1. Introduction
Declared as a global pandemic by the World Health Organization (WHO) in March 2020, Coronavirus disease 2019 (COVID-19) defines a spectrum of conditions sustained by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) ranging from mild disease to severe pneumonia [
1,
2]. To date, there have been 115,653,459 confirmed cases of COVID-19, including 2,571,823 deaths, reported to the WHO [
3]. Italy was the first European country to be hit hard by the COVID-19 and one of the European countries registering a high number of excess deaths during the first wave of the pandemic [
4].
The safety of healthcare workers in hospitals is a major concern during the COVID-19 outbreak, since more than 124,000 infections were registered by the end of March 2020 [
5]. With respect to other health professionals, nurses are exposed for several working hours per day to infected patients, presenting with a higher risk of contracting the infection [
6]. Hence, nurses dealing with COVID-19 are exposed to increased psychological and physical pressure, as already described in previous epidemics [
7,
8]. Indeed, during a pandemic, nurses experience worries about their own health, and the health of their colleagues and family [
9]. Furthermore, in the context of a pandemic, nurses face several issues that lead to burnout and physical/psychological breakdown, such as perceived lack of defensive resources, rapidly changing advice about the contagion, and occupational and organizational preparedness to deal with the pandemic [
9].
Burnout is defined as a protracted response to relational and emotional stressors at work, characterized by different levels of exhaustion, distrust and inadequacy, which lead to a pessimistic self-concept and work approach, with low attention for patients [
10]. In particular, job burnout can be recognized as a psychological syndrome in response to working stressors: this response is constructed on three dimensions, which include exhaustion (basic individual dimension: awareness of being put under pressure and drained of both physical and emotional abilities), cynicism (interpersonal context dimension: depersonalization, disengagement from work), and reduced accomplishment (self-evaluation dimension: a feeling of ineffectiveness and lack of success at work) [
10]. Both personal and work-related factors may impact burnout.
Individual factors are identified in demographic features (age, gender, marital status), temperament, adaptive capabilities [
11,
12,
13,
14]. Work-related factors include working stress and attitude, exposition to stressful experiences, salary, social support, availability of personal protective equipment (PPE) [
13,
14]. Previous investigations found a high level of burnout in healthcare professionals on the front line against COVID-19, impacted by different occupational and socio-demographic factors [
15,
16]. In particular, the occupational factors positively associated with burnout included high workload, job stress, time pressure, and restricted support by the working organization; on the contrary, adequate PPE was reported as protective against burnout [
15,
16]. Very recent literature focused on the psychological risks of healthcare workers related to COVID-19 outbreak, describing high levels of anxiety, depression, stress, and burnout [
17,
18,
19,
20,
21]. Working in critical situations and in a working environment characterized by a continuous contact with pain and death increases the risk of burnout for healthcare workers. Based on these theoretical premises, this study focused on the level of burnout in nurses working in an Italian University Hospital during the first wave of COVID-19 pandemic, aiming to identify associated factors. The theoretical framework underpinning our study is based on the Maslach theory of burnout, which is supported by most of the literature on burnout in nursing [
22]. To identify potential predictors of burnout, we aimed attention at both demographic and occupational variables, including the working department and the exposure risk to COVID-19. We also considered the perception of risk of COVID-19 infection by nurses, and the percentage of them thinking about quitting their job.
2. Methods
2.1. Study Design and Sampling
This was designed as a web-based cross-sectional study addressed to nurses working at the University Hospital “Policlinico Riuniti” in Foggia, Italy. Data were collected from 1 June to 30 September 2020 through an online questionnaire. The study was approved by our Institutional Review Board at the Ospedali Riuniti in Foggia and performed according to the Declaration of Helsinki. Online consent was obtained from all the participants.
The sample size was estimated considering α at 0.05, a medium effect size of 0.15, power of 90%, and the number of predictors at 18 for a linear multiple regression analysis; according to these input variables, the minimum sample size required for this study was 170. Power calculation was performed with the PS Power and Sample Size Calculations, version 3. Four hundred and eight nurses were invited to complete the survey. Of all the participants, 293 (71.8%) replied to the survey with completely answered questionnaires and were used as valid data.
2.2. Measurements
The online questionnaire was organized in sections aimed at collecting the following information:
Demographic variables and information regarding working Unit, professional experience, chronic diseases, previous SARS-CoV-2 infection, or contact with COVID-19 patients;
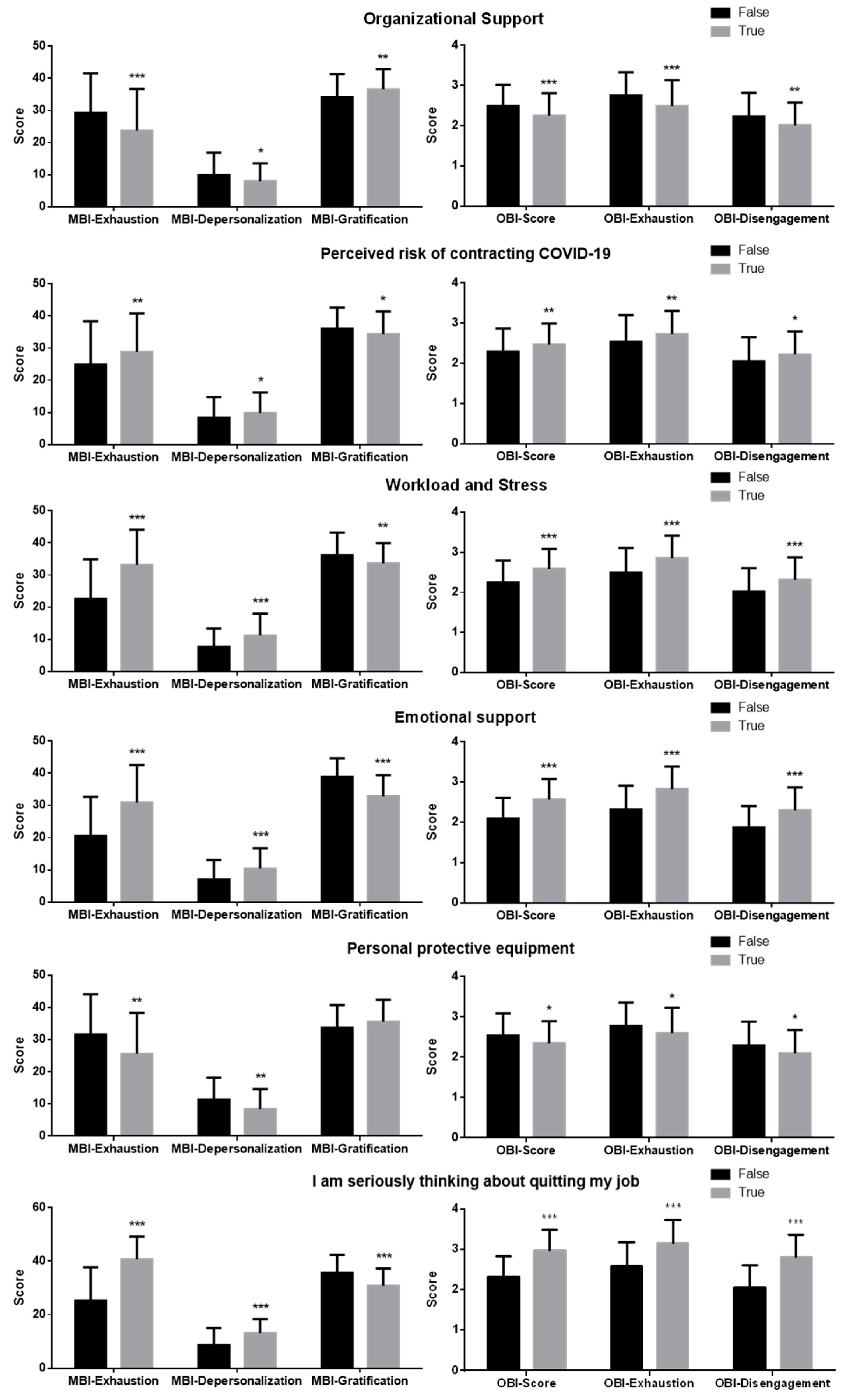
True/false statements on the impact of COVID-19 outbreak according to factors such as organizational support, perceived risk of contracting COVID-19, workload and stress, social relationship, emotional support, perceived fatality of COVID-19, personal protective equipment, consideration of leaving the job [
7];
The Maslach Burnout Inventory–Humans Service Survey (MBI-HSS), composed of questions related to occupational burnout scored by seven level frequency ratings ranging from 0 (never) to 6 (daily). The MBI analyzes three dimensions of burnout: emotional exhaustion (EE), depersonalization (D), and personal gratification (PG). The MBI cut-off values chosen to categorize scores in low, medium, and high were as follows: for EE, low ≤ 15, medium 16–26, high ≥ 27; for D, low ≤ 8, medium 9–13, high ≥ 14; for PG, low ≥ 37, medium 36–31, high ≤ 30 (this scale is inverted; the higher the PG, the lower the burnout) [
23];
The Oldenburg Burnout Inventory (OBI), composed of 16 items related to emotional exhaustion and disengagement from work, scored by a five-point scale ranging from 1 (strongly disagree) to 5 (strongly agree). The OBI analyzes two dimensions of burnout: disengagement and exhaustion. Scores ≥ 2.1 on disengagement and ≥2.25 on exhaustion were considered as high [
24].
The questionnaire included both the MBI-HSS and the OBI to improve the psychometric properties and reduce method artifacts due to one-sided questionnaire [
24].
The questionnaire was translated by a mother tongue Italian health professional, and further translated back by an independent, mother-tongue English speaker who did not dispose of prior information about it. Then, the questionnaire was initially forwarded to a team of experts (two assistant professors, two associate professors, and a full professor) for internal content validity. Experts considered aims, content (demographic and occupational information, and working factors), and appropriate use of language. Then, the questionnaire was pilot tested on 20 nurses. The reliability and validity tests were applied for the pilot test, and Cronbach’s α and McDonald ω greater than 0.8 for all scales were considered as acceptable. In particular, Cronbach’s α and McDonald ω for the working factors questionnaire section were 0.87 and 0.89, respectively.
2.3. Statistical Analysis
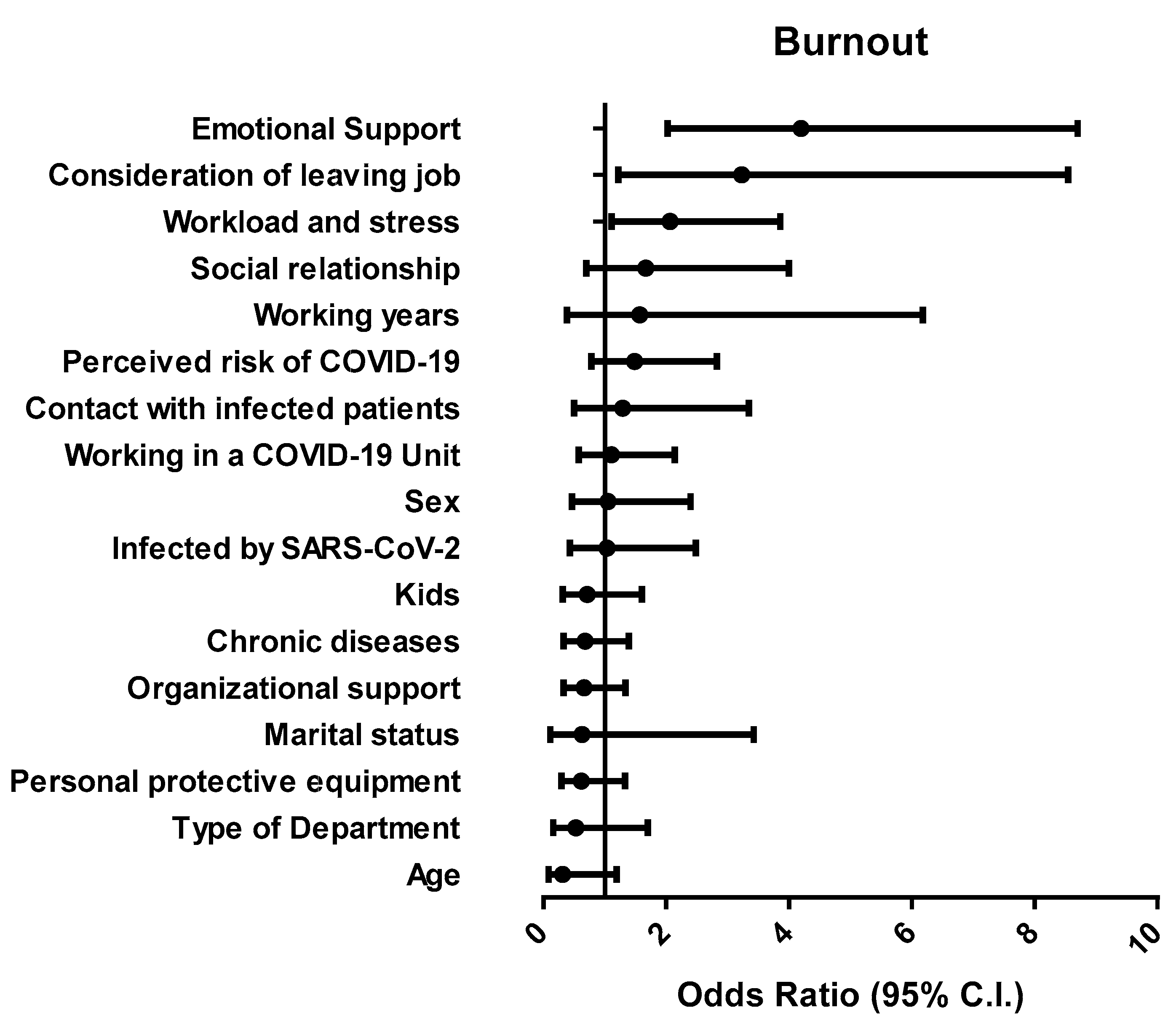
Data were expressed as count and percentages for categorical variables, and as mean ± standard deviation of the mean (SDM) for quantitative variables. Gaussian distribution of the samples was evaluated by the Kolgomorov–Smirnov test. Scale reliability and validity were assessed with Cronbach’s α and McDonald ω. Pearson’s correlation coefficient was used to correlate the MBI and OBI scores. The significance of differences was analyzed using independent t-tests (continuous variables, two groups), one-way analysis of variance (ANOVA) and Tukey as a post-hoc test (continuous variables, more than two groups), or in contingency tables by Pearson’s chi-square test and Fisher exact test (categorical variables). To explore factors associated with COVID-19-related burnout, multiple regression was performed using the enter method with input variables which resulted significant in the difference testing and correlation analysis. In the model, the MBI measurement was used as a dependent variable, while categorical variables such true/false statements were considered as “factors”. Finally, to test the mediating effect of working factors, a mediation analysis was performed, using the JASP version 0.14.1. All other analyses were performed using SPSS ver. 23.0 statistical software for Windows.
4. Discussion
The COVID-19 pandemic caused an overall rise of psychological problems, including anxiety, depressive disorders, insomnia, and burnout in health care workers [
17]. This study highlighted the psychological impact of the first wave of COVID-19 on nurses working in an Italian University hospital. Levels of burnout and exhaustion were consistent, since we found that almost 90% of participants met the criteria for medium/high burnout, while almost 70% exhibited emotional exhaustion.
Burnout is one of the most important determinants for discomfort and well-being alterations in health professionals. A consensus has recently defined burnout as an occupational, physical, and emotional exhaustion associated with continued exposure to work-related issues [
26]. Indeed, burnout causes reduced commitment to job-related activities, de-personalization, and decreased working abilities [
27]. Causes of burnout are frequently distinguished in individual and work-related variables [
28]. The present study focused on the identification of determinant factors of burnout in nurses to provide information necessary to reduce and prevent it during the ensuing waves of COVID-19 outbreak. To this, we adapted scales from previous investigations which measured burnout in other pandemics [
7,
8]. Psychometric properties of both MBI-HSS and OBI were previously reviewed, showing satisfactory content validity, structural validity, and internal consistency [
29]. Pandemics exert a significant psychological and emotional impact on nurses, who are indispensable to the healthcare support [
30]. Indeed, pandemics worsen the stress perceived by nurses, since they face strong physical, cognitive, and emotional demands [
31,
32]. According to mortality data, the first wave of the COVID-19 pandemic in Italy started on February 2020 and was considered as ended in the second half of May 2020 [
33]. Even though less than 40% of participants were working in COVID-19 Units, 83.4% cared for COVID-19 patients, and 14% got infected by SARS-CoV-2. A small but significant proportion of nurses (16%) considered they should not care for COVID-19 patients, and 12.9% of participants were thinking about being transferred to different Units or quitting their job.
A previous study analyzed burnout in frontline nurses during the first wave of pandemics in Wuhan, finding that about half of the participants reported moderate/high levels according to the MBI [
34]. Another study used the MBI in nurses during the first wave of pandemics in Japan, finding an overall burnout prevalence of 31.4% [
35]. In our study, we used the OBI in addition to the MBI, identifying burnout in nurses presenting with high scores according to both tools. Of note, the convergent validity of both instruments has been previously studied [
24]. Our results showed a 36% prevalence of burnout, according to both questionnaires. Among all the burnout sub-domains analyzed by both MBI and OBI, exhaustion was reported in more than 70% of nurses, with a 50% concordance between tests. A study performed on Italian nurses before the pandemic estimated moderate/high-frequency level of 47.5% for exhaustion, 54.7% for depersonalization, and 57.3% for personal unsatisfaction [
36]. Results from another Italian study suggested that working with COVID-19 patients and in areas with high rates of contagion is associated with high levels of stress, burnout, secondary trauma, anxiety, and depression in healthcare professionals [
19]. Even though we could not directly compare our results with previous data, the present study strongly suggests that the COVID-19 outbreak increased the frequency of burnout in nurses.
To address the causes of burnout in nurses during the first wave of COVID-19 pandemics, we considered several demographic and occupational factors, as well as seven working-related factors as potential predictors.
Of note, emotional support, consideration of leaving job, and workload and stress were predictive of burnout. Fears about personal safety and wellbeing of the family have been previously described as determinant factors for burnout related to COVID-19 [
37]. The COVID-19 pandemics caused a sudden rise in hospital admissions, with a consequent impact of workload and stress in nurses. A previous study suggested that each extra patient added to the workload of a nurse was associated with a 23% increase in burnout [
38]. On the contrary, we do not retain that shift work was a factor related to burnout, since no differences were reported in burnout-related scores between nurses working in different departments. Interestingly, exposure to patients infected by COVID-19 or working in COVID-19 department did not result as predictive factors for burnout, differently from previous studies [
8,
19,
39]. Stress is a factor significantly influencing burnout in several studies [
11,
12]. This study indicates that work-related stress induced by the first wave of COVID-19 pandemics is a factor associated with burnout in nurses. Thus, during the spread of an emerging infectious disease, management of workload and stress would contribute to prevent or reduce nurses’ burnout.
Other than workload and stress, employer consideration and support from family and friends were also predictive of burnout in nurses. Indeed, attention by the employer and assistance from colleagues or family were described as protecting effects that may directly or indirectly reduce burnout [
13,
14]. Thus, these aspects should be considered for further research in future investigations.
It is worth noting that factors significantly linked to burnout (workload and stress, consideration of leaving the job, and emotional support) were predictive of burnout even before the pandemic effect of COVID-19 [
13,
14,
38]. On the contrary, factors directly related to COVID-19 (such as perceived risk or fatality of the disease) did not result significantly associated to burnout. A possible explanation of this apparently paradoxical result may be offered by the impact of pandemic on motivating the dedication of nurses, increasing their empathy for patients, as well as providing a sense of satisfaction, with consequent decrease of burnout-related dimensions. Taken together, the results of this study indicate that the COVID-19 pandemics led to an exacerbation of the ongoing underlying problems that were pre-existing workplace factors contributing to nurse burnout. The final message of this investigation synergizes with similar studies in promoting immediate interventions for the management of psychological issues in the workplace [
17,
18,
19,
20,
21].
Limitations of our study include the recruitment of a small number of participants from a single hospital in Italy, so that these findings cannot be generalizable to other regions or countries. Moreover, data obtained by self-administered questionnaires were not related to clinical data on healthcare professionals’ health. Further, work factors considered in the study were assessed as true or false statements rather than on a Likert-type scale, so that correlation or linear regression analysis could not be performed. The relatively small variance explained by the significant factors, moderate concordance between tests examining similar concepts, and the possible influences of the large number of variables in the regression model represent additional limitations of this investigation. Finally, levels of burnout were not measured before the COVID-19 pandemics; thus, no comparisons on prevalence changes were possible.


 ,
, 



{kind=link}
{kind=link}