
Intimate Partners Violence against Women during a COVID-19 Lockdown Period: Results of an Online Survey in 7 Provinces of the Democratic Republic of Congo


 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Design
2.2. Study Instrument and Participants’ Recruitment
2.3. Study Variables
- Age: this is the respondent’s age at the last birthday; this variable was categorized into four modalities: 18–<30 years, 30–39 years, 40–49 years, and ≥50.
- Gender: this was a dummy variable categorized into 2 modalities: male and female.
- Marital status: this was the civil status of the respondent, a nominal variable categorized into 5 modalities: married, single, divorced, common-law, and widower. This variable was later dichotomized into two modalities, either the respondent lives alone or the respondent married/living together with a sexual partner.
- Level of education: this is the highest level of education attained by the respondent; this variable had three modalities, namely primary school, secondary/baccalaureate, and university level.
- Religion: this is the religious belief of the interviewee. This variable was categorized into 5 modalities: none, Protestant/Adventist, Catholic, Pentecostal, and other religions. This variable was re-categorized into three groups: Catholic, Pentecostal, and others.
- Belonging to the health sector: this was a dichotomous variable describing whether the respondent was a student/worker in the health sector (yes vs. no).
2.4. Data Management, Processing and Analysis
2.5. Ethical Considerations
3. Results
3.1. Sociodemographic and Health Characteristics of Women with Sexual Partners
3.2. Level of Intimate Partners’ Violence
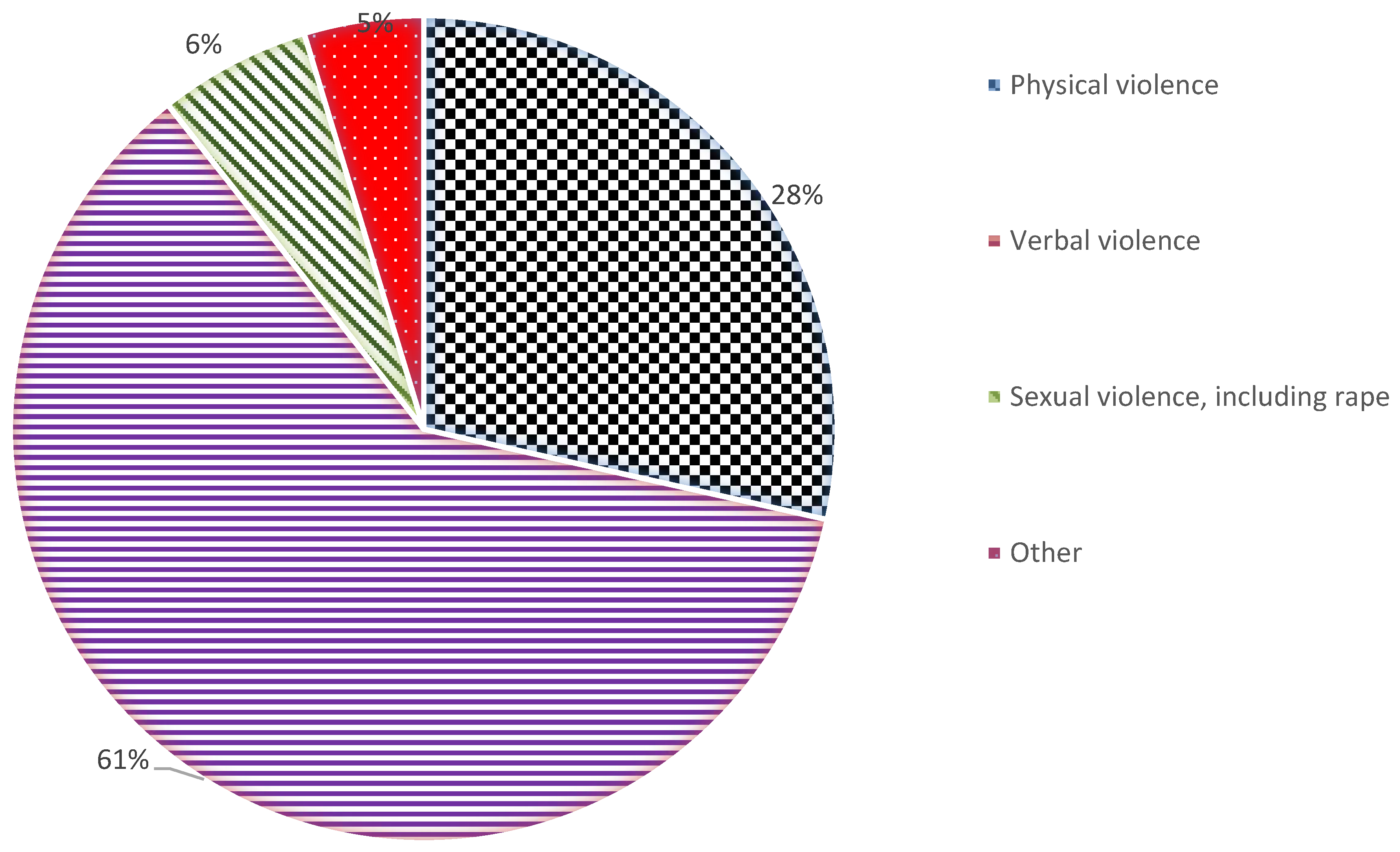
3.3. Types of Intimate Partners’ Violence
3.4. Factors Associated with Intimate Partners’ Violence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV). Available online: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 29 June 2020).
- Kasambule, A. Controversial Communication Around COVID-19 in DRC; Pulitzer Center: Washington, DC, USA, 2020; Available online: https://pulitzercenter.org/stories/controversial-communication-around-covid-19-drc (accessed on 20 March 2021).
- Evans, M.L.; Lindauer, M.; Farrell, M.E. A Pandemic within a Pandemic—Intimate Partner Violence during Covid-19. N. Engl. J. Med. 2020, 383, 2302–2304. [Google Scholar] [CrossRef]
- Miller, E.; McCaw, B. Intimate Partner Violence. N. Engl. J. Med. 2019, 380, 850–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tlapek, S.M. Women’s Status and Intimate Partner Violence in the Democratic Republic of Congo. J. Interpers. Violence 2014, 30, 2526–2540. [Google Scholar] [CrossRef]
- McClintock, H.F.; Trego, M.L.; Wang, E.M. Controlling Behavior and Lifetime Physical, Sexual, and Emotional Violence in sub-Saharan Africa. J. Interpers. Violence 2019. [Google Scholar] [CrossRef] [PubMed]
- Bradbury-Jones, C.; Isham, L. The pandemic paradox: The consequences of COVID-19 on domestic violence. J. Clin. Nurs. 2020, 29, 2047–2049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Telles, L.E.D.B.; Valença, A.M.; Barros, A.J.; Da Silva, A.G. Domestic violence in the COVID-19 pandemic: A forensic psychiatric perspective. Rev. Bras. de Psiquiatr. 2020. [Google Scholar] [CrossRef]
- Johnson, D.M.; Zlotnick, C. Remission of PTSD after victims of intimate partner violence leave a shelter. J. Trauma. Stress 2012, 25, 203–206. [Google Scholar] [CrossRef]
- Silva, E.P.; Lemos, A.; Andrade, C.H.; Ludermir, A.B. Intimate partner violence during pregnancy and behavioral problems in children and adolescents: A meta-analysis. J. Pediatr. 2018, 94, 471–482. [Google Scholar] [CrossRef]
- McGregor, M.J.; Wiebe, E.; Marion, S.A.; Livingstone, C. Why don’t more women report sexual assault to the police? Can. Med. Assoc. J. 2000, 162, 659–660. [Google Scholar]
- Sylaska, K.M.; Edwards, K.M. Disclosure of intimate partner violence to informal social support network members: A review of the literature. Trauma Violence Abuse 2014, 15, 3–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dicola, D.; Spaar, E. Intimate Partner Violence. Am. Fam. Physician 2016, 94, 646–651. [Google Scholar]
- The World Bank. Method Matters: Underreporting of Intimate Partner Violence in Nigeria and Rwanda; The World Bank: NY, USA, 2020; Available online: https://openknowledge.worldbank.org/handle/10986/33876 (accessed on 24 March 2021).
- Moreira, D.N.; da Costa, M.P. The impact of the Covid-19 pandemic in the precipitation of intimate partner violence. Int. J. Law Psychiatry 2020, 71, 101606. [Google Scholar] [CrossRef] [PubMed]
- Izugbara, C.O.; Obiyan, M.O.; Degfie, T.T.; Bhatti, A. Correlates of intimate partner violence among urban women in sub-Saharan Africa. PLoS ONE 2020, 15, e0230508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roesch, E.; Amin, A.; Gupta, J.; García-Moreno, C. Violence against women during covid-19 pandemic restrictions. BMJ 2020, 369, m1712. [Google Scholar] [CrossRef] [PubMed]
- Barbara, G.; Facchin, F.; Micci, L.; Rendiniello, M.; Giulini, P.; Cattaneo, C.; Vercellini, P.; Kustermann, A. COVID-19, Lockdown, and Intimate Partner Violence: Some Data from an Italian Service and Suggestions for Future Approaches. J. Women’s Health 2020, 29, 1239–1242. [Google Scholar] [CrossRef]
- Boserup, B.; McKenney, M.; Elkbuli, A. Alarming trends in US domestic violence during the COVID-19 pandemic. Am. J. Emerg. Med. 2020, 38, 2753–2755. [Google Scholar] [CrossRef]
- Leite, F.M.C.; Luis, M.A.; Amorim, M.H.C.; Maciel, E.L.N.; Gigante, D.P. Violência contra a mulher e sua associação com o perfil do parceiro íntimo: Estudo com usuárias da atenção primária. Rev. Bras. Epidemiol. 2019, 22, e190056. [Google Scholar] [CrossRef] [Green Version]
- Ditekemena, J.; Doumbia, S.; Ebrahim, S.H. COVID-19’s final frontier: The central Africa region. Travel Med. Infect. Dis. 2020, 37, 101694. [Google Scholar] [CrossRef]
- Douglas, M.; Katikireddi, S.V.; Taulbut, M.; McKee, M.; McCartney, G. Mitigating the wider health effects of covid-19 pandemic response. BMJ 2020, 369, m1557. [Google Scholar] [CrossRef]
- Ditekemena, J.D.; Nkamba, D.M.; Muhindo, H.M.; Siewe, J.N.F.; Luhata, C.; van den Bergh, R.; Kitoto, A.T.; van Damme, W.; Muyembe, J.J.; Colebunders, R.; et al. Factors associated with adherence to COVID-19 prevention measures in the Democratic Republic of Congo (DRC): Results of an online survey. BMJ Open 2021, 11, e043356. [Google Scholar] [CrossRef]
- Ditekemena, J.D.; Mavoko, H.M.; Obimpeh, M.; Van Hees, S.; Siewe Fodjo, J.N.; Nkamba, D.M.; Tshefu, A.; Van Damme, W.; Muyembe, J.J.; Colebunders, R. Adherence to COVID-19 prevention measures in the Democratic Republic of the Congo, results of two consecutive online surveys. Int. J. Environ. Res. Public Health 2021, 18, 2525. [Google Scholar] [CrossRef]
- Portet, S. A primer on model selection using the Akaike Information Criterion. Infect. Dis. Model. 2020, 5, 111–128. [Google Scholar] [CrossRef] [PubMed]
- Toma, L.A. Kasai: The Forgotten Province of DRC Gender Assessment October–November 2017; OXFAM: Nairobi, Kenya, 2018; Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/rr-kasai-drc-gender-assessment-020218-en.pdf (accessed on 27 March 2021).
- Barnawi, F.H. Prevalence and risk factors of domestic violence against women attending a primary care center in Riyadh, Saudi Arabia. J. Interpers. Violence 2017, 32, 1171–1186. [Google Scholar] [CrossRef]
- Gerino, E.; Caldarera, A.M.; Curti, L.; Brustia, P.; Rollè, L. Intimate Partner Violence in the Golden Age: Systematic Review of Risk and Protective Factors. Front. Psychol. 2018, 9, 1595. [Google Scholar] [CrossRef]
- Yakubovich, A.R.; Stöckl, H.; Murray, J.; Melendez-Torres, G.J.; Steinert, J.I.; Glavin, C.E.Y.; Humphreys, D.K. Risk and protective factors for intimate partner violence against women: Systematic review and meta-analyses of prospective-longitudinal studies. Am. J. Public Health 2018, 108, e1–e11. [Google Scholar] [CrossRef] [PubMed]
- Rome, E.S.; Miller, E. Intimate Partner Violence in the Adolescent. Pediatr. Rev. 2020, 41, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Urada, L.A.; Malow, R.M.; Santos, N.C.; Morisky, N.E. Age Differences among Female Sex Workers in the Philippines: Sexual Risk Negotiations and Perceived Manager Advice. AIDS Res. Treat. 2012, 2012, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, E.; Lasch, K.E.; Chandra, P.; Lee, J. The relation of family violence, employment status, welfare benefits, and alcohol drinking in the United States. West. J. Med. 2001, 174, 317–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, A.G.; Barnhart, J.E. It Takes Two: The Role of Partner Ethnicity and Age Characteristics on Condom Negotiations of Heterosexual Chinese and Filipina American College Women. AIDS Educ. Prev. 2006, 18, 68–80. [Google Scholar] [CrossRef]
- Zeng, J.; Jiang, M.; Yuan, M. Environmental Risk Perception, Risk Culture, and Pro-Environmental Behavior. Int. J. Environ. Res. Public health 2020, 17, 1750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riggs, D.S.; Caulfield, M.B.; Street, A.E. Risk for domestic violence: Factors associated with perpetration and victimization. J. Clin. Psychol. 2000, 56, 1289–1316. [Google Scholar] [CrossRef]
- Wada, K.; Higuchi, Y.; Smith, D.R. Socioeconomic status and self-reported health among middle-aged Japanese men: Results from a nationwide longitudinal study. BMJ Open 2015, 5, e008178. [Google Scholar] [CrossRef]
- Jewkes, R. Intimate partner violence: Causes and prevention. Lancet 2002, 359, 1423–1429. [Google Scholar] [CrossRef]
- Mberu, B.U.; Haregu, T.N.; Kyobutungi, C.; Ezeh, A.C. Health and health-related indicators in slum, rural, and urban communities: A comparative analysis. Glob. Health Action 2016, 9, 33163. [Google Scholar] [CrossRef] [PubMed]
- Bjelica, A.; Cetkovic, N.; Trninic-Pjevic, A.; Mladenović-Segedi, L. The phenomenon of pregnancy—A psychological view. Ginekol. Pol. 2018, 89, 102–106. [Google Scholar] [CrossRef]
- Shamu, S.; Abrahams, N.; Temmerman, M.; Musekiwa, A.; Zarowsky, C. A systematic review of African studies on intimate partner violence against pregnant women: Prevalence and risk factors. PLoS ONE 2011, 6, e17591. [Google Scholar] [CrossRef] [Green Version]
- Seedat, M.; Ashley Van, N.; Rachel, J.; Shahnaaz, S.; Kopano, R. Violence and injuries in South Africa: Prioritising an agenda for prevention. Lancet 2009, 374, 1011–1022. [Google Scholar] [CrossRef]
- World Health Organization. Understanding and Addressing Violence against Women; WHO: Geneva, Switzerland, 2012; Available online: https://apps.who.int/iris/bitstream/handle/10665/77432/WHO_RHR_12.36_eng.pdf;sequence=1 (accessed on 24 March 2021).
- Chisholm, C.A.; Bullock, L.; Ferguson, J.E. (Jef) Intimate partner violence and pregnancy: Epidemiology and impact. Am. J. Obstet. Gynecol. 2017, 217, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Chisholm, C.A.; Bullock, L.; Ferguson, J.E. (Jef) Intimate partner violence and pregnancy: Screening and intervention. Am. J. Obstet. Gynecol. 2017, 217, 145–149. [Google Scholar] [CrossRef]
- Ahmad, N.A.; Silim, U.A.; Rosman, A.; Mohamed, M.; Chan, Y.Y.; Kasim, N.M.; Yusof, M.; Razak, M.A.A.; Omar, M.; Aziz, F.A.A.; et al. Postnatal depression and intimate partner violence: A nationwide clinic-based cross-sectional study in Malaysia. BMJ Open 2018, 8, e020649. [Google Scholar] [CrossRef]
- Jewkes, R.; Abrahams, N. The epidemiology of rape and sexual coercion in South Africa: An overview. Soc. Sci. Med. 2002, 55, 1231–1244. [Google Scholar] [CrossRef]
- Eysenbach, G.; Wyatt, J. Using the Internet for Surveys and Health Research. J. Med. Internet Res. 2002, 4, e13. [Google Scholar] [CrossRef] [PubMed]
- United Nations Women. Violence Against Women and Girls: The Shadow Pandemic; UN Women: UY, USA, 2020; Available online: https://www.unwomen.org/en/news/stories/2020/4/statement-ed-phumzile-violence-against-women-during-pandemic (accessed on 29 April 2021).
- Glumbíková, K.; Gojová, A. Transformation of the identity of homeless women with an experience of domestic violence: Changing from a victim to a survivor: An example from shelters for mothers in the Czech Republic. J. Soc. Work Pract. 2019, 34, 151–162. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Total (%) | Province | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Haut-Katanga | Kasaï-Central | Kasaï-Oriental | Kinshasa | Kongo-Central | Kwilu | Nord-Kivu | |||
| Total n (%) | 4131 (100) | 511 (12.4) | 621 (15.0) | 578 (14.0) | 633 (15.3) | 616 (14.9) | 689 (16.7) | 483 (11.7) | |
| Gender, n = 4134 (%) | |||||||||
| Male | 1304 (31.6) | 7 (1.4) | 31 (5.0) | 137 (23.7) | 289 (45.7) | 297 (48.2) | 337 (48.9) | 206 (42.6) | <0.001 |
| Female | 2827 (68.4) | 504 (98.6) | 590 (95.0) | 441 (76.3) | 344 (54.3) | 319 (51.8) | 352 (51.1) | 277 (57.4) | |
| Women with partner, n = 2830 (%) | |||||||||
| Yes | 2002 (73.9) | 496 (98.4) | 565 (95.8) | 410 (93.0) | 200 (58.1) | 102 (32.0) | 130 (36.9) | 186 (67.2) | <0.001 |
| No | 738 (26.1) | 8 (1.6) | 25 (4.2) | 31 (7.0) | 144 (41.9) | 217 (68.0) | 222 (63.1) | 91 (32.8) | |
| Characteristics | Province | Total | ||||||
|---|---|---|---|---|---|---|---|---|
| Haut-Katanga | Kasaï-Central | Kasaï-Oriental | Kinshasa | Kongo-Central | Kwilu | Nord-Kivu | ||
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Total | 479 (23.9) | 563 (28.1) | 406 (20.3) | 171 (8.5) | 105 (5.2) | 126 (6.3) | 152 (7.6) | 2002 (100.0) |
| Age | ||||||||
| <30 | 153 (31.9) | 32 (5.7) | 181 (44.6) | 42 (24.6) | 31 (29.5) | 33 (26.2) | 53 (34.9) | 525 (26.2) |
| 30–39 | 178 (37.2) | 324 (57.5) | 110 (27.1) | 32 (18.7) | 31 (29.5) | 52 (41.3) | 67 (44.1) | 794 (39.7) |
| 40–49 | 117 (24.4) | 157 (27.9) | 73 (18.0) | 58 (33.9) | 32 (30.5) | 27 (21.4) | 19 (12.5) | 483 (24.1) |
| ≥50 | 31 (6.5) | 50 (8.9) | 42 (10.3) | 39 (22.8) | 11 (10.5) | 14 (11.1) | 13 (8.6) | 200 (10.0) |
| Education | ||||||||
| Primary | 14 (2.9) | 0 (0.0) | 60 (14.8) | 15 (8.8) | 11 (10.5) | 17 (13.5) | 11 (7.2) | 128 (6.4) |
| Secondary | 433 (90.4) | 485 (86.1) | 298 (73.4) | 115 (67.3) | 37 (35.2) | 67 (53.2) | 61 (40.1) | 1496 (74.7) |
| University | 32 (6.7) | 78 (13.9) | 48 (11.8) | 41 (24.0) | 57 (54.3) | 42 (33.3) | 80 (52.6) | 378 (18.9) |
| Marital | ||||||||
| Legally married/Cohabitation | 479 (100.0) | 563 (100.0) | 406 (100.0) | 163 (95.3) | 100 (95.2) | 116 (92.1) | 151 (99.3) | 1978 (98.8) |
| Single/Widow or Divorced | 0 (0.0) | 0 (0.0) | 0 (0.0) | 8 (4.7) | 5 (4.8) | 10 (7.9) | 1 (0.7) | 23 (1.2) |
| Religion | ||||||||
| Catholic | 261 (54.5) | 327 (58.1) | 136 (33.5) | 48 (28.1) | 19 (18.1) | 55 (43.7) | 64 (42.1) | 910 (45.5) |
| Protestant | 193 (40.3) | 20 (3.6) | 200 (49.3) | 42 (24.6) | 26 (24.8) | 22 (17.5) | 49 (32.2) | 552 (27.5) |
| Other | 25 (5.2) | 216 (38.4) | 70 (17.2) | 81 (47.4) | 60 (57.1) | 49 (38.9) | 39 (25.7) | 540 (27.0) |
| Occupation | ||||||||
| Jobless/Student | 286 (59.7) | 362 (64.3) | 194 (47.8) | 51 (29.8) | 49 (46.7) | 68 (54.0) | 56 (36.8) | 1066 (53.3) |
| With Job | 193 (40.3) | 201 (35.7) | 212 (52.2) | 120 (70.2) | 56 (53.3) | 58 (46.0) | 96 (63.2) | 936 (46.7) |
| Healthcare work | ||||||||
| No | 455 (95.0) | 560 (99.5) | 384 (94.6) | 157 (91,8) | 72 (68.6) | 107 (84.9) | 145 (95.4) | 1880 (93.9) |
| Yes | 24 (5.0) | 3 (0.5) | 22 (5.4) | 14 (8.2) | 33 (31.4) | 19 (15.1) | 7 (4.6) | 122 (6.1) |
| Income category | ||||||||
| Low | 457 (95.4) | 490 (87.0) | 171 (42.1) | 74 (43.3) | 58 (55.2) | 108 (85.7) | 114 (75.0) | 1472 (73.5) |
| Lower & middle | 2 (0.4) | 61 (10.8) | 202 (49.8) | 69 (40.4) | 15 (14.3) | 11 (8.7) | 5 (3.3) | 365 (18.2) |
| High/Upper middle | 20 (4.2) | 12 (2.1) | 33 (8.1) | 28 (16.4) | 32 (30.5) | 7 (5.6) | 33 (21.7) | 165 (8.2) |
| Living area | ||||||||
| Urban/town | 213 (44.5) | 563 (100.0) | 387 (95.3) | 132 (77.2) | 87 (82.9) | 2 (1.6) | 142 (93.4) | 1526 (76.2) |
| Suburban/rural | 266 (55.5) | 0 (0.0) | 19 (4.7) | 39 (22.8) | 18 (17.1) | 124 (98.4) | 10 (6.6) | 476 (23.8) |
| Pregnant woman | ||||||||
| Yes | 355 (74.1) | 478 (84.9) | 296 (72.9) | 113 (66.1) | 77 (73.3) | 96 (76.2) | 102 (67.1) | 1517 (75.8) |
| Non | 98 (20.5) | 85 (15.1) | 97 (23.9) | 39 (22.8) | 21 (20.0) | 13 (10.3) | 37 (24.3) | 390 (19.5) |
| Not sure | 26 (5.4) | 0 (0.0) | 13 (3.2) | 19 (11.1) | 7 (6.7) | 17 (13.5) | 13 (8.6) | 95 (4.8) |
| Smokers | ||||||||
| No | 439 (91.6) | 560 (99.5) | 403 (99.3) | 161 (94.2) | 99 (94.3) | 116 (92.1) | 148 (97.4) | 1926 (96.2) |
| Yes | 40 (8.4) | 3 (0.5) | 3 (0.7) | 10 (5.8) | 6 (5.7) | 10 (7.9) | 4 (2.6) | 76 (3.8) |
| Characteristics | Province | ||||||
|---|---|---|---|---|---|---|---|
| Haut-Katanga n = 479 | Kasaï-Central n = 563 | Kasaï-Oriental n = 406 | Kinshasa n = 171 | Kongo-Central n = 105 | Kwilu n = 126 | Nord-Kivu n = 152 | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Total IPV | 41 (8.6) | 16 (2.8) | 70 (17.2) | 29 (17.0) | 32 (30.5) | 20 (15.9) | 27 (17.8) |
| Verbal IPV | 13 (31.7) | 12 (75.0) | 54(77.1) | 13 (44.8) | 16 (50.0) | 16 (80.0) | 19 (70.4) |
| Physical IPV | 23 (56.1) | 4 (25.0) | 16 (22.9) | 7 (24.2) | 8 (25.0) | 4 (20.0) | 5 (18.5) |
| Sexual IPV | 2 (4.9) | 0 (0.0) | 0 (0.0) | 4 (13.8) | 8 (25.0) | 0 (0.0) | 0 (0.0) |
| Other IPV | 3 (7.3) | 0 (0.0) | 0 (0.0) | 5 (17.2) | 0 (0.0) | 0 (0.0) | 3 (11.1) |
| Variables | Modalities | OR Crude | IC95% OR Crude | OR Adjusted | IC95% OR Adjusted | p-Value |
|---|---|---|---|---|---|---|
| Age | Less than 30 | 1 | 1 | |||
| 30–39 | 0.59 | 0.42–0.84 | 0.66 | 0.46–0.95 | 0.0261 | |
| 40–49 | 0.67 | 0.46–0.98 | 0.75 | 0.50–1.11 | 0.1479 | |
| 50 and more | 0.21 | 0.10–0.42 | 0.23 | 0.11–0.48 | 0.0001 | |
| Religion | Catholic | 1 | 1 | |||
| Protestant | 1.50 | 1.07–2.12 | 1.31 | 0.92–1.88 | 0.1371 | |
| Other | 1.40 | 0.96–2.04 | 1.20 | 0.81–1.79 | 0.3695 | |
| Education level | Primary | 1 | 1 | |||
| Secondary | 0.65 | 0.41–1.02 | 0.98 | 0.59–1.64 | 0.9496 | |
| University | 0.41 | 0.24–0.70 | 0.78 | 0.41–1.47 | 0.4402 | |
| Residential setting | Suburban/rural | 1 | 1 | |||
| Urban/Town | 0.47 | 0.31–0.72 | 0.63 | 0.41–0.99 | 0.0479 | |
| Income category | High/Upper | 1 | 1 | |||
| Middle income | 0.55 | 0.34–0.87 | 0.48 | 0.29–0.79 | 0.0038 | |
| Low income | 2.32 | 1.39–3.88 | 1.84 | 1.04–3.24 | 0.0357 | |
| Being pregnant | No | 1 | 1 | |||
| Yes | 1.81 | 1.31–2.51 | 1.63 | 1.16–2.29 | 0.0053 | |
| Do not know | 2.47 | 1.49–4.09 | 2.01 | 1.17–3.44 | 0.0112 | |
| Smoking | No | 1 | 1 | |||
| Yes | 2.52 | 1.43–4.45 | 1.75 | 0.94–3.29 | 0.0792 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ditekemena, J.D.; Luhata, C.; Mavoko, H.M.; Siewe Fodjo, J.N.; Nkamba, D.M.; Van Damme, W.; Ebrahim, S.H.; Noestlinger, C.; Colebunders, R. Intimate Partners Violence against Women during a COVID-19 Lockdown Period: Results of an Online Survey in 7 Provinces of the Democratic Republic of Congo. Int. J. Environ. Res. Public Health 2021, 18, 5108. https://doi.org/10.3390/ijerph18105108
Ditekemena JD, Luhata C, Mavoko HM, Siewe Fodjo JN, Nkamba DM, Van Damme W, Ebrahim SH, Noestlinger C, Colebunders R. Intimate Partners Violence against Women during a COVID-19 Lockdown Period: Results of an Online Survey in 7 Provinces of the Democratic Republic of Congo. International Journal of Environmental Research and Public Health. 2021; 18(10):5108. https://doi.org/10.3390/ijerph18105108
Chicago/Turabian StyleDitekemena, John D., Christophe Luhata, Hypolite M. Mavoko, Joseph Nelson Siewe Fodjo, Dalau M. Nkamba, Wim Van Damme, Shahul H. Ebrahim, Christiana Noestlinger, and Robert Colebunders. 2021. "Intimate Partners Violence against Women during a COVID-19 Lockdown Period: Results of an Online Survey in 7 Provinces of the Democratic Republic of Congo" International Journal of Environmental Research and Public Health 18, no. 10: 5108. https://doi.org/10.3390/ijerph18105108
APA StyleDitekemena, J. D., Luhata, C., Mavoko, H. M., Siewe Fodjo, J. N., Nkamba, D. M., Van Damme, W., Ebrahim, S. H., Noestlinger, C., & Colebunders, R. (2021). Intimate Partners Violence against Women during a COVID-19 Lockdown Period: Results of an Online Survey in 7 Provinces of the Democratic Republic of Congo. International Journal of Environmental Research and Public Health, 18(10), 5108. https://doi.org/10.3390/ijerph18105108