Organizational Health Literacy in Facilities for People with Disabilities: First Results of an Explorative Qualitative and Quantitative Study

 , ,
, , 
Abstract
:1. Introduction
1.1. Organizational HL
1.2. Measurement of OHL, Interventions and Guides
1.3. State of the Art on OHL
1.4. Research Questions
- How can the HLHO-10-instrument be appropriately adapted for its use in facilities for people with disabilities?
- What is the degree of each of the 10 attributes of HLHO in facilities for people with disabilities? (quantitative study)
- What is the definition and role of OHL in facilities for people with disabilities? (qualitative study)
2. Data and Methods
2.1. The Quantitative Study
2.1.1. Database
2.1.2. Description of Instruments and Variables
2.1.3. Study Sample
2.1.4. Data Analysis
2.2. The Qualitative Study
2.2.1. Database
2.2.2. Interview Guide
2.2.3. Study Sample
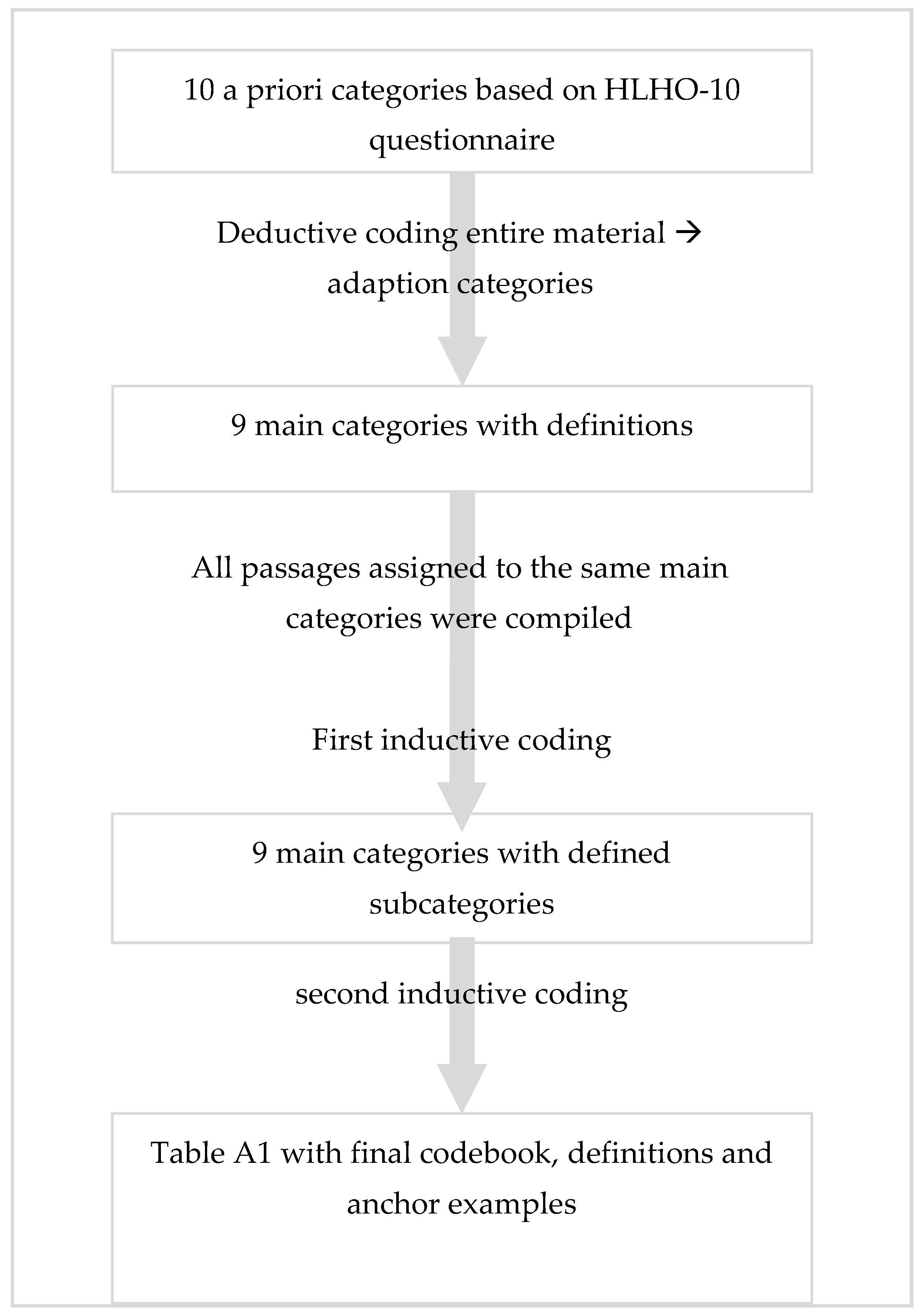
2.2.4. Analysis
3. Results
3.1. Results of the Quantitative Study
3.2. Results of the Qualitative Study
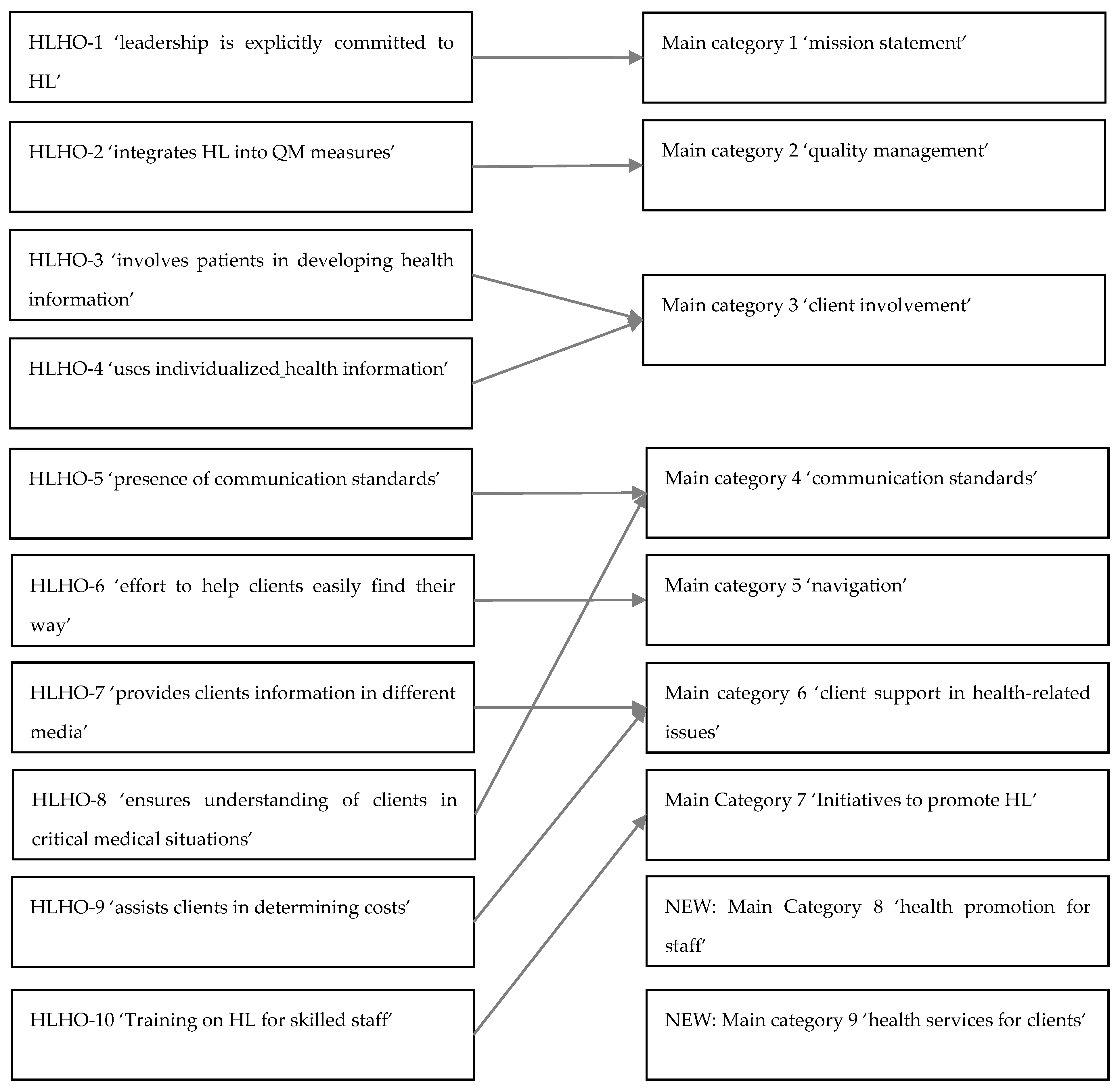
3.2.1. Understanding the OHL of Facilities for People with Disabilities
3.2.2. Main Category 1: Mission Statement
3.2.3. Main Category 2: Quality Management
3.2.4. Main Category 3: Client Involvement in Developing Health Information
3.2.5. Main Category 4: Communication Standards
3.2.6. Main Category 5: Navigation
3.2.7. Main Category 6: Client Support in Health-Related Issues
3.2.8. Main Category 7: Initiatives to Promote HL
3.2.9. Main Category 8: Health Promotion for Staff
3.2.10. Main Category 9: Health Services for Clients
4. Discussion
4.1. Summary of Quantitative and Qualitative Results
4.2. Discussion of Quantitative and Qualitative Results
5. Limitations
6. Implications to Strengthen OHL in Facilities for People with Disabilities
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Category | Subcategories | Definition | Anchor Examples |
|---|---|---|---|
| 1. Mission statement | The facility’s leadership is explicitly committed to HL (e.g., mission statement, HR planning). | ||
| 1.1. High level of HL in mission statement | Strongly anchored in mission statement or concept, part of processes, defined objectives, or liabilities | ‘It’s an integral part of our concept.’ (FPD 4, person B) | |
| 1.2. Medium level of HL in mission statement | HL is anchored to an extent in the mission statement; not as a binding objective or element in the concept; plays a relatively insignificant role or has a different designation | ‘But in writing I have to say that it’s only a small part.’ (FPD 1) | |
| 1.3. HL is not part of the mission statement | HL is not structurally embedded; the concept does not include any special requirements or rules regarding health | ‘(…) There are no completely integrated (…) no real processes anywhere that are a real part of the concept. That just isn’t happening.’ (FPD 3, person A) | |
| 1.4. Implicit anchoring and implementation of HL in mission statement | HL without conceptual requirements or binding objectives; health-relevant offerings or measures are voluntary and out of the interest of the skilled staff; part of a philosophical mission statement based on anthroposophical principles and holistic spiritual background | ‘There are many everyday processes that I would say might unconsciously lead to this way of health behavior.’ (FPD 3, person B) | |
| 2. Quality management | Is HL part of quality management in your facility? | ||
| 2.1. Quality management in general | QM in crisis situations: ensures understanding of the situation, routine or standard processes; QM in working conditions, work safety; measures to improve and monitor working conditions | ‘We have (…) trained first-aiders (…) and we have an internal direct number. So by a key combination on the phone (…) you start an internal emergency call when fast action is needed and first of all the first-aiders are on site and then it actually sets off a relatively fast chain reaction.’ (FPD 3 person B) | |
| 2.2. HL in Quality management | HL in quality management for working and living together; relevance of HL in the facility regarding possible conflict in operations or care; measures to prevent or availability of contact points; quality management measures that are aimed at ensuring medical care or supporting HL during medical interventions | ‘We have two colleagues who are trained in de-escalation techniques and how already told, they share their knowledge with the skilled staff. All employees are required to take part in this training.’ (FPD 3, person B) | |
| 3. Clients involvement | Are clients involved in developing health information in your facility? | ||
| 3.1. Participatory | Clients are involved in developing health information. | - | |
| 3.2. Non-participatory | Clients are not involved in developing health information. | ‘Up to now, this has mainly been due to the intuition of the employees. So, in principle, the employees always have a feeling for how my clients tick, what their interests are.’ (FPD 8) | |
| 4. Communication standards | Are there communication standards that ensure that clients understood critical information (e.g., translators, pause to allow time to think before responding, encourage questions)? | ||
| 4.1. Implementation | Design of the communication between skilled staff and clients | ‘So, that always has to be individual and it depends on the person.’ (FPD 3, person B) | |
| 4.2. Influences | Factors influencing the communicative situation, such as critical situations or individual clients’ limitations | ‘So, we always have appointments with the clients. Time appointments. (…) And during this time (…) There are always situations that make you see that you should really stop for a moment and really take more time for a topic. But I really don’t have the time because I already have to go somewhere else. It’s also a question of relationships whether you can put something off to another day. (…) The better your relationship is to a client, the better the possibility to communicate in this area. It’s very much about trust. (FPD 5) | |
| 4.3. Basics | Use of communication technologies and media | ‘Violence free communication and easy language.’ (FPD 5); ‘Use picture.’ (FPD 2) | |
| 5. Navigation | Is an effort made in your facility to help clients easily find their way (e.g., signs, information staff)? | ||
| 5.1. High level of navigation aids | A number of different aids to facilitate navigation are used, e.g., signs in plain language, pictograms, color codes, clearly designed homepage, flyers, information staff | ‘We have a homepage with an app for your phone. So that you can use it on your phone. We have an area with easy language. We have signs in the building. We have prepared all light switches that they can be used by people in a wheelchair. Barrier-free access to all rooms. In each work area, we have a flyer which we provide for initial interviews (…) Then there is a general flyer. Then we have regular open house days and celebrations for our skilled staff and clients.’ (FPD 5) | |
| 5.2 Medium level of navigation aids | There is at least one feature/tool that serves as a guide; for example, signs in plain language, pictograms, color codes, clearly designed homepage, flyer or information staff | ‘And I think we have a very strong presence of staff offering guidance. (…) Guidance is, I think, relatively easy. (…) We don’t even have decent signs. Every external remembers this. But every person in care will be able to tell you where the wool workshop is. There is much (…) always this presence from people, someone is always there.’ (FPD 2) | |
| 5.3 No navigation aids | There are no aids in the facility that explicitly serve as guidance | ‘I would say, at the moment there isn’t a guidance system and it’s not clear at all, so in terms of the homepage and all.’ (FPD 1) | |
| 5.4 Examples of navigation aids | Structures or systems that serve as guidance in the facility | ‘Homepage’; ‘plain language app’; ‘flyers for each area.’; ‘Signs.’ (FPD 5) | |
| 5.5 Wishes and prospects for an improved guidance system | Improvements to the system are planned or expressed as desirable | ‘We are working on what offerings we have in this area, what offers our homepage for navigation already, what’s missing, what we need, what relatives need, what our clients need, what outsiders need.’ (FPD 8) | |
| 6. Client support in health-related issues | In your facility, do you offer support in determining costs such as additional payments for medications or other treatments relative to health? | ||
| 6.1 Offerings/services | Offerings that are supported, e.g., doctor appointments, health offerings | ‘As a rule, we arrange an appointment with the doctor together with the clients. We call there together or the person calls and I help out depending on what the client can do. But the initiative has to be there. I can’t force anyone to go anywhere.’ (FPD 5) | |
| 6.2 Type/kind of support | Design of the support mechanisms | ‘That’s very diverse. It’s as individual as the people with us, as individual as the solutions. There are people who can hardly tell us about their illness, their pain, or other things. You have to observe very carefully to even see if they aren’t feeling well. And there are others that complain the whole day long about pain they don’t even have. You have to handle things on an individual basis and respond its.’ (FPD 7) | |
| 6.3 Media use for health-related topics | Auditory (audio media), visual (print media), audio-visual (media with images or videos and sound), multimodal (media combining language and images) | Language, audio material (FPD 8); ‘There’s a pictogram for every condition: stomach aches, fever, everything. We have a little box in the rehabilitation workshop for those clients who are able to show us what’s wrong with them.’ (FPD 3, person B) | |
| 7. Initiatives to promote HL | Are skilled staff in your facility trained in HL? | ||
| 7.1 Client-related training | Offerings training and further education related to special diseases or activities affecting clients; opportunities and resources for training in HL communication | ‘We have different departments such as care sector, assistant area. Assistants are trained, they work individualized how the clients prefer. And we, in assisted living, where I work, some clients I care for have a special condition like diabetes or trouble with their heart. I have a client who has multiple such as problems with her kidneys, and I went to special training courses.’ (FPD 5) | |
| 7.2 Staff-related training | Opportunities for skilled staff to inform themselves about HL, support for personally managing occupational health risks or developing a healthier lifestyle; measures, rules, or regulations with the aim of supporting skilled staff health | ‘Yes, well, I think, of course, self-management is a good thing, to have a good perception of oneself, that is, good provision for oneself, and team discussions and development discussions with skilled staff is a bit of a thing we do.’ (FPD 2) | |
| 7.3 Wishes and ideas about training | Concepts or ideas about an ideal HLO regarding skilled staff training; wishes for the establishment or expansion of training, or potential for development | ‘If it would be a concert of desire, I think it would be important for every skilled staff to have more training in communication to learn how I can best reach my clients.’ (FPD 8) | |
| 7.4 Planning and implementation | Modalities of training: type of training opportunities for skilled staff, optional or mandatory, frequency, regularity, external or internal training, dissemination in team, type of availability, implementation in HR development plans, origins and development of offerings | ‘We have an internal training network and if something is in the program [brochure] then you can apply to take part in it if you want to.’ (FPD 3, person B) | |
| 8. Health promoting for staff | All offerings to improve health in skilled staff | ||
| 8.1 Prevention and health promotion | Offerings to prevent, delay, or reduce the risk of health impairment as well as means for the prevention or early detection of disease; offerings to strengthen health and knowledge about improving health, and also to increase health-preserving factors; salutogenetic approach | ‘The sheltered workshop offers a sport activity free of charge at the gym of your choice in your preferred region. You can just join it, which is already a very big offer, of course. Employers expect there will be less downtime because of back problems or whatever happens when you don’t get enough exercise. That’s really something.’ (FPD 4, person A) | |
| 8.2 Disease management and health care | Offerings to support coping with the stress brought about by disease; psychological or physical support in coping with a disease and its consequences; support for offerings in health organizations, products, and services available within the health system and whose use involves cooperation with health insurance companies or other types of support | ‘B2: And I think that’s a really great thing, and then there’s also such an offer for the non-disabled employees that you can turn to your colleagues even after traumatizing experiences at work. (…) B1: [We have| Colleagues as first-aiders (…)’ (FPD 3, person B1 and B2) | |
| 8.3 Wishes and ideas | Specific wishes about new, more, or other health offerings; ideas about what offerings should be provided; need for changes or development; actual plans to restructure offerings; expanding or providing initial offerings for skilled staff | ‘We should see if we could do and embed things like this without consulting with the board. To simply bring things into life more freely and faster and to implement them as well. Yes.’ (FPD 1) | |
| 9. Health services for clients | All offerings to improve health for clients | ||
| 9.1 Prevention and health promotion | Offerings to prevent, delay, or reduce the risk of health impairment as well as means for the prevention or early detection of disease; offerings to strengthen health and knowledge about improving health, and also to increase health-promoting (environmental) factors; salutogenetic approach | ‘Nevertheless, in sheltered workshops there are health promoting offerings like exercise, eating the right food we’re looking at here.’ (FPD 7) | |
| 9.2 Health promotion and health care | Offerings to support coping with the stress brought about by disease; psychological or physical support in coping with disease and its consequences; support for offerings in health organizations, products, and services available within the health system and whose use involves cooperation with health insurance companies or other types of support | ‘If an individual (client) needs, for example, cancer treatment, then of course we look into how they can be dealt with individually, what has to happen, what else can be done, whether it’s possible to use external offerings. To go with them. Are there doctors they will come to us if the client can’t leave our premises?’ (FPD 8) | |
| 9.3 Wishes and ideas | Specific wishes about new, more, or other health offerings; ideas about what offerings should be provided; need for changes or development; actual plans to restructure offerings; expanding or providing initial offerings for clients | ‘(…) We have a recreation room. That’s where we’ll have this relaxation group. (…) We also want to offer a day group, expand it significantly and offer a larger spectrum. Where things like (…) health literacy, sport offers, nutrition offers play a more significant role. So, those are all ideas that are being developed. (…) There are already scheduled days, there are already staff being hired, but it’s all starting first in the summer.’ (FPD 1) |
References
- Nationaler Aktionsplan Gesundheitskompetenz. Available online: www.nap-gesundheitskompetenz.de (accessed on 20 April 2020).
- Sørensen, K.; van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Nationaler Aktionsplan Gesundheitskompetenz. In Die Gesundheitskompetenz in Deutschland Stärken; Schaeffer, D.; Hurrelmann, K.; Bauer, U.; Kolpatzik, K. (Eds.) KomPart: Berlin, Germany, 2018. [Google Scholar]
- Pelikan, J.M.; Ganahl, K.; Röthlin, F. Gesundheitskompetenz Verbessern. In Handlungsoptionen für Die Sozialversicherung; Oberösterreichische Gebietskrankenkasse: Linz, Austria, 2013. [Google Scholar]
- Kickbusch, I.; Pelikan, J.; Apfel, F.; Tsouros, A.D. Health Literacy. The Solid Facts; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Pelikan, J.M.; Ganahl, K. Die europäische Gesundheitskompetenz-Studie: Konzept, Instrument und ausgewählte Ergebnisse. In Health literacy: Forschungsstand und Perspektiven; Schaeffer, D., Pelikan, J.M., Eds.; Hogrefe: Bern, Switzerland, 2017; pp. 93–125. [Google Scholar]
- Quenzel, G.; Schaeffer, D. Health Literacy—Gesundheitskompetenz Vulnerabler Bevölkerungsgruppen. Ergebnisbericht; Universität Bielefeld: Bielefeld, Germany, 2016. [Google Scholar]
- Rathmann, K.; Nellen, C. Gesundheitskompetenz von Menschen mit Behinderung. Prävent. Gesundh. 2019, 9, 923. [Google Scholar] [CrossRef]
- Hollar, D.W., Jr.; Rowland, J. Promoting health literacy for people with disabilities and clinicians through a teamwork model. J. Fam. Strengths 2015, 15, 5. [Google Scholar]
- Geukes, C.; Bruland, D.; Latteck, Ä.-D. Health literacy in people with intellectual disabilities: A mixed-method literature review. Kontakt 2018, 20, 416–423. [Google Scholar] [CrossRef] [Green Version]
- Zweiter Teilhabebericht der Bundesregierung über die Lebenslagen von Menschen mit Beeinträchtigungen. Teilhabe—Beeinträchtigung—Behinderung; Bundesministerium für Arbeit und Soziales(BMAS), Ed.; Bundesministerium für Arbeit und Soziales: Bonn, Germany, 2016. [Google Scholar]
- Gesundheit und Gesellschaftliche Teilhabe von Menschen mit Lernschwierigkeiten; Bundesnetzwerk Bürgerschaftliches Engagement (BBE) (Ed.) Bundesnetzwerk Bürgerschaftliches Engagement: Berlin, Germany, 2015. [Google Scholar]
- Wetzel, L.D.; Rathmann, K. Inanspruchnahme und wahrgenommene Barrieren im Gesundheitswesen bei Menschen mit Behinderung in Deutschland: Ergebnisse der GEDA 2014/2015-EHIS. Prävent. Gesundh. 2019, 81, 662. [Google Scholar]
- Chinn, D. Critical health literacy: A review and critical analysis. Soc. Sci. Med. 2011, 73, 60–67. [Google Scholar] [CrossRef]
- Abel, T.; Sommerhalder, K. Gesundheitskompetenz/Health Literacy: Das Konzept und seine Operationalisierung. Bundesgesundheitsblatt Gesundh. Gesundh. 2015, 58, 923–929. [Google Scholar] [CrossRef] [PubMed]
- Wieczorek, C.C.; Ganahl, K.; Dietscher, C. Improving Organizational Health Literacy in Extracurricular Youth Work Settings. Health Lit. Res. Pract. 2017, 1, 233–238. [Google Scholar] [CrossRef] [Green Version]
- Palumbo, R.; Annarumma, C.; Musella, M. Exploring the meaningfulness of healthcare organizations: A multiple case study. Int. J. Public Sect. Manag. 2017, 30, 503–518. [Google Scholar] [CrossRef]
- Annarumma, C.; Palumbo, R. Contextualizing Health Literacy to Health Care Organizations. J. Health Manag. 2016, 18, 611–624. [Google Scholar] [CrossRef]
- Chinn, D. Review of Interventions to Enhance the Health Communication of People With Intellectual Disabilities: A Communicative Health Literacy Perspective. J. Appl. Res. Intellect. Disabil. 2017, 30, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ernstmann, N.; Halbach, S.; Kowalski, C.; Pfaff, H.; Ansmann, L. Measuring attributes of health literate health care organizations from the patients’ perspective: Development and validation of a questionnaire to assess health literacy-sensitive communication (HL-COM). Z. Evid. Fortbild. Qual. Gesundhwes. 2017, 121, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Brach, C.; Keller, D.; Hernandez, L.M.; Baur, C.; Parker, R.; Dreyer, B.; Schyve, P.; Lemerise, A.J.; Schillinger, D. Ten attributes of Health Literate Health Care Organizations. Discussion Paper. Institute of Medicine of the National Academies. Available online: https://nam.edu/wp-content/uploads/2015/06/BPH_Ten_HLit_Attributes.pdf (accessed on 11 September 2019).
- Brach, C. The Journey to Become a Health Literate Organization: A Snapshop of Health System Improvement. Stud. Health Technol. Inform. 2017, 240, 203–237. [Google Scholar] [PubMed]
- Hayran, O.; Özer, O. Organizational health literacy as a determinant of patient satisfaction. Public Health 2018, 163, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Adsul, P.; Wray, R.; Gautam, K.; Jupka, K.; Weaver, N.; Wilson, K. Becoming a health literate organization: Formative research results from healthcare organizations providing care for undeserved communities. Health Serv. Manage. Res. 2017, 30, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Stock, S.; Altin, S. Health Literate Healthcare Organizations and their Role in Future Healthcare. J. Nurs. Care 2015, 4, 1–3. [Google Scholar] [CrossRef]
- Pelikan, J.; Dietscher, C. Die Gesundheitskompetenz von Gesundheitseinrichtungen Entwickeln. Strategien und Beispiele; LBIHPR & ONGKG: Wien, Austria, 2015. [Google Scholar]
- Kowalski, C.; Lee, S.-Y.D.; Schmidt, A.; Wesselmann, S.; Wirtz, M.A.; Pfaff, H.; Ernstmann, N. The health literate health care organization 10 item questionnaire (HLHO-10): Development and validation. BMC Health Serv. Res. 2015, 15, 47. [Google Scholar] [CrossRef] [Green Version]
- Brega, A.G.; Barnard, J.; Mabachi, N.M.; Weiss, B.D.; DeWalt, D.A.; Brach, C.; Cifuentes, M.; Albright, K.; West, D.R. AHRQ Health Literacy Universal Precautions Toolkit, 2nd ed.; Colorado Health Outcomes Program: Aurora, CO, USA, 2015. [Google Scholar]
- Health Literacy Universal Precautions Toolkit; North Carolina Network Consortium and the Cecil G. Sheps Center for Health Services Research; DeWalt, D.A.; Callahan, L.F.; Hawk, V.H.; Broucksou, K.A.; Hink, A.; Rudd, R.; Brach, C. (Eds.) University of North Carolina at Chapel Hill: Chapel Hill, NC, USA, 2010. [Google Scholar]
- Dietscher, C.; Pelikan, J. Gesundheitskompetente Krankenbehandlungsorganisationen. Prävent. Gesundh. 2016, 11, 53–62. [Google Scholar] [CrossRef]
- Palumbo, R. Designing health-literate health care organization: A literature review. Health Serv. Manag. Res. 2016, 29, 79–87. [Google Scholar] [CrossRef]
- Farmanova, E.; Bonneville, L.; Bouchard, L. Organizational Health Literacy: Review of Theories, Frameworks, Guides, and Implementation Issues. Inquiry 2018, 55, 46958018757848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vamos, C.A.; Thompson, E.L.; Griner, S.B.; Liggett, L.G.; Daley, E.M. Applying Organizational Health Literacy to Maternal and Child Health. Matern. Child Health J. 2019, 23, 597–602. [Google Scholar] [CrossRef] [PubMed]
- Tempelmann, A.; Kolpatzik, K.; Ehrenreich, H.; Ströing, M.; Hans, C. Qualitätsorientierte Prävention und Gesundheitsförderung in Einrichtungen der Pflege: Das Projekt QualiPEP. Bundesgesundheitsblatt Gesundh. Gesundh. 2019, 62, 296–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tempelmann, A.; Ströing, M.; Ehrenreich, H.; Kolpatzik, K.; Hans, C. ‘QualiPEP’—Qualitätsorientierte Prävention und Gesundheitsförderung. In Pflege-Report 2019; Jacobs, K., Kuhlmey, A., Greß, S., Klauber, J., Schwinger, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Weaver, N.L.; Wray, R.J.; Zellin, S.; Gautam, K.; Jupka, K. Advancing organizational health literacy in health care organizations serving high-needs populations: A case study. J. Health Commun. 2012, 17 (Suppl. 3), 55–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, S.S.; Pisano, M.M.; Boone, A.L.; Baker, G.; Pers, Y.-M.; Pilotto, A.; Valsecchi, V.; Zora, S.; Zhang, X.; Fierloos, I.; et al. Evaluation Design of EFFICHRONIC: The Chronic Disease Self-Management Programme (CDSMP) Intervention for Citizens with a Low Socioeconomic Position. Int. J. Environ. Res. Public Health 2019, 16, 1883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lennox, N.; Taylor, M.; Rey-Conde, T.; Bain, C.; Boyle, F.M.; Purdie, D.M. Ask for it: Development of a health advocacy intervention for adults with intellectual disability and their general practitioners. Health Promot. Int. 2004, 19, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Anderson, P.; Harrison, O.; Cooper, C.; Jané-Llopis, E. Incentives for health. J. Health Commun. 2011, 16 (Suppl. 2), 107–133. [Google Scholar] [CrossRef]
- Greene, J.C.; Caracelli, V.J.; Garharn, W.F. Toward a conceptual framework for mixed method evaluation designs. In The Mixed Methods Reader; Plano Clark, V.L., Creswell, J.W., Eds.; Sage Publ: Los Angeles, CA, USA, 2008; pp. 119–148. ISBN 9781412951449. [Google Scholar]
- Kuckartz, U. Mixed Methods; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2014. [Google Scholar]
- Kruse, J.; Schmieder, C. Qualitative Interviewforschung. Ein integrativer Ansatz; Beltz Juventa: Weinheim, Germany, 2014. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Steinke, I. Kriterien Qualitativer Forschung. Ansätze zur Bewertung Qualitativ-Empirischer Sozialforschung; Juventa-Verl.: Weinheim, Germany, 1999. [Google Scholar]
- Kuckartz, U. Qualitative Inhaltsanalyse. Methoden, Praxis, Computerunterstützung, 4th ed.; Auflage; Beltz Juventa: Weinheim, Germany; Basel, Sweitzerland, 2018. [Google Scholar]
- Netzwerk Leichte Sprache. Die Regeln für Leichte Sprache. Available online: https://www.leichte-sprache.org/wp-content/uploads/2017/11/Regeln_Leichte_Sprache.pdf (accessed on 9 March 2020).
- Rosenberg, M.B. Speak Peace in a World of Conflict; Puddle Dancer Press: Encinitas, CA, USA, 2005. [Google Scholar]
- Kolpatzik, K. Gesundheitskompetenz im Fokus. Das Praxishandbuch; Kompart: Berlin, Germany, 2019. [Google Scholar]
- Roberts, N.J.; Partridge, M.R. Evaluation of a paper and electronic pictorial COPD action plan. Chron. Respir. Dis. 2011, 8, 31–40. [Google Scholar] [CrossRef]
- Chinn, D.; Homeyard, C. Easy read and accessible information for people with intellectual disabilities: Is it worth it? A meta-narrative literature review. Health Expect. 2017, 20, 1189–1200. [Google Scholar] [CrossRef] [Green Version]
- Yaneva, V. Easy-read Documents as a Gold Standard for Evaluation of Text Simplification Output. In Proceedings of the Student Research Workshop; INCOMA Ltd. Shoumen, BULGARIA: Hissar, India; Bulgaria, Balkans, 2015; pp. 30–36. [Google Scholar]
- Russell, L. Developing health resources with the help of people with Down syndrome. Learn. Disabil. Pract. 2006, 9, 16–18. [Google Scholar] [CrossRef]
- Tarleton, B. Writing it ourselves. Br. J. Learn. Disabil. 2005, 33, 65–69. [Google Scholar] [CrossRef]
- Goodwin, J.; Mason, V.; Williams, V.; Townsley, R. Easy Information about research: Getting the message out to people with learning disabilities. Br. J. Learn. Disabil. 2015, 43, 93–99. [Google Scholar] [CrossRef]
- Lewis, J.; Wood, B.; Cruickshank, S. Evaluation with Expectant and New Parents with Children from Pregnancy to Age 5 Years of CHANGE Re-Sources to Support Parents with Learning Disabilities. Available online: https://www.choiceforum.org/docs/enewpr.pdf (accessed on 20 April 2020).
- Geukes, C. Health Literacy und die Konstruktion von Gesundheit und Krankheit aus der Perspektive von älteren Menschen mit geistiger Behinderung. Forum Qual. Sozial./Forum Qual. Soc. Res. 2019, 20, 1–26. [Google Scholar] [CrossRef]
- Vockert, T.; Rathmann, K.; Dadaczynski, K. Die zielgruppenadäquate Erfassung der Gesundheitskompetenz in Leichter Sprache bei Menschen mit Behinderung im Setting der Behindertenhilfe: Ergebnisse einer Mixed-Methods-Studie. In Neue Ideen für mehr Gesundheit; Gemeinsame Jahrestagung der Deutschen Gesellschaft für Medizinische Soziologie (DGMS) und der Deutschen Gesellschaft für Sozialmedizin und Prävention, Ed.; Georg Thieme Verlag KG: New York, NY, USA, 2019. [Google Scholar]
- Groene, R.O.; Rudd, R.E. Results of a feasibility study to assess the health literacy environment: Navigation, written, and oral communication in 10 hospitals in Catalonia, Spain. J. Commun. Healthc. 2011, 4, 227–237. [Google Scholar] [CrossRef]
- Edwards, M.; Wood, F.; Davies, M.; Edwards, A. ‘Distributed health literacy’: Longitudinal qualitative analysis of the roles of health literacy mediators and social networks of people living with a long-term health condition. Health Expect. 2015, 18, 1180–1193. [Google Scholar] [CrossRef] [Green Version]
- Terhanian, G. How to Produce Credible, Trustworthy Information Through Internet-Based Survey Research. Paper Presented at the Annual Conference of the American Association for Public Opinion Research, Portland, OR, USA, 18–21 May 2000. [Google Scholar]
- Batinic, B.; Moser, K. Neue Befragungsmethoden für die Medienpsychologie: Online-Panels. Z. Für Medien. 2001, 13, 45–49. [Google Scholar] [CrossRef]
- Gräf, L. Online-Befragung. Eine Praktische Einführung für Anfänger; Lit-Verl.: Berlin, Germany, 2010. [Google Scholar]
- Zanobini, P.; Lorini, C.; Baldasseroni, A.; Dellisanti, C.; Bonaccorsi, G. A Scoping Review on How to Make Hospitals health Literate Healthcare Organizations. Int. J. Environ. Res. Public Health 2020, 17, 1036. [Google Scholar] [CrossRef] [Green Version]
- Sheridan, S.L.; Halpern, D.J.; Viera, A.J.; Berkman, N.D.; Donahue, K.E.; Crotty, K. Interventions for individuals with low health literacy: A systematic review. J. Health Commun. 2011, 16 (Suppl. 3), 30–54. [Google Scholar] [CrossRef]
- Hernandez, L.M. How Can Health Care Organizations Become More Health Literate: Workshop Summary; National Academic Press: Washington, DC, USA, 2012. [Google Scholar]
- Kripalani, S.; Robertson, R.; Love-Ghaffari, M.H.; Henderson, L.E.; Praska, J.; Strawder, A.; Katz, M.G.; Jacobson, T.A. Development of an illustrated medication schedule as a low-literacy patient education tool. Patient Educ. Couns. 2007, 66, 368–377. [Google Scholar] [CrossRef]
- IHI. Institute for Healthcare Improvement: Ask Me 3: Good Questions for Your Good Health. Available online: http://www.ihi.org/resources/Pages/Tools/Ask-Me-3-Good-Questions-for-Your-Good-Health.aspx (accessed on 2 October 2019).
- Rudd, R.E.; Anderson, J.E. The Health Literacy Environment of Hospitals and Health Centers. Partners for Action: Making Your Healthcare Facility Literacy-Friendly. 2006. Available online: https://cdn1.sph.harvard.edu/wp-content/uploads/sites/135/2012/09/healthliteracyenvironment.pdf (accessed on 3 October 2019).
- Johnson, A. First impressions: Towards becoming a health-literate health service. Aust. Health Rev. 2014, 38, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Rudd, R.E.; Groene, O.R.; Navarro-Rubio, M.D. On health literacy and health outcomes: Background, impact, and future directions. Rev. Calid. Asist. 2013, 28, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Paakkari, L.; Okan, O. Health Literacy-Talking the Language of (School) Education. Health Lit. Res. Pract. 2019, 3, e161–e164. [Google Scholar] [CrossRef] [PubMed] [Green Version]



| Qualitative Survey | Quantitative Survey | |||
|---|---|---|---|---|
| Frequency in | Frequency in | |||
| n | % | n | % | |
| Sex of Respondents | ||||
| Male | 5 | 50.0 | 45 | 34.6 |
| Female | 5 | 50.0 | 85 | 65.4 |
| Total | n = 10 | n = 130 | ||
| Age of Respondents | ||||
| 18–30 years | 2 | 20.0 | 3 | 2.3 |
| 31–40 years | 1 | 10.0 | 30 | 23.1 |
| 41–50 years | 3 | 30.0 | 43 | 33.1 |
| 51–60 years | 3 | 30.0 | 42 | 32.3 |
| 61 years and older | 1 | 10.0 | 12 | 9.2 |
| Position in the Organization | ||||
| Executive | 1 | 10.0 | 5 | 3.8 |
| Manager | 6 | 60.0 | 108 | 83.1 |
| Skilled staff | 2 | 20.0 | 6 | 4.6 |
| Other | 1 | 10.0 | 11 | 8.5 |
| Financing | ||||
| State (municipal or federal) | 3 | 37.5 | 16 | 12.3 |
| Non-state/church | 2 | 25.0 | 90 | 69.2 |
| Private or other | 3 | 37.5 | 24 | 18.5 |
| Type of Organization | ||||
| Housing for people with disabilities | 3 | 37.5 | 96 | 73.8 |
| Sheltered workshops | 3 | 37.5 | 34 | 26.2 |
| Combination of housing and workshop | 2 | 25.0 | - | - |
| Number of Skilled Staff | ||||
| Fewer than 50 | 3 | 37.5 | 77 | 59.2 |
| More than 50 | 5 | 62.5 | 53 | 40.8 |
| Profit or Non-Profit Facility | ||||
| Non-profit | 7 | 87.5 | 114 | 87.7 |
| For profit | 1 | 12.5 | 16 | 12.3 |
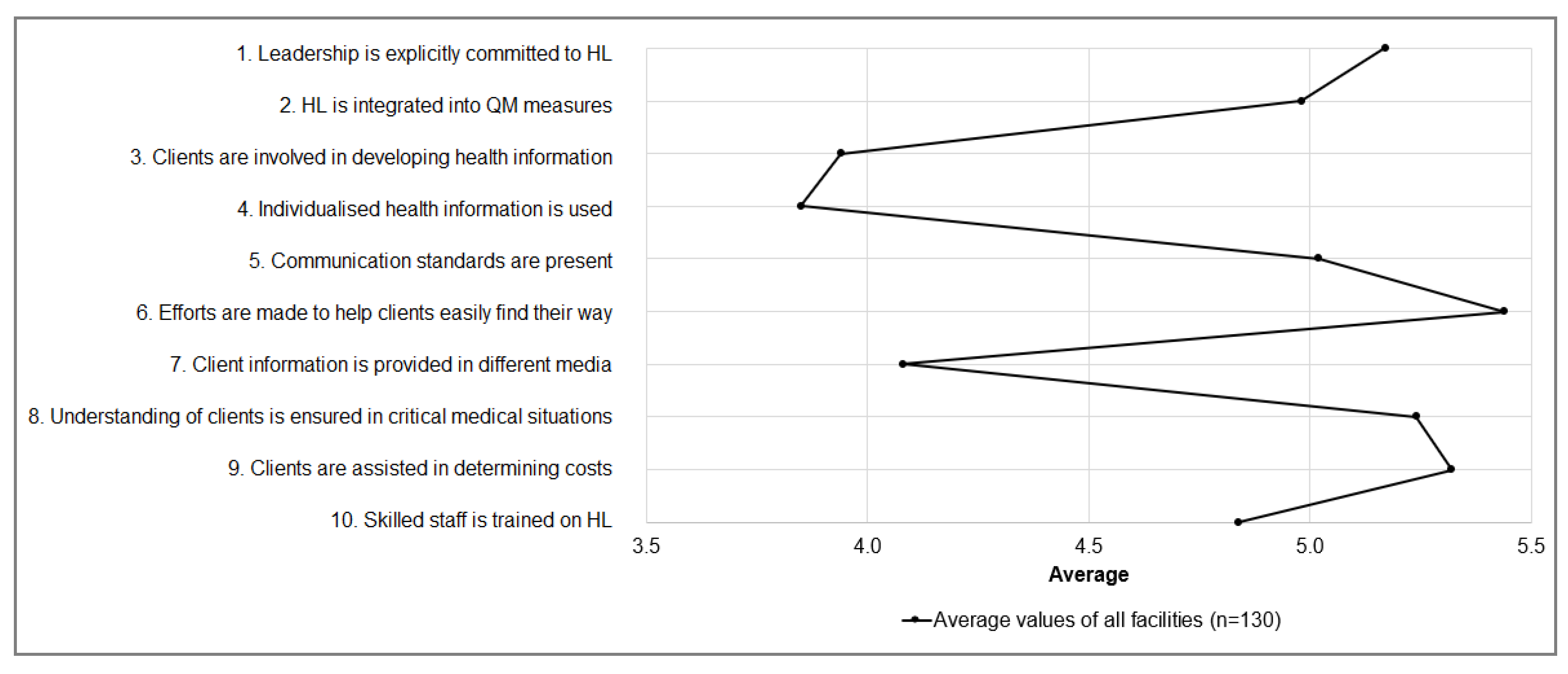
| HLHO-10 Items | M | SD | Min.–Max. |
|---|---|---|---|
| 1. Is the leadership explicitly committed to HL (e.g., mission statement, HR planning)? | 5.2 | 1.4 | 1–7 |
| 2. Is HL in your organization integrated into quality management measures? | 5.0 | 1.5 | 1–7 |
| 3. Are clients involved in developing health information in your organization | 3.9 | 1,7 | 1–7 |
| 4. Is individualized health information provided by your organization (e.g., other languages, large print, braille)? | 3.9 | 1.9 | 1–7 |
| 5. Are there communication standards in your organization that ensure patients actually understand the information they need (e.g., translators, time to think before answering, asking for questions)? | 5.0 | 1.6 | 1–7 |
| 6. Does your organization make an effort to ensure clients can easily find their way (e.g., signposts, health information staff)? | 5.4 | 1.5 | 2–7 |
| 7. Is information in your organization available for different client groups in different media (e.g., 3D models, DVDs, illustrated stories)? | 4.1 | 1.9 | 1–7 |
| 8. Does your organization ensure that especially in critical situations your clients actually understand everything (e.g., intake of medication, therapeutic measures, patient consent)? | 5.2 | 1.5 | 1–7 |
| 9. Does your organization assist clients in determining possible costs (e.g., additional payments for medical or other health-related treatments)? | 5.3 | 1.8 | 1–7 |
| 10. Do employees and skilled staff in your organization receive training in HL? | 4.8 | 1.6 | 1–7 |
| Average mean of HLHO-10: overall degree of organizational health literacy | 4.8 | 1.1 | 2–7 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rathmann, K.; Vockert, T.; Wetzel, L.D.; Lutz, J.; Dadaczynski, K. Organizational Health Literacy in Facilities for People with Disabilities: First Results of an Explorative Qualitative and Quantitative Study. Int. J. Environ. Res. Public Health 2020, 17, 2886. https://doi.org/10.3390/ijerph17082886
Rathmann K, Vockert T, Wetzel LD, Lutz J, Dadaczynski K. Organizational Health Literacy in Facilities for People with Disabilities: First Results of an Explorative Qualitative and Quantitative Study. International Journal of Environmental Research and Public Health. 2020; 17(8):2886. https://doi.org/10.3390/ijerph17082886
Chicago/Turabian StyleRathmann, Katharina, Theres Vockert, Lorena Denise Wetzel, Judith Lutz, and Kevin Dadaczynski. 2020. "Organizational Health Literacy in Facilities for People with Disabilities: First Results of an Explorative Qualitative and Quantitative Study" International Journal of Environmental Research and Public Health 17, no. 8: 2886. https://doi.org/10.3390/ijerph17082886
APA StyleRathmann, K., Vockert, T., Wetzel, L. D., Lutz, J., & Dadaczynski, K. (2020). Organizational Health Literacy in Facilities for People with Disabilities: First Results of an Explorative Qualitative and Quantitative Study. International Journal of Environmental Research and Public Health, 17(8), 2886. https://doi.org/10.3390/ijerph17082886