Avoidable Mortality Attributable to Anthropogenic Fine Particulate Matter (PM2.5) in Australia

 ,
,  , , ,
, , , 
 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Region and Period
2.2. Assessment of Anthropogenic vs. Non-Anthropogenic PM2.5 Concentrations
2.3. Health Outcomes
2.4. Quantification of Mortality Attributable to Anthropogenic PM2.5
2.5. Life Expectancy Calculations
2.6. Economic Valuation
3. Results
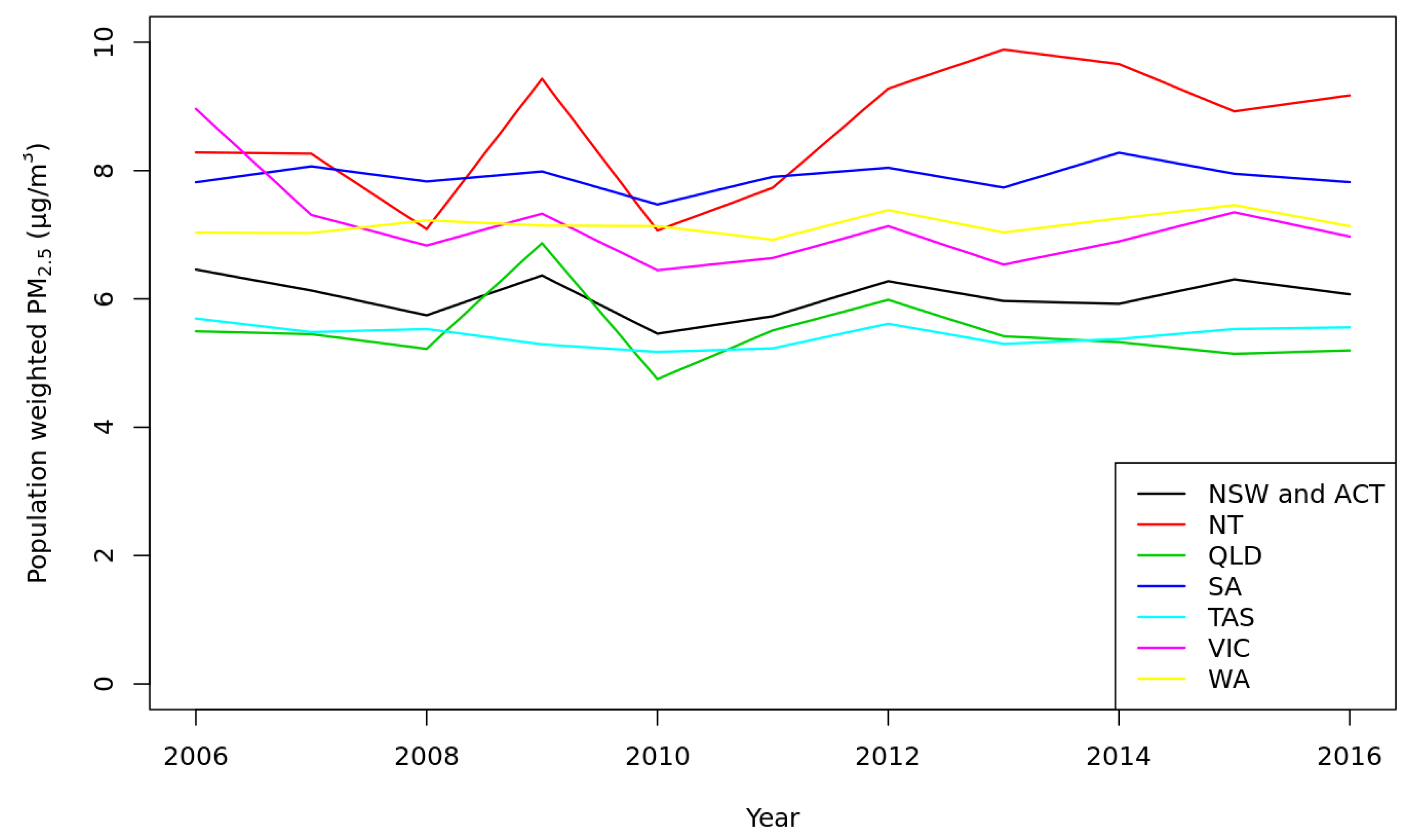
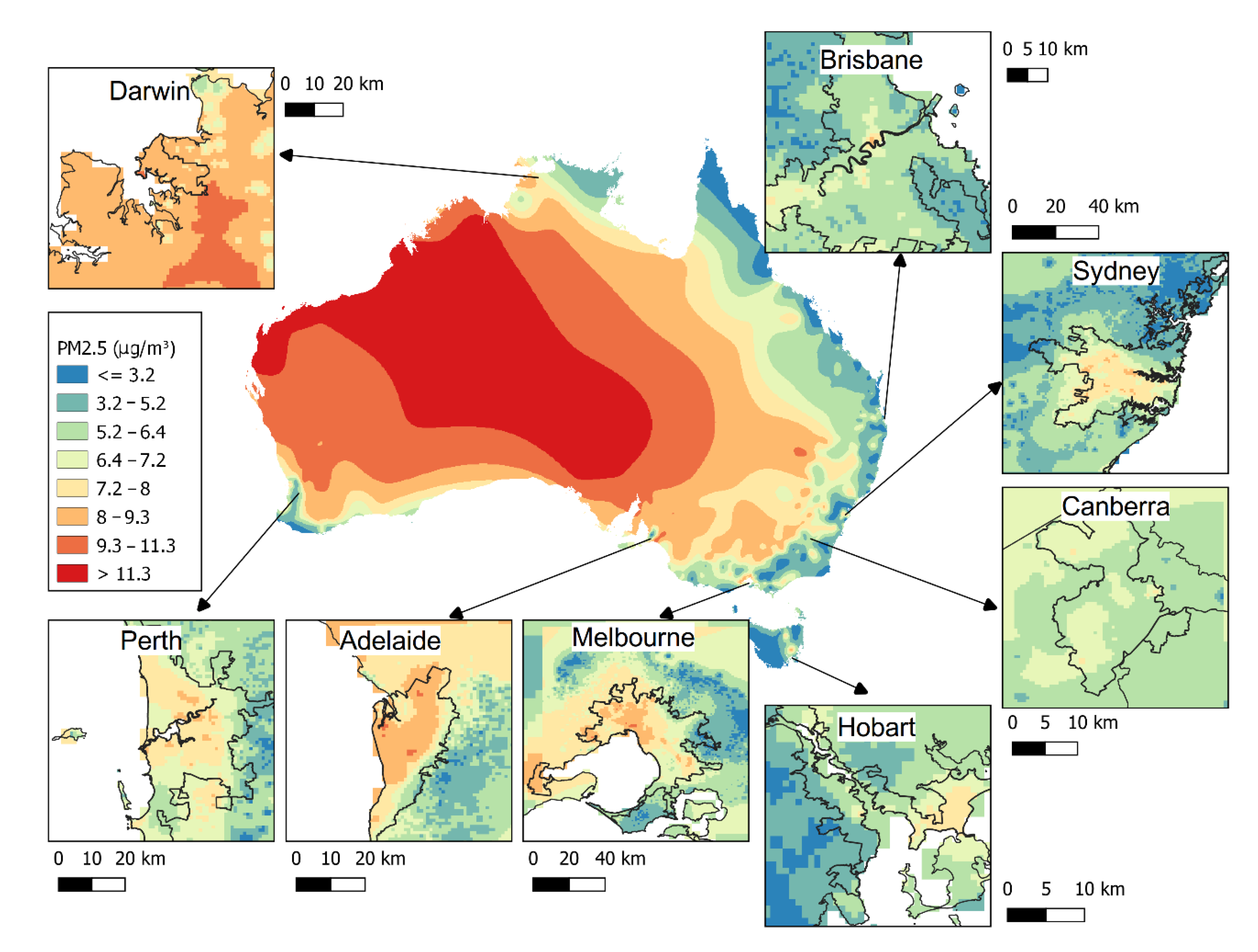
3.1. Exposure Assessment
3.2. Mortality Burden
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef]
- Shah, A.S.V.; Langrish, J.P.; Nair, H.; A McAllister, D.; Hunter, A.L.; Donaldson, K.; E Newby, D.; Mills, N.L. Global association of air pollution and heart failure: A systematic review and meta-analysis. Lancet 2013, 382, 1039–1048. [Google Scholar] [CrossRef]
- Hansen, C.A.; Barnett, A.G.; Jalaludin, B.B.; Morgan, G.G. Ambient Air Pollution and Birth Defects in Brisbane, Australia. PLoS ONE 2009, 4, e5408. [Google Scholar] [CrossRef] [PubMed]
- Clifford, A.; Lang, L.; Chen, R.; Anstey, K.J.; Seaton, A. Exposure to air pollution and cognitive functioning across the life course—A systematic literature review. Environ. Res. 2016, 147, 383–398. [Google Scholar] [CrossRef] [PubMed]
- Peters, A.; Dockery, D.W.; Heinrich, J.; E Wichmann, H. Medication use modifies the health effects of particulate sulfate air pollution in children with asthma. Environ. Health Perspect. 1997, 105, 430–435. [Google Scholar] [CrossRef]
- Kollanus, V.; Tiittanen, P.; Niemi, J.V.; Lanki, T. Effects of long-range transported air pollution from vegetation fires on daily mortality and hospital admissions in the Helsinki metropolitan area, Finland. Environ. Res. 2016, 151, 351–358. [Google Scholar] [CrossRef]
- Hanigan, I.; Rolfe, M.I.; Knibbs, L.D.; Salimi, F.; Cowie, C.T.; Heyworth, J.; Marks, G.B.; Guo, Y.; Cope, M.; Bauman, A.; et al. All-cause mortality and long-term exposure to low level air pollution in the ‘45 and up study’ cohort, Sydney, Australia, 2006–2015. Environ. Int. 2019, 126, 762–770. [Google Scholar] [CrossRef]
- Lelieveld, J.; Pozzer, A.; Pöschl, U.; Fnais, M.; Haines, A.; Münzel, T. Loss of life expectancy from air pollution compared to other risk factors: A worldwide perspective. Cardiovasc. Res. 2020, 116, 1910–1917. [Google Scholar] [CrossRef]
- Broome, R.; Powell, J.; Cope, M.E.; Morgan, G.G. The mortality effect of PM2.5 sources in the Greater Metropolitan Region of Sydney, Australia. Environ. Int. 2020, 137, 105429. [Google Scholar] [CrossRef]
- Kulkarni, S.; Sobhani, N.; Miller-Schulze, J.P.; Shafer, M.M.; Schauer, J.J.; Solomon, P.A.; Saide, P.; Spak, S.N.; Cheng, Y.; Van Der Gon, H.A.C.D.; et al. Source sector and region contributions to BC and PM2.5 in Central Asia. Atmos. Chem. Phys. Discuss. 2014, 14, 11343–11392. [Google Scholar] [CrossRef]
- Carnell, E.J.; Vieno, M.; Vardoulakis, S.; Beck, R.C.; Heaviside, C.; Tomlinson, S.J.; Dragosits, U.; Heal, M.R.; Reis, S. Modelling public health improvements as a result of air pollution control policies in the UK over four decades—1970 to 2010. Environ. Res. Lett. 2019, 14, 074001. [Google Scholar] [CrossRef]
- Rich, D.Q. Accountability studies of air pollution and health effects: Lessons learned and recommendations for future natural experiment opportunities. Environ. Int. 2017, 100, 62–78. [Google Scholar] [CrossRef] [PubMed]
- Broome, R.A.; Cope, M.E.; Goldsworthy, B.; Goldsworthy, L.; Emmerson, K.; Jegasothy, E.; Morgan, G.G. The mortality effect of ship-related fine particulate matter in the Sydney greater metropolitan region of NSW, Australia. Environ. Int. 2016, 87, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.A.; Hammitt, J.K.; O’Keeffe, L. Valuing Mortality Risk Reductions in Global Benefit-Cost Analysis. J. Benefit-Cost Anal. 2019, 10, 15–50. [Google Scholar] [CrossRef] [PubMed]
- Knibbs, L.D.; Van Donkelaar, A.; Martin, R.V.; Bechle, M.J.; Brauer, M.; Cohen, D.D.; Cowie, C.T.; Dirgawati, M.; Guo, Y.; Hanigan, I.C.; et al. Satellite-Based Land-Use Regression for Continental-Scale Long-Term Ambient PM2.5 Exposure Assessment in Australia. Environ. Sci. Technol. 2018, 52, 12445–12455. [Google Scholar] [CrossRef] [PubMed]
- Hoek, G.; Krishnan, R.M.; Beelen, R.; Peters, A.; Ostro, B.; Brunekreef, B.; Kaufman, J.D. Long-term air pollution exposure and cardio- respiratory mortality: A review. Environ. Health 2013, 12, 43. [Google Scholar] [CrossRef]
- WHO. Health Risks of Air Pollution in Europe—HRAPIE Project: Recommendations for Concentration-Response Functions for Cost-Benefit Analysis of Particulate Matter, Ozone and Nitrogen Dioxide; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Miller, B.G.; Hurley, J. Life table methods for quantitative impact assessments in chronic mortality. J. Epidemiology Community Health 2003, 57, 200–206. [Google Scholar] [CrossRef]
- Australian Government Office of Best Practice Regulation. Best Practice Regulation Guidance Note Value of a statistical life Guidance Note 2019. Available online: https://www.pmc.gov.au/sites/default/files/publications/value-of-statistical-life-guidance-note_0_0.pdf (accessed on 31 June 2020).
- Zhang, Y.; Beggs, P.; McGushin, A. The 2020 special report of the MJA-Lancet Countdown on health and climate change: Lessons learnt from Australia’s ‘Black Summer’. Med. J. Aust. 2021, 213, 490–492. [Google Scholar] [CrossRef]
- Van Vuuren, D.; Edmonds, J.; Kainuma, M.; Riahi, K.; Thomson, A.; Hibbard, K.; Hurtt, G.C.; Kram, T.; Krey, V.; Lamarque, J.-F.; et al. The representative concentration pathways: An overview. Clim. Chang. 2011, 109, 5–31. [Google Scholar] [CrossRef]
- Zheng, Y.; Xue, T.; Zhang, Q.; Geng, G.; Tong, D.; Li, X.; He, K. Air quality improvements and health benefits from China’s clean air action since 2013. Environ. Res. Lett. 2017, 12, 114020. [Google Scholar] [CrossRef]
- Zhao, Y.; Nielsen, C.P.; Lei, Y. Quantifying the uncertainties of a bottom-up emission inventory of anthropogenic atmospheric pollutants in China. Atmos. Chem. Phys. 2011, 46, 3973–3980. [Google Scholar] [CrossRef]
- Abbafati, C.; Machado, D.B.; Cislaghi, B. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 10258. [Google Scholar]
- Banks, E.; Joshy, G.; Weber, M.F.; Liu, B.; Grenfell, R.; Egger, S.J.; Paige, E.; Lopez, A.D.; Sitas, F.; Beral, V. Tobacco smoking and all-cause mortality in a large Australian cohort study: Findings from a mature epidemic with current low smoking prevalence. BMC Med. 2015, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Hoek, G. Long-term exposure to PM and all-cause and cause-specific mortality: A systematic review and meta-analysis. Environ. Int. 2020, 143, 105974. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Year | Anthropogenic PM2.5 | Natural PM2.5 | Total PM2.5 |
|---|---|---|---|
| 2006 | 3.2 | 3.9 | 7.1 |
| 2007 | 3.1 | 3.5 | 6.6 |
| 2008 | 3.2 | 3.1 | 6.3 |
| 2009 | 3.2 | 3.7 | 6.9 |
| 2010 | 3.1 | 2.8 | 5.9 |
| 2011 | 3.1 | 3.1 | 6.2 |
| 2012 | 3.2 | 3.6 | 6.7 |
| 2013 | 3.2 | 3.1 | 6.3 |
| 2014 | 3.2 | 3.2 | 6.4 |
| 2015 | 3.2 | 3.4 | 6.6 |
| 2016 | 3.1 | 3.3 | 6.4 |
| Region | AN (95%CI) | YLL (95%CI) |
|---|---|---|
| NSW and ACT | 940 (615–1241) | 13,956 (9094–18509) |
| VIC | 650 (425–858) | 9366 (6103–12421) |
| QLD | 517 (338–682) | 7925 (5165–10509) |
| WA | 197 (129–260) | 3178 (2072–4213) |
| SA | 188 (123–249) | 2653 (1729–3518) |
| TAS | 102 (67–135) | 1419 (925–1882) |
| NT | 21 (14–28) | 464 (303–615) |
| National | 2616 (1712–3455) | 38,962 (25391–51669) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanigan, I.C.; Broome, R.A.; Chaston, T.B.; Cope, M.; Dennekamp, M.; Heyworth, J.S.; Heathcote, K.; Horsley, J.A.; Jalaludin, B.; Jegasothy, E.; et al. Avoidable Mortality Attributable to Anthropogenic Fine Particulate Matter (PM2.5) in Australia. Int. J. Environ. Res. Public Health 2021, 18, 254. https://doi.org/10.3390/ijerph18010254
Hanigan IC, Broome RA, Chaston TB, Cope M, Dennekamp M, Heyworth JS, Heathcote K, Horsley JA, Jalaludin B, Jegasothy E, et al. Avoidable Mortality Attributable to Anthropogenic Fine Particulate Matter (PM2.5) in Australia. International Journal of Environmental Research and Public Health. 2021; 18(1):254. https://doi.org/10.3390/ijerph18010254
Chicago/Turabian StyleHanigan, Ivan C., Richard A. Broome, Timothy B. Chaston, Martin Cope, Martine Dennekamp, Jane S. Heyworth, Katharine Heathcote, Joshua A. Horsley, Bin Jalaludin, Edward Jegasothy, and et al. 2021. "Avoidable Mortality Attributable to Anthropogenic Fine Particulate Matter (PM2.5) in Australia" International Journal of Environmental Research and Public Health 18, no. 1: 254. https://doi.org/10.3390/ijerph18010254
APA StyleHanigan, I. C., Broome, R. A., Chaston, T. B., Cope, M., Dennekamp, M., Heyworth, J. S., Heathcote, K., Horsley, J. A., Jalaludin, B., Jegasothy, E., Johnston, F. H., Knibbs, L. D., Pereira, G., Vardoulakis, S., Vander Hoorn, S., & Morgan, G. G. (2021). Avoidable Mortality Attributable to Anthropogenic Fine Particulate Matter (PM2.5) in Australia. International Journal of Environmental Research and Public Health, 18(1), 254. https://doi.org/10.3390/ijerph18010254