Mothers’ Healthcare Autonomy, Maternal-Health Utilization and Healthcare for Children under-3 Years: Analysis of the Nigeria DHS Data (2008–2018)


Abstract
:1. Introduction
2. Methods
2.1. Data Source and Study Design
2.2. Sample Selection Criteria
2.3. Outcome Variables
2.4. Independent Variables
2.5. Covariates
2.6. Statistical Analysis
2.7. Ethical Standards Disclosure:
3. Results
3.1. Sample Characteristics
3.2. Univariate and Bivariate Analysis
3.3. Regression Result
3.3.1. Association between Mother’s Health Autonomy, Healthcare Utilization and Child’s Immunization
3.3.2. Association between Mother’s Health Autonomy, Healthcare Utilization and Treatment of Diarrhoea
3.3.3. Association between Mother’s Health Autonomy, Healthcare Utilization and Treatment of Fever
3.3.4. Association between Mother’s Health Autonomy, Healthcare Utilization and Treatment of ARI
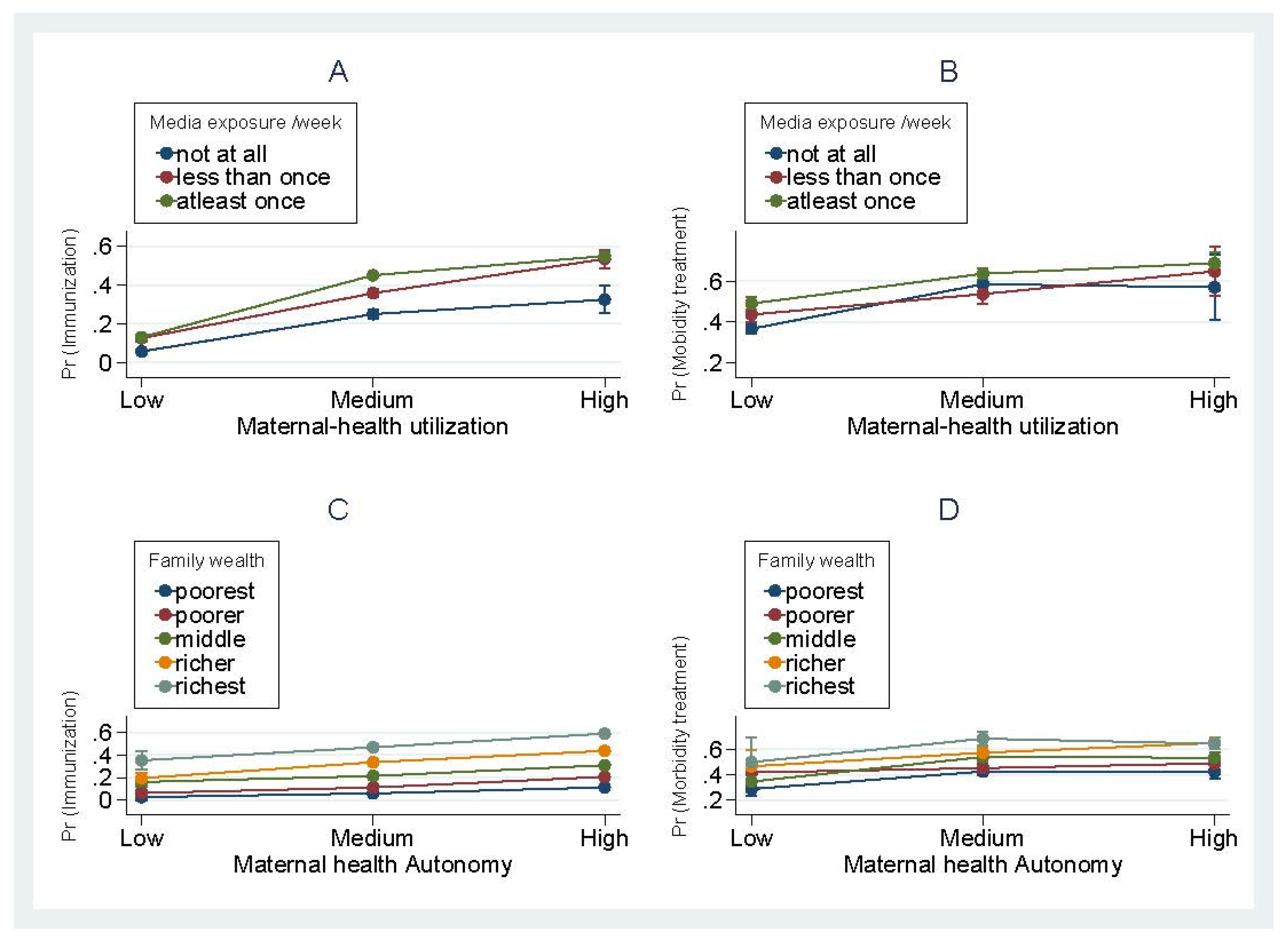
3.3.5. Interactions Effect
4. Discussion
4.1. Summary of Results
4.2. Relevance of Result
4.3. Relationship between Maternal Healthcare Utilization and Child Healthcare
4.4. Policy Implication
4.5. Strength and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Availability of data and materials
Appendix A


{kind=link}
{kind=link}
| Variables | Immunization± | Diarrhoea | Fever | ARI | ||||
|---|---|---|---|---|---|---|---|---|
| AOR | CI | AOR | CI | AOR | CI | AOR | CI | |
| Health Autonomy (B = Low) | ||||||||
| substantial | 1.53 *** | (1.12–2.11) | 1.08 | (0.82–1.43) | 1.53 *** | (1.15–2.05) | 1.65 ** | (1.09–2.52) |
| High | 1.87 *** | (1.34–2.62) | 1.16 | (0.83–1.62) | 1.51 ** | (1.09–2.10) | 1.24 | (0.78–1.99) |
| Health Utilization (B = Low) | ||||||||
| Medium | 3.53 *** | (2.82–4.41) | 1.25 * | (0.96–1.61) | 1.89 *** | (1.47–2.43) | 1.63 *** | (1.21–2.21) |
| High | 5.61 *** | (4.01–7.84) | 1.46 | (0.81–2.63) | 2.21 *** | (1.43–3.41) | 2.67 *** | (1.45–4.91) |
| Observations | 16694 | 4047 | 4973 | 1575 | ||||
| Number of groups | 1295 | 892 | 1037 | 665 | ||||
| Immunization± | Diarrhoea | Fever | ARI | |||||
|---|---|---|---|---|---|---|---|---|
| AOR | CI | AOR | CI | AOR | CI | AOR | CI | |
| Health Autonomy(B = Low) | ||||||||
| substantial | 1.49 *** | (1.11–2.01) | 1.19 | (0.87–1.62) | 1.47 ** | (1.06–2.04) | 1.56 * | (0.93–2.62) |
| High | 1.64 *** | (1.20–2.24) | 1.04 | (0.71–1.50) | 1.28 | (0.89–1.85) | 1.13 | (0.65–1.97) |
| Health Utilization (B = Low) | ||||||||
| Medium | 3.65 *** | (2.95–4.51) | 1.24 | (0.92–1.68) | 2.03 *** | (1.52–2.70) | 2.11 *** | (1.33–3.34) |
| High | 5.33 *** | (3.96–7.17) | 1.59 | (0.80–3.17) | 3.64 *** | (2.14–6.20) | 5.07 *** | (1.97–13.06) |
| Observations | 18119 | 3535 | 4151 | 1342 | ||||
| Number of groups | 904 | 728 | 841 | 537 | ||||
References
- WHO. Children: Reducing Mortality. Available online: https://www.who.int/news-room/fact-sheets/detail/children-reducing-mortality (accessed on 2 January 2020).
- Ahuru, R.R. The influence of women empowerment on maternal and childcare use in Nigeria. Int. J. Healthc. Manag. 2019, 1–10. [Google Scholar] [CrossRef]
- National Population Commission (NPC) [Nigeria] and ICF International. Nigeria Demographic and Health Survey 2018. NPC and ICF international. Abuja, Nigeria, and Rockville, Maryland, USA. 2019. Available online: http://measuredhs.com/publications/publication-sr171-summary-reports-key-findings.cfm (accessed on 10 December 2019).
- Federal Ministry of Health. National Child Health Policy; Federal Ministry of Health: Abuja, Nigeria, 2006. [Google Scholar]
- UNICEF Nigeria. The Children- Maternal and Child Health. Available online: https://www.unicef.org/children_1926.html (accessed on 4 March 2020).
- Dagnew, A.B.; Tewabe, T.; Murugan, R. Level of modern health care seeking behaviors among mothers having under five children in Dangila town, north West Ethiopia, 2016: A cross sectional study. Ital. J. Pediatr. 2018, 44, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Okafor, I.P.; Dolapo, D.C.; Onigbogi, M.O.; Iloabuchi, I.G. Rural-urban disparities in maternal immunization knowledge and childhood health-seeking behavior in Nigeria: A mixed method study. Afr. Health Sci. 2014, 14, 339–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, M. The effect of maternal decisional authority on children’s vaccination in East Asia. PLoS ONE 2018, 13, 1–11. [Google Scholar] [CrossRef]
- Woldemicael, G. Do Women with Higher Autonomy Seek More Maternal and Child Health-Care. In Stockholm Research Reports in Demography; Stock Univ Dept Sociol: Stockholm, Sweden, 2007; pp. 1–28. [Google Scholar]
- Malhotra, C.; Malhotra, R.; Østbye, T.; Subramanian, S.V. Maternal autonomy and child health care utilization in India: Results from the national family health survey. Asia Pacific J. Public Heal. 2014, 26, 401–413. [Google Scholar] [CrossRef]
- Akinyemi, J.O.; Banda, P.; De Wet, N.; Akosile, A.E.; Odimegwu, C.O. Household relationships and healthcare seeking behaviour for common childhood illnesses in sub-Saharan Africa: A cross-national mixed effects analysis. BMC Health Serv. Res. 2019, 19, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Carlson, G.J.; Kordas, K.; Murray-Kolb, L.E. Associations between women’s autonomy and child nutritional status: A review of the literature. Matern. Child Nutr. 2015, 11, 452–482. [Google Scholar] [CrossRef]
- Cunningham, K.; Ruel, M.; Ferguson, E.; Uauy, R. Women’s empowerment and child nutritional status in South Asia: A synthesis of the literature. Matern Child Nutr. 2015, 11, 1–19. [Google Scholar] [CrossRef]
- Oluchi, S.E.; Manaf, R.A.; Ismail, S.; Udeani, T.K. Predictors of health-seeking behavior for fever cases among caregivers of under-five children in malaria-endemic area of Imo State, Nigeria. Int. J. Environ. Res. Public Health 2019, 16, 3752. [Google Scholar] [CrossRef] [Green Version]
- Abdulkadir, M.B.; Ibraheem, R.M.; Johnson, W.B.R. Sociodemographic and clinical determinants of time to care-seeking among febrile children under-five in North-Central Nigeria. Oman Med. J. 2015, 30, 331–335. [Google Scholar] [CrossRef]
- Falola, T.O.; Kirk-Greene, M.; Hamilton, A.; Ade Ajayi, J.F.; Udo, R.K. Nigeria. Encyclopædia Britannica. Available online: https://www.britannica.com/place/Nigeria (accessed on 27 November 2019).
- Morakinyo, O.M.; Fagbamigbe, A.F. Neonatal, infant and under-five mortalities in Nigeria: An examination of trends and drivers (2003–2013). PLoS ONE 2017, 12, e0182990. [Google Scholar] [CrossRef] [Green Version]
- UNESCO. Education Literacy Rate. Available online: http://data.uis.unesco.org/ (accessed on 4 December 2019).
- National Population Commission (NPC) [Nigeria] and ICF International. Nigeria Demographic and Health Survey 2008. NPC and ICF international Abuja, Nigeria, and Rockville, Maryland, USA. 2009. Available online: http://measuredhs.com/publications/publication-sr171-summary-reports-key-findings.cfm (accessed on 10 December 2019).
- National Population Commission (NPC) [Nigeria] and ICF International. Nigeria Demographic and Health Survey 2013. NPC and ICF international Abuja, Nigeria, and Rockville, Maryland, USA. 2014. Available online: http://measuredhs.com/publications/publication-sr171-summary-reports-key-findings.cfm (accessed on 10 December 2019).
- UNICEF—World Health Organisation. Oral Rehydration Salts—Production of the new ORS. UNICEF, World Health Organisation. 2016. Available online: http://whqlibdoc.who.int/hq/2006/WHO_FCH_CAH_06.1.pdf?ua=1 (accessed on 12 January 2020).
- Kayode, G.A.; Adekanmbi, V.T.; Uthman, O.A. Risk factors and a predictive model for under-five mortality in Nigeria: Evidence from Nigeria demographic and health survey. BMC Pregnancy Childbirth 2012, 12, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simieneh, M.M.; Mengistu, M.Y.; Gelagay, A.A.; Gebeyehu, M.T. Mothers’ health care seeking behavior and associated factors for common childhood illnesses, Northwest Ethiopia: Community based cross-sectional study. BMC Health Serv. Res. 2019, 19, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Mukiira, C.; Ibisomi, L. Health care seeking practices of caregivers of children under 5 with diarrhea in two informal settlements in Nairobi, Kenya. J. Child Heal Care. 2015, 19, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Pratley, P. Associations between quantitative measures of women’s empowerment and access to care and health status for mothers and their children: A systematic review of evidence from the developing world. Soc. Sci. Med. 2016, 169, 119–131. [Google Scholar] [CrossRef]
- Liu, X. Applied Ordinal Logistic Regression Using StataApplied Ordinal Logistic Regression Using Stata: From Single-Level to Multilevel Modeling; Sage Publications: London, UK; New Delhi, India, 2015; pp. 461–491. [Google Scholar]
- Andersen, R.M. National health surveys and the behavioral model of health services use. Med. Care. 2008, 46, 647–653. [Google Scholar] [CrossRef]
- Henry, V.D. Northern Nigeria Maternal, Newborn and Child Health Programme: Selected Analyses from Population-Based Baseline Survey. Open Demogr. J. 2011, 4, 11–21. [Google Scholar] [CrossRef]
- Halim, N.; Bohara, A.K.; Ruan, X. Healthy mothers, healthy children: Does maternal demand for antenatal care matter for child health in Nepal? Health Policy Plan 2011, 26, 242–256. [Google Scholar] [CrossRef] [Green Version]
- Masangwi, S.; Ferguson, N.; Grimason, A.; Morse, T.; Kazembe, L. Care-seeking for diarrhoea in Southern Malawi: Attitudes, practices and implications for diarrhoea control. Int. J. Environ. Res. Public Health 2016, 13, 1140. [Google Scholar] [CrossRef] [Green Version]
- Charyeva, Z.; Cannon, M.; Oguntunde, O.; Garba, A.M.; Sambisa, W.; Bassi, A.P.; Ibrahim, M.A.; Danladi, S.E.; Lawal, N. Reducing the burden of diarrhea among children under five years old: Lessons learned from oral rehydration therapy corner program implementation in Northern Nigeria. J. Heal Popul. Nutr. 2015, 34, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Ratzan, S.C.; Parker, R.M. Health literacy. Natl. Libr. Med. Curr. Bibliogr. Med. Bethesda Natl. Institutes Heal US Dep. Heal Hum. Serv. 2000. Available online: https://www.nlm.nih.gov/archive/20061214/pubs/cbm/hliteracy.html (accessed on 4 March 2020).
- Schrauben, S.J.; Wiebe, D.J. Health literacy assessment in developing countries: A case study in Zambia. Health Promot. Int. 2017, 32, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Onwujekwe, O.; Obi, F.; Ichoku, H.; Ezumah, N.; Okeke, C.; Ezenwaka, U.; Uzochukwu, B.; Wang, H. Assessment of a Free Maternal and Child Health Program and the Prospects for Program Re-Activation and Scale-Up using a New Health Fund in Nigeria. Niger. J. Clin. Pract. 2019, 22, 1516. [Google Scholar] [PubMed]

| Total | Year | |||||
|---|---|---|---|---|---|---|
| 2008 | 2013 | 2018 | ||||
| N = | % | % | % | % | p-Value | |
| Gender | 0.803 | |||||
| Male | 17176 | 50.7 | 50.2 | 50.8 | 51.5 | |
| Female | 16693 | 49.3 | 49.8 | 49.2 | 48.5 | |
| Birth order | 0.001 | |||||
| First born | 5541 | 16.4 | 16.2 | 16.6 | 16.2 | |
| 2–3rd | 11162 | 33.0 | 32.9 | 32.7 | 33.8 | |
| 4–6th | 11234 | 33.2 | 33.0 | 32.9 | 34.3 | |
| 7th+ | 5932 | 17.5 | 18.0 | 17.8 | 15.7 | |
| Birth weight | 0.000 | |||||
| Small | 5003 | 14.9 | 15.5 | 15.0 | 13.5 | |
| Average | 13996 | 41.8 | 37.9 | 40.7 | 52.6 | |
| Large | 14523 | 43.3 | 46.6 | 44.3 | 33.9 | |
| Method of delivery | 0.000 | |||||
| Normal | 33046 | 98.0 | 98.5 | 97.9 | 97.0 | |
| Caesarean session | 687 | 2.0 | 1.6 | 2.1 | 3.0 | |
| Mother’s Age | 0.000 | |||||
| 15–19 | 2044 | 6.0 | 6.9 | 5.8 | 4.9 | |
| 20–24 | 6912 | 20.4 | 20.7 | 20.6 | 19.2 | |
| 25–29 | 9770 | 28.9 | 29.1 | 28.4 | 29.4 | |
| 30–34 | 7319 | 21.6 | 20.7 | 21.8 | 23.2 | |
| 35+ | 7824 | 23.1 | 22.7 | 23.4 | 23.3 | |
| Mother’s Education | 0.000 | |||||
| no education | 16420 | 48.5 | 52.0 | 48.5 | 41.0 | |
| primary | 6649 | 19.6 | 21.9 | 19.3 | 15.6 | |
| secondary | 8624 | 25.5 | 21.3 | 25.7 | 33.9 | |
| higher | 2176 | 6.4 | 4.9 | 6.5 | 9.5 | |
| Mother’s EM/Week | 0.000 | |||||
| None | 11784 | 34.8 | 34.6 | 35.0 | 35.1 | |
| less than once | 6359 | 18.8 | 13.4 | 21.8 | 23.2 | |
| at least once | 15700 | 46.4 | 52.1 | 43.2 | 41.8 | |
| Father’s Education | 0.000 | |||||
| no education | 12854 | 38.4 | 41.9 | 38.2 | 31.3 | |
| primary | 6407 | 19.1 | 21.3 | 19.3 | 14.2 | |
| secondary | 9948 | 29.7 | 26.2 | 29.2 | 38.6 | |
| higher | 4275 | 12.8 | 10.6 | 13.4 | 15.9 | |
| Family wealth | 0.000 | |||||
| poorest | 8251 | 24.4 | 27.1 | 23.3 | 21.1 | |
| poor | 7685 | 22.7 | 23.6 | 23.0 | 19.9 | |
| middle | 6433 | 19.0 | 18.2 | 18.8 | 21.2 | |
| richer | 6076 | 17.9 | 16.7 | 18.1 | 20.2 | |
| richest | 5424 | 16.0 | 14.4 | 16.8 | 17.6 | |
| DMF | 0.000 | |||||
| Big problem | 11759 | 34.8 | 40.2 | 32.4 | 29.1 | |
| not a big problem | 21997 | 65.2 | 59.8 | 67.6 | 71.0 | |
| Residency | 0.000 | |||||
| Urban | 10781 | 31.8 | 27.7 | 32.9 | 38.2 | |
| Rural | 23088 | 68.2 | 72.3 | 67.2 | 61.8 | |
| Geopolitical zone | 0.000 | |||||
| Northcentral | 5533 | 16.3 | 17.3 | 15.1 | 17.1 | |
| Northeast | 7481 | 22.1 | 23.9 | 21.6 | 19.4 | |
| Northwest | 10192 | 30.1 | 28.7 | 32.8 | 26.5 | |
| Southeast | 2962 | 8.8 | 7.9 | 7.8 | 12.9 | |
| Southsouth | 3530 | 10.4 | 10.2 | 10.8 | 10.1 | |
| Southwest | 4171 | 12.3 | 11.9 | 12.0 | 13.9 | |
| Immunization N = 16694 | Diarrhoea N = 4047 | |||||||||||||
| No | % | Yes | % | Total | % | χ2 P-Value | No | % | Yes | % | Total | % | χ2 P-Value | |
| Health autonomy | <0.01 | <0.01 | ||||||||||||
| Low | 1674 | 13.1 | 145 | 3.7 | 1819 | 10.9 | 113 | 15.5 | 373 | 11.3 | 486 | 12.0 | ||
| Substantial | 7507 | 59.0 | 1739 | 43.9 | 9246 | 55.4 | 475 | 65.0 | 2022 | 60.3 | 2497 | 61.7 | ||
| High | 3548 | 27.9 | 2081 | 52.5 | 5629 | 33.7 | 143 | 19.6 | 921 | 27.8 | 1064 | 26.3 | ||
| Health utilization | <0.01 | <0.01 | ||||||||||||
| Low | 8464 | 66.5 | 848 | 21.4 | 9312 | 55.8 | 561 | 76.7 | 1999 | 60.3 | 2560 | 63.3 | ||
| Substantial | 3555 | 27.9 | 2309 | 58.2 | 5864 | 35.1 | 150 | 20.5 | 1112 | 33.5 | 1262 | 31.2 | ||
| High | 710 | 5.6 | 808 | 20.4 | 1518 | 9.1 | 20 | 2.7 | 205 | 6.2 | 225 | 5.6 | ||
| Fever N = 4973 | ARI N = 1575 | |||||||||||||
| No | % | Yes | % | Total | % | χ2 P-Value | No | % | Yes | % | Total | % | χ2 P-Value | |
| Health autonomy | <0.01 | <0.01 | ||||||||||||
| Low | 360 | 14.9 | 216 | 8.4 | 576 | 11.6 | 122 | 14.5 | 53 | 7.3 | 175 | 11.1 | ||
| Substantial | 1416 | 58.7 | 1483 | 58.0 | 2899 | 58.3 | 481 | 57.0 | 440 | 60.2 | 921 | 58.5 | ||
| High | 638 | 26.4 | 860 | 33.6 | 1498 | 30.1 | 241 | 28.6 | 238 | 32.6 | 479 | 30.5 | ||
| Health utilization | <0.01 | <0.01 | ||||||||||||
| Low | 1653 | 68.5 | 1263 | 49.4 | 2916 | 58.6 | 600 | 71.1 | 345 | 47.2 | 945 | 60.0 | ||
| Substantial | 643 | 26.6 | 1058 | 41.3 | 1701 | 34.2 | 216 | 25.6 | 321 | 43.9 | 537 | 34.1 | ||
| High | 118 | 4.9 | 238 | 9.3 | 356 | 7.2 | 28 | 3.3 | 65 | 8.9 | 93 | 5.9 | ||
| RANDOM EFFECT | Immunization | Diarrhoea | Fever | ARI | ||||
|---|---|---|---|---|---|---|---|---|
| CI | CI | CI | CI | |||||
| Variance at community level | 0.00 *** | (0.00–0.01) | 2.85 *** | (1.34–6.07) | 0.10 *** | (0.05–0.22) | 0.13 *** | (0.05–0.32) |
| Variance at Household | 2.46 *** | (1.82–3.32) | 1.30 ** | (1.04–1.63) | 1.57 *** | (1.19–2.06) | 1.67 *** | (1.15–2.43) |
| Log likelihood | −6880.2246 | −1788.5715 | −3065.34 | −934.90057 | ||||
| Model fit Statistics LR test | 272.25 *** | 11.49*** | 43.13 *** | 14.52 *** | ||||
| ICC from Null model: | ||||||||
| Community | 0.25 | (0.23–0.27) | 0.11 | (0.06–0.16) | 0.13 | (0.10–0.18) | 0.21 | (0.05–0.22) |
| Household | Community | 0.86 | (0.83–0.88) | 0.61 | (0.44–0.76) | 0.83 | (0.74–0.90) | 0.87 | (0.05–0.22) |
| Observations | 16694 | 4047 | 4973 | 1575 | ||||
| Number of groups | 1295 | 892 | 1037 | 665 | ||||
| Variables | Immunization | Diarrhoea | Fever | ARI | ||||
|---|---|---|---|---|---|---|---|---|
| AOR | CI | AOR | CI | AOR | CI | AOR | CI | |
| Survey year | ||||||||
| ref = 2008 | ||||||||
| 2013 | 1.63 *** | (1.36–1.95) | 1.42 *** | (1.12–1.78) | 0.32 *** | (0.24–0.44) | 0.44 *** | (0.33–0.60) |
| 2018 | 2.33 *** | (1.84–2.94) | 1.06 | (0.82–1.37) | 2.43 *** | (1.82–3.25) | 1.98 *** | (1.41–2.77) |
| Health Autonomy | ||||||||
| ref = Low | ||||||||
| Medium | 1.53 *** | (1.12–2.11) | 1.08 | (0.82–1.43) | 1.53 *** | (1.15–2.05) | 1.65 ** | (1.09–2.52) |
| High | 1.87 *** | (1.34–2.62) | 1.16 | (0.83–1.62) | 1.51 ** | (1.09–2.10) | 1.24 | (0.78–1.99) |
| Health Utilization | ||||||||
| ref = Low | ||||||||
| Medium | 3.53 *** | (2.82–4.41) | 1.25 * | (0.96–1.61) | 1.89 *** | (1.47–2.43) | 1.63 *** | (1.21–2.21) |
| High | 5.61 *** | (4.01–7.84) | 1.46 | (0.81–2.63) | 2.21 *** | (1.43–3.41) | 2.67 *** | (1.45–4.91) |
| Child Level Covariates | ||||||||
| Gender | ||||||||
| ref = Male | ||||||||
| Female | 1.02 | (0.89–1.18) | 0.91 | (0.76–1.10) | 0.99 | (0.84–1.16) | 0.97 | (0.76–1.23) |
| Birth order | ||||||||
| ref = First born | ||||||||
| 2–3rd | 0.72 *** | (0.57–0.92) | 1.11 | (0.80–1.54) | 0.88 | (0.66–1.18) | 0.97 | (0.64–1.47) |
| 4–6th | 0.55 *** | (0.42–0.73) | 1.15 | (0.79–1.67) | 0.90 | (0.65–1.25) | 0.78 | (0.48–1.27) |
| 7th+ | 0.52 *** | (0.36–0.74) | 1.45 | (0.90–2.33) | 0.93 | (0.62–1.39) | 0.80 | (0.44–1.44) |
| PWB | ||||||||
| ref = Small | ||||||||
| Average | 1.37 ** | (1.08–1.74) | 0.96 | (0.75–1.22) | 1.31 ** | (1.02–1.67) | 1.51 ** | (1.07–2.13) |
| Large | 1.29 ** | (1.01–1.64) | 1.26 * | (0.98–1.63) | 1.57 *** | (1.22–2.04) | 2.17 *** | (1.54–3.08) |
| Delivery method | ||||||||
| Ref = normal birth | ||||||||
| C & S | 1.84 *** | (1.18–2.86) | 0.55 | (0.22–1.42) | 0.96 | (0.50–1.86) | 0.95 | (0.36–2.55) |
| Maternal and Household Level Covariates | ||||||||
| Mothers’ age | ||||||||
| Ref = 15–19 years | ||||||||
| 20–24 | 1.70 ** | (1.08–2.68) | 0.83 | (0.55–1.23) | 1.52 ** | (1.01–2.29) | 1.58 | (0.89–2.80) |
| 25–29 | 2.75 *** | (1.72–4.40) | 0.96 | (0.62–1.48) | 1.41 | (0.92–2.17) | 1.50 | (0.82–2.75) |
| 30–34 | 3.17 *** | (1.92–5.21) | 1.13 | (0.69–1.85) | 1.56 * | (0.98–2.50) | 1.78 * | (0.92–3.44) |
| 35+ | 3.55 *** | (2.11–5.97) | 1.07 | (0.63–1.82) | 1.48 | (0.90–2.43) | 1.77 | (0.88–3.56) |
| Mothers’ education | ||||||||
| ref= No education | ||||||||
| primary | 1.87 *** | (1.47–2.37) | 1.04 | (0.78–1.38) | 1.57 *** | (1.19–2.07) | 1.29 | (0.90–1.85) |
| secondary | 2.89 *** | (2.19–3.80) | 1.10 | (0.75–1.63) | 1.58 *** | (1.13–2.20) | 1.42 | (0.92–2.20) |
| higher | 2.78 *** | (1.89–4.08) | 1.18 | (0.52–2.71) | 2.68 *** | (1.50–4.79) | 1.63 | (0.74–3.59) |
| Media exposure/Week | ||||||||
| ref = None | ||||||||
| less than once | 1.29 ** | (1.02–1.63) | 1.09 | (0.84–1.43) | 1.04 | (0.81–1.33) | 1.27 | (0.87–1.85) |
| at least once | 1.51 *** | (1.22–1.87) | 1.25 * | (0.98–1.60) | 1.46 *** | (1.16–1.85) | 1.69 *** | (1.24–2.30) |
| Father’s education | ||||||||
| ref = low | ||||||||
| primary | 1.86 *** | (1.44–2.42) | 1.33 ** | (1.00–1.76) | 1.11 | (0.86–1.44) | 0.78 | (0.53–1.15) |
| secondary | 1.98 *** | (1.52–2.56) | 1.49 ** | (1.08–2.06) | 1.21 | (0.92–1.60) | 0.94 | (0.64–1.38) |
| higher | 2.57 *** | (1.87–3.54) | 1.62 ** | (1.00–2.63) | 1.34 | (0.92–1.94) | 2.05 *** | (1.22–3.43) |
| Family wealth | ||||||||
| ref = poorest | ||||||||
| poor | 1.43 ** | (1.08–1.88) | 1.23 * | (0.97–1.56) | 1.34 ** | (1.05–1.71) | 0.98 | (0.69–1.39) |
| middle | 1.89 *** | (1.41–2.53) | 1.91 *** | (1.34–2.72) | 1.30 * | (0.98–1.75) | 0.87 | (0.58–1.31) |
| richer | 2.62 *** | (1.88–3.67) | 1.28 | (0.83–1.98) | 1.83 *** | (1.26–2.68) | 1.17 | (0.70–1.98) |
| richest | 4.02 *** | (2.69–6.02) | 1.91 ** | (1.01–3.60) | 1.91 *** | (1.19–3.08) | 1.19 | (0.60–2.36) |
| Community Level Covariates | ||||||||
| Residency | ||||||||
| ref = Urban | ||||||||
| Rural | 0.85 | (0.70–1.04) | 0.81 | (0.59–1.10) | 1.40 ** | (1.08–1.80) | 1.21 | (0.84–1.74) |
| Geopolitical zone | ||||||||
| ref = Northcentral | ||||||||
| North east | 0.57 *** | (0.43–0.75) | 0.82 | (0.57–1.17) | 1.14 | (0.84–1.55) | 0.74 | (0.49–1.11) |
| Northwest | 0.28 *** | (0.21–0.38) | 0.74 | (0.50–1.07) | 1.47 ** | (1.06–2.05) | 1.00 | (0.62–1.64) |
| Southeast | 1.15 | (0.84–1.57) | 1.80 | (0.86–3.77) | 0.84 | (0.56–1.26) | 0.97 | (0.54–1.72) |
| Southsouth | 1.20 | (0.90–1.62) | 0.68 | (0.36–1.29) | 0.71 * | (0.47–1.05) | 1.10 | (0.63–1.90) |
| Southwest | 0.54 *** | (0.40–0.73) | 0.60* | (0.34–1.04) | 0.66 * | (0.41–1.05) | 0.52 | (0.24–1.14) |
| Distance to medical facility | ||||||||
| (ref = Big problem) | ||||||||
| Not a problem | 1.21 ** | (1.02–1.45) | 1.28 ** | (1.04–1.59) | 1.31 *** | (1.08–1.59) | 1.58 *** | (1.21–2.08) |
| Constant (Intercept) | 143.29 *** | (22.82–99.51) | 1.56 | (0.38–6.46) | 5.99 * | (0.94–38.08) | 1.00 | (1.00–1.00) |
| Observations | 16694 | 4047 | 4973 | 1575 | ||||
| Number of groups | 1295 | 892 | 1037 | 665 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ariyo, T.; Jiang, Q. Mothers’ Healthcare Autonomy, Maternal-Health Utilization and Healthcare for Children under-3 Years: Analysis of the Nigeria DHS Data (2008–2018). Int. J. Environ. Res. Public Health 2020, 17, 1816. https://doi.org/10.3390/ijerph17061816
Ariyo T, Jiang Q. Mothers’ Healthcare Autonomy, Maternal-Health Utilization and Healthcare for Children under-3 Years: Analysis of the Nigeria DHS Data (2008–2018). International Journal of Environmental Research and Public Health. 2020; 17(6):1816. https://doi.org/10.3390/ijerph17061816
Chicago/Turabian StyleAriyo, Tolulope, and Quanbao Jiang. 2020. "Mothers’ Healthcare Autonomy, Maternal-Health Utilization and Healthcare for Children under-3 Years: Analysis of the Nigeria DHS Data (2008–2018)" International Journal of Environmental Research and Public Health 17, no. 6: 1816. https://doi.org/10.3390/ijerph17061816
APA StyleAriyo, T., & Jiang, Q. (2020). Mothers’ Healthcare Autonomy, Maternal-Health Utilization and Healthcare for Children under-3 Years: Analysis of the Nigeria DHS Data (2008–2018). International Journal of Environmental Research and Public Health, 17(6), 1816. https://doi.org/10.3390/ijerph17061816