
Validation of the Italian Version of the Behavioral Inhibition Questionnaire (BIQ) for Preschool Children


 ,
,  and
and 
Abstract
1. Introduction
1.1. The Assessment of Behavioral Inhibition
1.2. The Behavioral Inhibition Questionnaire (BIQ)
2. Materials and Methods
2.1. Participants
2.2. Procedure and Measures
2.3. Statistical Analyses
3. Results
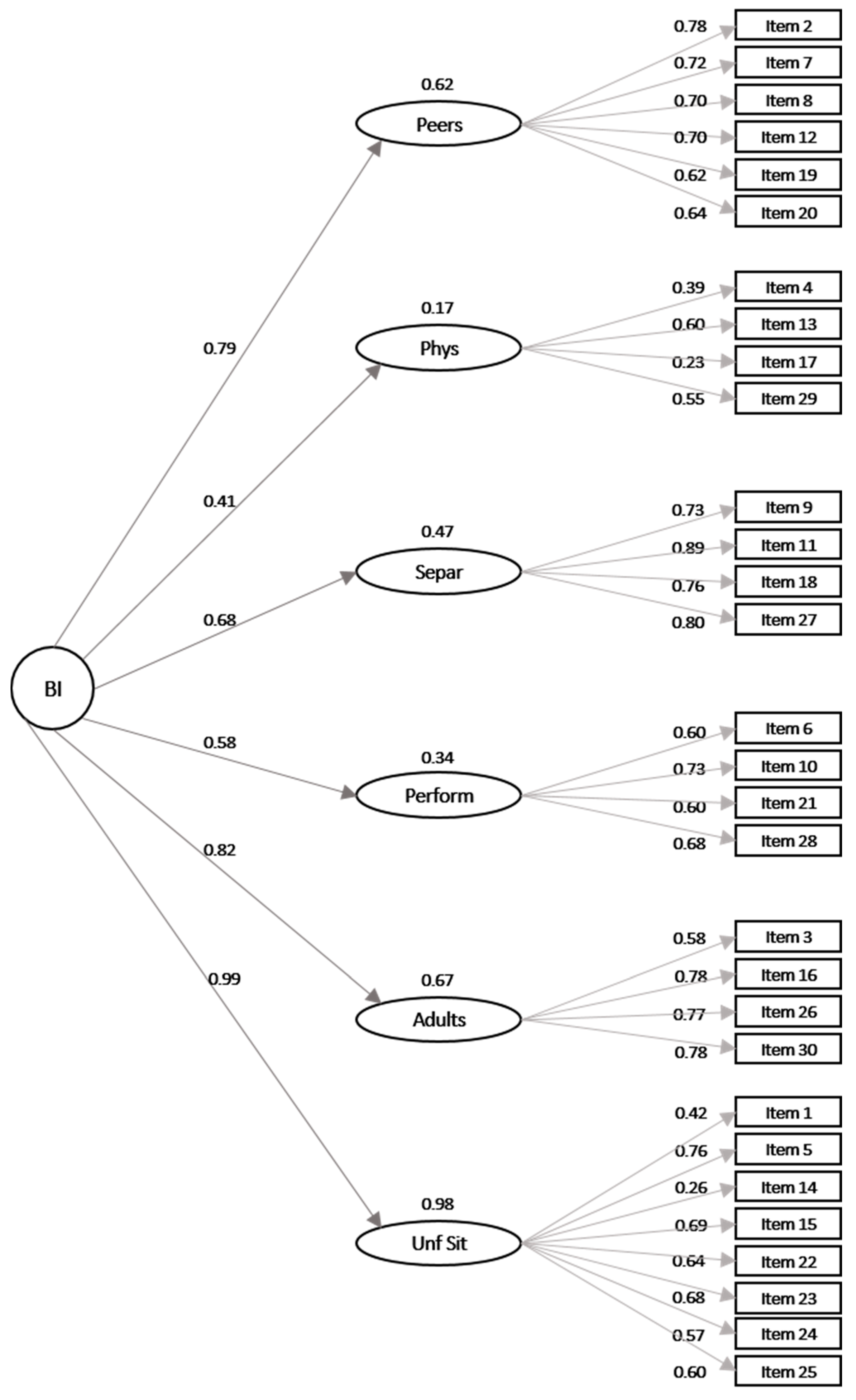
3.1. Confirmatory Factor Analysis
3.2. Measurement Invariance
3.3. Internal Consistency
3.4. Inter-Rater Reliability
3.5. Convergent, Divergent and Discriminant Validity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kagan, J. Heart rate and heart rate variability as signs of a temperamental dimension in infants. In Measuring Emotions in Infants and Children; Izard, C.E., Ed.; Cambridge University Press: Cambridge, UK, 1982; pp. 3–20. [Google Scholar]
- Kagan, J.; Reznick, J.S.; Snidman, N. Biological bases of childhood shyness. Science 1988, 240, 167–171. [Google Scholar] [CrossRef]
- Kagan, J.; Reznick, J.S.; Snidman, N. Temperamental inhibition in early childhood. In The Study of Temperament: Changes, Continuities, and Challenges; Plomin, R., Dunn, J., Eds.; Erlbaum: Hillsdale, NJ, USA, 1985; pp. 53–66. [Google Scholar]
- Broeren, S.; Muris, P. A psychometric evaluation of the behavioral inhibition questionnaire in a non-clinical sample of Dutch children and adolescents. Child Psychiatry Hum. Dev. 2010, 41, 214–229. [Google Scholar] [CrossRef] [PubMed]
- Fox, N.A.; Henderson, H.A.; Marshall, P.J.; Nichols, K.E.; Ghera, M.M. Behavioral inhibition: Linking biology and behavior within a developmental framework. Annu. Rev. Psychol. 2005, 56, 235–262. [Google Scholar] [CrossRef] [PubMed]
- Hirshfeld-Becker, D.R.; Micco, J.; Henin, A.; Bloomfield, A.; Biederman, J.; Rosenbaum, J. Behavioral inhibition. Depress. Anxiety 2008, 25, 357–367. [Google Scholar] [CrossRef]
- Kagan, J.; Snidman, N. The Long Shadow of Temperament; Harvard University Press: Cambridge, MA, USA, 2004. [Google Scholar]
- Henderson, H.A.; Pine, D.S.; Fox, N.A. Behavioral inhibition and developmental risk: A dual-processing perspective. Neuropsychopharmacology 2015, 40, 207–224. [Google Scholar] [CrossRef]
- Rothbart, M.K.; Ellis, L.K.; Rueda, M.R.; Posner, M.I. Developing mechanisms of temperamental effortful control. J. Pers. 2003, 71, 1113–1143. [Google Scholar] [CrossRef] [PubMed]
- White, L.K.; McDermott, J.M.; Degnan, K.A.; Henderson, H.A.; Fox, N.A. Behavioral inhibition and anxiety: The moderating roles of inhibitory control and attention shifting. J. Abnorm. Child Psychol. 2011, 39, 735–747. [Google Scholar] [CrossRef]
- Eisenberg, N.; Smith, C.; Spinrad, T.L. Effortful control: Relations with emotion regulation, adjustment, and socialization in childhood. In Handbook of Self-Regulation: Research, Theory, and Applications; Baumeister, R.F., Vohs, K.D., Eds.; Guilford: New York, NY, USA, 2011; pp. 263–283. [Google Scholar]
- Biederman, J.; Rosenbaum, J.F.; Bolduc-Murphy, E.A.; Faraone, S.V.; Chaloff, J.; Hirshfeld, D.R.; Kagan, J. A 3-Year Follow-up of Children with and without Behavioral Inhibition. J. Am. Acad. Child Adolesc. Psychiatry 1993, 32, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Kagan, J.; Snidman, N.; Arcus, D. Childhood derivatives of high and low reactivity in infancy. Child Dev. 1998, 69, 1483–1493. [Google Scholar] [CrossRef]
- Van Brakel, A.M.L. Behavioural Inhibition as a Risk Factor for the Development of Childhood Anxiety Disorders. Ph.D. Thesis, Maastricht University, Maastricht, The Netherlands, 2007. [Google Scholar]
- Moehler, E.; Kagan, J.; Parzer, P.; Wiebel, A.; Brunner, R.; Resch, F. Relation of behavioral inhibition to neonatal and infant cardiac activity, reactivity and habituation. J. Individ. Differ. 2006, 41, 1349–1358. [Google Scholar] [CrossRef]
- Fox, N.A.; Rubin, K.H.; Calkins, S.D.; Marshall, T.R.; Coplan, R.J.; Porges, S.W.; Long, J.M.; Stewart, S. Frontal activation asymmetry and social competence at four years of age. Child Dev. 1995, 66, 1770–1784. [Google Scholar] [CrossRef]
- Else-Quest, N.M.; Hyde, J.S.; Goldsmith, H.H.; Van Hulle, C.A. Gender differences in temperament: A meta-analysis. Psychol. Bull. 2006, 132, 33–72. [Google Scholar] [CrossRef] [PubMed]
- Dyson, M.W.; Klein, D.N.; Olino, T.M.; Dougherty, L.R.; Durbin, C.E. Social and non-social behavioral inhibition in preschool-age children: Differential associations with parent-reports of temperament and anxiety. Child Psychiatry Hum. Dev. 2011, 42, 390–405. [Google Scholar] [CrossRef] [PubMed]
- Gagne, J.R.; Miller, M.M.; Goldsmith, H.H. Early-but modest-gender differences in focal aspects of childhood temperament. Pers. Individ. Differ. 2013, 55, 95–100. [Google Scholar] [CrossRef]
- Johnson, V.C.; Olino, T.M.; Klein, D.N.; Dyson, M.W.; Bufferd, S.J.; Durbin, C.E.; Dougherty, L.R.; Hayden, E.P. A Longitudinal Investigation of Predictors of the Association between Age 3 and Age 6 Behavioural Inhibition. J. Res. Pers. 2016, 63, 51–61. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bishop, G.; Spence, S.H.; McDonald, C. Can Parents and Teachers Provide a Reliable and Valid Report of Behavioral Inhibition? Child Dev. 2003, 74, 1899–1917. [Google Scholar] [CrossRef]
- Kim, J.; Klein, D.N.; Olino, T.M.; Dyson, M.W.; Dougherty, L.R.; Durbin, C.E. Psychometric properties of the Behavioral Inhibition Questionnaire in preschool children. J. Pers. Assess. 2011, 93, 545–555. [Google Scholar] [CrossRef]
- Martin, R.P.; Wisenbaker, J.; Baker, J.; Huttunen, M.O. Gender differences in temperament at six months and five years. Infant Behav. Dev. 1997, 20, 339–347. [Google Scholar] [CrossRef]
- Mullen, M.; Snidman, N.; Kagan, J. Brief report free-play behavior in inhibited and uninhibited children. Infant Behav. Dev. 1993, 16, 383–389. [Google Scholar] [CrossRef]
- Stevenson-Hinde, J.; Shouldice, A. 4.5 to 7 years: Fearful behaviour, fears and worries. J. Child Psychol. Psychiatry 1995, 36, 1027–1038. [Google Scholar] [CrossRef]
- Gartstein, M.A.; Carranza, J.A.; González-Salinas, C.; Ato, E.; Galián, M.D.; Erickson, N.L.; Potapova, N. Cross-Cultural Comparisons of Infant Fear: A Multi-Method Study in Spain and the United States. J. Cross-Cult. Psychol. 2016, 47, 1178–1193. [Google Scholar] [CrossRef]
- Gartstein, M.A.; Gonzalez, C.; Carranza, J.A.; Ahadi, S.A.; Ye, R.; Rothbart, M.K.; Yang, S.W. Studying cross-cultural differences in the development of infant temperament: People’s Republic of China, the United States of America, and Spain. Child Psychiatry Hum. Dev. 2006, 37, 145–161. [Google Scholar] [CrossRef] [PubMed]
- Howard, M.; Muris, P.; Loxton, H.; Wege, A. Anxiety-Proneness, Anxiety Symptoms, and The Role of Parental Overprotection in Young South African Children. J. Child Fam. Stud. 2017, 26, 262–270. [Google Scholar] [CrossRef]
- Rubin, K.H.; Hemphill, S.A.; Chen, X.; Hastings, P.; Sanson, A.; Coco, A.L.; Zappulla, C.; Chung, O.-B.; Park, S.-Y.; Doh, H.S.; et al. A cross-cultural study of behavioral inhibition in toddlers: East-West-North-South. Int. J. Behav. Dev. 2006, 30, 219–226. [Google Scholar] [CrossRef]
- Vreeke, L.J.; Muris, P.; Mayer, B.; Huijding, J.; Bos, A.E.; van der Veen, M.; Raat, H.; Verheij, F. The assessment of an inhibited, anxiety-prone temperament in a Dutch multi-ethnic population of preschool children. Eur. Child Adolesc. Psychiatry 2012, 21, 623–633. [Google Scholar] [CrossRef] [PubMed]
- Geng, F.; Hu, Y.; Wang, Y.; Chen, F. Two types of behavioral inhibition: Relations to effortful control and attention in school children. J. Res. Pers. 2011, 45, 662–669. [Google Scholar] [CrossRef]
- Chronis-Tuscano, A.; Degnan, K.A.; Pine, D.S.; Perez-Edgar, K.; Henderson, H.A.; Diaz, Y.; Raggi, V.L.; Fox, N.A. Stable early maternal report of behavioral inhibition predicts lifetime social anxiety disorder in adolescence. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 928–935. [Google Scholar] [CrossRef]
- Crockenberg, S.C.; Leerkes, E.M. Infant and maternal behavior moderate reactivity to novelty to predict anxious behavior at 2.5 years. Dev. Psychopathol. 2006, 18, 17–34. [Google Scholar] [CrossRef]
- Degnan, K.A.; Fox, N.A. Behavioral inhibition and anxiety disorders: Multiple levels of a resilience process. Dev. Psychopathol. 2007, 19, 729–746. [Google Scholar] [CrossRef]
- Degnan, K.A.; Henderson, H.A.; Fox, N.A.; Rubin, K.H. Predicting Social Wariness in Middle Childhood: The Moderating Roles of Child Care History, Maternal Personality and Maternal Behavior. Soc. Dev. 2008, 17, 471–487. [Google Scholar] [CrossRef]
- Bourdon, J.L.; Savage, J.E.; Verhulst, B.; Carney, D.M.; Brotman, M.A.; Pine, D.S.; Leibenluft, E.; Roberson-Nay, R.; Hettema, J.M. The Genetic and Environmental Relationship between Childhood Behavioral Inhibition and Preadolescent Anxiety. Twin Res. Hum. Genet. Off. J. Int. Soc. Twin Stud. 2019, 22, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Frenkel, T.I.; Fox, N.A.; Pine, D.S.; Walker, O.L.; Degnan, K.A.; Chronis-Tuscano, A. Early childhood behavioral inhibition, adult psychopathology and the buffering effects of adolescent social networks: A twenty-year prospective study. J. Child Psychol. Psychiatry 2015, 56, 1065–1073. [Google Scholar] [CrossRef]
- Stumper, A.; Danzig, A.P.; Dyson, M.W.; Olino, T.M.; Carlson, G.A.; Klein, D.N. Parents’ behavioral inhibition moderates association of preschoolers’ BI with risk for age 9 anxiety disorders. J. Affect. Disord. 2017, 210, 35–42. [Google Scholar] [CrossRef]
- Nigg, J.T. Temperament and developmental psychopathology. J. Child Psychol. Psychiatry 2006, 47, 395–422. [Google Scholar] [CrossRef]
- Williams, L.R.; Degnan, K.A.; Perez-Edgar, K.E.; Henderson, H.A.; Rubin, K.H.; Pine, D.S.; Steinberg, L.; Fox, N.A. Impact of behavioral inhibition and parenting style on internalizing and externalizing problems from early childhood through adolescence. J. Abnorm. Child Psychol. 2009, 37, 1063–1075. [Google Scholar] [CrossRef] [PubMed]
- Bayer, J.K.; Morgan, A.; Prendergast, L.A.; Beatson, R.; Gilbertson, T.; Bretherton, L.; Hiscock, H.; Rapee, R.M. Predicting Temperamentally Inhibited Young Children’s Clinical-Level Anxiety and Internalizing Problems from Parenting and Parent Wellbeing: A Population Study. J. Abnorm. Child Psychol. 2019, 47, 1165–1181. [Google Scholar] [CrossRef] [PubMed]
- Biederman, J.; Hirshfeld-Becker, D.R.; Rosenbaum, J.F.; Herot, C.; Friedman, D.; Snidman, N.; Kagan, J.; Faraone, S.V. Further evidence of association between behavioral inhibition and social anxiety in children. Am. J. Psychiatry 2001, 158, 1673–1679. [Google Scholar] [CrossRef] [PubMed]
- Buzzell, G.A.; Troller-Renfree, S.V.; Barker, T.V.; Bowman, L.C.; Chronis-Tuscano, A.; Henderson, H.A.; Kagan, J.; Pine, D.S.; Fox, N.A. A Neurobehavioral Mechanism Linking Behaviorally Inhibited Temperament and Later Adolescent Social Anxiety. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 1097–1105. [Google Scholar] [CrossRef] [PubMed]
- Hudson, J.L.; Murayama, K.; Meteyard, L.; Morris, T.; Dodd, H.F. Early Childhood Predictors of Anxiety in Early Adolescence. J. Abnorm. Child Psychol. 2019, 47, 1121–1133. [Google Scholar] [CrossRef]
- Lonigan, C.J.; Phillips, B.M. Temperamental influences on the development of anxiety disorders. In The Developmental Psychopathology of Anxiety; Vasey, M.W., Dadds, M.R., Eds.; Oxford University Press: Oxford, UK, 2001; pp. 60–91. [Google Scholar]
- Walker, O.L.; Henderson, H.A.; Degnan, K.A.; Penela, E.C.; Fox, N.A. Associations Between Behavioral Inhibition and Children’s Social Problem Solving Behavior During Social Exclusion. Soc. Dev. 2014, 23, 487–501. [Google Scholar] [CrossRef]
- Muris, P.; Hendriks, E.; Bot, S. Children of Few Words: Relations among Selective Mutism, Behavioral Inhibition, and (Social) Anxiety Symptoms in 3- to 6-Year-Olds. Child Psychiatry Hum. Dev. 2016, 47, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Clauss, J.A.; Blackford, J.U. Behavioral inhibition and risk for developing social anxiety disorder: A meta-analytic study. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 1066–1075.e1. [Google Scholar] [CrossRef] [PubMed]
- Rubin, K.H.; Coplan, R.J.; Bowker, J.C. Social withdrawal in childhood. Annu. Rev. Psychol. 2009, 60, 141–171. [Google Scholar] [CrossRef] [PubMed]
- Garcia Coll, C.; Kagan, J.; Reznick, J.S. Behavioral inhibition in young children. Child Dev. 1984, 55, 1005–1019. [Google Scholar] [CrossRef]
- Goldsmith, H.H.; Reilly, J.; Lemery, K.S.; Longley, S.; Prescott, A. The Laboratory Assessment Temperament Battery—Preschool Version. Description of Procedures; University of Wisconsin: Madison, WI, USA, 1999. [Google Scholar]
- Rothbart, M.K.; Bates, J.E. Temperament. In Handbook of Child. Psychology; Damon, W., Lerner, R., Eisenberg, N., Eds.; Wiley: New York, NY, USA, 2006; Volume 3. [Google Scholar]
- Mernick, B.; Pine, A.; Gendler, T.; Shechner, T. A Psychometric Evaluation of the Behavioral Inhibition Questionnaire in a Non-Clinical Sample of Israeli Children and Adolescents. J. Child Fam. Stud. 2018, 27, 1794–1804. [Google Scholar] [CrossRef]
- Gensthaler, A.; Möhler, E.; Resch, F.; Paulus, F.; Schwenck, C.; Freitag, C.M.; Goth, K. Retrospective Assessment of Behavioral Inhibition in Infants and Toddlers: Development of a Parent Report Questionnaire. Child Psychiatry Hum. Dev. 2013, 44, 152–165. [Google Scholar] [CrossRef] [PubMed]
- Ballespí, S.; Jané, M.C.; Riba, M.D.; Domènech-Llaberia, E. Preschool Behavioural Inhibition Scale—Teacher’s form (PBIS-T): Psychometric properties. Psicothema 2003, 15, 205–210. [Google Scholar]
- Ballespí, S.; Jané, M.C.; Riba, M.D. The Behavioural Inhibition Scale for children aged 3 to 6 (BIS 3–6): Validity based on its relation with observational measures. J. Psychopathol. Behav. Assess. 2012, 34, 487–496. [Google Scholar] [CrossRef]
- Presley, R.; Martin, R.P. Toward a structure of preschool temperament: Factor structure of the temperament assessment battery for children. J. Pers. 1994, 62, 415–448. [Google Scholar] [CrossRef]
- Rothbart, M.K.; Ahadi, S.A.; Hershey, K.L.; Fisher, P. Investigations of temperament at three to seven years: The Children’s Behavior Questionnaire. Child Dev. 2001, 72, 1394–1408. [Google Scholar] [CrossRef]
- Coplan, R.J.; Prakash, K.; O’Neil, K.; Armer, M. Do you “want” to play? Distinguishing between conflicted shyness and social disinterest in early childhood. Dev. Psychol. 2004, 40, 244–258. [Google Scholar] [CrossRef]
- Edwards, S.L. Temperament and Environmental Risk Factors Contributing to Anxiety Symptoms in Preschool-Aged Children; Macquarie University: Sydney, Australia, 2007. [Google Scholar]
- Birmaher, B.; Khetarpal, S.; Brent, D.; Cully, M.; Balach, L.; Kaufman, J.; Neer, S.M. The Screen for Child Anxiety Related Emotional Disorders (SCARED): Scale Construction and Psychometric Characteristics. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 545–553. [Google Scholar] [CrossRef]
- Conners, C.K.; Sitarenios, G.; Parker, J.D.A.; Epstein, J.N. The Revised Conners’ Parent Rating Scale (CPRS-R): Factor Structure, Reliability, and Criterion Validity. J. Abnorm. Child Psychol. 1998, 26, 257–268. [Google Scholar] [CrossRef]
- Fu, X.; Taber-Thomas, B.C.; Perez-Edgar, K. Frontolimbic functioning during threat-related attention: Relations to early behavioral inhibition and anxiety in children. Biol. Psychol. 2017, 122, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Morales, S.; Taber-Thomas, B.C.; Perez-Edgar, K.E. Patterns of attention to threat across tasks in behaviorally inhibited children at risk for anxiety. Dev. Sci. 2017, 20, e12391. [Google Scholar] [CrossRef] [PubMed]
- Poole, K.L.; Anaya, B.; Perez-Edgar, K.E. Behavioral inhibition and EEG delta-beta correlation in early childhood: Comparing a between-subjects and within-subjects approach. Biol. Psychol. 2020, 149, 107785. [Google Scholar] [CrossRef] [PubMed]
- Premo, J.E.; Mannella, K.A.; Duval, E.R.; Liu, Y.; Morrison, C.L.; Moser, J.S.; Muzik, M.; Rosenblum, K.L.; Fitzgerald, K.D. Startle to neutral, not negative stimuli: A neurophysiological correlate of behavioral inhibition in young children. Dev. Psychobiol. 2021. [Google Scholar] [CrossRef]
- Chronis-Tuscano, A.; Rubin, K.H.; O’Brien, K.A.; Coplan, R.J.; Thomas, S.R.; Dougherty, L.R.; Cheah, C.S.; Watts, K.; Heverly-Fitt, S.; Huggins, S.L.; et al. Preliminary evaluation of a multimodal early intervention program for behaviorally inhibited preschoolers. J. Consult. Clin. Psychol. 2015, 83, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Vreeke, L.J.; Muris, P. Relations between behavioral inhibition, big five personality factors, and anxiety disorder symptoms in non-clinical and clinically anxious children. Child Psychiatry Hum. Dev. 2012, 43, 884–894. [Google Scholar] [CrossRef] [PubMed]
- Edwards, S.L.; Rapee, R.M.; Kennedy, S. Prediction of anxiety symptoms in preschool-aged children: Examination of maternal and paternal perspectives. J. Child Psychol. Psychiatry 2010, 51, 313–321. [Google Scholar] [CrossRef]
- Vreeke, L.J.; Muris, P.; Mayer, B.; Huijding, J.; Rapee, R.M. Skittish, shielded, and scared: Relations among behavioral inhibition, overprotective parenting, and anxiety in native and non-native Dutch preschool children. J. Anxiety Disord. 2013, 27, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Broeren, S.; Muris, P.; Diamantopoulou, S.; Baker, J.R. The course of childhood anxiety symptoms: Developmental trajectories and child-related factors in normal children. J. Abnorm. Child Psychol. 2013, 41, 81–95. [Google Scholar] [CrossRef]
- Azham, A.A.; Janon, N.S. The Relationship between Parental Anxiety, Child’s Behavioral Inhibition and Child Anxiety. Southeast Asia Early Child. J. 2021, 10, 50–61. [Google Scholar]
- Kennedy, S.J.; Rapee, R.M.; Edwards, S.L. A selective intervention program for inhibited preschool-aged children of parents with an anxiety disorder: Effects on current anxiety disorders and temperament. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Lau, E.X.; Rapee, R.M.; Coplan, R.J. Combining child social skills training with a parent early intervention program for inhibited preschool children. J. Anxiety Disord. 2017, 51, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Barrett, P.; Fisak, B.; Cooper, M. The Treatment of Anxiety in Young Children: Results of an Open Trial of the Fun FRIENDS Program. Behav. Chang. 2015, 32, 231–242. [Google Scholar] [CrossRef]
- van der Sluis, C.M.; van der Bruggen, C.O.; Brechman-Toussaint, M.L.; Thissen, M.A.; Bogels, S.M. Parent-directed cognitive behavioral therapy for young anxious children: A pilot study. Behav. Ther. 2012, 43, 583–592. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modelling, 2nd ed.; The Guilford Press: New York, NY, USA, 2005. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Axia, G. QUIT: Questionari Italiani del Temperamento; Erickson: Trento, Italy, 2002. [Google Scholar]
- Conners, C.K. Conners’ Rating Scales—Revised; Adattamento italiano a cura di Maria Nobile, Barbara Alberti e Alessandro Zuddas; Giunti OS—Organizzazioni Speciali: Firenze, Italy, 2007. [Google Scholar]
- International Test Commission. The ITC Guidelines for Translating and Adapting Tests, 2nd ed.; Available online: www.InTestCom.org (accessed on 16 July 2020).
- Thomas, A.; Chess, S. Temperament and Development; Brunner/Mazel: New York, NY, USA, 1977. [Google Scholar]
- Leen-Feldner, E.W.; Zvolensky, M.J.; Feldner, M.T.; Lejuez, C.W. Behavioral inhibition: Relation to negative emotion regulation and reactivity. J. Individ. Differ. 2004, 36, 1235–1247. [Google Scholar] [CrossRef]
- Di Maggio, R.; Zappulla, C.; Pace, U. La valutazione del temperamento infantile: Osservazioni dirette e indirette delle espressioni emotive nel primo anno di vita. [The evaluation of infant temperament: Direct and indirect observations of emotional expressions in the first year of life.]. Psicol. Clin. Svilupp. 2016, 20, 451–468. [Google Scholar]
- Provenzi, L.; Cassiano, R.G.M.; Scotto di Minico, G.; Linhares, M.B.M.; Montirosso, R. Study Protocol for the Preschooler Regulation of Emotional Stress (PRES) Procedure. Front. Psychol. 2017, 8, 1653. [Google Scholar] [CrossRef] [PubMed]
- Brooker, R.J.; Buss, K.A.; Lemery-Chalfant, K.; Aksan, N.; Davidson, R.J.; Goldsmith, H.H. The development of stranger fear in infancy and toddlerhood: Normative development, individual differences, antecedents, and outcomes. Dev. Sci. 2013, 16, 864–878. [Google Scholar] [CrossRef] [PubMed]
- Fang, H.; Gagne, J.R. Young children’s behavioral inhibition mediates the association between maternal negative affectivity and internalizing problems: Observations, parent-report, and moderation of associations by age. Int. J. Behav. Dev. 2017, 42, 284–293. [Google Scholar] [CrossRef]
- Pfeifer, M.; Goldsmith, H.H.; Davidson, R.J.; Rickman, M. Continuity and change in inhibited and uninhibited children. Child Dev. 2002, 73, 1474–1485. [Google Scholar] [CrossRef]
- Robinson, J.L.; McGrath, J.; Corley, R.P. The conduct of the study: Sample and procedures. In Infancy to Early Childhood: Genetic and Environmental Influences on Developmental Change; Emde, R.N., Hewitt, J.K., Eds.; Oxford University Press: New York, NY, USA, 2001; pp. 23–41. [Google Scholar]
- Volbrecht, M.M.; Goldsmith, H.H. Early temperamental and family predictors of shyness and anxiety. Dev. Psychol. 2010, 46, 1192–1205. [Google Scholar] [CrossRef] [PubMed]
- Kagan, J.; Reznick, J.S.; Snidman, N. The physiology and psychology of behavioral inhibition in children. Child Dev. 1987, 58, 1459–1473. [Google Scholar] [CrossRef]
- Arbuckle, J.L. Amos (Version 26.0) [Computer Program]; IBM SPSS: Chicago, IL, USA, 2019. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Evaluating model fit. In Structural Equation Modelling: Concepts, Issues and Applications; Hoyle, R.H., Ed.; SAGE: Thousand Oaks, CA, USA, 1995; pp. 76–99. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Mulaik, S.A.; James, L.R.; Van Alstine, J.; Bennet, N.; Lind, S.; Stilwell, C.D. Evaluation of goodness-of-fit indices for structural equation models. Psychol. Bull. 1985, 105, 430–445. [Google Scholar] [CrossRef]
- Muris, P.; Meesters, C.; Bouwman, L.; Notermans, S. Relations among behavioral inhibition, shame- and guilt-proneness, and anxiety disorders symptoms in non-clinical children. Child Psychiatry Hum. Dev. 2015, 46, 209–216. [Google Scholar] [CrossRef]
- Rubin, K.H.; Cheah, C.S.L.; Fox, N. Emotion regulation, parenting and display of social reticence in preschoolers. Early Educ. Dev. 2001, 12, 97–115. [Google Scholar] [CrossRef]
- Kochanska, G.; Coy, K.C.; Tjebkes, T.L.; Husarek, S.J. Individual differences in emotionality in infancy. Child Dev. 1998, 69, 375–390. [Google Scholar] [CrossRef] [PubMed]
- Buss, A.; Plomin, R. Theory and Measurement of EAS, Temperament: Early Developing Personality Traits; Hillsdale, L., Ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1984. [Google Scholar]
- Sandstrom, A.; Uher, R.; Pavlova, B. Prospective Association between Childhood Behavioral Inhibition and Anxiety: A Meta-Analysis. J. Abnorm. Child Psychol. 2020, 48, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Durbin, C.E.; Wilson, S. Convergent validity of and bias in maternal reports of child emotion. Psychol. Assess. 2012, 24, 647–660. [Google Scholar] [CrossRef] [PubMed]
- Hayden, E.P.; Durbin, C.E.; Klein, D.N.; Olino, T.M. Maternal personality influences the relationship between maternal reports and laboratory measures of child temperament. J. Pers. Assess. 2010, 92, 586–593. [Google Scholar] [CrossRef]
- Faisca, L.; Ferreira, L.I.; Fernandes, C.C.; Gagne, J.R.; Martins, A.T. Behavioral Inhibition in childhood: European Portuguese Adaptation of an observational measure (Lab-TAB). Children 2021, 8, 162. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, H.H.; Campos, J.J. The structure of temperamental fear and pleasure in infants: A psychometric perspective. Child Dev. 1990, 61, 1944–1964. [Google Scholar] [CrossRef] [PubMed]
- Rothbart, M.K.; Derryberry, D.; Hershey, K. Stability of temperament in childhood: Laboratory infant assessment to parent report at seven years. In Temperament and Personality Development across the Life Span; Molfese, V.J., Molfese, D.L., Eds.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2000; pp. 85–119. [Google Scholar]
- Mangelsdorf, S.C.; Schoppe, S.J.; Buur, H. The meaning of parental reports: A contextual approach to the study of temperament and behavior problems in childhood. In Temperament and Personality Development across the Life Span; Molfese, V.J., Molfese, D.L., Eds.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2000; pp. 121–140. [Google Scholar]
- Kagan, J. The Temperamental Thread. How Genes, Culture, Time, and Luck Make Us Who We Are; Dana Press: New York, NY, USA, 2010. [Google Scholar]


{kind=link}
| Sample Characteristics | Parents (N = 417) | Mothers (N = 230) | Fathers (N = 187) |
|---|---|---|---|
| Age, mean ± SD (range) | 38.5 ± 5.4 (26–56) | 37.0 ± 4.5 (26–48) | 40.4 ± 5.8 (26–56) |
| Nationality, n (%) | |||
| Italian | 378 (91%) | 209 (91%) | 168 (91%) |
| Foreign | 39 (9%) | 20 (9%) | 16 (9%) |
| Educational Level, n (%) | |||
| Primary | 6 (1%) | 2 (1%) | 4 (2%) |
| Secondary | 117 (29%) | 52 (23%) | 65 (36%) |
| High school | 201 (50%) | 117 (52%) | 84 (46%) |
| University | 82 (20%) | 54 (24%) | 28 (16%) |
| Marital status, n (%) | |||
| Married | 275 (68%) | 148 (66%) | 127 (71%) |
| Living together | 25 (6%) | 13 (6%) | 12 (7%) |
| Separated | 16 (4%) | 11 (5%) | 5 (3%) |
| Single | 86 (22%) | 52 (23%) | 34 (19%) |
| Factors | Mean | SE | F (1384) | Mean | SE | F (1209) | Mean | SE | F (1174) |
|---|---|---|---|---|---|---|---|---|---|
| Parents a | Mothers b | Fathers c | |||||||
| Total BIQ | |||||||||
| Males | 89.47 | 2.06 | 11.96 ** | 94.52 | 3.00 | 0.09 | 90.99 | 2.89 | 2.24 |
| Females | 99.22 | 1.92 | (P.η2 = 0.03) | 95.74 | 2.82 | (P.η2 < 0.01) | 96.81 | 2.61 | (P.η2 = 0.01) |
| Total | 94.35 | 1.41 | 95.13 | 2.06 | 93.90 | 1.95 | |||
| Peers | |||||||||
| Males | 18.20 | 0.59 | 13.15 ** | 18.80 | 0.84 | 4.07 * | 17.73 | 0.82 | 8.03 ** |
| Females | 21.12 | 0.55 | (P.η2 = 0.03) | 21.13 | 0.79 | (P.η2 = 0.02) | 20.87 | 0.74 | (P.η2 = 0.04) |
| Total | 19.66 | 0.40 | 19.87 | 0.58 | 19.30 | 0.55 | |||
| Physical Challenges | |||||||||
| Males | 10.64 | 0.31 | 1.29 | 10.34 | 0.42 | 1.51 | 10.84 | 0.45 | 0.10 |
| Females | 11.12 | 0.29 | (P.η2 < 0.01) | 11.05 | 0.40 | (P.η2 = 0.01) | 11.03 | 0.41 | (P.η2 < 0.01) |
| Total | 10.88 | 0.21 | 10.70 | 0.29 | 10.93 | 0.30 | |||
| Separation | |||||||||
| Males | 12.39 | 0.49 | 4.08 | 14.38 | 0.71 | 2.43 | 12.65 | 0.66 | 0.03 |
| Females | 13.74 | 0.46 | (P.η2 = 0.01) | 12.87 | 0.67 | (P.η2 = 0.01) | 12.49 | 0.60 | (P.η2 < 0.01) |
| Total | 13.06 | 0.33 | 13.63 | 0.49 | 12.57 | 0.45 | |||
| Performance Situations | |||||||||
| Males | 12.88 | 0.41 | 0.48 | 13.41 | 0.56 | 0.22 | 13.03 | 0.59 | 0.04 |
| Females | 13.26 | 0.38 | (P.η2 < 0.01) | 13.05 | 0.53 | (P.η2 < 0.01) | 12.87 | 0.53 | (P.η2 < 0.01) |
| Total | 13.07 | 0.28 | 13.23 | 0.39 | 12.95 | 0.40 | |||
| Adults | |||||||||
| Males | 12.41 | 0.42 | 12.20 ** | 12.86 | 0.60 | 0.80 | 12.99 | 0.60 | 2.79 |
| Females | 14.42 | 0.39 | (P.η2 = 0.03) | 13.60 | 0.57 | (P.η2 < 0.01) | 14.34 | 0.54 | (P.η2 = 0.02) |
| Total | 13.42 | 0.29 | 13.23 | 0.41 | 13.66 | 0.41 | |||
| Unfamiliar situations | |||||||||
| Males | 23.04 | 0.62 | 9.30 ** | 24.72 | 0.90 | 0.30 | 23.76 | 0.87 | 1.56 |
| Females | 25.64 | 0.58 | (P.η2 = 0.02) | 24.04 | 0.85 | (P.η2 < 0.01) | 25.22 | 0.78 | (P.η2 = 0.01) |
| Total | 24.34 | 0.42 | 24.38 | 0.62 | 24.49 | 0.58 | |||
| Model | GFI | NFI | PNFI | SRMR |
|---|---|---|---|---|
| Parent BIQ | ||||
| Model 1: 1 factor | 0.93 | 0.91 | 0.84 | 0.09 |
| Model 2: 3 correlated factors | 0.95 | 0.92 | 0.85 | 0.08 |
| Model 3: 6 correlated factors | 0.97 | 0.96 | 0.86 | 0.06 |
| Model 4: 6 first-order factors. 1 second-order factor | 0.97 | 0.96 | 0.88 | 0.06 |
| Model | Parental Role (Mothers and Fathers) | |||
|---|---|---|---|---|
| GFI | NFI | PNFI | SRMR | |
| Configural invariance: Factor structure constrained to be equal | 0.97 | 0.95 | 0.85 | 0.06 |
| Metric invariance: Factor loadings constrained to be equal | 0.96 | 0.94 | 0.88 | 0.07 |
| Parents | Mothers | Fathers | ||||
|---|---|---|---|---|---|---|
| Alpha | Item-Total | Alpha | Item-Total | Alpha | Item-Total | |
| Total BIQ | 0.92 | 0.15–0.71 | 0.92 | 0.15–0.73 | 0.90 | 0.13–0.67 |
| Peers | 0.85 | 0.56–0.70 | 0.86 | 0.57–0.70 | 0.83 | 0.50–0.70 |
| Physical Challenges | 0.41 | 0.07–0.33 | 0.44 | 0.07–0.35 | 0.37 | 0.07–0.34 |
| Separation | 0.87 | 0.69–0.76 | 0.88 | 0.72–0.79 | 0.84 | 0.63–0.75 |
| Performance Situations | 0.75 | 0.49–0.64 | 0.75 | 0.48–0.66 | 0.74 | 0.49–0.60 |
| Adults | 0.81 | 0.51–0.71 | 0.84 | 0.53–0.73 | 0.78 | 0.49–0.68 |
| Unfamiliar Situations | 0.80 | 0.27–0.68 | 0.83 | 0.26–0.70 | 0.76 | 0.27–0.69 |
| BIQ Total Score | QUIT Dimensions | |||||
|---|---|---|---|---|---|---|
| Social Orientation | Novelty Inhibition | Motor Activity | Positive Emotionality | Negative Emotionality | Attention | |
| Parents a | −0.37 ** | 0.49 ** | −0.04 | −0.37 * | 0.24 ** | −0.16 ** |
| Mothers b | −0.37 ** | 0.50 ** | 0.01 | −0.32 ** | 0.23 ** | −0.14 * |
| Fathers c | −0.37 ** | 0.47 ** | −0.12 | −0.45 ** | 0.26 ** | −0.21 * |
| LAB-TAB Social Inhibition Indexes | LAB-TAB Non-Social Inhibition Indexes | |||
|---|---|---|---|---|
| BIQ Total Score and Subscales | Intensity of Decrease in Activity | Intensity of Verbal Hesitancy | Total Number of Objects Touched | Latency to Intentionally Touch the First Object |
| Parents (N = 41) | ||||
| Total BIQ | 0.33 * | 0.08 | −0.25 | 0.25 |
| Peers | 0.28 | −0.03 | −0.19 | 0.09 |
| Physical Challenges | −0.08 | −0.04 | −0.13 | 0.32 * |
| Separation | 0.40 ** | 0.14 | −0.38 * | 0.21 |
| Performance Situations | 0.18 | −0.16 | −0.25 | 0.17 |
| Adults | 0.36 * | 0.13 | −0.39 * | 0.46 ** |
| Unfamiliar Situations | 0.44 ** | 0.22 | −0.19 | −0.28 |
| Mothers (N = 23) | ||||
| Total BIQ | 0.39 | 0.13 | −0.26 | 0.28 |
| Peers | 0.28 | 0.00 | −0.10 | 0.09 |
| Physical Challenges | −0.06 | 0.17 | −0.22 | 0.39 |
| Separation | 0.52 * | 0.26 | −0.47 * | 0.23 |
| Performance Situations | 0.10 | −0.19 | −0.19 | 0.12 |
| Adults | 0.42 * | 0.27 | −0.42 * | 0.47 * |
| Unfamiliar Situations | 0.43 * | 0.26 | −0.22 | 0.26 |
| Fathers (N = 18) | ||||
| Total BIQ | 0.34 | 0.02 | −0.27 | 0.22 |
| Peers | 0.31 | −0.01 | −0.31 | 0.09 |
| Physical Challenges | −0.02 | −0.34 | −0.04 | 0.22 |
| Separation | 0.29 | −0.00 | −0.26 | 0.20 |
| Performance Situations | 0.31 | −0.11 | −0.31 | 0.26 |
| Adults | 0.29 | −0.08 | −0.38 | 0.45 |
| Unfamiliar Situations | 0.44 | 0.16 | −0.18 | 0.20 |
| BIQ Subscales | Peers | Phys | Separ | Perform | Adults |
|---|---|---|---|---|---|
| Phys | 0.40 | ||||
| Separ | 0.54 | 0.31 | |||
| Perform | 0.52 | 0.30 | 0.31 | ||
| Adults | 0.64 | 0.24 | 0.54 | 0.62 | |
| Unf Sit | 0.76 | 0.60 | 0.75 | 0.48 | 0.77 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agostini, F.; Benassi, M.; Minelli, M.; Mandolesi, L.; Giovagnoli, S.; Neri, E. Validation of the Italian Version of the Behavioral Inhibition Questionnaire (BIQ) for Preschool Children. Int. J. Environ. Res. Public Health 2021, 18, 5522. https://doi.org/10.3390/ijerph18115522
Agostini F, Benassi M, Minelli M, Mandolesi L, Giovagnoli S, Neri E. Validation of the Italian Version of the Behavioral Inhibition Questionnaire (BIQ) for Preschool Children. International Journal of Environmental Research and Public Health. 2021; 18(11):5522. https://doi.org/10.3390/ijerph18115522
Chicago/Turabian StyleAgostini, Francesca, Mariagrazia Benassi, Marianna Minelli, Luca Mandolesi, Sara Giovagnoli, and Erica Neri. 2021. "Validation of the Italian Version of the Behavioral Inhibition Questionnaire (BIQ) for Preschool Children" International Journal of Environmental Research and Public Health 18, no. 11: 5522. https://doi.org/10.3390/ijerph18115522
APA StyleAgostini, F., Benassi, M., Minelli, M., Mandolesi, L., Giovagnoli, S., & Neri, E. (2021). Validation of the Italian Version of the Behavioral Inhibition Questionnaire (BIQ) for Preschool Children. International Journal of Environmental Research and Public Health, 18(11), 5522. https://doi.org/10.3390/ijerph18115522