
Life Course Nature Exposure and Mental Health Outcomes: A Systematic Review and Future Directions


Abstract
:1. Introduction
- What types of mental health benefits are associated with early-life nature exposure?
- How strong and consistent is the evidence relating to associations between life course nature exposure and mental health?
- To what degree does the current evidence support a critical period or time-variant effect of nature on mental health?
- What theoretical and methodological challenges and unanswered questions remain for future studies?
2. Materials and Methods
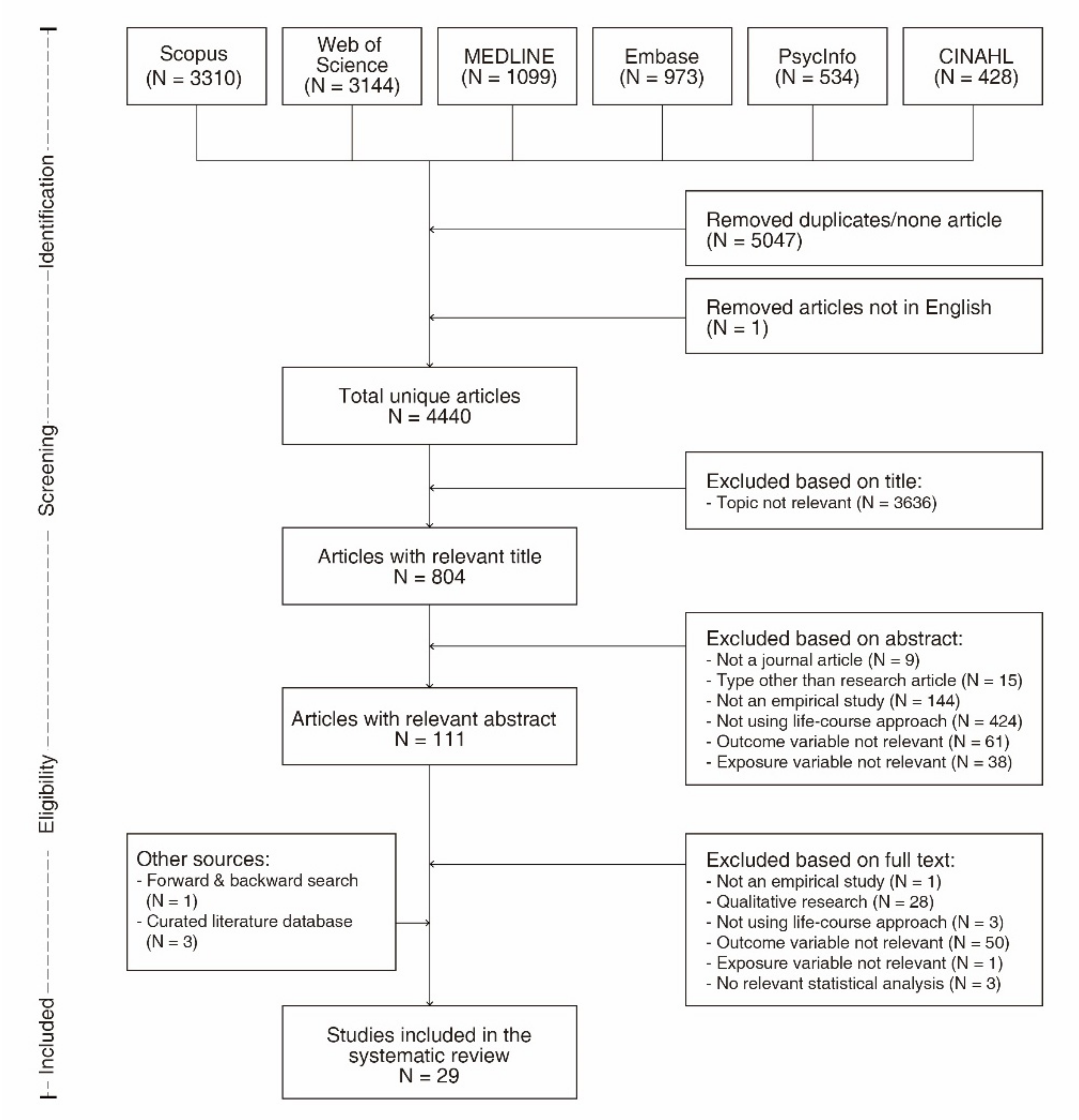
2.1. Search Strategy
2.2. Inclusion Criteria
- Reported original empirical research published in a peer-reviewed journal;
- Were written in English;
- Included a measure of nature or green space as exposure (or independent variable). We included both objectively-measured and self-reported green space, regardless of whether the measure was related to nearby nature close to home or other types of visits to or use of green space. Both quantity and quality measures were considered eligible;
- Reported at least one measure of mental health as the outcome, including psychological, affective, and cognitive measures;
- Performed an inferential statistical test to examine the relationship between nature exposure and mental health outcome.
2.3. Assessment of Study Bias
2.4. Data Extraction and Synthesis
2.5. Protocol Registration
3. Results
3.1. Study Characteristics
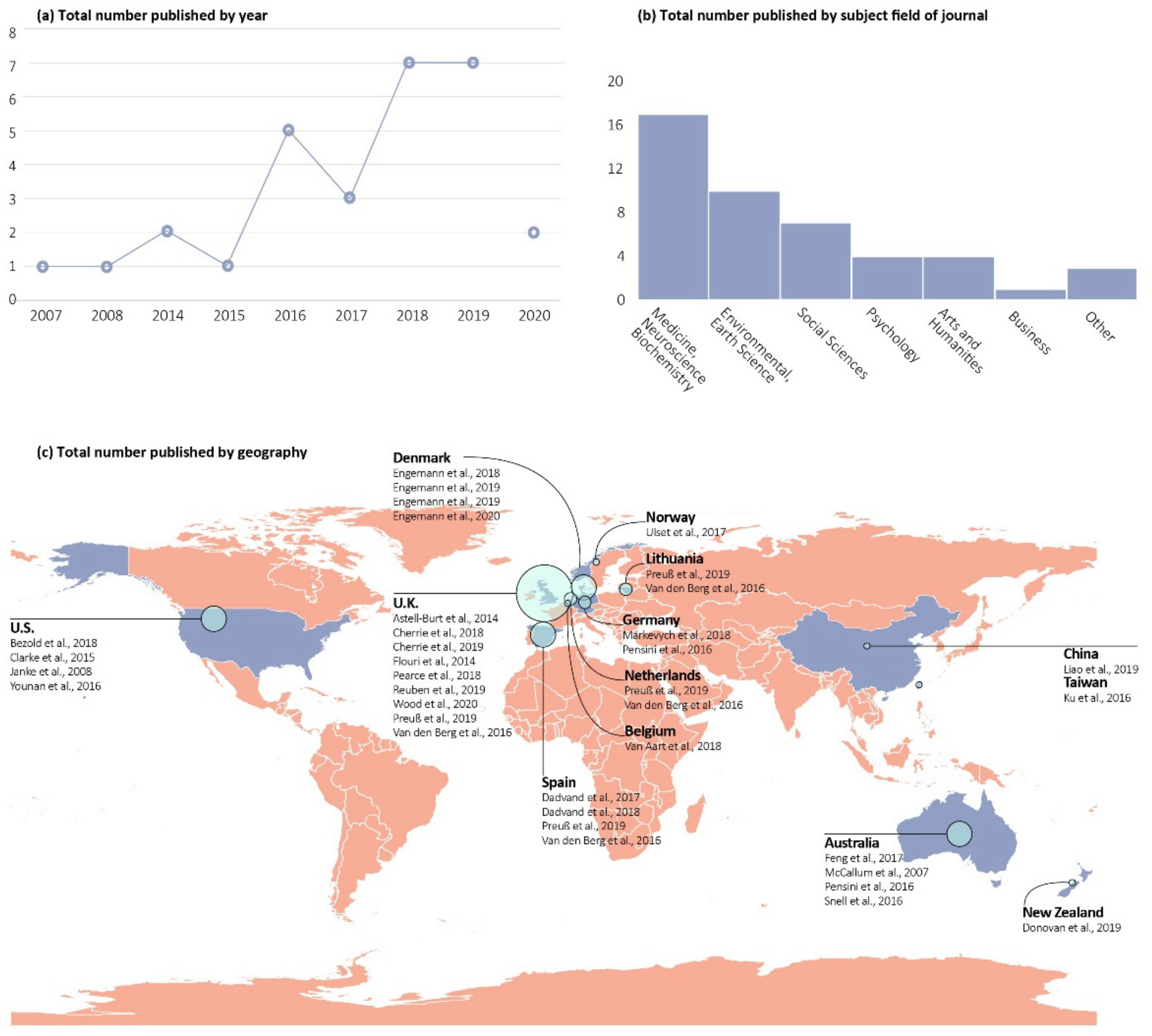
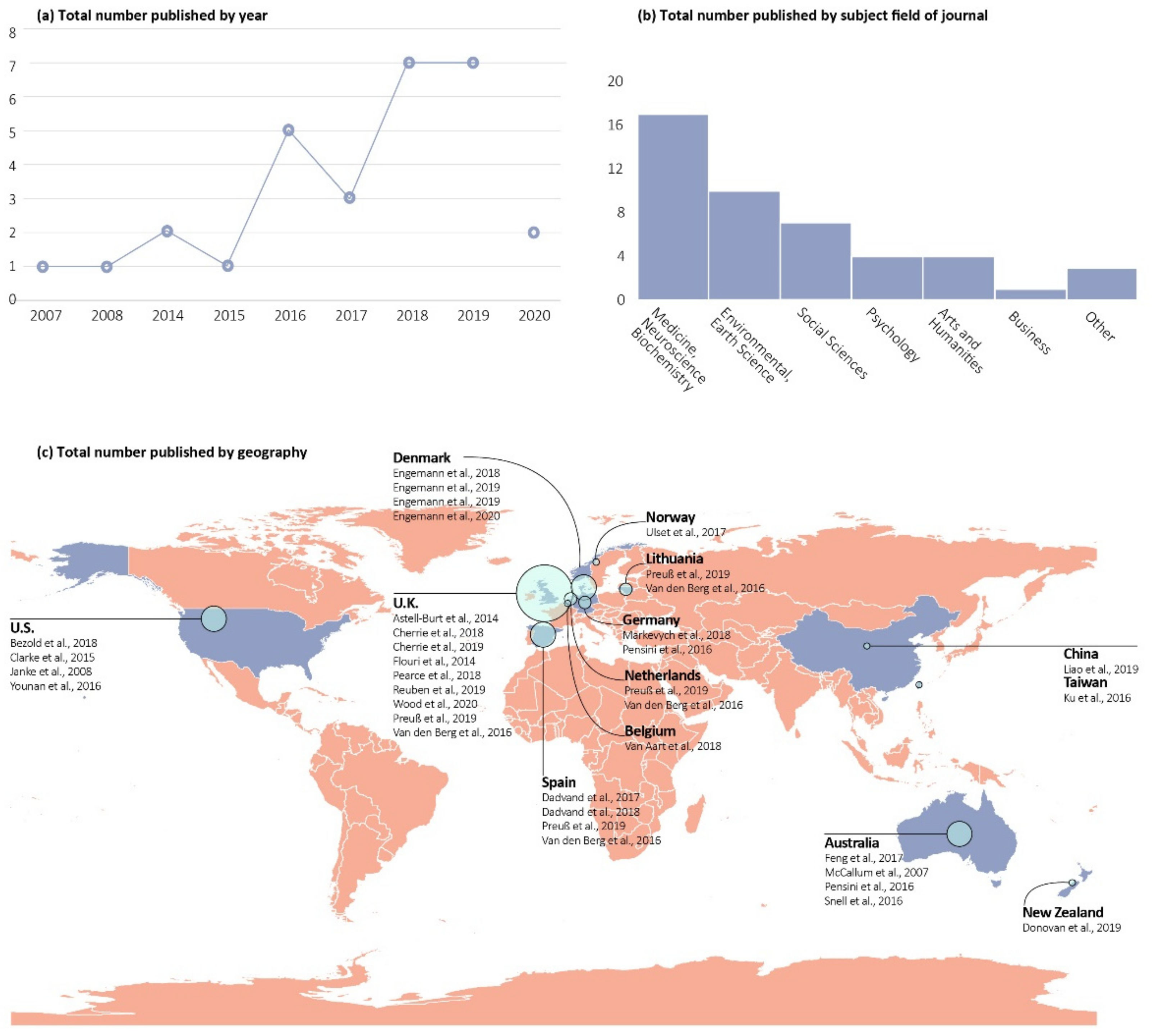
3.1.1. Temporal Trends, Discipline, and Geographical Distribution
3.1.2. Study Design
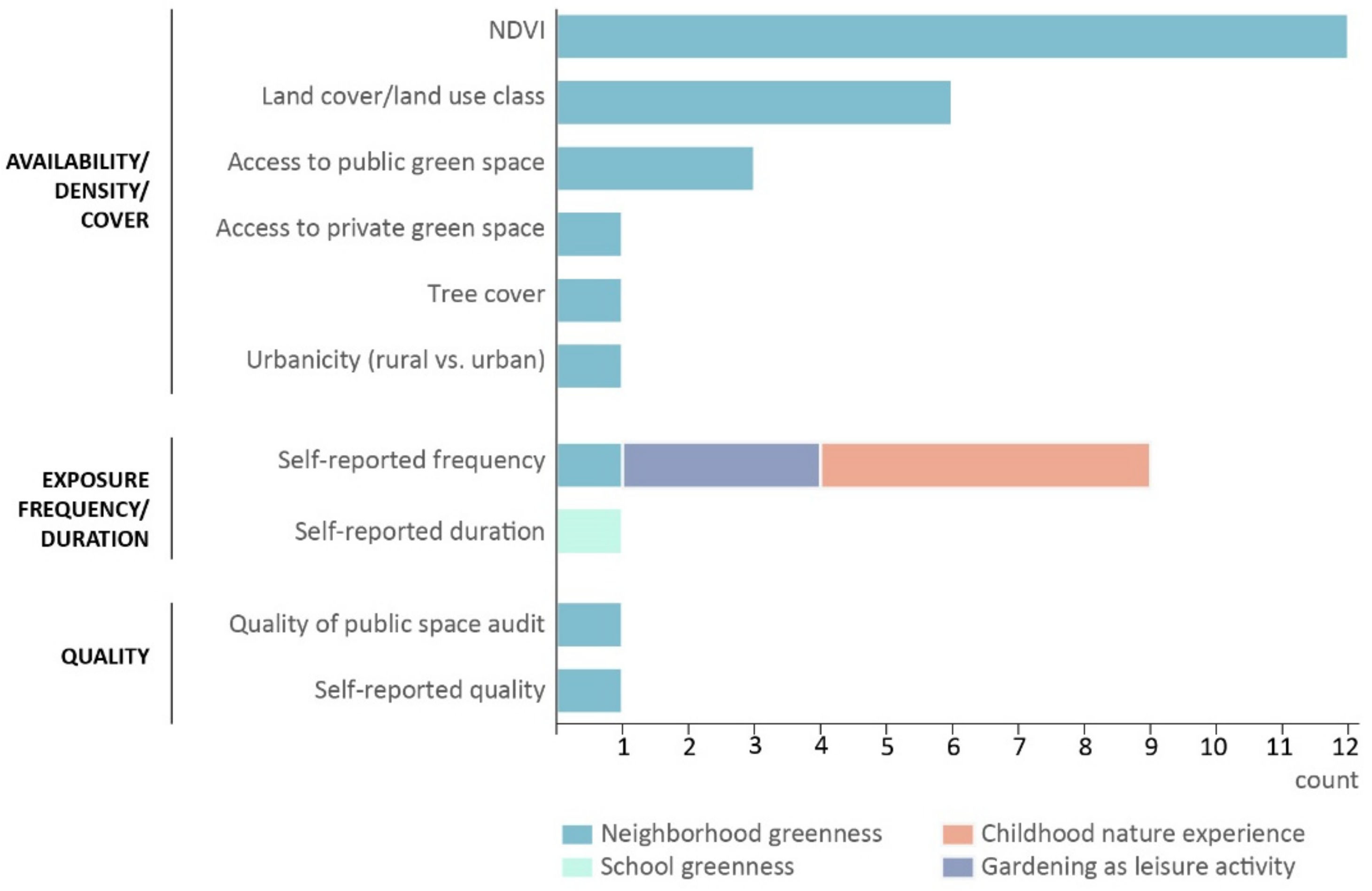
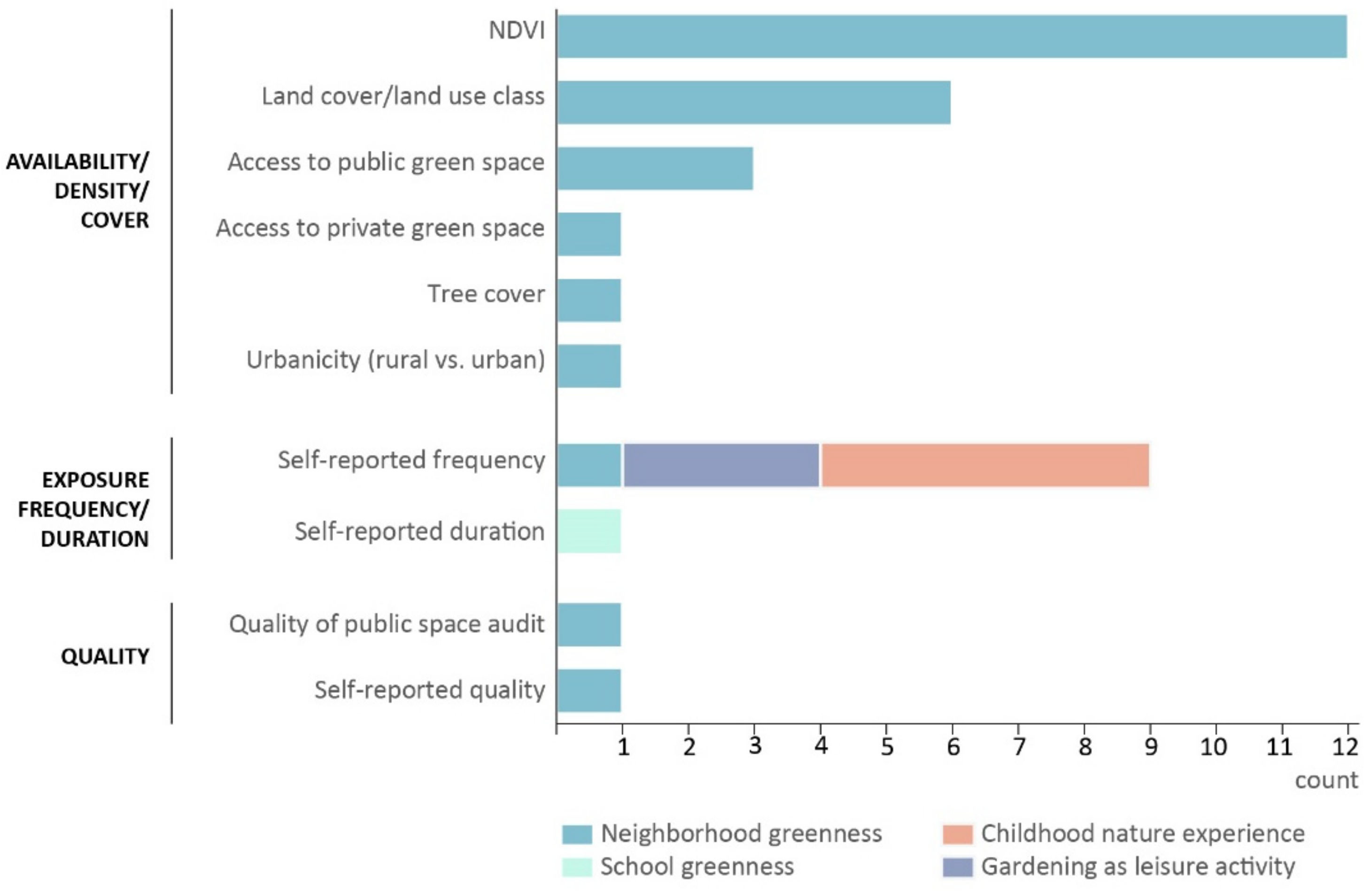
3.2. Measures of Lifelong Exposure to Nature
3.3. Mental Health Outcomes and the Directions and Strengths of Results
3.3.1. Reduced Incidence of Mental Disorders
3.3.2. Reduced Psychiatric Symptoms and Increased Positive Emotions
3.3.3. Reduced Behavioral Problems
3.3.4. Increased Cognitive Function
3.3.5. Increased Subjective Well-Being
3.4. Mediators and Moderators
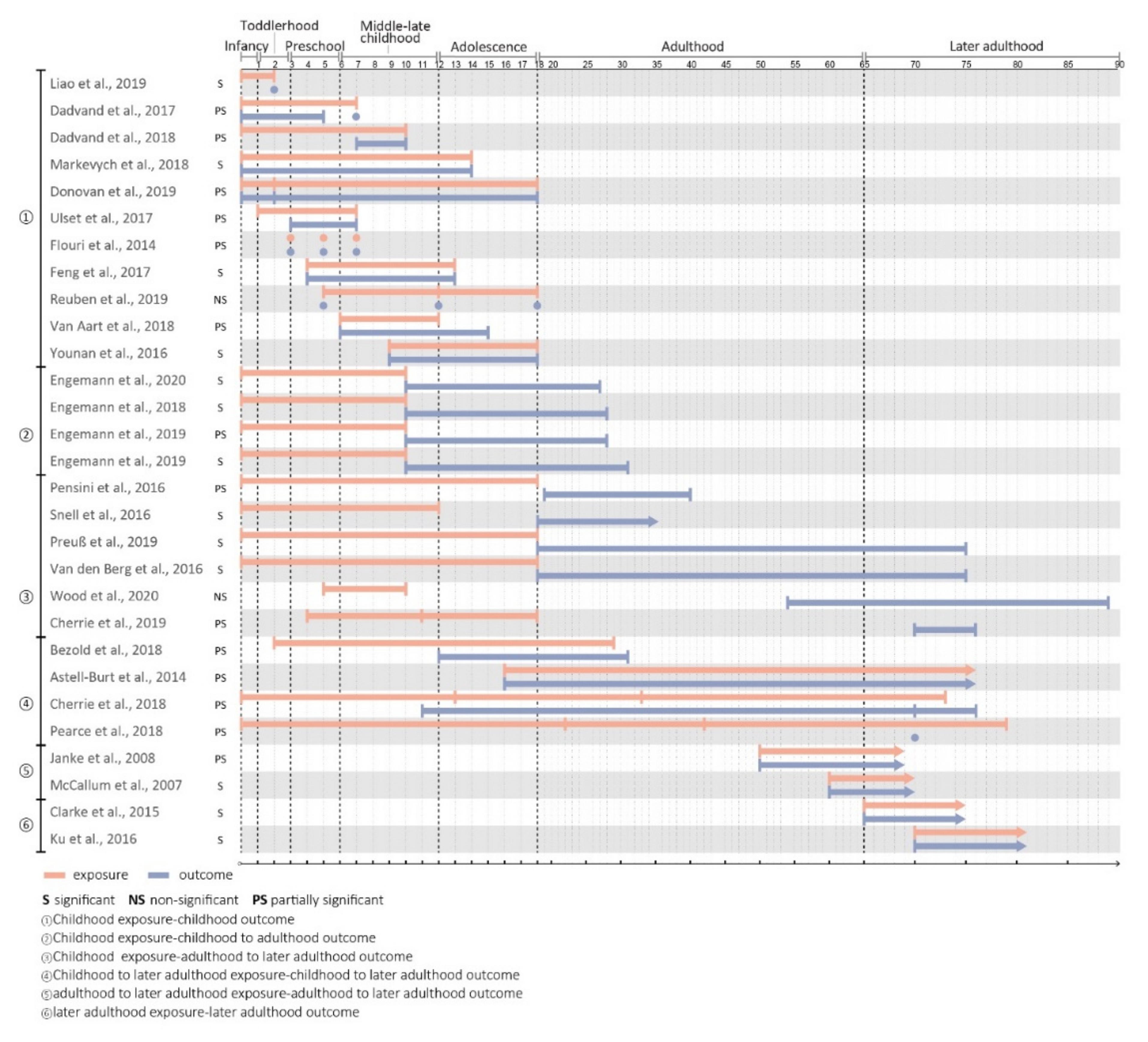
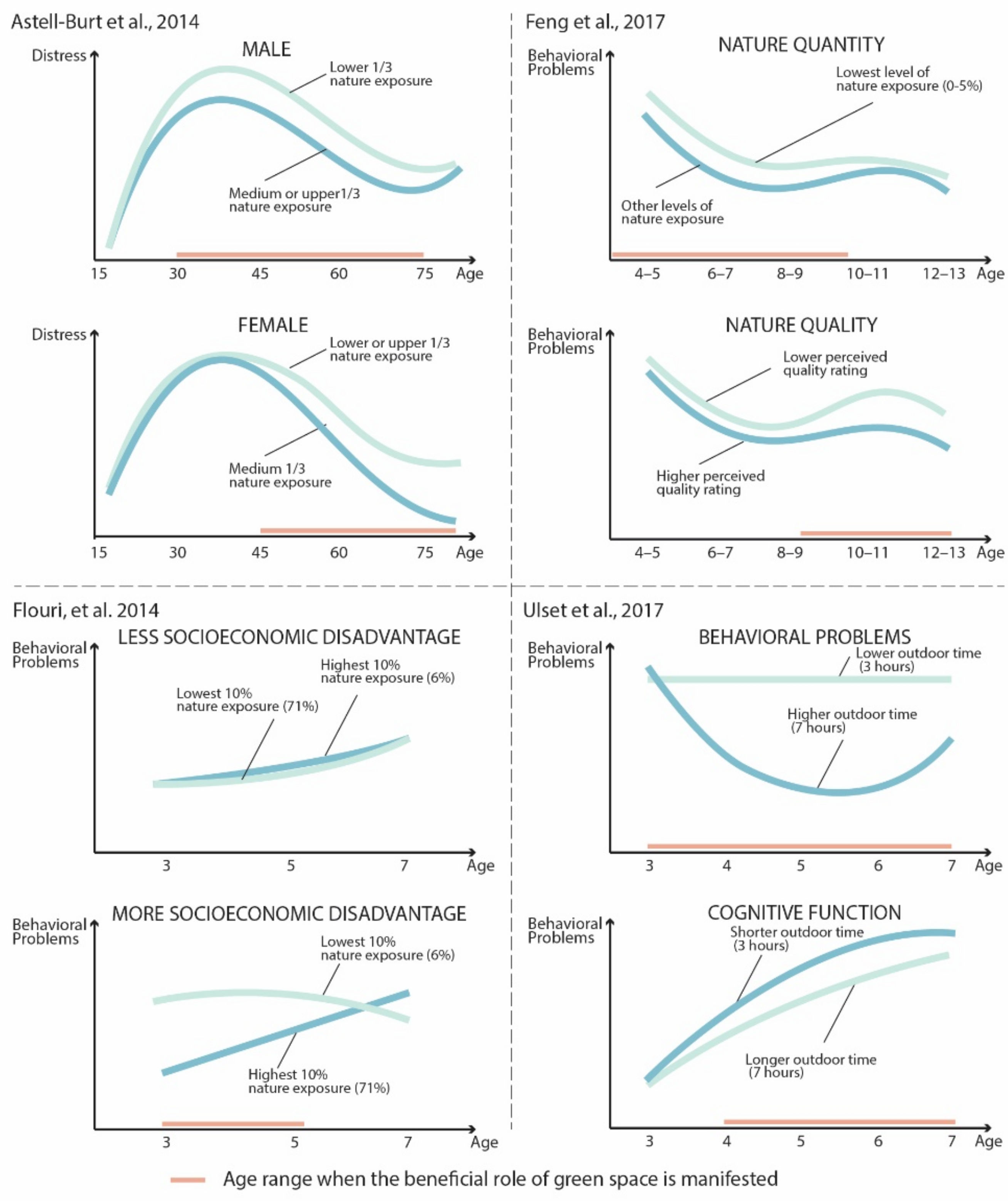
3.5. Life Stages and Time Span of Nature Exposure
4. Discussion
4.1. Summary of Findings and Implications for Practice
4.2. Insights from Qualitative Studies on Life Course Nature Exposure and Mental Health
4.3. Validity Concerns and Methodological Considerations
4.3.1. Internal Validity
4.3.2. External Validity
4.3.3. Construct Validity
4.3.4. Statistical Conclusion Validity
4.4. Unanswered Questions and Future Directions within the Life Course Perspective
4.4.1. Timing in Lives
- Are the mental health benefits of nature gained at all life stages or do they depend on stage?
- Is there a critical window when lack of nature exposure may cause irreversible results? Is exposure during childhood or later adulthood more important for lifelong mental health than at other stages?
- If there is a critical period for establishing behavioral or biological advantages from nature exposure, are the effects modifiable by exposure later in life?
4.4.2. Life Course Trajectories, Transitions, and Turning Points
- Are the protective benefits of nature cumulative?
- How do life course transitions such as becoming a parent, the death of a loved one, or retiring from one’s job relate to time spent in nature? How does this relate to subsequent mental health outcomes?
- Are some life course transitions more likely than others to become turning points, such that people shift toward greater engagement with nature and to a more positive mental health life course trajectory?
4.4.3. Cultural and Contextual Influences
- Does nearby nature, as a neighborhood contextual factor, moderate the stress–mental health relationship over time? How might this be relevant in the context of the global COVID-19 pandemic?
- Are there important pathways through which early contextual factors influence later outcomes?
4.4.4. Linked Lives
- What is the role of family members in connecting a child to nature and, ultimately mental health outcomes?
- How might an individual’s nature connection influence their spouse’s time in and connection to nature as well as their navigation of life course transitions and subsequent mental health outcomes?
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Faber Taylor, A.F.; Wiley, A.; Kuo, F.E.; Sullivan, W.C. Growing up in the inner city: Green spaces as places to grow. Environ. Behav. 1998, 30, 3–27. [Google Scholar] [CrossRef]
- Chawla, L.; Keena, K.; Pevec, I.; Stanley, E. Green schoolyards as havens from stress and resources for resilience in childhood and adolescence. Health Place 2014, 28, 1–13. [Google Scholar] [CrossRef]
- Wells, N.M.; Evans, G.W. Nearby nature: A buffer of life stress among rural children. Environ. Behav. 2003, 35, 311–330. [Google Scholar] [CrossRef]
- Feda, D.; Seelbinder, A.; Baek, S.; Raja, S.; Yin, L.; Roemmich, J. Neighbourhood parks and reduction in stress among adolescents: Results from Buffalo, New York. Indoor Built Environ. 2015, 24, 631–639. [Google Scholar] [CrossRef]
- Li, D.; Deal, B.; Zhou, X.; Slavenas, M.; Sullivan, W.C. Moving beyond the neighborhood: Daily exposure to nature and adolescents’ mood. Landsc. Urban Plan. 2018, 173, 33–43. [Google Scholar] [CrossRef]
- Cox, D.T.; Shanahan, D.F.; Hudson, H.L.; Fuller, R.A.; Anderson, K.; Hancock, S.; Gaston, K.J. Doses of nearby nature simultaneously associated with multiple health benefits. Int. J. Environ. Res. Public Health 2017, 14, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roe, J.J.; Thompson, C.W.; Aspinall, P.A.; Brewer, M.J.; Duff, E.I.; Miller, D.; Mitchell, R.; Clow, A. Green space and stress: Evidence from cortisol measures in deprived urban communities. Int. J. Environ. Res. Public Health 2013, 10, 4086–4103. [Google Scholar] [CrossRef] [Green Version]
- Browning, M.H.; Lee, K.; Wolf, K.L. Tree cover shows an inverse relationship with depressive symptoms in elderly residents living in US nursing homes. Urban For. Urban Green. 2019, 41, 23–32. [Google Scholar] [CrossRef]
- Finlay, J.; Franke, T.; McKay, H.; Sims-Gould, J. Therapeutic landscapes and wellbeing in later life: Impacts of blue and green spaces for older adults. Health Place 2015, 34, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Douglas, O.; Lennon, M.; Scott, M. Green space benefits for health and well-being: A life-course approach for urban planning, design and management. Cities 2017, 66, 53–62. [Google Scholar] [CrossRef] [Green Version]
- Houlden, V.; Weich, S.; de Albuquerque, J.; Jarvis, S.; Rees, K. The relationship between greenspace and the mental wellbeing of adults: A systematic review. PLoS ONE 2018, 13, 667. [Google Scholar]
- Collins, R.M.; Spake, R.; Brown, K.A.; Ogutu, B.O.; Smith, D.; Eigenbrod, F. A systematic map of research exploring the effect of greenspace on mental health. Landsc. Urban Plan. 2020, 201, 89–91. [Google Scholar] [CrossRef]
- Marshall, V.W.; Mueller, M.M. Theoretical roots of the life-course perspective. Soc. Dyn. Life Course 2003, 3, 3–32. [Google Scholar]
- Bronfenbrenner, U.; Morris, P.A. The ecology of developmental processes. Handb. Child Psychol. 1998, 1, 993–1028. [Google Scholar]
- Elder, G.H. The Life Course Paradigm: Social Change and Individual Development. In Examining Lives in Context: Perspectives on the Ecology of Human Development; Moen, P., Elder, G.H., Jr., Lüscher, K., Eds.; American Psychological Association: Washington, DC, USA, 1995. [Google Scholar]
- Wells, N.M.; Lekies, K.S. Nature and the life course: Pathways from childhood nature experiences to adult environmentalism. Child. Youth Environ. 2006, 16, 1–24. [Google Scholar]
- Kuh, D.; Ben-Shlomo, Y.; Lynch, J.; Hallqvist, J.; Power, C. Life course epidemiology. J. Epidemiol. Community Health 2003, 57, 778. [Google Scholar] [CrossRef]
- Thompson, C.W.; Aspinall, P.; Montarzino, A. The childhood factor: Adult visits to green places and the significance of childhood experience. Environ. Behav. 2008, 40, 111–143. [Google Scholar] [CrossRef]
- World Health Organization. Preamble to the Constitution of the World Health Organization as Adopted by the International Health Conference, New York, NY, USA, 19–22 June 1946; Signed on 22 July 1946 by the Representatives of 61 States (Official Records of the World Health Organization, no. 2, p 100) and Entered into Force on 7 April 1948. 1948. Available online: http://www.who.int/governance/eb/who_constitution_en.pdf (accessed on 4 May 2021).
- Hartig, T.; Mitchell, R.; De Vries, S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [Green Version]
- Jacob, C.M.; Baird, J.; Barker, M.; Cooper, C.; Hanson, M. The Importance of a Life Course Approach to Health: Chronic Disease Risk from Preconception through Adolescence and Adulthood. World Health Organization, 2017; pp. 1–41. Available online: https://www.who.int/life-course/publications/importance-of-life-course-approach-to-health/en/ (accessed on 1 June 2020).
- Astell-Burt, T.; Mitchell, R.; Hartig, T. The association between green space and mental health varies across the lifecourse. A longitudinal study. J. Epidemiol. Community Health 2014, 68, 578–583. [Google Scholar] [CrossRef]
- Van den Berg, M.; Van Poppel, M.; Van Kamp, I.; Andrusaityte, S.; Balseviciene, B.; Cirach, M.; Danileviciute, A.; Ellis, N.; Hurst, G.; Masterson, D.; et al. Visiting green space is associated with mental health and vitality: A cross-sectional study in four European cities. Health Place 2016, 38, 8–15. [Google Scholar] [CrossRef]
- Markevych, I.; Tesch, F.; Datzmann, T.; Romanos, M.; Schmitt, J.; Heinrich, J. Outdoor air pollution, greenspace, and incidence of ADHD: A semi-individual study. Sci. Total Environ. 2018, 642, 1362–1368. [Google Scholar] [CrossRef] [PubMed]
- Cherrie, M.P.C.; Shortt, N.K.; Mitchell, R.J.; Taylor, A.M.; Redmond, P.; Thompson, C.W.; Starr, J.M.; Deary, I.J.; Pearce, J.R. Green space and cognitive ageing: A retrospective life course analysis in the Lothian Birth Cohort 1936. Soc. Sci. Med. 2018, 196, 56–65. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Reprint—Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Phys. Ther. 2009, 89, 873–880. [Google Scholar] [CrossRef]
- Atkinson, K.M.; Koenka, A.C.; Sanchez, C.E.; Moshontz, H.; Cooper, H. Reporting standards for literature searches and report inclusion criteria: Making research syntheses more transparent and easy to replicate. Res. Synth. Methods 2015, 6, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Nature and Children Network. Making the Case for Children and Nature; Research Library. Available online: https://www.childrenandnature.org/resources/category/greening-schoolyards/get-started/make-the-case/ (accessed on 1 June 2020).
- Blane, D.B.; Netuveli, G.; Stone, J. The development of life course epidemiology. Rev. Épidémiologie Santé Publique 2007, 55, 31–38. [Google Scholar] [CrossRef]
- National Heart and Lung Institute. Quality Assessment Tool for Case Series Studies. National Institutes of Health, 2014. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 1 June 2020).
- Taylor, M.F.; Brice, J.; Buck, N.; Prentice-Lane, E. British Household Panel Survey User Manual: Volume A: Introduction, Technical Report and Appendices; University of Essex Colchester: Colchester, UK, 1993. [Google Scholar]
- Deary, I.J.; Gow, A.J.; Taylor, M.D.; Corley, J.; Brett, C.; Wilson, V.; Campbell, H.; Whalley, L.J.; Visscher, P.M.; Porteous, D.J. The Lothian Birth Cohort 1936: A study to examine influences on cognitive ageing from age 11 to age 70 and beyond. BMC Geriatr. 2007, 7, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plewis, I.; Calderwood, L.; Hawkes, D.; Hughes, G.; Joshi, H. Millennium Cohort Study: Technical Report on Sampling; Centre for Longitudinal Study, Institute of Education: London, UK, 2007. [Google Scholar]
- Clarke, P.J.; Weuve, J.; Barnes, L.; Evans, D.A.; de Leon, C.F.M. Cognitive decline and the neighborhood environment. Ann. Epidemiol. 2015, 25, 849–854. [Google Scholar] [CrossRef] [Green Version]
- Feng, X.Q.; Astell-Burt, T. Residential Green Space Quantity and Quality and Child Well-being: A Longitudinal Study. Am. J. Prev. Med. 2017, 53, 616–624. [Google Scholar] [CrossRef]
- Preuß, M.; Nieuwenhuijsen, M.; Marquez, S.; Cirach, M.; Dadvand, P.; Triguero-Mas, M.; Gidlow, C.; Grazuleviciene, R.; Kruize, H.; Zijlema, W. Low childhood nature exposure is associated with worse mental health in adulthood. Int. J. Environ. Res. Public Health 2019, 16, 467. [Google Scholar] [CrossRef] [Green Version]
- Pensini, P.; Horn, E.; Caltabiano, N.J. An exploration of the relationships between adults’ childhood and current nature exposure and their mental well-being. Child. Youth Environ. 2016, 26, 125–147. [Google Scholar] [CrossRef]
- Engemann, K.; Jens-Christian, S.; Lars, A.; Jørgen, B.; Camilla, G.; Bo, M.P.; Oleguer, P.-R.; Constantinos, T.; Bøcker, P.C. Natural surroundings in childhood are associated with lower schizophrenia rates. Schizophr. Res. 2019, 8, 89. [Google Scholar] [CrossRef] [PubMed]
- Reuben, A.; Arseneault, L.; Belsky, D.W.; Caspi, A.; Fisher, H.L.; Houts, R.M.; Moffitt, T.E.; Odgers, C. Residential neighborhood greenery and children’s cognitive development. Soc. Sci. Med. 2019, 230, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Younan, D.; Tuvblad, C.; Li, L.; Wu, J.; Lurmann, F.; Franklin, M.; Berhane, K.; McConnell, R.; Wu, A.H.; Baker, L.A. Environmental determinants of aggression in adolescents: Role of urban neighborhood greenspace. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 591–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donovan, G.H.; Michael, Y.L.; Gatziolis, D.; Mannetje, A.; Douwes, J. Association between exposure to the natural environment, rurality, and attention-deficit hyperactivity disorder in children in New Zealand: A linkage study. Lancet Planet. Health 2019, 3, E226–E234. [Google Scholar] [CrossRef] [Green Version]
- Dadvand, P.; Tischer, C.; Estarlich, M.; Llop, S.; Dalmau-Bueno, A.; Lopez-Vicente, M.; Valentin, A.; de Keijzer, C.; Fernandez-Somoano, A.; Lertxundi, N.; et al. Lifelong residential exposure to green space and attention: A population-based prospective study. Environ. Health Perspect. 2017, 125, 97016. [Google Scholar] [CrossRef] [Green Version]
- Engemann, K.; Pedersen, C.B.; Arge, L.; Tsirogiannis, C.; Mortensen, P.B.; Svenning, J.-C. Childhood exposure to green space—A novel risk-decreasing mechanism for schizophrenia? Schizophr. Res. 2018, 199, 142–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engemann, K.; Pedersen, C.B.; Arge, L.; Tsirogiannis, C.; Mortensen, P.B.; Svenning, J.-C. Residential green space in childhood is associated with lower risk of psychiatric disorders from adolescence into adulthood. Proc. Natl. Acad. Sci. USA 2019, 116, 5188–5193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engemann, K.; Pedersen, C.B.; Agerbo, E.; Arge, L.; Borglum, A.D.; Erikstrup, C.; Hertel, O.; Hougaard, D.M.; McGrath, J.J.; Mors, O.; et al. Association Between Childhood Green Space, Genetic Liability, and the Incidence of Schizophrenia. Schizophr. Bull. 2020, 16, 908. [Google Scholar]
- McCallum, J.; Simons, L.A.; Simons, J.; Friedlander, Y. Delaying dementia and nursing home placement—The Dubbo study of elderly Australians over a 14-year follow-up. Ann. N. Y. Acad. Sci. 2007, 1114, 121–129. [Google Scholar] [CrossRef]
- Bezold, C.P.; Banay, R.F.; Coull, B.A.; Hart, J.E.; James, P.; Kubzansky, L.D.; Missmer, S.A.; Laden, F. The relationship between surrounding greenness in childhood and adolescence and depressive symptoms in adolescence and early adulthood. Ann. Epidemiol. 2018, 28, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Pearce, J.; Cherrie, M.; Shortt, N.; Deary, I.; Thompson, C.W. Life course of place: A longitudinal study of mental Health Place. Trans. Inst. Br. Geogr. 2018, 43, 555–572. [Google Scholar] [CrossRef]
- Janke, M.C.; Nimrod, G.; Kleiber, D.A. Leisure activity and depressive symptoms of widowed and married women in later life. J. Leis. Res. 2008, 40, 250–266. [Google Scholar] [CrossRef]
- Van Aart, C.J.C.; Michels, N.; Sioen, I.; De Decker, A.; Bijnens, E.M.; Janssen, B.G.; De Henauw, S.; Nawrot, T.S. Residential landscape as a predictor of psychosocial stress in the life course from childhood to adolescence. Environ. Int. 2018, 120, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Wood, C.J.; Smyth, N. The health impact of nature exposure and green exercise across the life course: A pilot study. Int. J. Environ. Health Res. 2020, 30, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Flouri, E.; Midouhas, E.; Joshi, H. The role of urban neighbourhood green space in children’s emotional and behavioural resilience. J. Environ. Psychol. 2014, 40, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Ulset, V.; Vitaro, F.; Brendgen, M.; Bekkhus, M.; Borge, A.I.H. Time spent outdoors during preschool: Links with children’s cognitive and behavioral development. J. Environ. Psychol. 2017, 52, 69–80. [Google Scholar] [CrossRef]
- Rueda, M.R.; Fan, J.; McCandliss, B.D.; Halparin, J.D.; Gruber, D.B.; Lercari, L.P.; Posner, M.I. Development of attentional networks in childhood. Neuropsychologia 2004, 42, 1029–1040. [Google Scholar] [CrossRef]
- Grizzle, R. Wechsler Intelligence Scale for Children, Fourth Edition. In Encyclopedia of Child Behavior and Development; Goldstein, S., Naglieri, J.A., Eds.; Springer: Boston, MA, USA, 2011. [Google Scholar] [CrossRef]
- Liao, J.Q.; Zhang, B.; Xia, W.; Cao, Z.Q.; Zhang, Y.M.; Liang, S.W.; Hu, K.; Xu, S.Q.; Li, Y.Y. Residential exposure to green space and early childhood neurodevelopment. Environ. Int. 2019, 128, 70–76. [Google Scholar] [CrossRef]
- Dadvand, P.; Pujol, J.; Macia, D.; Martinez-Vilavella, G.; Blanco-Hinojo, L.; Mortamais, M.; Alvarez-Pedrerol, M.; Fenoll, R.; Esnaola, M.; Dalmau-Bueno, A.; et al. The association between lifelong greenspace exposure and 3-dimensional brain magnetic resonance imaging in Barcelona schoolchildren. Environ. Health Perspect. 2018, 126, 27012. [Google Scholar] [CrossRef] [Green Version]
- Cherrie, M.P.C.; Shortt, N.K.; Thompson, C.W.; Deary, I.J.; Pearce, J.R. Association between the activity space exposure to parks in childhood and adolescence and cognitive aging in later life. Int. J. Environ. Res. Public Health 2019, 16, 632. [Google Scholar] [CrossRef] [Green Version]
- Ku, P.W.; Fox, K.R.; Chen, L.J. Leisure-Time Physical Activity, Sedentary Behaviors and Subjective Well-Being in Older Adults: An Eight-Year Longitudinal Research. Soc. Indic. Res. 2016, 127, 1349–1361. [Google Scholar] [CrossRef]
- Snell, T.L.; Lam, J.C.S.; Lau, W.W.-Y.; Lee, I.; Maloney, E.M.; Mulholland, N.; Wilson, L.; Wynne, L.J. Contact with nature in childhood and adult depression. Child. Youth Environ. 2016, 26, 111–124. [Google Scholar] [CrossRef]
- Kahneman, D.; Diener, E.; Schwarz, N. Well-Being: Foundations of Hedonic Psychology; Russell Sage Foundation: New York, NY, USA, 1999. [Google Scholar]
- Dwan, K.; Altman, D.G.; Arnaiz, J.A.; Bloom, J.; Chan, A.-W.; Cronin, E.; Decullier, E.; Easterbrook, P.J.; Von Elm, E.; Gamble, C. Systematic review of the empirical evidence of study publication bias and outcome reporting bias. PLoS ONE 2008, 3, e3081. [Google Scholar] [CrossRef] [Green Version]
- Engemann, K.; Svenning, J.-C.; Arge, L.; Brandt, J.; Erikstrup, C.; Geels, C.; Hertel, O.; Mortensen, P.B.; Plana-Ripoll, O.; Tsirogiannis, C. Associations between growing up in natural environments and subsequent psychiatric disorders in Denmark. Environ. Res. 2020, 188, 109788. [Google Scholar] [CrossRef]
- Hartley, K.; Perazzo, J.; Brokamp, C.; Gillespie, G.L.; Cecil, K.M.; LeMasters, G.; Yolton, K.; Ryan, P. Residential surrounding greenness and self-reported symptoms of anxiety and depression in adolescents. Environ. Res. 2021, 17, 194. [Google Scholar]
- Torres Toda, M.; Riol, A.A.; Cirach, M.; Estarlich, M.; Fernández-Somoano, A.; González-Safont, L.; Guxens, M.; Julvez, J.; Riaño-Galán, I.; Sunyer, J. Residential Surrounding Greenspaceand Mental Health in Three Spanish Areas. Int. J. Environ. Res. Public Health 2020, 17, 5670. [Google Scholar] [CrossRef] [PubMed]
- Blane, D.B. Collecting retrospective data: Development of a reliable method and a pilot study of its use. Soc. Sci. Med. 1996, 42, 751–757. [Google Scholar] [CrossRef]
- Bell, S.L.; Phoenix, C.; Lovell, R.; Wheeler, B.W. Seeking everyday wellbeing: The coast as a therapeutic landscape. Soc. Sci. Med. 2015, 142, 56–67. [Google Scholar] [CrossRef]
- Bell, S.L.; Wheeler, B.W.; Phoenix, C. Using Geonarratives to Explore the Diverse Temporalities of Therapeutic Landscapes: Perspectives from “Green” and “Blue” Settings. Ann. Am. Assoc. Geogr. 2017, 107, 93–108. [Google Scholar] [CrossRef] [Green Version]
- MacIntyre, T.E.; Walkin, A.M.; Beckmann, J.; Calogiuri, G.; Gritzka, S.; Oliver, G.; Donnelly, A.A.; Warrington, G. An Exploratory Study of Extreme Sport Athletes’ Nature Interactions: From Well-Being to Pro-environmental Behavior. Front. Psychol. 2019, 10, 96–99. [Google Scholar] [CrossRef] [Green Version]
- Milligan, C.; Bingley, A. Restorative places or scary spaces? The impact of woodland on the mental well-being of young adults. Health Place 2007, 13, 799–811. [Google Scholar] [CrossRef] [PubMed]
- Diduck, A.P.; Raymond, C.M.; Rodela, R.; Moquin, R.; Boerchers, M. Pathways of learning about biodiversity and sustainability in private urban gardens. J. Environ. Plan. Manag. 2020, 63, 1056–1076. [Google Scholar] [CrossRef]
- Lloyd, K.; Burden, J.; Kiewa, J. Young Girls and Urban Parks: Planning for Transition through Adolescence. J. Park Recreat. Adm. 2008, 26, 21–38. [Google Scholar]
- Weimann, H.; Björk, J.; Håkansson, C. Experiences of the urban green local environment as a factor for well-being among adults: An exploratory qualitative study in southern Sweden. Int. J. Environ. Res. Public Health 2019, 16, 904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pace, J.; Walker, J. “Place-ing” Dementia Prevention and Care in Nunatu Kavut, Labrador. Can. J. Aging 2020, 39, 247–262. [Google Scholar] [CrossRef] [PubMed]
- Husser, E.K.; Roberto, K.A.; Allen, K.R. Nature as nurture: Rural older women’s perspectives on the natural environment. J. Women Aging 2020, 32, 44–67. [Google Scholar] [CrossRef] [Green Version]
- Tillmann, S.; Tobin, D.; Avison, W.; Gilliland, J. Mental health benefits of interactions with nature in children and teenagers: A systematic review. J. Epidemiol. Commun. Health 2018, 72, 958–966. [Google Scholar] [CrossRef]
- Wells, N.M.; Lekies, K.S. Children and nature: Following the trail to environmental attitudes and behavior. In Citizen Science Public Participation in Environmental Research; Dickinson, J., Bonney, R., Eds.; Cornell University Press: Ithaca, NY, USA, 2012; pp. 201–213. [Google Scholar]
- Scopelliti, M.; Giuliani, M.V. Choosing restorative environments across the lifespan: A matter of place experience. J. Environ. Psychol. 2004, 24, 423–437. [Google Scholar] [CrossRef]
- Holt, E.W.; Lombard, Q.K.; Best, N.; Smiley-Smith, S.; Quinn, J.E. Active and passive use of green space, health, and well-being amongst university students. Int. J. Environ. Res. Public Health 2019, 16, 424. [Google Scholar] [CrossRef] [Green Version]
- Chiang, Y.-C.; Li, D.; Jane, H.-A. Wild or tended nature? The effects of landscape location and vegetation density on physiological and psychological responses. Landsc. Urban Plan. 2017, 167, 72–83. [Google Scholar] [CrossRef]
- De Vries, S.; Snep, R. Biodiversity in the context of ‘biodiversity–mental health’ research. In Biodiversity and Health in the Face of Climate Change; Springer: Cham, Switzerland, 2019; pp. 159–173. [Google Scholar]
- Dahly, D.L. Growth mixture modelling for life course epidemiology. In Modern Methods for Epidemiology; Springer: Berlin/Heidelberg, Germany, 2012; pp. 223–241. [Google Scholar]
- Curran, P.J.; Obeidat, K.; Losardo, D. Twelve frequently asked questions about growth curve modeling. J. Cogn. Dev. 2010, 11, 121–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, J.; Rogerson, M.; Barton, J.; Bragg, R. Age and connection to nature: When is engagement critical? Front. Ecol. Environ. 2019, 17, 265–269. [Google Scholar] [CrossRef]
- Wethington, E. An overview of the life course perspective: Implications for health and nutrition. J. Nutr. Educ. Behav. 2005, 37, 115–120. [Google Scholar] [CrossRef]
- Ben-Shlomo, Y.; Kuh, D. A Life Course Approach to Chronic Disease Epidemiology: Conceptual Models, Empirical Challenges and Interdisciplinary Perspectives; Oxford University Press: Oxford, UK, 2002. [Google Scholar]
- Chawla, L. Childhood experiences associated with care for the natural world: A theoretical framework for empirical results. Child. Youth Environ. 2007, 17, 144–170. [Google Scholar]
- Elder, G.H.; Johnson, M.K.; Crosnoe, R. The emergence and development of life course theory. In Handbook of the Life Course; Springer: Berlin/Heidelberg, Germany, 2003; pp. 3–19. [Google Scholar]
- Escobar, D.F.S.S.; Jesus, T.F.D.; Noll, M. Assessing the Mental Health of Brazilian Students Involved in Risky Behaviors. Int. J. Environ. Res. Public Health 2020, 17, 3647. [Google Scholar] [CrossRef]
- Seven, Ü.S.; Stoll, M.; Dubbert, D.; Kohls, C.; Werner, P.; Kalbe, E. Perception, attitudes, and experiences regarding mental health problems and web based mental health information amongst young people with and without migration background in Germany. A qualitative study. Int. J. Environ. Res. Public Health 2021, 18, 81. [Google Scholar] [CrossRef]
- Wheaton, B.; Clarke, P. Space meets time: Integrating temporal and contextual influences on mental health in early adulthood. Am. Sociol. Rev. 2003, 5, 680–706. [Google Scholar] [CrossRef]
- Mitchell, R.J.; Richardson, E.A.; Shortt, N.K.; Pearce, J.R. Neighborhood environments and socioeconomic inequalities in mental well-being. Am. J. Prev. Med. 2015, 49, 80–84. [Google Scholar] [CrossRef]
- Wells, N.M. The natural environment as a resilience factor: Nature’s role as a buffer of the effects of risk and adversity. In Nature and Psychology: Biology, Cognitive, Developmental, and Social Pathways to Well-Being, Proceedings of the Nebraska Symposium on Motivation, The University of Nebraska, Lincoln, NE, USA, 11–12 April 2019; Schutte, A.R., Torquate, J., Stevens, J.R., Eds.; Springer Nature: Basel, Switzerland, In press.
- Wells, N.M. The role of nature in children’s resilience: Cognitive and social processes. In Greening in the Red Zone; Tidball, K., Krasny, M., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; pp. 95–109. [Google Scholar]
- Kuo, F.E. Coping with poverty: Impacts of environment and attention in the inner city. Environ. Behav. 2001, 33, 5–34. [Google Scholar] [CrossRef]
- Tahara, M.; Mashizume, Y.; Takahashi, K. Coping Mechanisms: Exploring Strategies Utilized by Japanese Healthcare Workers to Reduce Stress and Improve Mental Health during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 131. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; North, C.S. Mental health and the Covid-19 pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Escobar, D.F.S.S.; Jesus, T.F.D.; Noll, M. Family and School Context: Effects on the Mental Health of Brazilian Students. Int. J. Environ. Res. Public Health 2020, 17, 6042. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Article | Geography | Population | Study Design | Nature Exposure | Mental Health Outcome | Confounders | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Country | Urbanicity | Population 1 | Sample Size 2 | Type of Study | Dataset | Setting | Type | Measurement | Domain | Measurement | |||
| 1 | Astell-Burt et al., 2014 | UK | Urban | Adults (16+ year) | 2681 wards; 65,407 person-years | Longitudinal | British Household Panel Survey (BHPS) | Neighborhood greenness | Availability/density/cover | Land cover class (%; green and natural environment) | Psychiatric symptoms/psychological conditions | General Health Questionnaire (GHQ) | Demographics (e.g., age) SES (e.g., household income) Health behavior self/family (e.g., smoking status) |
| 2 | Bezold et al., 2018 | US | NR | Children and early adolescents (9–14 year) | 8374 persons | Longitudinal | Growing Up Today Study (GUTS) | Neighborhood greenness | Availability/density/cover | NDVI | Psychiatric symptoms/psychological conditions | McKnight Risk Factor Survey (MRFS) The Center for Epidemiologic Studies ten-item depression scale (CES-D 10) | Demographics (e.g., age) SES (e.g., household income) Health record self/family (e.g., maternal history of depression) |
| 3 | Cherrie et al., 2018 | UK | Mixed | Adults born in 1936 | 281 persons | Longitudinal | Lothian Birth Cohort 1936 | Neighborhood greenness | Availability/density/cover | Public park availability (%) | Cognitive function | Moray House Test No.12 (MHT) | Demographics (e.g., sex) SES (e.g., occupation) Health behavior self/family (e.g., childhood/adulthood smoking) |
| 4 | Cherrie et al., 2019 | UK | NR | Adults born in 1936 | 281 persons | Longitudinal | Lothian Birth Cohort 1936 | Neighborhood greenness | Availability/density/cover | Public park availability (%) | Cognitive function | Moray House Test No.12 (MHT) | Demographics (e.g., sex) SES (e.g., occupation) Health behavior self/family (e.g., childhood/adulthood smoking) |
| 5 | Clarke et al., 2015 | US | Urban | Older adults (65+ year) | 82 block groups; 6158 persons | Longitudinal | Chicago Health and Aging Project (1993–2011) | Neighborhood greenness | Quality | Quality of public space audit | Cognitive function | East Boston Memory Test (EBMT) Symbol digit modalities test (SDMT) Mini Mental State Examination (MMSE) | Demographics SES Health record self/family (e.g., chronic conditions) Social network (e.g., size) Environment (e.g., sidewalk) |
| 6 | Dadvand et al., 2017 | Spain | Urban | Pregnant women (16+ year) | 888/987 persons | longitudinal | INfancia y Medio Ambiente (INMA) | Neighborhood greenness | Availability/density/cover | NDVI Residential surrounding tree cover (VCF) | Cognitive function | Conners’ Kiddie Continuous Performance Test (K-CPT) Attentional Network Task (ANT) | Demographics SES (e.g., maternal education) Health record self/family (e.g., maternal smoking) Environment (e.g., neighborhood SES) |
| 7 | Dadvand et al., 2018 | Spain | Urban | Children (7–10 year) | 39 schools; 253/2897 persons | Longitudinal | Brain Development and Air Pollution Ultrafine Particles in School Children (BREATHE) | Neighborhood greenness | Availability/density/cover | NDVI | Cognitive function Brain development | N-back Working Memory Test (WT) Attentional Network Task (ANT) Brain region peak voxel gray/white matter | Demographics (e.g., sex) SES (e.g., maternal education) |
| 8 | Donovan et al., 2019 | New Zealand | Mixed | Children born in 1998 | 49,923 persons; | Longitudinal | New Zealand’s Integrated Data Infrastructure (IDI) | Neighborhood greenness | Availability/density/cover | NDVI Land cover class (%) Urbanicity (urban vs. rural) | Incidence of mental disorders | Reported incidence | Demographics (e.g., sex) SES (e.g., parental education) Health record self/family (e.g., infections) Environment (e.g., traffic-related air pollution) |
| 9 | Engemann et al., 2018 | Denmark | Mixed | Adults born 1985–2003 | 943,027 persons | Longitudinal | Danish Civil Registration System, Danish Psychiatric Central Research Register | Neighborhood greenness | Availability/density/cover | NDVI | Incidence of mental disorders | Reported incidence | Demographics (e.g., sex) SES (e.g., parental education) |
| 10 | Engemann et al., 2019 a | Denmark | Mixed | Adults born 1985–2003 | 943,027 persons | Longitudinal | Danish Civil Registration System, Danish Psychiatric Central Research Register | Neighborhood greenness | Availability/density/cover | NDVI | Incidence of mental disorders | Reported incidence | Demographics (e.g., sex) SES (e.g., parental education) Health record self/family (e.g., parents’ records of psychiatric disorder) Environment (e.g., neighborhood SES) |
| 11 | Engemann et al., 2019 b | Denmark-Europe | Mixed | Adults born 1985–2003 | 943,027 persons | Longitudinal | Danish Civil Registration System, Danish Psychiatric Central Research Register | Neighborhood greenness | Availability/density/cover | Land cover class (%; urban, agriculture, near-natural green space, and blue space) NDVI | Incidence of mental disorders | Reported incidence | Demographics (e.g., sex) SES (e.g., parental education) Health record self/family (e.g., parents’ records of mental illness) Environment (e.g., neighborhood SES) |
| 12 | Engemann et al., 2020 | Denmark-Europe | Mixed | Adults born 1981–2005 | 19,746 persons | Longitudinal | iPSYCH2012 case-cohort sample | Neighborhood greenness | Availability/density/cover | NDVI | Incidence of mental disorders | Reported incidence | Demographics (e.g., sex) SES (e.g., parental education) |
| 13 | Feng et al., 2017 | Australia | Mixed | Children (4–5 year) | 4968 persons | Longitudinal | Longitudinal Study of Australian Children (LSAC) | Neighborhood greenness | Mixed (Availability/density/cover, Quality) | Land use class (%; parkland) Self-reported quality | Emotional/conduct problems | Strengths and Difficulties Questionnaire (SDQ) | Demographics (e.g., sex) Environment (e.g., neighborhood SES) |
| 14 | Flouri et al., 2014 | UK | Urban | Children born 2000–2001 | 6384 persons | Longitudinal | Millennium Cohort Study | Neighborhood greenness | Mixed (Availability/density/cover, Frequency/duration) | Land use class (%; green space domestic gardens, fresh water) Sole access to a garden Frequency of park visit | Emotional/conduct problems | Strengths and Difficulties Questionnaire (SDQ) | Demographics (e.g., sex) SES Health record self/family (e.g., maternal psychological distress) Health behavior self/family (e.g., physical activity) Environment (e.g., neighborhood deprivation) Adverse life events |
| 15 | Janke et al., 2008 | US | NR | Women who became widowed 1986–1989 or 1989–1994 | 296 persons | Longitudinal | Americans Changing Lives (ACL) | Gardening as leisure activity | Frequency/duration | Frequency of informal, formal, and physical leisure activities, including gardening | Psychiatric symptoms/psychological conditions | The Center for Epidemiologic Studies ten-item depression scale (CES-D 10) | Demographics SES |
| 16 | Ku et al., 2016 | Taiwan | NR | Older adults (70+ year) | 1268 | Longitudinal | Survey of Health and Living Status of the Elderly | Gardening as leisure activity | Frequency/duration | Frequency of engagement in leisure activity, including gardening | Mental well-being | Life Satisfaction Index A (LSIA) | Demographics (e.g., sex) SES (e.g., educational level) Health record self/family (e.g., depressive symptoms) Health behavior self/family (e.g., physical activity) |
| 17 | Liao et al., 2019 | China | Mixed | Women who became pregnant 2012–2015 | 1312 mother–child pairs | Longitudinal | NA | Neighborhood greenness | Availability/density/cover | NDVI | Cognitive function | Bayley Scales of Infant Development (BSID) | Health behavior self/family (e.g., physical activity) Environment (e.g., PM2.5) |
| 18 | Markevych et al., 2018 | Germany | Mixed | Children born 2000–2004 | 186 postal code areas; 66,823 persons | Longitudinal | AOK PLUS statutory health insurance company dataset | Neighborhood greenness | Availability/density/cover | NDVI | Incidence of mental disorders | Reported incidence | Demographics (e.g., sex) SES (e.g., unemployment) Environment (e.g., air pollution) |
| 19 | McCallum et al., 2007 | Australia | Semi-urban | Older Adults (60+ year) | 2805 persons | Longitudinal | Dubbo Study of the Elderly | gardening as leisure activity | Frequency/duration | Frequency of gardening | Incidence of mental disorders | Reported incidence | Demographics (e.g., age) SES (e.g., education) Health record self/family (e.g., stroke) Health behavior self/family (e.g., walking) Environment (e.g., neighborhood SES) |
| 20 | Pearce et al., 2018 | UK | NR | Adults born in 1936 | 23 wards; 328/531/1091 persons | Longitudinal | Lothian Birth Cohort 1936 | Neighborhood greenness | Availability/density/cover | Public park availability (%) | Psychiatric symptoms/psychological conditions | Hospital Anxiety and Depression Scale (HADS) | Demographics (e.g., age) SES (e.g., education) Health behavior self/family (e.g., smoking) |
| 21 | Pensini et al., 2016 3 | Australia | NR | Adults (19–40 year) | 646 persons | Cross-sectional | NA | Childhood nature experience | Frequency/duration | Frequency of time spent in 13 types of natural environments (Natural Environment Exposure Scales [NEES]) | Mental well-being | Warwick-Edinburgh Mental Well-Being Scale (WEMBS) Ryff Scales of Psychological Well-Being (PWB) Meaning in Life Questionnaire (MLQ) | Current nature exposure |
| Germany | 141 persons | ||||||||||||
| 22 | Preuß et al., 2019 | Spain, the Netherlands, Lithuania, and UK | Urban | Adults (18–75) | 30 neighborhoods; 3585 persons | Cross-sectional | Positive Health Effects of the Natural Outdoor Environment in Typical Populations in Different Regions in Europe (PHENOTYPE) | Childhood nature experience | Frequency/duration | Frequency of visits to natural outdoor environment (NOE) during childhood | Mental well-being | Short-Form Health Survey (SF-36) | Demographics (e.g., age) SES (e.g., education) Health behavior self/family (e.g., smoking) Environment (e.g., neighborhood SES) |
| 23 | Reuben et al., 2019 | UK | Urban and suburban | Twins born 1994–1995 | 1658 persons | Longitudinal | Environmental Risk (E-Risk) Longitudinal Twin Study | Neighborhood greenness | Availability/density/cover | NDVI | Cognitive function | Weschler Intelligence Scale (WISC) Cambridge Neuropsychological Test Automated Battery (CANTAB) | Demographics (e.g., age) SES (e.g., education) Environment (e.g., neighborhood SES) |
| 24 | Snell et al., 2016 | Australia | NR | Adults (18+ year) | 300 persons | Cross-sectional | NA | Childhood nature experience | Frequency/duration | Frequency of visits to four different natural environments during childhood | Psychiatric symptoms/psychological conditions | Depression Anxiety and Stress Scales (DASS) | Current nature exposure |
| 25 | Ulset et al., 2017 | Norway | Suburban | Children (1–6 year) | 28 daycare centers; 562 individuals; 2136 person-years | Longitudinal | NA | School greenness | Frequency/duration | Duration of time outside at daycare centers of two different types (nature-based vs. conventional) | Emotional/conduct problems Cognitive function | Strengths and Difficulties Questionnaire (SDQ) Weschler Intelligence Scale (WISC) | Demographics (e.g., age) SES (e.g., education) Health record self/family (e.g., parental inattention-hyperactivity) Environment (e.g., daycare center quality) |
| 26 | van Aart et al., 2018 | Belgium | Semi-urban | Children (around 7–12 year) | 172/224 persons | Longitudinal | Identification and prevention of dietary- and lifestyle-induced health effects in children and infants project (IDEFICS) | Neighborhood greenness | Availability/density/cover | Land cover class (%; semi-natural, forested, agriculture, industrial, residential) | Emotional/conduct problems Psychiatric symptoms/psychological conditions | Recent feelings of happiness, sadness, anger, and anxiousness Strengths and Difficulties Questionnaire (SDQ) Hair cortisol | Demographics (e.g., age) SES (e.g., parental education) Environment (e.g., air pollution) |
| 27 | van den Berg et al., 2016 | Spain, the Netherlands, Lithuania, and UK | Urban | Adults (18–75 year) | 30 neighborhoods; 3748 persons | Cross-sectional | PHENOTYPE | Childhood nature experience | Frequency/duration | Frequency of time spent in natural environments during childhood | Mental well-being | Short-Form Health Survey (SF-36) | Demographics (e.g., age) SES (e.g., education) |
| 28 | Wood et al., 2020 | UK–Europe | NR | Adults (54–89) | 45 persons | Cross-sectional | NA | Childhood nature experience | Frequency/duration | Frequency of childhood nature exposure | Mental well-being Psychiatric symptoms/psychological conditions | Warwick-Edinburgh Mental Well-Being Scale (WEMBS) Perceived Stress Scale (PSS) Heart Rate Variability (HRV) | |
| 29 | Younan et al., 2016 | US | Urban | Twins and triplets born 1990–1995 | 640 families; 1287 persons | Longitudinal | Risk Factors for Antisocial Behavior (RFAB) twin study | Neighborhood greenness | Availability/density/cover | NDVI | Emotional/conduct problems | Child Behavior Checklist (CBCL) | SES Environment (e.g., neighborhood quality) |
| Domain | Mediators/Pathways | Moderators/Effect Modifiers | ||||
|---|---|---|---|---|---|---|
| Variables | No. of Studies Testing the Mediator | No. of Studies Finding Significant Mediation | Variables | No. of Studies Testing the Moderator | No. of Studies Finding Significant Moderation | |
| Sociodemographic | Age/Age2/Age3 | 5 | 5/5 | |||
| Gender | 2 | 2/2 | ||||
| Marital status | 1 | 1/1 | ||||
| Socioeconomic status | 2 | 2/2 | ||||
| Personal/parental health and physical activity | Parents’ mental and physical health | 2 | 0/2 | Parents’ mental and physical health (BMI) | 1 | 1/1 |
| Parents’ physical activity | 1 | 0/1 | ||||
| Physical health | 1 | 0/1 | ||||
| Physical activity | 1 | 0/1 | ||||
| Experience with nature | Current/adulthood nature exposure | 3 | 2/3 | Current/adulthood nature exposure | 3 | 3/3 |
| Perceived amount of nature available | 1 | 0/1 | ||||
| Connectedness with nature | 1 | 0/1 | ||||
| Environmental and contextual | PM2.5 | 2 | 0/2 | |||
| Noise | 1 | 1/1 | ||||
| Density | 1 | 1/1 | ||||
| Land use | 1 | 1/1 | ||||
| Urbanicity/urbanization | 2 | 0/2 | ||||
| Perceived safety (traffic accidents) | 1 | 1/1 | ||||
| Neighborhood deprivation | 1 | 1/1 | ||||
| Others | Genetics | 2 | 0/2 | |||
| Adverse life events | 1 | 0/1 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, D.; Menotti, T.; Ding, Y.; Wells, N.M. Life Course Nature Exposure and Mental Health Outcomes: A Systematic Review and Future Directions. Int. J. Environ. Res. Public Health 2021, 18, 5146. https://doi.org/10.3390/ijerph18105146
Li D, Menotti T, Ding Y, Wells NM. Life Course Nature Exposure and Mental Health Outcomes: A Systematic Review and Future Directions. International Journal of Environmental Research and Public Health. 2021; 18(10):5146. https://doi.org/10.3390/ijerph18105146
Chicago/Turabian StyleLi, Dongying, Tess Menotti, Yizhen Ding, and Nancy M. Wells. 2021. "Life Course Nature Exposure and Mental Health Outcomes: A Systematic Review and Future Directions" International Journal of Environmental Research and Public Health 18, no. 10: 5146. https://doi.org/10.3390/ijerph18105146
APA StyleLi, D., Menotti, T., Ding, Y., & Wells, N. M. (2021). Life Course Nature Exposure and Mental Health Outcomes: A Systematic Review and Future Directions. International Journal of Environmental Research and Public Health, 18(10), 5146. https://doi.org/10.3390/ijerph18105146