Impacts of Emergency Medical Technician Configurations on Outcomes of Patients with Out-Of-Hospital Cardiac Arrest




Abstract
1. Background
2. Materials and Methods
2.1. Study Design
2.2. EMS in Tainan City
2.3. Definition of Crew Number, ALS Team, and EMT-Paramedic Ratio
2.4. Exposure and Outcome
2.5. Statistical Analysis
2.6. Ethical Consideration
3. Results
3.1. Patient Population
3.2. Clinical Predictors of Sustained ROSC
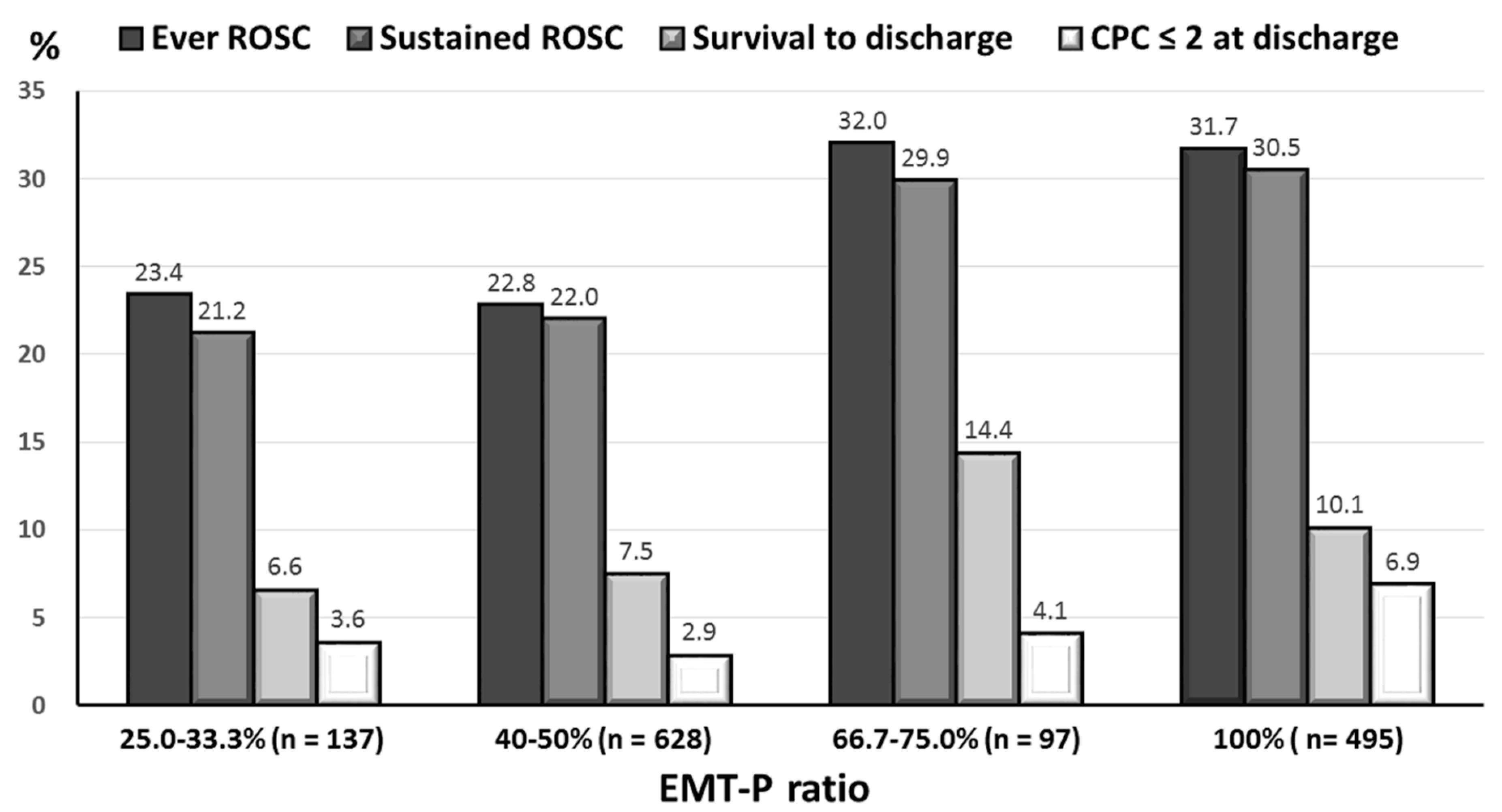
3.3. The Impact of Crew Number and EMT-Paramedic Ratio on Patient Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Sasson, C.; Rogers, M.A.; Dahl, J.; Kellermann, A.L. Predictors of survival from out-of-hospital cardiac arrest: A systematic review and meta-analysis. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 63–81. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Despres, J.P.; Fullerton, H.J.; et al. Heart disease and stroke statistics—2015 update: A report from the American Heart Association. Circulation 2015, 131, e29–e322. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.Y.; Wang, J.Y.; Teng, N.C.; Chao, T.T.; Tsai, S.L.; Chen, C.L.; Hsu, J.Y.; Wu, C.P.; Lai, C.C.; Chen, L. The secular trends in the incidence rate and outcomes of out-of-hospital cardiac arrest in Taiwan—A nationwide population-based study. PLoS ONE 2015, 10, e0122675. [Google Scholar] [CrossRef] [PubMed]
- Kleinman, M.E.; Brennan, E.E.; Goldberger, Z.D.; Swor, R.A.; Terry, M.; Bobrow, B.J.; Gazmuri, R.J.; Travers, A.H.; Rea, T. Part 5: Adult Basic Life Support and Cardiopulmonary Resuscitation Quality: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132, S414–S435. [Google Scholar] [CrossRef]
- Link, M.S.; Berkow, L.C.; Kudenchuk, P.J.; Halperin, H.R.; Hess, E.P.; Moitra, V.K.; Heumar, R.W.; O’Neil, B.J.; Paxton, J.H.; Silvers, S.M.; et al. Part 7: Adult Advanced Cardiovascular Life Support: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132, S444–S464. [Google Scholar] [CrossRef]
- Bakalos, G.; Mamali, M.; Komninos, C.; Koukou, E.; Tsantilas, A.; Tzima, S.; Rosenberg, T. Advanced life support versus basic life support in the pre-hospital setting: A meta-analysis. Resuscitation 2011, 82, 1130–1137. [Google Scholar] [CrossRef]
- Hasegawa, K.; Hiraide, A.; Chang, Y.; Brown, D.F. Association of prehospital advanced airway management with neurologic outcome and survival in patients with out-of-hospital cardiac arrest. JAMA 2013, 309, 257–266. [Google Scholar] [CrossRef]
- Sanghavi, P.; Jena, A.B.; Newhouse, J.P.; Zaslavsky, A.M. Outcomes after out-of-hospital cardiac arrest treated by basic vs advanced life support. JAMA Intern. Med. 2015, 175, 196–204. [Google Scholar] [CrossRef]
- Hagihara, A.; Onozuka, D.; Nagata, T.; Hasegawa, M. Effects of advanced life support on patients who suffered cardiac arrest outside of hospital and were defibrillated. Am. J. Emerg. Med. 2018, 36, 73–78. [Google Scholar] [CrossRef]
- Training Course of EMT-Intermediate. Ministry of Justice, Republic of China, 2008. Available online: https://law.moj.gov.tw/LawClass/LawGetFile.ashx?FileId=0000234403&lan=C (accessed on 15 July 2019).
- Training Course of EMT-Paramedic. Ministry of Justice, Republic of China, 2008. Available online: https://law.moj.gov.tw/LawClass/LawGetFile.ashx?FileId=0000234404&lan=C. (accessed on 15 July 2019).
- Regulations Governing Emergency Medical Technicians. Ministry of Justice, Republic of China, 2008. Available online: https://law.moj.gov.tw/LawClass/LawAll.aspx?pcode=L0020141 (accessed on 15 July 2019).
- Kajino, K.; Kitamura, T.; Iwami, T.; Daya, M.; Ong, M.E.H.; Nishiyama, C.; Sakai, T.; Tanigawa, K.S.; Hayashida, S.; Nishiuchi, T.; et al. Impact of the number of on-scene emergency life-saving technicians and outcomes from out-of-hospital cardiac arrest in Osaka City. Resuscitation 2014, 85, 59–64. [Google Scholar] [CrossRef]
- Warren, S.A.; Prince, D.K.; Huszti, E.; Rea, T.D.; Fitzpatrick, A.L.; Andrusiek, D.L.; Darling, S.; Morrison, L.J.; Vilke, G.M.; Nichol, G.; et al. Volume versus outcome: More emergency medical services personnel on-scene and increased survival after out-of-hospital cardiac arrest. Resuscitation 2015, 94, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Eschmann, N.M.; Pirrallo, R.G.; Aufderheide, T.P.; Lerner, E.B. The association between emergency medical services staffing patterns and out-of-hospital cardiac arrest survival. Prehosp. Emerg. Care 2010, 14, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, S.; Oshima, K.; Aoki, M.; Miyazaki, D.; Sakurai, A.; Tahara, Y.; Nagao, K.; Yonemoto, N.; Yaguchi, A.; Morimura, N. Does the number of emergency medical technicians affect the neurological outcome of patients with out-of-hospital cardiac arrest? Am. J. Emerg. Med. 2017, 35, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.T.; Chiang, W.C.; Hsieh, M.J.; Huang, E.P.C.; Yang, W.S.; Chien, Y.C.; Wang, Y.C.; Lee, B.C.; Sim, S.S.; Tsai, K.C.; et al. The effect of the number and level of emergency medical technicians on patient outcomes following out of hospital cardiac arrest in Taipei. Resuscitation 2018, 122, 48–53. [Google Scholar] [CrossRef]
- Dawson, D.E.; Brown, W.E., Jr.; Harwell, T.S. Assessment of nationally registered emergency medical technician certification training in the United States: The LEADS Project. Longitudinal Emergency Medical Technician Attributes Demo-graphic Study. Prehosp. Emerg. Care 2003, 7, 114–119. [Google Scholar] [CrossRef]
- Travers, A.H.; Rea, T.D.; Bobrow, B.J.; Edeison, D.P.; Berg, R.A.; Sayre, M.R.; Berg, M.D.; Chameides, L.; O’Connor, R.E.; Swor, R.A. Part 4: CPR overview: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010, 122, S676–S684. [Google Scholar] [CrossRef]
- Chiang, W.C.; Ko, P.C.; Wang, H.C.; Yang, C.W.; Shih, F.Y.; Hsiung, K.H.; Ma, M.H.M. EMS in Taiwan: Past, present, and future. Resuscitation 2009, 80, 9–13. [Google Scholar] [CrossRef]
- Wang, H.E.; Schmicker, R.H.; Daya, M.R.; Stephen, S.W.; Idris, A.H.; Carldon, J.N.; Colella, M.R.; Herren, H.; Hansen, M.; Richmond, N.J.; et al. Effect of a Strategy of Initial Laryngeal Tube Insertion vs Endotracheal Intubation on 72-Hour Survival in Adults With Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial. JAMA 2018, 320, 769–778. [Google Scholar] [CrossRef]
- Lin, C.H.; Chiang, W.C.; Ma, M.H.; Wu, S.Y.; Tsai, M.C.; Chi, C.H. Use of automated external defibrillators in patients with traumatic out-of-hospital cardiac arrest. Resuscitation 2013, 84, 586–591. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Royston, P.; Moons, K.G.; Altman, D.G.; Vergouwe, Y. Prognosis and prognostic research: Developing a prognostic model. BMJ 2009, 338, b604. [Google Scholar] [CrossRef] [PubMed]
- Gold, L.S.; Eisenberg, M.S. The effect of paramedic experience on survival from cardiac arrest. Prehosp. Emerg. Care 2009, 13, 341–344. [Google Scholar] [CrossRef]
- Bayley, R.; Weinger, M.; Meador, S.; Slovis, C. Impact of ambulance crew configuration on simulated cardiac arrest resuscitation. Prehosp. Emerg. Care 2008, 12, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Hunziker, S.; Johansson, A.C.; Tschan, F.; Semmer, N.K.; Rock, L.; Howell, M.D.; Marsch, S. Teamwork and leadership in cardiopulmonary resuscitation. J. Am. Coll. Cardiol. 2011, 57, 2381–2388. [Google Scholar] [CrossRef] [PubMed]
- Finn, J.C.; Bhanji, F.; Lockey, A.; Monsieurs, K.; Frengley, R.; Iwami, T.; Lang, E.; Ma, M.H.M.; Mancini, M.E.; McNeil, M.A.; et al. Part 8: Education, implementation, and teams: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Resuscitation 2015, 95, e203–e224. [Google Scholar] [CrossRef]
- Perkins, G.D.; Ji, C.; Deakin, C.D.; Quinn, T.; Nolan, J.P.; Scomparin, C.; Regan, S.; Slowther, A.; Pocock, H.; Black, J.J.M.; et al. A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. N. Engl. J. Med. 2018, 379, 711–721. [Google Scholar] [CrossRef]
- O’Keeffe, C.; Nicholl, J.; Turner, J.; Goodacre, S. Role of ambulance response times in the survival of patients with out-of-hospital cardiac arrest. Emerg. Med. J. 2011, 28, 703–706. [Google Scholar] [CrossRef]
- Shin, S.D.; Kitamura, T.; Hwang, S.S.; Kajino, K.; Song, K.J.; Ro, Y.S.; Nischiuchi, T.; Iwami, T. Association between resuscitation time interval at the scene and neurological outcome after out-of-hospital cardiac arrest in two Asian cities. Resuscitation 2014, 85, 203–210. [Google Scholar] [CrossRef]
- Geri, G.; Gilgan, J.; Wu, W.; Vijendira, S.; Ziegler, C.; Drennan, I.R.; Morrison, L.; Lin, S. Does transport time of out-of-hospital cardiac arrest patients matter? A systematic review and meta-analysis. Resuscitation 2017, 115, 96–101. [Google Scholar] [CrossRef]
- Swor, R.A.; Jackson, R.E.; Compton, S.; Domeier, R.; Zalenski, R.; Honeycutt, L.; Kuhn, G.J.; Frederiksen, S.; Pascual, R.G. Cardiac arrest in private locations: Different strategies are needed to improve outcome. Resuscitation 2003, 58, 171–176. [Google Scholar] [CrossRef]
- Chiang, W.C.; Chen, S.Y.; Ko, P.C.; Hsieh, M.J.; Wang, H.C.; Huang, E.P.C.; Yang, C.W.; Chong, K.M.; Chen, W.T.; Chen, S.Y.; et al. Prehospital intravenous epinephrine may boost survival of patients with traumatic cardiac arrest: A retrospective cohort study. Scand. J. Trauma Resusc. Emerg. Med. 2015, 23, 102. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.H.; Chou, N.K.; Becker, L.B.; Lin, J.W.; Yu, H.Y.; Chi, N.H.; Hunag, S.C.; Ko, W.J.; Wang, S.S.; Tseng, L.J.; et al. Improved outcome of extracorporeal cardiopulmonary resuscitation for out-of-hospital cardiac arrest—A comparison with that for extracorporeal rescue for in-hospital cardiac arrest. Resuscitation 2014, 85, 1219–1224. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.P.; Soar, J.; Cariou, A.; Cronberg, T.; Moulaert, V.R.; Deakin, C.D.; Bottiger, B.W.; Friberg, H.; Sunde, K.; Sandroni, C. European Resuscitation Council and European Society of Intensive Care Medicine 2015 guidelines for post-resuscitation care. Intensive Care Med. 2015, 41, 2039–2056. [Google Scholar] [CrossRef] [PubMed]
- Dyson, K.; Bray, J.E.; Smith, K.; Bernard, S.; Straney, L.; Finn, J. Paramedic Exposure to Out-of-Hospital Cardiac Arrest Resuscitation Is Associated With Patient Survival. Circ. Cardiovasc. Qual. Outcomes 2016, 9, 154–160. [Google Scholar] [CrossRef]
- Tuttle, J.E.; Hubble, M.W. Paramedic Out-of-hospital Cardiac Arrest Case Volume Is a Predictor of Return of Spontaneous Circulation. West J. Emerg. Med. 2018, 19, 654–659. [Google Scholar] [CrossRef]
- Lin, C.H.; Ng, Y.Y.; Chiang, W.C.; Karim, S.A.; Shin, S.D.; Tanaka, H.; Nishiuchi, T.; Kajino, K.; Khunkhlai, N.; Ma, M.H.; et al. Variation of current protocols for managing out-of-hospital cardiac arrest in prehospital settings among Asian countries. J. Formos. Med. Assoc. 2016, 115, 628–638. [Google Scholar] [CrossRef]
- Lu, C.H.; Fang, P.H.; Lin, C.H. Dispatcher-assisted cardiopulmonary resuscitation for traumatic patients with out-of-hospital cardiac arrest. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 97. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Patient Number (%) in Varied Groups of EMT-Paramedic Ratio | γ | p Value | |||
|---|---|---|---|---|---|---|
| 25.0–33.3% n = 137 | 40.0–50.0% n = 628 | 66.7–75.0% n = 97 | 100.0% n = 495 | |||
| Younger adults (<65 years) | 60 (43.8) | 209 (33.3) | 42 (43.3) | 196 (39.6) | −0.40 | 0.60 |
| Male | 92 (67.2) | 404 (64.3) | 68 (70.1) | 320 (64.6) | 0 | 1.00 |
| Witnessed cardiac arrest | 66 (48.2) | 315 (50.2) | 50 (51.5) | 230 (46.5) | −0.20 | 0.80 |
| Bystander CPR | 48 (35.0) | 211 (33.6) | 37 (38.1) | 148 (29.9) | −0.40 | 0.60 |
| Prehospital ROSC | 14 (10.2) | 22 (3.5) | 7 (7.2) | 48 (9.7) | −0.20 | 0.80 |
| EMS time interval | ||||||
| Response time ≤ 5 min | 81 (59.1) | 437 (69.6) | 48 (49.5) | 275 (55.6) | −0.60 | 0.40 |
| Scene time ≤ 8 min | 95 (69.3) | 461 (73.4) | 74 (96.3) | 383 (77.4) | 0.80 | 0.20 |
| Transport time ≤ 5 min | 95 (69.3) | 377 (60.0) | 45 (46.4) | 186 (37.6) | −1.00 | 0.01 |
| Indoor location of arrest | 127 (92.7) | 575 (91.6) | 83 (85.6) | 437 (88.3) | −0.80 | 0.20 |
| Transport to medical centers | 56 (40.9) | 330 (52.5) | 50 (51.5) | 277 (56.0) | 0.80 | 0.20 |
| Prehospital treatment | ||||||
| Laryngeal mask airway | 114 (83.2) | 514 (81.8) | 83 (85.6) | 423 (85.5) | 0.60 | 0.40 |
| Defibrillation | 22 (16.1) | 92 (14.6) | 16 (16.2) | 103 (20.8) | 0.80 | 0.20 |
| Intravenous epinephrine | 9 (6.6) | 24 (3.8) | 28 (28.9) | 127 (25.7) | 0.60 | 0.40 |
| Comorbidities | ||||||
| Hypertension | 48 (35.0) | 221 (35.2) | 30 (30.9) | 184 (37.2) | 0.40 | 0.60 |
| Diabetes mellitus | 37 (27.0) | 186 (29.6) | 21 (21.6) | 136 (27.5) | 0 | 1.00 |
| Heart disease | 39 (28.5) | 149 (23.7) | 19 (19.6) | 132 (26.7) | −0.40 | 0.60 |
| Chronic kidney disease | 14 (10.2) | 75 (11.9) | 10 (10.3) | 77 (15.6) | 0.80 | 0.20 |
| Neurological disease | 26 (19.0) | 100 (15.9) | 19 (19.6) | 67 (13.5) | −0.40 | 0.60 |
| Hemato-oncological disease | 13 (9.5) | 70 (11.1) | 12 (12.4) | 69 (13.9) | 1.00 | 0.01 |
| COPD | 10 (7.3) | 37 (5.9) | 14 (14.4) | 34 (6.9) | 0 | 1.00 |
| Chronic liver disease | 6 (4.4) | 23 (3.7) | 7 (7.2) | 17 (3.4) | −0.40 | 0.60 |
| Psychological disease | 5 (3.6) | 11 (1.8) | 5 (5.2) | 13 (2.6) | 0 | 1.00 |
| Outcomes | ||||||
| Ever ROSC | 32 (23.4) | 143 (22.8) | 31 (32.0) | 157 (31.7) | 0.60 | 0.40 |
| Sustained (≥ 2 h) ROSC | 29 (21.2) | 138 (22.0) | 29 (29.9) | 151 (30.5) | 1.00 | 0.01 |
| Survive to discharge | 9 (6.6) | 47 (7.5) | 14 (14.4) | 50 (10.1) | 0.80 | 0.20 |
| Favorable neurologic status at discharge * | 5 (3.6) | 18 (2.9) | 4 (4.1) | 34 (6.9) | 0.80 | 0.20 |
| Variables | Patient No (%) with ROSC | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|---|
| Yes, n = 347 | No, n = 1010 | OR (95% CI) | p Value | Adjusted OR (95% CI) | p Value | |
| Younger adults (<65 years) | 165 (47.6) | 342 (33.9) | 1.75 (1.39−2.27) | <0.01 | 1.76 (1.33−2.33) | <0.01 |
| Witnessed cardiac arrest | 243 (70.0) | 418 (41.4) | 3.31 (2.55−4.30) | <0.01 | 2.86 (2.16−3.78) | <0.01 |
| Bystander cardiopulmonary resuscitation | 225 (64.8) | 688 (68.1) | 0.86 (0.67−1.12) | 0.26 | NS | NS |
| EMS response time ≤ 5 min | 198 (57.1) | 643 (63.7) | 0.76 (0.59−0.97) | 0.03 | NS | NS |
| Prehospital ROSC | 75 (21.6) | 16 (1.6) | 17.13 (9.82−29.87) | <0.01 | 12.48 (7.03−22.16) | <0.01 |
| Indoor location of arrest | 298 (85.9) | 924 (91.5) | 0.57 (0.39−0.82) | <0.01 | NS | NS |
| Prehospital management | ||||||
| Defibrillation | 94 (27.1) | 139 (13.8) | 2.33 (1.73−3.13) | <0.01 | 1.45 (1.03−2.04) | 0.03 |
| Intravenous epinephrine | 60 (17.3) | 128 (12.7) | 1.44 (1.03−2.01) | 0.03 | NS | NS |
| Comorbidities | ||||||
| Diabetes mellitus | 114 (32.9) | 266 (26.3) | 1.37 (1.05−1.78) | 0.02 | 1.48 (1.11−1.99) | <0.01 |
| Heart disease | 101 (29.1) | 238 (23.6) | 1.33 (1.01−1.75) | 0.04 | NS | NS |
| Chronic kidney disease | 54 (15.6) | 122 (12.1) | 1.34 (0.95−1.90) | 0.09 | NS | NS |
| Variables | Sustained ROSC | Survival at Discharge | CPC ≤ 2 at Discharge | |||
|---|---|---|---|---|---|---|
| Adjusted OR * (95% CI) | p Value | Adjusted OR * (95% CI) | p Value | Adjusted OR * (95% CI) | p Value | |
| EMT number (averagely increased one person) | ||||||
| Total | 1.02 (0.76−1.37) | 0.89 | 1.03 (0.68−1.57) | 0.89 | 1.19 (0.68−2.09) | 0.55 |
| EMT-intermediate | 1.26 (0.99−1.55) | 0.06 | 1.13 (0.84−1.52) | 0.44 | 1.44 (0.94−2.20) | 0.09 |
| EMT-paramedic | 1.49 (1.14−1.93) | 0.003 | 1.23 (0.82−1.84) | 0.32 | 1.76 (0.98−3.15) | 0.06 |
| EMT-paramedic ratio (averagely increased the ratio of 10%) | 1.08 (1.02−1.13) | <0.01 | 1.03 (0.95−1.11) | 0.54 | 1.12 (1.01−1.26) | 0.048 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fang, P.-H.; Lin, Y.-Y.; Lu, C.-H.; Lee, C.-C.; Lin, C.-H. Impacts of Emergency Medical Technician Configurations on Outcomes of Patients with Out-Of-Hospital Cardiac Arrest. Int. J. Environ. Res. Public Health 2020, 17, 1930. https://doi.org/10.3390/ijerph17061930
Fang P-H, Lin Y-Y, Lu C-H, Lee C-C, Lin C-H. Impacts of Emergency Medical Technician Configurations on Outcomes of Patients with Out-Of-Hospital Cardiac Arrest. International Journal of Environmental Research and Public Health. 2020; 17(6):1930. https://doi.org/10.3390/ijerph17061930
Chicago/Turabian StyleFang, Pin-Hui, Yu-Yuan Lin, Chien-Hsin Lu, Ching-Chi Lee, and Chih-Hao Lin. 2020. "Impacts of Emergency Medical Technician Configurations on Outcomes of Patients with Out-Of-Hospital Cardiac Arrest" International Journal of Environmental Research and Public Health 17, no. 6: 1930. https://doi.org/10.3390/ijerph17061930
APA StyleFang, P.-H., Lin, Y.-Y., Lu, C.-H., Lee, C.-C., & Lin, C.-H. (2020). Impacts of Emergency Medical Technician Configurations on Outcomes of Patients with Out-Of-Hospital Cardiac Arrest. International Journal of Environmental Research and Public Health, 17(6), 1930. https://doi.org/10.3390/ijerph17061930