Girls’ Empowerment and Adolescent Pregnancy: A Systematic Review

 , ,
, , 


Abstract
:1. Introduction
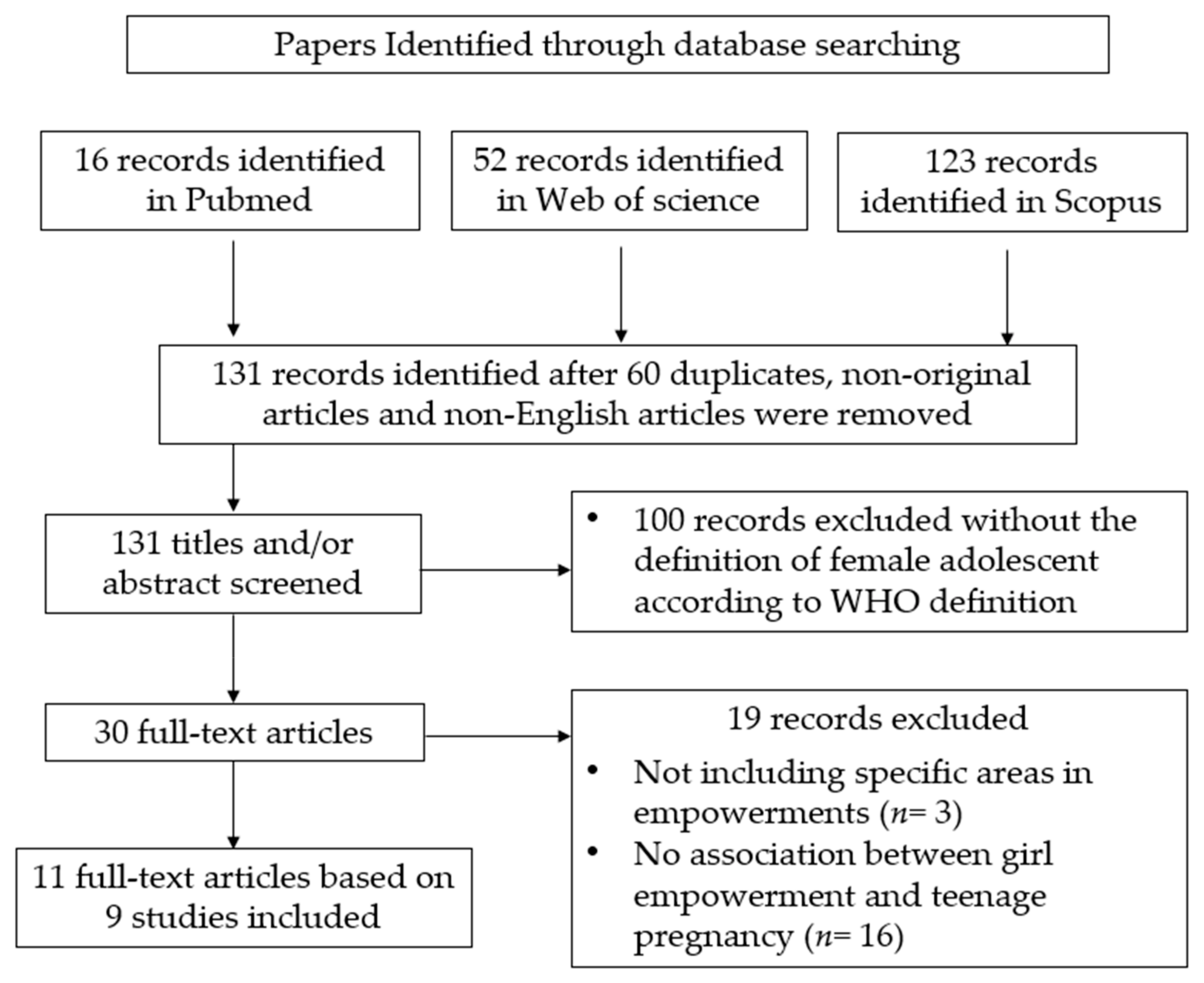
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Selected Studies
2.4. Summary Information
2.5. Quality of Studies
2.6. Ethical Approval
3. Results
Quality Assessment
4. Discussion
4.1. Summary of Evidence
4.2. Educational Empowerment
4.3. Community Empowerment
4.4. Economic Empowerment
4.5. Policy Empowerment
4.6. Lower and Middle Income Countries
4.7. Limitations and Future Considerations
4.8. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Adolescent Pregnancy. Fact Sheets 2018 12/2018. Available online: https://www.who.int/news-room/fact-sheets/detail/adolescent-pregnancy (accessed on 14 December 2018).
- World Health Organization. Adolescent Health. Maternal, Newborn, Child and Adolescent Health 2018 12/2018. Available online: https://www.who.int/maternal_child_adolescent/adolescence/en/ (accessed on 14 December 2018).
- Wikipedia. Adolescence. Adolescence 2018. Available online: https://en.wikipedia.org/wiki/Adolescence (accessed on 14 December 2018).
- Boislard, M.-A.; Van De Bongardt, D.; Blais, M. Sexuality (and Lack Thereof) in Adolescence and Early Adulthood: A Review of the Literature. Behav. Sci. 2016, 6, 8. [Google Scholar] [CrossRef] [PubMed]
- Hanna, B. Negotiating motherhood: The struggles of teenage mothers. J. Adv. Nurs. 2001, 34, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Hofferth, S.L.; Hayes, C.D.; Council, N.R. The children of teen childbearers, in Risking the Future: Adolescent Sexuality, Pregnancy, and Childbearing, Volume II: Working Papers and Statistical Appendices; National Academies Press (US): Cambridge, MA, USA, 1987. [Google Scholar]
- The Urban Child Institute. How Adolescent Parenting Affects Children, Families, and Communities. Editorials 2014 27/02/2014. Available online: http://www.urbanchildinstitute.org/articles/editorials/how-adolescent-parenting-affects-children-families-and-communities (accessed on 12 January 2020).
- Harrykissoon, S.D.; Rickert, V.I.; Wiemann, C.M. Prevalence and patterns of intimate partner violence among adolescent mothers during the postpartum period. Arch. Pediatr. Adolesc. Med. 2002, 156, 325–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santelli, J.S.; Sharma, V.; Viner, R., 3rd. Inequality, National Wealth, Economic Development and Global Trends in Teenage Birth Rates, 1990–2010. J. Adolesc. Health 2013, 52, S4–S5. [Google Scholar] [CrossRef]
- Rahman, A. Women’s Empowerment: Concept and Beyond. Double Blind Peer Rev. Int. Res. J. 2013, 13, 9–13. [Google Scholar]
- Presler-Marshall, E.; Jones, N. Empowering Girls to Prevent Early Pregnancy; Overseas Development Institute: London, UK, 2012. [Google Scholar]
- Van Rooyen, C.; Stewart, R.; De Wet, T. The Impact of Microfinance in Sub-Saharan Africa: A Systematic Review of the Evidence. World Dev. 2012, 40, 2249–2262. [Google Scholar] [CrossRef] [Green Version]
- Kirby, D.B.; Laris, B.; Rolleri, L.A. Sex and HIV Education Programs: Their Impact on Sexual Behaviors of Young People throughout the World. J. Adolesc. Health 2007, 40, 206–217. [Google Scholar] [CrossRef]
- Wakoko, F. Microfinance and Women’s Empowerment in Uganda: A Socioeconomic Approach; The Ohio State University: Columbus, OH, USA, 2003. [Google Scholar]
- Kemigisha, E.; Bruce, K.; Ivanova, O.; Leye, E.; Coene, G.; Ruzaaza, G.N.; Ninsiima, A.B.; Mlahagwa, W.; Nyakato, V.N.; Michielsen, K. Evaluation of a school based comprehensive sexuality education program among very young adolescents in rural Uganda. BMC Public Health 2019, 19, 1393. [Google Scholar] [CrossRef] [Green Version]
- De Castro, F.; Rojas-Martínez, R.; Villalobos-Hernández, A.; Allen-Leigh, B.; Braverman-Bronstein, A.; Billings, D.L.; Uribe-Zúñiga, P. Sexual and reproductive health outcomes are positively associated with comprehensive sexual education exposure in Mexican high-school students. PLoS ONE 2018, 13. [Google Scholar] [CrossRef] [Green Version]
- Denwigwe, C. Teenage Empowerment through Self-Understanding and Decision-Making Skills for Prevention of Teenage Pregnancy; University of Calabar Press: Calabar, Nigeria, 2018. [Google Scholar]
- Bandiera, O.; Buehren, N.; Burgess, R.; Goldstein, M.; Gulesci, S.; Rasul, I.; Sulaiman, M. Empowering Adolescent Girls; World Bank: Washington, DC, USA, 2012. [Google Scholar]
- Biello, K.B.; Sipsma, H.L.; Ickovics, J.R.; Kershaw, T. Economic Dependence and Unprotected Sex: The Role of Sexual Assertiveness among Young Urban Mothers. J. Urban Health 2010, 87, 416–425. [Google Scholar] [CrossRef] [Green Version]
- Do, M.; Kurimoto, N. Women’s empowerment and choice of contraceptive methods in selected African countries. Int. Perspect. Sex. Reprod. Health 2012, 38, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Reed, E.; Donya, B.; Dasgupta, A.; Ghule, M.; Battala, M.; Nair, S.; Silverman, J.; Jadhav, A.; Palaye, P.; Saggurti, N.; et al. Access to Money and Relation to Women’s Use of Family Planning Methods Among Young Married Women in Rural India. Matern. Child Health J. 2016, 20, 1203–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braine, T. Adolescent pregnancy: A culturally complex issue. Bull World Health Organ 2009, 87, 410–411. [Google Scholar] [PubMed]
- Akella, D. Socio-Cultural Influences on Teenage Pregnancy and Contemporary Prevention Measures; IGI Global: Hershey, PA, USA, 2018. [Google Scholar]
- Ahorlu, C.S.; Pfeiffer, C.; Obrist, B. Socio-cultural and economic factors influencing adolescents’ resilience against the threat of teenage pregnancy: A cross-sectional survey in Accra, Ghana. Reprod. Health 2015, 12, 117. [Google Scholar] [CrossRef] [Green Version]
- DiCenso, A.; Guyatt, G.; Willan, A.; Griffith, L. Interventions to reduce unintended pregnancies among adolescents: Systematic review of randomised controlled trials. BMJ 2002, 324. [Google Scholar] [CrossRef] [Green Version]
- Holt, K.; Lince, N.; Hargey, A.; Nkala, B.; Mclntyre, J.; Gray, G.; Mnyani, C.; Blanchard, K. Assessment of service availability and health care workers’ opinions about young women’s sexual and reproductive health in Soweto, South Africa. Afr. J. Reprod. Health 2012, 16, 283–293. [Google Scholar]
- Govender, T.; Reddy, P.; Ghuman, S. Obstetric outcomes and antenatal access among adolescent pregnancies in KwaZulu-Natal, South Africa. So. Afr. Fam. Pract. 2017, 60, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Kassa, G.M.; Arowojolu, A.O.; Odukogbe, A.A.; Yalew, A.W. Prevalence and determinants of adolescent pregnancy in Africa: A systematic review and Meta-analysis. Reprod. Health 2018, 15, 195. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. An. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- NIH. Quality Assessment Tool for Observational Cohort and Cross Sectional Studies. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 30 July 2018).
- Critical Appraisal Skills Programme. Critical Appraisal Skills Programme: Making Sense of Evidence, in Critical Appraisal Skills Programme; Critical Appraisal Skills Programme: Pavilion, Middle Town, Oxford, UK, 2014. [Google Scholar]
- Sterne, J.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366. [Google Scholar] [CrossRef] [Green Version]
- Lehman, S.J.; Koerner, S.S. Adolescent Women’s Sports Involvement and Sexual Behavior/Health: A Process-Level Investigation. J. Youth Adolesc. 2004, 33, 443–455. [Google Scholar] [CrossRef]
- Fischl, R.A.F.; Herman, W.H.; Sereika, S.M.; Hannan, M.; Becher, D.; Mansfiel, M.J.; Freytag, L.L.; Milaszewski, K.; Botscheller, A.N.; Charron-Prochownik, D. Impact of a Preconception Counseling Program for Teens With Type 1 Diabetes (READY-Girls) on Patient-Provider Interaction, Resource Utilization, and Cost. Diabetes Care 2010, 33, 701–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juma, M.; Alaii, J.; Bartholomew, L.K.; Askew, I.; Borne, B.V.D. Understanding orphan and non-orphan adolescents’ sexual risks in the context of poverty: A qualitative study in Nyanza Province, Kenya. BMC Int. Health Hum. Rights 2013, 13, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarnquist, C.; Omondi, B.; Sinclair, J.; Gitau, C.; Paiva, L.; Mulinge, M.; Cornfield, D.N.; Maldonado, Y. Rape Prevention Through Empowerment of Adolescent Girls. Pediatrics 2014, 133, e1226–e1232. [Google Scholar] [CrossRef] [Green Version]
- Vaz, R.F.; Monteiro, D.L.M.; Rodrigues, N.C.P. Trends of teenage pregnancy in Brazil, 2000–2011. Rev. Assoc. Médica Bras. 2016, 62, 330–335. [Google Scholar] [CrossRef]
- Lys, C.; Reading, C. Coming of age: How young women in the Northwest Territories understand the barriers and facilitators to positive, empowered, and safer sexual health. Int. J. Circumpolar Health 2012, 71, 5. [Google Scholar] [CrossRef]
- Fagbamigbe, A.F.; Idemudia, E. Survival analysis and prognostic factors of timing of first childbirth among women in Nigeria. BMC Pregnancy Childbirth 2016, 16. [Google Scholar] [CrossRef] [Green Version]
- Shrestha, S. Socio-cultural factors influencing adolescent pregnancy in rural Nepal. Int. J. Adolesc. Med. Health 2002, 14, 101–110. [Google Scholar] [CrossRef]
- Thorsén, C.; Aneblom, G.; Gemzell-Danielsson, K. Perceptions of contraception, non-protection and induced abortion among a sample of urban Swedish teenage girls: Focus group discussions. Eur. J. Contracept. Reprod. Health Care 2006, 11, 302–309. [Google Scholar] [CrossRef]
- Kaphagawani, N.C.; Kalipeni, E. Sociocultural factors contributing to teenage pregnancy in Zomba district, Malawi. Glob. Public Health 2016, 12, 1–17. [Google Scholar] [CrossRef]
- Biney, A.; Nyarko, P. Is a woman’s first pregnancy outcome related to her years of schooling? An assessment of women’s adolescent pregnancy outcomes and subsequent educational attainment in Ghana. Reprod. Health 2017, 14, 123. [Google Scholar] [CrossRef] [PubMed]
- Westall, J. Poor education linked with teen pregnancies. BMJ 1997, 314, 535–540. [Google Scholar] [CrossRef] [Green Version]
- Almeida, M.-D.-C.C.; Aquino, E.M.L. Adolescent pregnancy and completion of basic education: A study of young people in three state capital cities in Brazil. Cad. De Saúde Pública 2011, 27, 2386–2400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitz, K. Adolescent pregnancy prevention: A review of interventions and programs. Clin. Psychol. Rev. 1999, 19, 457–471. [Google Scholar] [CrossRef]
- Salam, R.A.; Das, J.K.; Lassi, Z.S.; Bhutta, A.Z. Adolescent Health Interventions: Conclusions, Evidence Gaps, and Research Priorities. J. Adolesc. Health 2016, 59, S88–S92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oringanje, C.; Meremikwu, M.M.; Eko, H.; Esu, E.B.; Meremikwu, A.; Ehiri, E.J. Interventions for preventing unintended pregnancies among adolescents. Cochrane Database Syst. Rev. 2016, 2. [Google Scholar] [CrossRef]
- Bandiera, O.; Buehren, N.; Burgess, R.; Goldstein, M.; Gulesci, S.; Rasul, I.; Sulaiman, M. Women’s Empowerment in Action; World Bank: Washington, DC, USA, 2017. [Google Scholar]
- Choudhury, S.; Erausquin, J.T.; Withers, M. Global Perspectives on Women’s Sexual and Reproductive Health across the Lifecourse; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescence and the social determinants of health. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef]
- Raj, A.; Saggurti, N.; Lawrence, D.; Balaiah, N.; Silverman, J.G. Association between adolescent marriage and marital violence among young adult women in India. Int. J. Gynecol. Obstet. 2010, 110, 35–39. [Google Scholar] [CrossRef] [Green Version]
- Raj, A. When the mother is a child: The impact of child marriage on the health and human rights of girls. Arch. Dis. Child. 2010, 95, 931–935. [Google Scholar] [CrossRef]
- Agana, T.A.; Millar, D. Socio-Cultural Practices and Girls Schooling System in the Upper West Region of Ghana. Sky J. Edu. Res. 2015, 3, 97–112. [Google Scholar]
- Mzuza, M.K.; Yudong, Y.; Kapute, F. Analysis of Factors Causing Poor Passing Rates and High Dropout Rates among Primary School Girls in Malawi. World J. Educ. 2014, 4, 48–61. [Google Scholar] [CrossRef]
- Steinberg, L. We Know Some Things: Parent-Adolescent Relationships in Retrospect and Prospect. J. Res. Adolesc. 2001, 11, 1–19. [Google Scholar] [CrossRef]
- Pittman, L.D.; Chase-Lansdale, P.L. African American Adolescent Girls in Impoverished Communities: Parenting Style and Adolescent Outcomes. J. Res. Adolesc. 2001, 11, 199–224. [Google Scholar] [CrossRef]
- Bos, G.A.M.V.D.; Smits, J.P.J.M.; Westert, G.P.; Van Straten, A. Socioeconomic variations in the course of stroke: Unequal health outcomes, equal care? J. Epidemiol. Community Health 2002, 56, 943–948. [Google Scholar]
- Singh, G.K.; Siahpush, M.; Kogan, M.D.; Frieden, T.R.; Dietz, W.; Collins, J. Neighborhood Socioeconomic Conditions, Built Environments, And Childhood Obesity. Health Aff. 2010, 29, 503–512. [Google Scholar] [CrossRef] [Green Version]
- McCleary-Sills, J.; Douglas, Z.; Rwehumbiza, A.; Hamisi, A.; Mabala, R. Gendered norms, sexual exploitation and adolescent pregnancy in rural Tanzania. Reprod. Health Matters 2013, 21, 97–105. [Google Scholar] [CrossRef]
- UNDP. Human Development Index. Human Development Reports 2018 12/2018. Available online: http://www.hdr.undp.org/en/content/human-development-index-hdi (accessed on 14 December 2018).
- Baird, S.; Chirwa, E.; De Hoop, J.; Özler, B. Girl Power: Cash Transfers and Adolescent Welfare. Evidence from a Cluster-Randomized Experiment in Malawi; National Bureau of Economic Research: Cambridge, MA, USA, 2013. [Google Scholar]
- Trussell, J. The cost of unintended pregnancy in the United States. Contraception 2007, 75, 168–170. [Google Scholar] [CrossRef]
- Chandra-Mouli, V.; Camacho, A.V.; Michaud, P.-A. WHO Guidelines on Preventing Early Pregnancy and Poor Reproductive Outcomes Among Adolescents in Developing Countries. J. Adolesc. Health 2013, 52, 517–522. [Google Scholar] [CrossRef]
- Teitelman, A.M.; Ratcliffe, S.; Morales-Aleman, M.M.; Sullivan, C.M. Sexual relationship power, intimate partner violence, and condom use among minority urban girls. J. Interpers. Violence 2008, 23, 1694–1712. [Google Scholar] [CrossRef]
- GirlsnotBrides. Sustainable Development Goals (SDGs). Available online: https://www.girlsnotbrides.org/themes/sustainable-development-goals-sdgs/ (accessed on 19 November 2019).
- UNFPA. State of World Population 2013. In The State of World Population; Kollodge, R., Ed.; Information and External Relations Division, UNFPA: New York, NY, USA, 2013. [Google Scholar]


{kind=link}
| Title | Study Authors /Reference ID | Year | Country | Study Design/Quality 1 | Sample | Type of Empowerment | Empowerment (Measurement) | Major Findings |
|---|---|---|---|---|---|---|---|---|
| Adolescent women’s sports involvement and sexual behavior/health: A process-level investigation | Lehman et al. [33] | 2004 | United States | Mixed Methods investigation Low | 176 adolescent women, 18–19 years | Educational and community empowerment | Self-empowerment/efficacy were asked to complete 4 scales (Masculinity, Femininity, Self-Reliance, Self-Efficacy) | Adolescent women’s involvement in organized team sports was significantly associated with the following: (a) sexual-risk-taking behavior (r = −0.34, p < 0.001), (b) sexual health-seeking behavior (r = 0.24, p < 0.01) 2, and (c) sexual/reproductive health (r = 0.21, p < 0.01). |
| Impact of a preconception counseling program for teens with type 1 diabetes (READY-Girls) on patient-provider interaction, resource utilization, and cost | Rodgers Fischl et al. [34] | 2010 | United States | Randomized controlled Low | 88 teens with type I diabetes, (control n = 43), (intervention n = 45), age range 13.2–19.7, M age = 16.7 | Economy, policy, educational empowerment | (a) Knowledge, attitudes, intentions and behaviors 3 (b) economic analysis (resource utilization, direct medical costs, break-even cost analysis | IG had significant and sustained group and time interaction for benefits and knowledge (preconception counseling and reproductive health. (3 months, p < 0.001, 9 months, p < 0.01 (benefits) p <0.001 (knowledge) and (intention). Direct medical costs were low. |
| Understanding orphan and non-orphan adolescents’ sexual risks in the context of poverty: A qualitative study in Nyanza Province, Kenya | Juma et al. [35] | 2013 | Kenya | Qualitative High | 78 (53%) participants were adolescent aged 14–17 years (with 41 female (53%) and 37 male (47%)). 69 (47%) were caregivers | Economic and policy empowerment | This study used focus group discussions (FGDs) and key informant interviews (KIIs) with the following themes relating to poverty and risky sexual behavior. | Poverty seen as key predisposing factor to risky sexual behaviors. Poverty linked with factors that increase vulnerability to transactional sex, early marriage, sexual experimentation, and increased risk of unintended pregnancies and STI/HIV 6 |
| Rape prevention through empowerment of adolescent girls | Sarnquist et al. [36] | 2014 | Kenya | A prospective cohort Low | 1978 adolescents (intervention group)(SOC) 4 group = 428 | Educational empowerment | The intervention was grounded in social learning theory and the health belief model and was adapted from existing empowerment and self-defense modules. (self-reported anonymous survey conducted) | Decrease in annual sexual assault rates (RR = 1.61 95% CI (1.26, 1.86) compared to SOC’s 1.02 95%CI (0.67, 1.57) 5. 52.3% from intervention group reported using learned skills to stop an assault. |
| Trends of adolescent pregnancy in Brazil, 2000–2011 | Vaz et al. [37] | 2016 | Brazil | The cross-sectional (repeated) 2000-2011 Fair | The number of live births to women aged 10–19 years. | Social, educational and economic empowerment | Descriptive study to evaluate frequency of adolescent pregnancy correlating with human development index (HDI), conducted with data from the Brazilian Live Births Information System (Sinasc) of the Unified Health System (Datasus). | Drop in live births from adolescent mothers 23.5% (2000) to 19.2% (2011). HDI score were inversely proportional to the proportion of live births from adolescent mothers |
| Coming of age: how young women in the Northwest Territories understand the barriers and facilitators to positive, empowered, and safer sexual health | Lys et al. [38] | 2012 | Canada | Qualitative (semi-structured, face-to-face interviews) High | 12 females aged 15–19 | Community and educational empowerment | (a) self-perceived barriers facilitators to empowered, safe sexual health | 4 themes influencing adolescents discussed: sexual health knowledge, relationships with the self and others, access to quality sexual health resources, and alcohol use/abuse. |
| Survival analysis and prognostic factors of timing of first childbirth among women in Nigeria | Fagbamigbe et al. [39] | 2016 | Nigeria | The cross-sectional (repeated) High | 38,948 women aged 15–49 years were identified as eligible for individual interviews | Educational empowerment | The dependent variable in this study was age at first child birth while region and geographical zones of residence, education, religion, residence and ethnicity were the independent variables. | Median survival time to first birth (years): 27 (higher education) 18 (no formal education), adjusted hazard ratio (3.36 95%CI (3.17, 3.55) among women with no formal education compared to those with higher education. Other significant factors include residence, age of 1st marriage, religion, ethnicity, use of contraceptives |
| Socio-cultural factors influencing adolescent pregnancy in rural Nepal | Shrestha S. et al. [40] | 2002 | Nepal | Retrospective Fair | 575 adolescent mothers (aged under 19 years at first pregnancy). Comparing 575 mature mothers | Community and educational empowerment | Socio-economic factors are presented in relation to their influence on pregnancy. | Comparatively adolescents had parents/elders decide majority of adolescent marriages |
| Perceptions of contraception, non-protection and induced abortion among a sample of urban Swedish adolescent girls: Focus group discussions | Thorsen et al. [41] | 2006 | Sweden | Qualitative (4 focus group discussions) Fair | 16 urban adolescent girls aged 15–18 years. | Educational empowerment | Attitudes toward contraception, induced abortion and non-protection | Themes were: a) contraception: need for accessibility and affordability b) induced abortion: increased rate linked with younger sexual initiation, c) non-protection: alcohol use, partners reluctant to use condoms, common sex abuse, need for quality sex education in school. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nkhoma, D.E.; Lin, C.-P.; Katengeza, H.L.; Soko, C.J.; Estinfort, W.; Wang, Y.-C.; Juan, S.-H.; Jian, W.-S.; Iqbal, U. Girls’ Empowerment and Adolescent Pregnancy: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 1664. https://doi.org/10.3390/ijerph17051664
Nkhoma DE, Lin C-P, Katengeza HL, Soko CJ, Estinfort W, Wang Y-C, Juan S-H, Jian W-S, Iqbal U. Girls’ Empowerment and Adolescent Pregnancy: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(5):1664. https://doi.org/10.3390/ijerph17051664
Chicago/Turabian StyleNkhoma, Dumisani Enricho, Chia-Ping Lin, Hexin Latumer Katengeza, Charles Jenya Soko, Wanda Estinfort, Yao-Chin Wang, Shing-Hwa Juan, Wen-Shan Jian, and Usman Iqbal. 2020. "Girls’ Empowerment and Adolescent Pregnancy: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 5: 1664. https://doi.org/10.3390/ijerph17051664
APA StyleNkhoma, D. E., Lin, C.-P., Katengeza, H. L., Soko, C. J., Estinfort, W., Wang, Y.-C., Juan, S.-H., Jian, W.-S., & Iqbal, U. (2020). Girls’ Empowerment and Adolescent Pregnancy: A Systematic Review. International Journal of Environmental Research and Public Health, 17(5), 1664. https://doi.org/10.3390/ijerph17051664