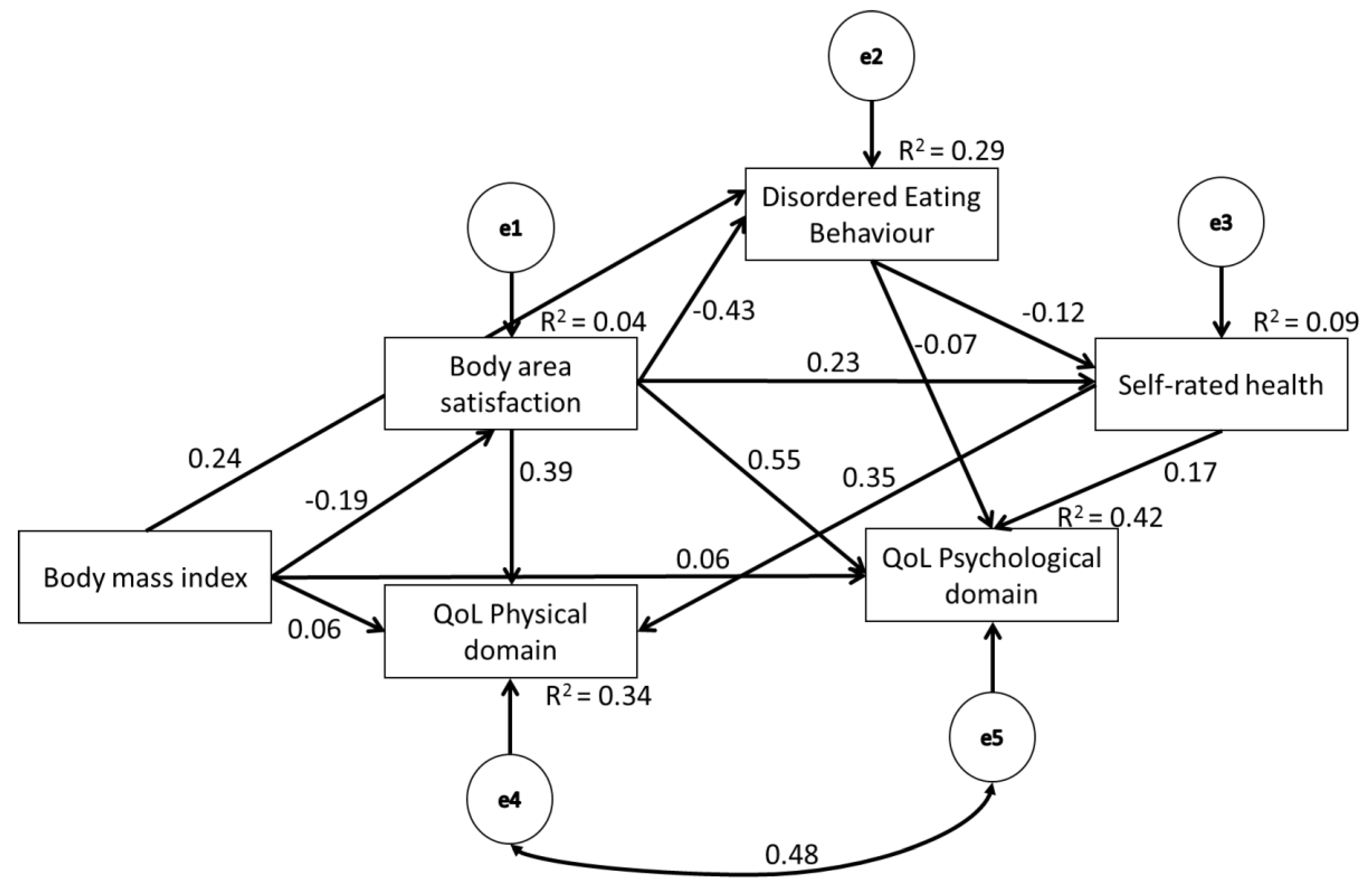
Mediation analysis was conducted using AMOS version 24 (Analysis of Momentary Structure, SPSS, IBM Corp., Armonk, NY, USA) with 2000 bootstrap samples to estimate the size of the total, direct, and indirect effects and to provide 95% confidence intervals (CIs) for each effect. The significance of the direct, indirect, and total effects was assessed with chi-square tests, and the significance of the mediational paths was further confirmed through the bootstrap resampling method, with 2000 bootstrap samples and 95% bias-corrected CIs. The effects were considered significant (p < 0.05) if zero did not appear in the interval between the lower and the upper limits of the CIs. The goodness of fit of the models was assessed using various good fit values: goodness of fit index (GFI; 0.95 < GFI < 1.00); the adjusted goodness of fit index (AGFI; 0.90 < AGFI < 0.95); the comparative fit index (CFI; 0.95 < CFI < 1.00); the Tucker Lewis Index (TLI; 0.95 < TLI < 1.00); and the root of the mean square error of approximation (RMSEA; 0.00 < RMSEA < 0.05 indicates a good fit, while 0.05 < RMSEA < 0.08 indicates an acceptable fit).





{kind=link}