E-Cigarette-Only and Dual Use among Adolescents in Ireland: Emerging Behaviours with Different Risk Profiles


 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Ethical Approval
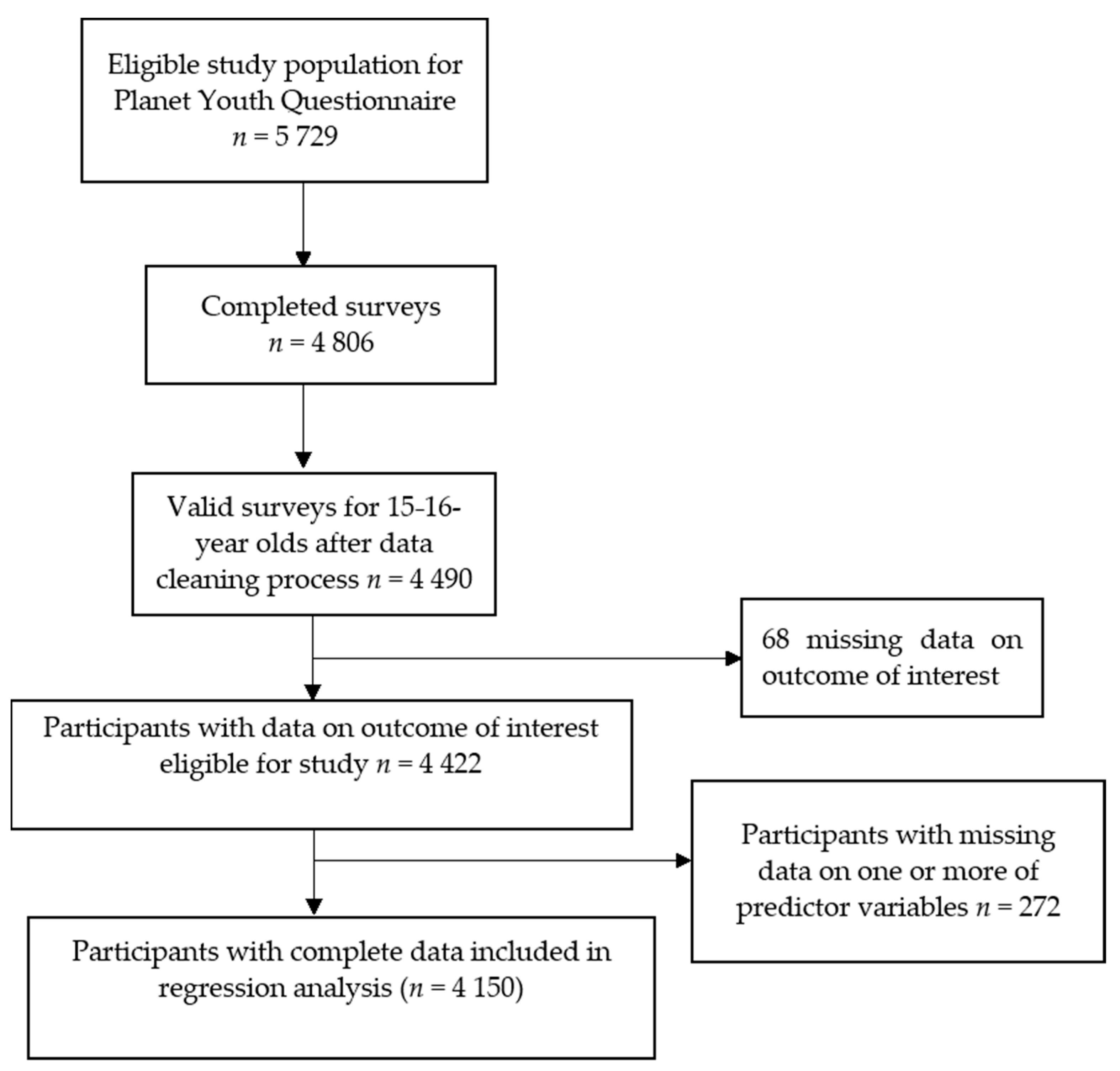
2.4. Participants
2.5. Outcome
2.6. Predictors
- Sociodemographic factors: Gender, Parental Education;
- Family-related factors: Parental supervision, Parental smoking behaviour, Parental reaction to conventional cigarette use;
- Peer group-related factors: Friends smoking behaviours, Feeling it necessary to smoke to fit in;
- Community/Leisure time factors: Value for Conventional Social Norms, Team Sport Participation;
- Individual factors: Academic achievement, Self-rated Mental Health;
2.7. Statistical Analysis
3. Results
3.1. Description of Sample
3.2. Characteristics of Study Population
3.3. Prevalence of Nicotine Product Use
3.4. Results of Multinomial Logistic Regression
3.4.1. Sociodemographic Factors
3.4.2. Family-Related Factors
3.4.3. Peer-Related Factors
3.4.4. Community/Leisure Time Related Factors
3.4.5. Individual Factors
4. Discussion
4.1. Epidemiology of Nicotine Product Use
4.2. Factors Associated with Nicotine Product Use
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Health Service Executive, Environmental Health, Tobacco Control. Available online: https://www.hse.ie/eng/services/list/1/environ/tobacco-control.html (accessed on 1 August 2020).
- Forouzanfar, M.H.; Alexander, L.; Anderson, H.R.; Bachman, V.F.; Biryukov, S.; Brauer, M.; Burnett, R.; Casey, D.; Coates, M.M.; Cohen, A.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef]
- Ferkol, T.W.; Farber, H.J.; La Grutta, S.; Leone, F.T.; Marshall, H.M.; Neptune, E.; Pisinger, C.; Vanker, A.; Wisotzky, M.; Zabert, G.E.; et al. Electronic cigarette use in youths: A position statement of the Forum of International Respiratory Societies. Eur. Respir. J. 2018, 51, 1800278. [Google Scholar] [CrossRef] [PubMed]
- Perry, C.L. The tobacco industry and underage youth smoking: Tobacco industry documents from the Minnesota litigation. Arch. Pediatr. Adolesc. Med. 1999, 153, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Bold, K.W.; Kong, G.; Camenga, D.R.; Simon, P.; Cavallo, D.A.; Morean, M.E.; Krishnan-Sarin, S. Trajectories of e-cigarette and conventional cigarette use among youth. Pediatrics 2018, 141, e20171832. [Google Scholar] [CrossRef] [PubMed]
- Astor, R.L.; Urman, R.; Barrington-Trimis, J.L.; Berhane, K.; Steinberg, J.; Cousineau, M.; Leventhal, A.M.; Unger, J.B.; Cruz, T.; Pentz, M.A.; et al. Tobacco retail licensing and youth product use. Pediatrics 2019, 143, e20173536. [Google Scholar] [CrossRef]
- Hartman-Boyce, J.; McRobbie, H.; Bullen, C.; Begh, R.; Stead, L.F.; Hajek, P. Electronic cigarettes for smoking cessation. Cochrane Database Syst. Rev. 2016, 9, CD010216. [Google Scholar] [CrossRef]
- Kmietowicz, Z. Public Health England insists e-cigarettes are 95% safer than smoking. BMJ 2018, 363, k5429. [Google Scholar] [CrossRef]
- Kalkhoran, S.; Glantz, S.A. E-cigarettes and smoking cessation in real-world and clinical settings: A systematic review and me-ta-analysis. Lancet Respir. Med. 2016, 4, 116–128. [Google Scholar] [CrossRef]
- Yuan, M.; Cross, S.J.; Loughlin, S.E.; Leslie, F.M. Nicotine and the adolescent brain. J. Physiol. 2015, 593, 3397–3412. [Google Scholar] [CrossRef]
- Khouja, J.N.; Suddell, S.F.; Peters, S.E.; Taylor, A.E.; Munafò, M.R. Is e-cigarette use in non-smoking young adults associated with later smoking? A systematic review and meta-analysis. Tob. Control. 2021, 30, 8–15. [Google Scholar] [CrossRef]
- Alzahrani, T.; Pena, I.; Temesgen, N.; Glantz, S. Association between electronic cigarette use and myocardial infarction. Am. J. Prev. Med. 2018, 55, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Ndunda, P.M.; Muutu, T.M. Abstract 9: Electronic cigarette use is associated with a higher risk of stroke. Stroke 2019, 50, A9. [Google Scholar] [CrossRef]
- Wills, T.A.; Pagano, I.; Williams, R.J.; Tam, E. E-cigarette use and respiratory disorder in an adult sample. Drug Alcohol Depend. 2019, 194, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Rubinstein, M.L.; Delucchi, K.; Benowitz, N.L.; Ramo, D.E. Adolescent exposure to toxic volatile organic chemicals from e-cigarettes. Pediatrics 2018, 141, e20173557. [Google Scholar] [CrossRef] [PubMed]
- Jackler, R.; Chau, C.; Getachew, B.D.; Whitcomb, M.M.; Heidenreich, J.-L.; Bhatt, A.M.; Kim-O’Sullivan, S.H.S.; Hoffman, Z.; Jackler, L.M.; Ramamurthi, D. JUUL Advertising Over Its First Three Years on the Market; Stanford University School of Medicine: Stanford, CA, USA, 2019; Unpublished Report; Available online: http://tobacco.stanford.edu/tobacco_main/publications/JUUL_Marketing_Stanford.pdf (accessed on 21 August 2020).
- Cullen, K.A.; Gentzke, A.S.; Sawdey, M.D.; Chang, J.T.; Anic, G.M.; Wang, T.W.; Creamer, M.R.; Jamal, A.; Ambrose, B.K.; King, B.A. E-cigarette use among youth in the United States, 2019. JAMA 2019, 322, 2095–2103. [Google Scholar] [CrossRef] [PubMed]
- Action on Smoking and Health (ASH) Use of E-Cigarettes Among Young People in Great Britain June 2019. Available online: https://ash.org.uk/wp-content/uploads/2019/06/ASH-Factsheet-Youth-E-cigarette-Use-2019.pdf (accessed on 12 March 2020).
- Babineau, K.; Taylor, K.; Clancy, L. Electronic cigarette use among Irish youth: A cross sectional study of prevalence and associated factors. PLoS ONE 2015, 10, e0126419. [Google Scholar] [CrossRef]
- Költő, A.; Gavin, A.; Molcho, M.; Kelly, C.; Walker, L.; Gabhainn, S.N. The Irish Health Behaviour in School-Aged Children [HBSC] Study 2018 [Internet]. National University of Ireland Galway. 2020. Available online: http://www.nuigalway.ie/media/healthpromotionresearchcentre/hbscdocs/nationalreports/2018-report---online-version-interactive---updated.pdf (accessed on 14 November 2020).
- Weaver, S.R.; Kim, H.; Glasser, A.M.; Sutfin, E.L.; Barrington-Trimis, J.L.; Payne, T.J.; Saddleson, M.; Loukas, A. Establishing consensus on survey measures for electronic nicotine and non-nicotine delivery system use: Current challenges and considerations for researchers. Addict. Behav. 2018, 79, 203–212. [Google Scholar] [CrossRef]
- Adelman, W.P. Dual use and dual truths: Categorizing the adolescent electronic cigarette user. J. Adolesc. Health 2019, 65, 167–168. [Google Scholar] [CrossRef]
- Hanewinkel, R.; Isensee, B. Risk factors for e-cigarette, conventional cigarette, and dual use in German adolescents: A cohort study. Prev. Med. 2015, 74, 59–62. [Google Scholar] [CrossRef]
- Wills, T.A.; Knight, R.; Williams, R.J.; Pagano, I.; Sargent, J.D. Risk factors for exclusive e-cigarette use and dual e-cigarette use and tobacco use in adolescents. Pediatrics 2014, 135, e43–e51. [Google Scholar] [CrossRef]
- Barrington-Trimis, J.L.; Berhane, K.; Unger, J.B.; Cruz, T.B.; Huh, J.; Leventhal, A.M.; Urman, R.; Wang, K.; Howland, S.; Gilreath, T.D.; et al. Psychosocial Factors associated with adolescent electronic cigarette and cigarette use. Pediatrics 2015, 136, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Jeon, C.; Jung, K.J.; Kimm, H.; Lee, S.; Barrington-Trimis, J.L.; McConnell, R.; Samet, J.M.; Jee, S.H. E-cigarettes, conventional cigarettes, and dual use in Korean adolescents and university students: Prevalence and risk factors. Drug Alcohol Depend. 2016, 168, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Western Region Drug and Alcohol Task Force. Planet Youth Growing Up in the West [Internet]. Available online: https://planetyouth.ie (accessed on 1 March 2020).
- Central Statistics Office. Census of Population 2016—Profile 3 an Age Profile of Ireland. Available online: https://www.cso.ie/en/csolatestnews/presspages/2017/census2016profile3-anageprofileofireland/ (accessed on 4 August 2020).
- Kristjansson, A.L.; Mann, M.J.; Sigfusson, J.; Thorisdottir, I.E.; Allegrante, J.P.; Sigfusdottir, I.D. Development and guiding principles of the Icelandic model for preventing adolescent substance use. Health Promot. Pract. 2019, 21, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.; Campbell, R.; Hildon, Z.; Hobbs, L.; Michie, S. Theories of behaviour and behaviour change across the social and behavioural sciences: A scoping review. Health Psychol. Rev. 2015, 9, 323–344. [Google Scholar] [CrossRef] [PubMed]
- Kristjansson, A.L.; James, J.E.; Allegrante, J.P.; Sigfusdottir, I.D.; Helgason, A.R. Adolescent substance use, parental monitoring, and leisure-time activities: 12-year outcomes of primary prevention in Iceland. Prev. Med. 2010, 51, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Dean, D.G. Alienation: Its meaning and measurement. Am. Sociol. Rev. 1961, 26, 753–758. [Google Scholar] [CrossRef]
- Bernburg, J.G.; Thorlindsson, T. Community structure and adolescent delinquency in Iceland: A contextual analysis. Criminology 2007, 45, 415–444. [Google Scholar] [CrossRef]
- Chaffee, B.W.; Couch, E.T.; Gansky, S.A. Trends in characteristics and multi-product use among adolescents who use electronic cigarettes, United States 2011–2015. PLoS ONE 2017, 12, e0177073. [Google Scholar] [CrossRef]
- The Economic and Social Research Institute. Growing Up in Ireland. Key Findings: Child Cohort at 17/18 Years. Risky Health Behaviours and Sexual Activity; Report No. 4; The Economic and Social Research Institute: Dublin, Ireland, 2016; Available online: https://www.esri.ie/system/files/media/file-uploads/2016-11/SUSTAT59.pdf (accessed on 17 June 2020).
- O’brien, D.; Long, J.; Lee, C.; Mccarthy, A.; Quigley, J. Electronic Cigarette Use and Tobacco Cigarette Smoking Initiation in Adolescents: An Evidence Review; Health Research Board: Dublin, Ireland, 2020. Available online: https://www.hrb.ie/fileadmin/2._Plugin_related_files/Publications/2020_publication-related_files/2020_HIE/Evidence_Centre/Electronic_cigarette_use_and_tobacco_cigarette_smoking_initiation_in_adolescents.pdf (accessed on 15 October 2020).
- Ren, M.; Lotfipour, S. Nicotine gateway effects on adolescent substance use. West. J. Emerg. Med. 2019, 20, 696–709. [Google Scholar] [CrossRef]
- Veliz, P.T.; McCabe, S.E.; McCabe, V.V.; Boyd, C.J. Adolescent sports participation, e-cigarette use, and cigarette smoking. Am. J. Prev. Med. 2017, 53, e175–e183. [Google Scholar] [CrossRef]
- Miech, R.; Patrick, M.E.; O’Malley, P.M.; Johnston, L.D. What are kids vaping? Results from a national survey of US adoles-cents. Tob. Control 2017, 26, 386–391. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Valid | Total | Non-User | E-Cig Only | Cig Only | Dual-User | p | |
|---|---|---|---|---|---|---|---|
| 4422 | 3447 | 225 | 339 | 411 | |||
| Sociodemographic | n | n (%) | |||||
| Gender | 4407 | ||||||
| Male | 2170 (49.2%) | 1596 (46.5%) | 155 (68.9%) | 164 (48.5%) | 255 (62.3%) | ||
| Female | 2237 (50.8%) | 1839 (53.5%) | 70 (31.1%) | 174 (51.5%) | 154 (37.7%) | <0.001 | |
| Maternal education | 4409 | ||||||
| Primary | 308 (7%) | 199 (5.8%) | 23 (10.3%) | 39 (11.6%) | 47 (11.5%) | ||
| Secondary | 1121 (25.4%) | 858 (24.9%) | 57 (25.4%) | 84 (25%) | 122 (29.8%) | ||
| Tertiary | 2291 (52.0%) | 1874 (54.5%) | 89 (39.7%) | 159 (47.3%) | 169 (41.3%) | ||
| Did not know | 689 (15.6%) | 509 (14.8%) | 55 (24.6%) | 54 (16.1%) | 71 (17.4%) | <0.001 | |
| Family-related factors | |||||||
| Parent smokes | 4397 | ||||||
| Yes | 1172 (26.7%) | 766 (22.3%) | 82 (36.8%) | 127 (37.7%) | 197 (48.9%) | ||
| No | 3225 (73.3%) | 2668 (77.7%) | 141 (63.2%) | 210 (62.3%) | 206 (51.1%) | <0.001 | |
| Parent reaction to cig use | 4374 | ||||||
| Totally/very against | 4113 (94%) | 3315 (97.2%) | 212 (94.6%) | 284 (84.3%) | 302 (75.3%) | <0.001 | |
| Rather/would not care | 261 (6.0%) | 97 (2.8%) | 12 (5.4%) | 53 (15.7%) | 99 (24.7%) | ||
| Parental supervision | 4422 | ||||||
| Mean (SD) | 6.92 (1.39) | 7.17 (1.19) | 6.42(1.52) | 6.14(1.58) | 5.74(1.78) | <0.001 | |
| Peer-related factors | |||||||
| Smoke to fit in | 4414 | ||||||
| Yes | 610 (13.8%) | 261 (7.6%) | 43 (19.2%) | 125 (36.9%) | 181 (44.3%) | ||
| No | 3804 (86.2%) | 3181 (92.4%) | 181 (80.8%) | 214 (63.1%) | 228 (55.7%) | <0.001 | |
| Friends who smoke | 4354 | ||||||
| None | 1269 (29.1%) | 1213 (35.7%) | 33 (14.9%) | 9 (2.7%) | 14 (3.5%) | ||
| A few/some | 2487 (57.1%) | 1952 (57.5%) | 141 (63.5%) | 218 (64.7%) | 176 (44.2%) | ||
| Most/almost all | 598 (13.7%) | 232 (6.8%) | 48 (21.6%) | 110 (32.6%) | 208 (52.3%) | <0.001 | |
| Community/leisure | |||||||
| Value for social norms | 4398 | ||||||
| Mean (SD) | 22.20 (5.79) | 22.94 (5.66) | 21.47(5.48) | 19.70(5.31) | 18.40(5.38) | <0.001 | |
| Team sport participation | 4351 | ||||||
| Almost never | 1599 (36.8%) | 1194 (35.1%) | 64 (29.2%) | 163 (48.7%) | 178 (44.6%) | ||
| 1–3 times/week | 1716 (39.4%) | 1360 (40.0%) | 96 (43.8%) | 107 (31.9%) | 153 (38.3%) | ||
| ≥4 times/week | 1036 (23.8%) | 844 (24.8%) | 59 (26.9%) | 65 (19.4%) | 68 (17.0%) | <0.001 | |
| Individual | |||||||
| Academic achievement | 4414 | ||||||
| Below average | 439 (9.9%) | 248 (7.2%) | 42 (18.7%) | 51 (15.0%) | 98 (23.8%) | ||
| Average | 1730 (39.2%) | 1275 (37.1%) | 96 (42.7%) | 165 (48.7%) | 194 (47.2%) | ||
| Above average | 2245 (50.9%) | 1916 (55.7%) | 87 (38.6%) | 123 (36.3%) | 119 (29.0%) | <0.001 | |
| Mental health | 4408 | ||||||
| Good or very good | 2626 (59.6%) | 2165 (62.9%) | 131 (58.2%) | 152 (45.1%) | 178 (44.0%) | ||
| Moderate | 1058 (24.0%) | 796 (23.1%) | 57 (25.3%) | 98 (29.1%) | 107 (26.4%) | ||
| Bad or very bad | 724 (16.4%) | 480 (13.9%) | 37 (16.4%) | 87 (25.8%) | 120 (29.6%) | <0.001 | |
| Valid | Total | Male | Female | p Value | |
|---|---|---|---|---|---|
| n (% of Total) | n (% of Males) | n (% of Females) | |||
| Current nicotine product user | 4412 | 977 (22.1%) | 577 (26.6%) | 400 (17.9%) | <0.001 |
| Ever nicotine product user | 4419 | 2160 (48.9%) | 1173 (53.9%) | 987 (44.0%) | <0.001 |
| Conventional Cigarettes | |||||
| Ever use | 4410 | 1652 (37.5%) | 870 (40.0%) | 782 (35.0%) | |
| Current use | 4412 | 749 (17.0%) | 420 (19.3%) | 329 (14.7%) | <0.001 |
| Electronic Cigarettes | |||||
| Ever use | 4424 | 1776 (40.1%) | 1010 (46.4%) | 766 (34.1%) | |
| Current use | 4412 | 637 (14.4%) | 412 (18.9%) | 225 (10.0%) | <0.001 |
| Current Nicotine Product Use | 4407 | ||||
| None | 3435 (77.9%) | 1596 (73.5%) | 1839 (82.2%) | ||
| E-Cigarette only | 225 (5.1%) | 155 (7.1%) | 70 (3.1%) | ||
| Conventional cigarette only | 338 (7.7%) | 164 (7.6%) | 174 (7.8%) | ||
| Dual-use | 409 (9.3%) | 255 (11.8%) | 154 (6.9%) | <0.001 | |
| Ever Nicotine Product Use | 4407 | ||||
| None | 2259 (51.3%) | 1005 (46.3%) | 1254 (56.1%) | ||
| E-cigarette only | 498 (11.3%) | 298 (13.7%) | 200 (8.9%) | ||
| Conventional cigarette only | 382 (8.7%) | 161 (7.4%) | 221 (9.9%) | ||
| Dual-use | 1268 (28.8%) | 707 (32.6%) | 561 (25.1%) | <0.001 | |
| E-Cig vs. Non | Cig vs. Non | Dual Use vs. Non | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | AOR | 95% CI | p | n (%) | AOR | 95% CI | p | n (%) | AOR | 95% CI | p | |
| Sociodemographic | ||||||||||||
| Gender | ||||||||||||
| Female | 66 (31.7) | Ref | 165 (51.6) | 143 (39.0) | ||||||||
| Male | 142 (68.3) | 2.24 | 1.61–3.10 | <0.001 | 155 (48.4) | 1.28 | 0.97–1.68 | 0.081 | 224 (61.0) | 2.36 | 1.76–3.16 | <0.001 |
| Maternal education | ||||||||||||
| Tertiary | 82 (39.4) | Ref | 154 (48.1) | 151 (41.1) | ||||||||
| Secondary | 55 (26.4) | 1.18 | 0.82–1.71 | 0.370 | 79 (24.7) | 0.82 | 0.60–1.12 | 0.209 | 109 (29.7) | 1.08 | 0.78–1.49 | 0.635 |
| Primary | 22 (10.6) | 1.89 | 1.12–3.19 | 0.016 | 37 (11.6) | 1.42 | 0.90–2.33 | 0.133 | 44 (12.0) | 1.45 | 0.91–2.31 | 0.122 |
| Did not know | 49 (23.6) | 1.40 | 0.94–2.07 | 0.100 | 50 (15.6) | 0.76 | 0.52–1.11 | 0.149 | 63 (17.2) | 0.79 | 0.54–1.15 | 0.218 |
| Family-related factors | ||||||||||||
| Parent smokes | ||||||||||||
| No | 131 (63.0) | Ref | 201 (62.8) | 184 (50.1) | ||||||||
| Yes | 77 (37.0) | 1.71 | 1.25–2.34 | <0.001 | 119 (37.2) | 1.58 | 1.20–2.09 | 0.001 | 183 (49.9) | 2.44 | 1.85–3.22 | <0.001 |
| Parental reaction to cigarette use | ||||||||||||
| Totally/very against | 196 (94.2) | Ref | 272 (85.0) | 278 (75.7) | ||||||||
| Rather against/would not care | 12 (5.8) | 1.31 | 0.69–2.51 | 0.409 | 48 (15.0) | 3.49 | 2.27–5.37 | <0.001 | 89 (24.3) | 4.65 | 3.09–7.01 | <0.001 |
| Parental supervision: mean (SD) | ||||||||||||
| 1 SD increase corresponds to | 7 (2) | 0.71 | 0.62–0.82 | <0.001 | 6 (3) | 0.63 | 0.56–0.71 | <0.001 | 6 (2) | 0.60 | 0.53–0.67 | <0.001 |
| Peer-related factors | ||||||||||||
| Feel necessary to smoke to fit in | ||||||||||||
| No | 168 (80.8) | Ref | 203 (63.4) | 213 (58.0) | ||||||||
| Yes | 40 (19.2) | 2.13 | 1.45–3.13 | <0.001 | 117 (36.6) | 4.36 | 3.25–5.83 | <0.001 | 154 (42.0) | 5.13 | 3.81–6.91 | <0.001 |
| Friends who smoke | ||||||||||||
| None | 30 (14.4) | Ref | 7 (2.2) | 13 (3.5) | ||||||||
| A few/some | 131 (63) | 2.15 | 1.45–3.13 | <0.001 | 206 (64.4) | 14.19 | 6.60–30.53 | <0.001 | 162 (44.1) | 5.41 | 3.0–9.76 | <0.001 |
| Most/almost all | 47 (22.6) | 5.19 | 3.10–8.44 | <0.001 | 107 (33.4) | 40.52 | 18.31–89.68 | <0.001 | 192 (52.3) | 31.44 | 17.06–57.92 | <0.001 |
| Community/leisure | ||||||||||||
| Value for conventional social norms: mean (SD) | ||||||||||||
| 1 SD increase corresponds to | 21 (7) | 0.95 | 0.81–1.12 | 0.535 | 19 (7) | 0.78 | 0.66–0.91 | 0.001 | 18 (7) | 0.68 | 0.57–0.79 | <0.001 |
| Team sport involvement | ||||||||||||
| Almost never | 59 (28.4) | 156 (48.8) | 162 (44.1) | |||||||||
| 1–3 times/week | 93 (44.7) | 1.34 | 0.94–1.92 | 0.105 | 102 (31.9) | 0.57 | 0.43–0.77 | <0.001 | 142 (38.7) | 0.77 | 0.57–1.05 | 0.094 |
| ≥4 times/week | 56 (26.9) | 1.31 | 0.87–1.97 | 0.199 | 62 (19.4) | 0.63 | 0.44–0.90 | 0.011 | 63 (17.2) | 0.63 | 0.43–0.93 | 0.019 |
| Individual | ||||||||||||
| Self-reported academic achievement | ||||||||||||
| Above average | 80 (38.5) | 116 (36.3) | 106 (28.9) | |||||||||
| Average | 89 (42.8) | 1.43 | 1.03–1.98 | 0.03 | 158 (49.4) | 1.58 | 1.20–2.09 | 0.001 | 175 (47.7) | 1.76 | 1.30–2.37 | <0.001 |
| Below average | 39 (18.8) | 2.53 | 1.62–3.93 | <0.001 | 46 (14.4) | 1.47 | 0.96–2.26 | 0.076 | 86 (23.4) | 2.43 | 1.62–3.63 | <0.001 |
| Self-reported mental health | ||||||||||||
| Good or very good | 120 (57.7) | 143 (44.7) | 158 (43.1) | |||||||||
| Moderate | 51(24.5) | 1.04 | 0.72–1.48 | 0.853 | 93 (29.1) | 1.13 | 0.83–1.54 | 0.44 | 99 (27.0) | 1.06 | 0.76–1.47 | 0.723 |
| Bad or very bad | 37 (17.8) | 1.16 | 0.75–1.78 | 0.506 | 84 (26.3) | 1.22 | 0.85–1.74 | 0.275 | 110 (30.0) | 1.32 | 0.92–1.89 | 0.130 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bowe, A.K.; Doyle, F.; Stanistreet, D.; O’Connell, E.; Durcan, M.; Major, E.; O’Donovan, D.; Kavanagh, P. E-Cigarette-Only and Dual Use among Adolescents in Ireland: Emerging Behaviours with Different Risk Profiles. Int. J. Environ. Res. Public Health 2021, 18, 332. https://doi.org/10.3390/ijerph18010332
Bowe AK, Doyle F, Stanistreet D, O’Connell E, Durcan M, Major E, O’Donovan D, Kavanagh P. E-Cigarette-Only and Dual Use among Adolescents in Ireland: Emerging Behaviours with Different Risk Profiles. International Journal of Environmental Research and Public Health. 2021; 18(1):332. https://doi.org/10.3390/ijerph18010332
Chicago/Turabian StyleBowe, Andrea K., Frank Doyle, Debbi Stanistreet, Emer O’Connell, Michéal Durcan, Emmet Major, Diarmuid O’Donovan, and Paul Kavanagh. 2021. "E-Cigarette-Only and Dual Use among Adolescents in Ireland: Emerging Behaviours with Different Risk Profiles" International Journal of Environmental Research and Public Health 18, no. 1: 332. https://doi.org/10.3390/ijerph18010332
APA StyleBowe, A. K., Doyle, F., Stanistreet, D., O’Connell, E., Durcan, M., Major, E., O’Donovan, D., & Kavanagh, P. (2021). E-Cigarette-Only and Dual Use among Adolescents in Ireland: Emerging Behaviours with Different Risk Profiles. International Journal of Environmental Research and Public Health, 18(1), 332. https://doi.org/10.3390/ijerph18010332