Edge of the Present: A Virtual Reality Tool to Cultivate Future Thinking, Positive Mood and Wellbeing


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. The Intervention
2.3. Design
2.4. Procedure
2.5. Outcome Measures
- What was your overall enjoyment level in this environment?
- How strong was your sense of presence, “being there”, in the virtual environment?
- What was your overall comfort level in this environment?
3. Results
3.1. Demographics
3.2. Hopelessness, Well-Being, and Mood
3.3. Mixed Model Anova
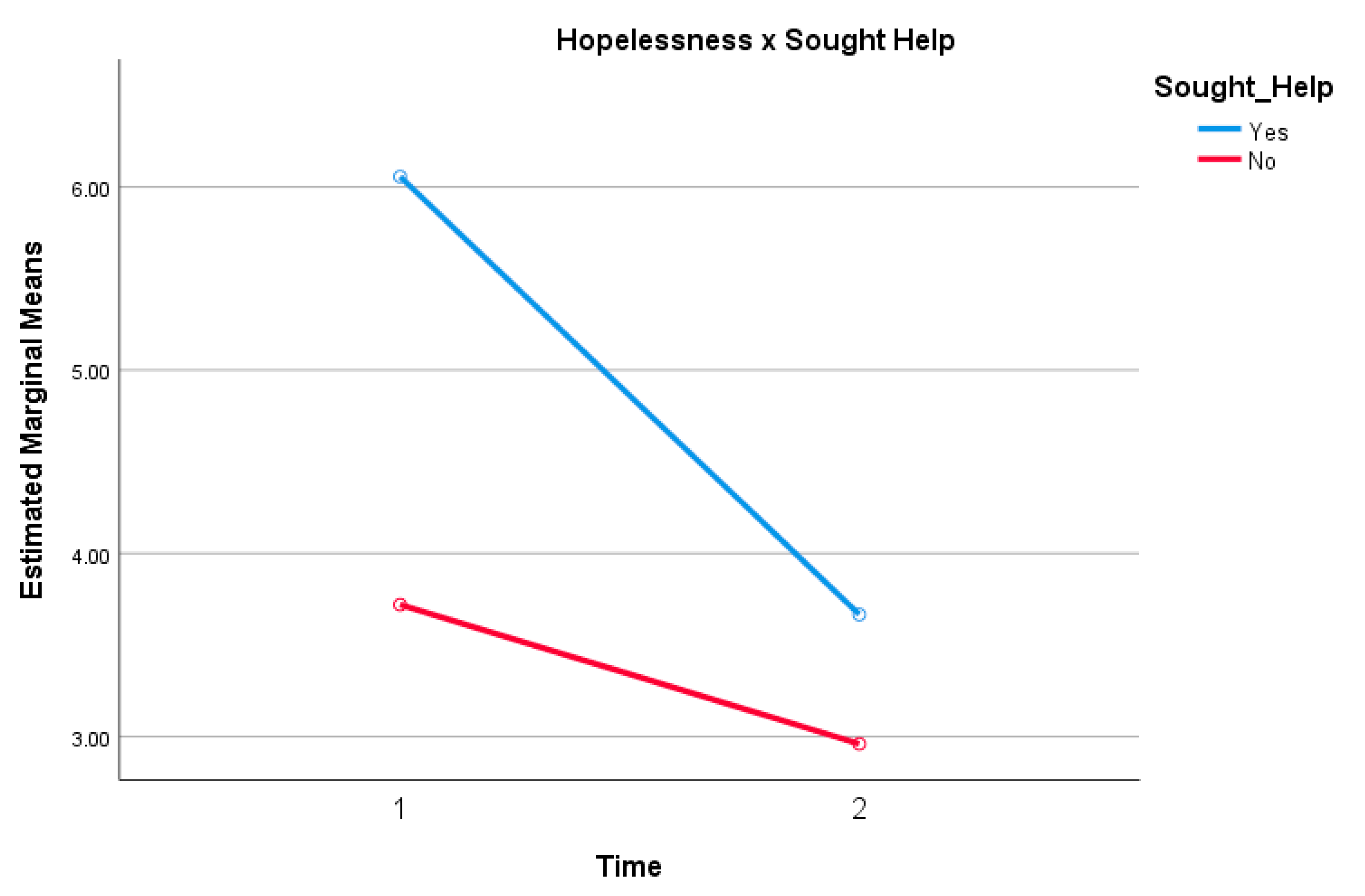
3.3.1. Hopelessness
3.3.2. Well-Being
3.3.3. Positive and Negative Mood
3.4. Open-Ended Comments
“… I just love coming back here. I have treatment resistant depression and I’ve done traditional therapy as well as the Ketamine trials and all of that. But nothing has made me feel instantly better than this virtual reality work. This is the seventh time that I’ve been back and I just can’t get enough of it. Maybe it’s because I have an addictive personality, but I just feel like my mood is instantly better!”“I just didn’t know how badly I needed this. It just made me feel instantly relaxed and calm. I’ve been going through a lot today and after exploring the rest of the festival, I just feel like I needed something to make me feel good again. I’m not sure what it was… if it’s getting back to nature? I understand that it’s not real but there’s something about being in nature that makes you feel like you can breathe again.”“That felt really surreal for me. There is an element of discomfort initially because when you’ve got the headset on, you can’t see your hands. Even though I can open and close things, it was difficult looking down and not seeing my hands in front of me. That’s mainly because I do a lot of yoga and I’m very aware of my body and its effect on my surroundings. But once I got over that and came back again, I realised that I really would have benefited from this if I had this as a teenager. When I was 14, I was institutionalized. When all you’re doing is looking at the same walls all day, I would’ve loved something like this to help me escape that environment.”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Connor, R.C.; Smyth, R.; Williams, J.M.G. Intrapersonal positive future thinking predicts repeat suicide attempts in hospital-treated suicide attempters. J. Consult. Clin. Psychol. 2015, 83, 169–176. [Google Scholar] [CrossRef]
- MacLeod, A.K.; Salaminiou, E. Reduced positive future-thinking in depression: Cognitive and affective factors. Cogn. Emot. 2001, 15, 99–107. [Google Scholar] [CrossRef]
- Conaghan, S.; Davidson, K.M. Hopelessness and the anticipation of positive and negative future experiences in older parasuicidal adults. Br. J. Clin. Psychol. 2002, 41, 233–242. [Google Scholar] [CrossRef]
- MacLeod, A.K.; Rose, G.S.; Williams, J.M.G. Components of hopelessness about the future in parasuicide. Cogn. Ther. Res. 1993, 17, 441–455. [Google Scholar] [CrossRef]
- Macleod, A.K.; Pankhania, B.; Lee, M.; Mitchell, D. Parasuicide, depression and the anticipation of positive and negative future experiences. Psychol. Med. 1997, 27, 973–977. [Google Scholar] [CrossRef]
- Zhang, J.; Li, Z. The association between depression and suicide when hopelessness is controlled for. Compr. Psychiatry 2013, 54, 790–796. [Google Scholar] [CrossRef] [Green Version]
- Sarkohi, A. Future Thinking and Depression. Ph.D. Thesis, Linköping University, Linköping, Sweden, Unpublished work. 2011. [Google Scholar]
- Beck, A.T. Cognitive Therapy of Depression; Guildford Press: New York, NY, USA, 1979. [Google Scholar]
- Wilson, F.C.L.; Gregory, J.D. Overgeneral autobiographical memory and depression in older adults: A systematic review. Aging Ment. Health 2017, 22, 575–586. [Google Scholar] [CrossRef]
- Slofstra, C.; Eisma, M.C.; Holmes, E.A.; Bockting, C.L.; Nauta, M.H. Rethinking a Negative Event: The Affective Impact of Ruminative versus Imagery-Based Processing of Aversive Autobiographical Memories. Front. Psychiatry 2017, 8, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pictet, A. Looking on the bright side in social anxiety: The potential benefit of promoting positive mental imagery. Front. Hum. Neurosci. 2014, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, E.A.; Lang, T.J.; Deeprose, C. Mental Imagery and Emotion in Treatment across Disorders: Using the Example of Depression. Cogn. Behav. Ther. 2009, 38, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Nelis, A.; Holmes, E.A.; Palmieri, R.; Bellelli, G.; Raes, F. Thinking back about a positive event: The impact of pro-cessing style on positive affect. Front. Psychiatry 2015, 6, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, E.A.; Crane, C.; Fennell, M.J.; Williams, J.M.G. Imagery about suicide in depression—“Flash-forwards”? J. Behav. Ther. Exp. Psychiatry 2007, 38, 423–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morina, N.; Deeprose, C.; Pusowski, C.; Schmid, M.; Holmes, E.A. Prospective mental imagery in patients with major depressive disorder or anxiety disorders. J. Anxiety Disord. 2011, 25, 1032–1037. [Google Scholar] [CrossRef] [Green Version]
- Chin, J.; Holden, R.R. Multidimensional Future Time Perspective as Moderators of the Relationships between Suicide Motivation, Preparation, and Its Predictors. Suicide Life Threat. Behav. 2013, 43, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Reeve, S.; Robinson, A.; Ehlers, A.; Clark, D.; Spanlang, B.; Slater, M. Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol. Med. 2017, 47, 2393–2400. [Google Scholar] [CrossRef]
- Rizzo, A.; Bouchard, S. Virtual Reality for Psychological and Neurocognitive Interventions; Springer: Berlin/Heidelberg, Germany, 2019; pp. 14–40. [Google Scholar]
- Bell, I.H.; Nicholas, J.; Alvarez-Jimenez, M.; Thompson, A.; Valmaggia, L. Virtual reality as a clinical tool in mental health research and practice. Dialog Clin. Neurosci. 2020, 22, 169–177. [Google Scholar] [CrossRef]
- Lodola, A. Mixed Reality vs. Augmented Reality: What’s the Difference? 2018. Available online: https://www.aniwaa.com/blog/mixed-reality-vs-augmented-reality-whats-the-difference/ (accessed on 1 December 2020).
- Falconer, C.J.; Rovira, A.; King, J.A.; Gilbert, P.; Antley, A.; Fearon, P.; Ralph, N.; Slater, M.; Brewin, C.R. Embodying self-compassion within virtual reality and its effects on patients with depression. BJPsych Open 2016, 2, 74–80. [Google Scholar] [CrossRef] [Green Version]
- Hviid, L.B.; Ravnkilde, B.; Ahdidan, J.; Rosenberg, R.; Stødkilde-Jørgensen, H.; Videbech, P. Hippocampal visuospatial function and volume in remitted depressed patients: An 8-year follow-up study. J. Affect. Disord. 2010, 125, 177–183. [Google Scholar] [CrossRef]
- Dehn, L.B.; Kater, L.; Piefke, M.; Botsch, M.; Driessen, M.; Beblo, T. Training in a comprehensive everyday-like virtual reality environment compared to computerized cognitive training for patients with depression. Comput. Hum. Behav. 2018, 79, 40–52. [Google Scholar] [CrossRef]
- Gould, N.F.; Holmes, M.K.; Fantie, B.D.; Luckenbaugh, D.A.; Pine, D.S.; Gould, T.D.; Burgess, N.; Manji, H.K.; Zarate, C.A. Performance on a Virtual Reality Spatial Memory Navigation Task in Depressed Patients. Am. J. Psychiatry 2007, 164, 516–519. [Google Scholar] [CrossRef]
- Franklin, J.C.; Huang, X.; Bastidas, D. Virtual reality suicide: Development of a translational approach for studying suicide causes. Behav. Res. Ther. 2019, 120, 103360. [Google Scholar] [CrossRef]
- Fat, L.N.; Scholes, S.; Boniface, S.; Mindell, J.; Stewart-Brown, S. Evaluating and establishing national norms for mental wellbeing using the short Warwick–Edinburgh Mental Well-being Scale (SWEMWBS): Findings from the Health Survey for England. Qual. Life Res. 2017, 26, 1129–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iliceto, F.; Fino, E. Beck Hopelessness Scale (BHS): A second-order confirmatory factor analysis. Eur. J. Psychol. Assess. 2015, 31, 31–37. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS Scales. J. Personal. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Tran, V. Positive Affect Negative Affect Scale (PANAS). In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013. [Google Scholar]
- Torisu, T. Sense of Presence in Social VR Experience. 2016. Available online: http://www.interactivearchitecture.org/sense-of-presence-in-social-vr-experience.html (accessed on 1 December 2020).
- Bystrom, K.-E.; Barfield, W.; Hendrix, C. A Conceptual Model of the Sense of Presence in Virtual Environments. Presence: Teleoperators Virtual Environ. 1999, 8, 241–244. [Google Scholar] [CrossRef]
- Dinh, H.Q.; Walker, N.; Hodges, L.F.; Song, C.G. Evaluating the importance of multi-sensory input on memory and the sense of presence in virtual environments. Proc. IEEE Virtual Real. 1999. [CrossRef]
- Deeprose, C.; Holmes, E.A. An Exploration of Prospective Imagery: The Impact of Future Events Scale. Behav. Cogn. Psychother. 2010, 38, 201–209. [Google Scholar] [CrossRef]
- Pharr, J.R.; Moonie, S.; Bungum, T. The Impact of Unemployment on Mental and Physical Health, Access to Health Care and Health Risk Behaviors. ISRN Public Heal. 2012, 2012, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Lindgren, R.; Johnson-Glenberg, M. Emboldened by Embodiment: Six Precepts for Research on Embodied Learning and Mixed Reality. Educ. Res. 2013, 42, 445–452. [Google Scholar] [CrossRef]
- Vujcic, M.; Tomicevic-Dubljevic, J.; Grbic, M.; Lecic-Tosevski, D.; Vukovic, O.; Toskovic, O. Nature based solution for improving mental health and well-being in urban areas. Environ. Res. 2017, 158, 385–392. [Google Scholar] [CrossRef]


{kind=link}
| Baseline Characteristic | Full Sample | |
|---|---|---|
| n | % | |
| Gender | ||
| Female | 53 | 67.1 |
| Male | 23 | 29.1 |
| Non-binary | 3 | 3.8 |
| Age | ||
| 18–24 | 18 | 22.8 |
| 25–34 | 19 | 24.1 |
| 35–44 | 13 | 16.5 |
| 45–54 | 13 | 16.5 |
| 55–64 | 14 | 17.7 |
| 65+ | 2 | 2.5 |
| Preferred language | ||
| English | 58 | 73.4 |
| Other | 21 | 26.6 |
| Education | ||
| Secondary school | 10 | 12.7 |
| University/college | 69 | 87.3 |
| Employment | ||
| Employed, full-time (FT) | 24 | 30.4 |
| Employed, part-time (PT) | 25 | 31.6 |
| Not employed, looking for work | 5 | 6.3 |
| Not employed, not looking for work | 1 | 1.3 |
| Retired | 4 | 5.1 |
| Disabled, unable to work | 1 | 1.3 |
| Student | 14 | 17.7 |
| Self-employed | 4 | 5.1 |
| Other | 1 | 1.3 |
| Virtual reality experience | ||
| None at all | 4 | 5.1 |
| A little | 11 | 13.9 |
| Quite a bit | 51 | 64.6 |
| A lot | 13 | 16.5 |
| Sought help | ||
| Yes | 54 | 68.4 |
| No | 25 | 31.6 |
| Variable | Pre | Post | ||
|---|---|---|---|---|
| M | SD | M | SD | |
| Beck Hopelessness Scale | 5.32 | 4.31 | * 3.44 | 3.12 |
| Positive and Negative Affect Schedule (Positive Mood) | 30.71 | 7.87 | * 35.91 | 6.37 |
| Positive and Negative Affect Schedule (Negative Mood) | 16.98 | 5.75 | * 14.13 | 4.44 |
| Short Warwick-Edinburgh Mental Well-Being Scale | 3.36 | 0.64 | * 3.80 | 0.53 |
| Employment × Hopelessness | Pre | Post | Change Score | |||
|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |
| Employed, FT | 3.29 | 2.68 | * 2.67 | 2.04 | 0.63 | 2.01 |
| Employed, PT | 6.84 | 4.39 | * 4.28 | 3.29 | 2.56 | 3.62 |
| Not employed, looking for work | 5.80 | 5.63 | * 3.00 | 1.58 | 2.80 | 4.15 |
| Retired | 4.00 | 3.46 | * 3.00 | 1.63 | 1.00 | 3.46 |
| Student | 5.14 | 3.57 | * 3.07 | 2.92 | 2.07 | 2.46 |
| Employment × Well-Being | Pre | Post | Change Score | |||
|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | |
| Employed, FT | 3.64 | 0.65 | * 4.00 | 0.57 | 0.36 | 0.48 |
| Employed, PT | 3.23 | 0.45 | * 3.64 | 0.41 | 0.41 | 0.41 |
| Not employed, looking for work | 3.09 | 0.70 | * 3.97 | 0.40 | 0.89 | 0.79 |
| Retired | 3.46 | 0.55 | * 3.89 | 0.65 | 0.43 | 0.45 |
| Student | 3.38 | 0.74 | * 3.74 | 0.54 | 0.37 | 0.58 |
| Self-employed | 3.43 | 0.68 | * 3.50 | 0.60 | 0.07 | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Habak, S.; Bennett, J.; Davies, A.; Davies, M.; Christensen, H.; Boydell, K.M. Edge of the Present: A Virtual Reality Tool to Cultivate Future Thinking, Positive Mood and Wellbeing. Int. J. Environ. Res. Public Health 2021, 18, 140. https://doi.org/10.3390/ijerph18010140
Habak S, Bennett J, Davies A, Davies M, Christensen H, Boydell KM. Edge of the Present: A Virtual Reality Tool to Cultivate Future Thinking, Positive Mood and Wellbeing. International Journal of Environmental Research and Public Health. 2021; 18(1):140. https://doi.org/10.3390/ijerph18010140
Chicago/Turabian StyleHabak, Stephanie, Jill Bennett, Alex Davies, Michaela Davies, Helen Christensen, and Katherine M. Boydell. 2021. "Edge of the Present: A Virtual Reality Tool to Cultivate Future Thinking, Positive Mood and Wellbeing" International Journal of Environmental Research and Public Health 18, no. 1: 140. https://doi.org/10.3390/ijerph18010140