
Patterns, Management, and Outcome of Traumatic Femur Fracture: Exploring the Experience of the Only Level 1 Trauma Center in Qatar

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Agarwal-Harding, K.J.; Meara, J.G.; Greenberg, S.L.; Hagander, L.E.; Zurakowski, D.; Dyer, G.S. Estimating the Global Incidence of Femoral Fracture from Road Traffic Collisions. J. Bone Jt. Surg. Am. Vol. 2015, 97, e31. [Google Scholar] [CrossRef]
- Anyaehie, U.; Ejimofor, O.; Akpuaka, F.; Nwadinigwe, C. Pattern of femoral fractures and associated injuries in a Nigerian tertiary trauma centre. Niger. J. Clin. Pr. 2015, 18, 462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, A.M.; Tang, Q.O.; Spicer, D. The Epidemiology of Adult Distal Femoral Shaft Fractures in a Central London Major Trauma Centre Over Five Years. Open Orthop. J. 2017, 11, 1277–1291. [Google Scholar] [CrossRef]
- Salminen, S.T.; Pihlajamäki, H.K.; Avikainen, V.J.; Böstman, O.M. Population Based Epidemiologic and Morphologic Study of Femoral Shaft Fractures. Clin. Orthop. Relat. Res. 2000, 372, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Alobaidi, A.S.; Al-Hassani, A.; El-Menyar, A.; Abdelrahman, H.; Tuma, M.; Al-Thani, H.; Aldosari, M.A. Early and late intramedullary nailing of femur fracture: A single center experience. Int. J. Crit. Illn. Inj. Sci. 2016, 6, 143–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Femur Injuries and Fractures. Available online: https://emedicine.medscape.com/article/90779-overview (accessed on 21 May 2021).
- Matityahu, A.; Elliott, I.; Marmor, M.; Caldwell, A.; Coughlin, R.; Gosselin, R.A. Time intervals in the treatment of fractured femurs as indicators of the quality of trauma systems. Bull. World Heal. Organ. 2013, 92, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Yoon, R.S.; Liporace, F.A. Impact of Intramedullary Nailing in the Treatment of Femur Fractures An Evolutionary Perspective. Bull. Hosp. Jt. Dis. (2013) 2018, 76, 9–13. [Google Scholar]
- O’Brien, P.J. Fracture fixation in patients having multiple injuries. Can. J. Surg. 2003, 46, 124–128. [Google Scholar]
- Rodriguez-Merchan, E.C.; Moraleda, L.; Gomez-Cardero, P. Injuries Associated with Femoral Shaft Fractures with Special Emphasis on Occult Injuries. Arch. Bone Jt. Surg. 2013, 1, 59–63. [Google Scholar] [PubMed]
- Adili, A.; Bhandari, M.; Lachowski, R.J.; Kwok, D.C.; Dunlop, R.B. Organ injuries associated with femoral fractures: Implications for severity of injury in motor vehicle collisions. J. Trauma 1999, 46, 386–391. [Google Scholar] [CrossRef]
- Brumback, R.J.; Virkus, W.W. Intramedullary Nailing of the Femur: Reamed Versus Nonreamed. J. Am. Acad. Orthop. Surg. 2000, 8, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-C.; Rau, C.-S.; Kuo, S.C.H.; Chien, P.-C.; Hsieh, C.-H. The influence of ageing on the incidence and site of trauma femoral fractures: A cross-sectional analysis. BMC Musculoskelet. Disord. 2019, 20, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Chang, M.-W.; Liu, H.-T.; Huang, C.-Y.; Chien, P.-C.; Hsieh, H.-Y.; Hsieh, C.-H. Location of Femoral Fractures in Patients with Different Weight Classes in Fall and Motorcycle Accidents: A Retrospective Cross-Sectional Analysis. Int. J. Environ. Res. Public Heal. 2018, 15, 1082. [Google Scholar] [CrossRef] [Green Version]
- Harvin, J.A.; Harvin, W.H.; Camp, E.; Caga-Anan, Z.; Burgess, A.R.; Wade, C.E.; Holcomb, J.B.; Cotton, B.A. Early femur fracture fixation is associated with a reduction in pulmonary complications and hospital charges. J. Trauma Acute Care Surg. 2012, 73, 1442–1449. [Google Scholar] [CrossRef]
- Medda, S.; Halvorson, J. Diaphyseal Femur Fracture; [Updated 2019 Dec 12]; StatPearls Publishing: Treasure Island, FL, USA, 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK493169/ (accessed on 22 May 2021).
- El-Menyar, A.; Al-Thani, H.; Abdelrahman, H.; Zarour, A.; Latifi, R.; Asim, M. Blunt traumatic injury in the Arab Middle Eastern populations. J. Emergencies Trauma Shock. 2014, 7, 88–96. [Google Scholar] [CrossRef]
- Mekkodathil, A.; El-Menyar, A.; Kanbar, A.; Hakim, S.; Ahmed, K.; Siddiqui, T.; Al-Thani, H. Epidemiological and clinical characteristics of fall-related injuries: A retrospective study. BMC Public Heal. 2020, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hu, G.; Baker, S.P. An Explanation for the Recent Increase in the Fall Death Rate Among Older Americans: A Subgroup Analysis. Public Heal. Rep. 2012, 127, 275–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Menyar, A.; Muneer, M.; Samson, D.; Al-Thani, H.; Alobaidi, A.; Mussleman, P.; Latifi, R. Early versus late intramedullary nailing for traumatic femur fracture management: Meta-analysis. J. Orthop. Surg. Res. 2018, 13, 1–11. [Google Scholar] [CrossRef]
- Ibeanusi, S.E.; Chioma, J. Pattern and Outcome of Femoral Fractures Treated in a Regional Trauma Centre in South South, Nigeria. Int. Arch. Orthop. Surg. 2019, 2, 6. [Google Scholar] [CrossRef]
- Sonbol, A.M.; Almulla, A.A.; Hetaimish, B.M.; Taha, W.S.; Mohmmedthani, T.S.; Alfraidi, T.A.; Alrashidi, Y.A. Prevalence of femoral shaft fracture and associated injuries among adults after road traffic collisions in a Saudi Arabian trauma center. J. Musculoskelet. Surg. Res. 2018, 2, 62–65. [Google Scholar] [CrossRef]
- Kouris, G.; Hostiuc, S.; Negoi, I. Femoral fractures in road traffic accidents. Rom. J. Leg. Med. 2012, 20, 279–282. [Google Scholar] [CrossRef]
- Ugezu, A.I.; Nze, I.N.; Ihegihu, C.C.; Chukwuka, N.C.; Ndukwu, C.U.; Ofiaeli, R.O. Management of Femoral Shaft Fractures in a Tertiary Centre, South East Nigeria. Afr. Med. J. 2018, 6, 27–34. [Google Scholar]
- Brumback, R.J.; Uwagie-Ero, S.; Lakatos, R.P.; Poka, A.; Bathon, G.H.; Burgess, A.R. Intramedullary nailing of femoral shaft fractures. Part II: Fracture-healing with static interlocking fixation. J. Bone Joint Surg. 1988, 70A, 1453–1462. [Google Scholar] [CrossRef]
- Winquist, R.A.; Hansen, S.T., Jr.; Clawson, D.K. Closed intramedullary nailing of femoral fractures: A report of five hundred and twenty cases. J. Bone Joint Surg. 1984, 66A, 529–539. [Google Scholar] [CrossRef]
- Brumback, R.J.; Ellison, P.S., Jr.; Lakatos, R.P.; Poka, A.; Bathon, G.H.; Burgess, A.R. Intramedullary nailing of open fractures of the femoral shaft. J. Bone Joint Surg. Am. 1989, 71, 1324–1331. [Google Scholar] [CrossRef] [PubMed]
- Pape, H.-C.; Giannoudis, P.; Krettek, C. The timing of fracture treatment in polytrauma patients: Relevance of damage control orthopedic surgery. Am. J. Surg. 2002, 183, 622–629. [Google Scholar] [CrossRef]
- Li, A.B.; Zhang, W.J.; Guo, W.J.; Wang, X.H.; Jin, H.M.; Zhao, Y.M. Reamed versus unreamed intramedullary nailing for the treatment of femoral fractures: A meta-analysis of prospective randomized controlled trials. Medicine 2016, 95, e4248. [Google Scholar] [CrossRef]
- Canadian Orthopaedic Trauma Society. Reamed versus unreamed intramedullary nailing of the femur: Comparison of the rate of ARDS in multiple injured patients. J. Orthop. Trauma 2006, 20, 384–387. [Google Scholar] [CrossRef]
- Giannoudis, P.V.; Tzioupis, C.; Pape, H.-C. Fat embolism: The reaming controversy. Injury 2006, 37, S50–S58. [Google Scholar] [CrossRef] [PubMed]
- Charash, W.E.; Fabian, T.C.; Croce, M.A. Delayed surgical fixation of femur fractures is a risk factor for pulmonary failure independent of thoracic trauma. J. Trauma 1997, 37, 667–672. [Google Scholar] [CrossRef]
- Bishop, J.A.; Rodriguez, E.K. Closed Intramedullary Nailing of the Femur in the Lateral Decubitus Position. J. Trauma Inj. Infect. Crit. Care 2010, 68, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Wolinsky, P.R.; Mccarty, E.C.; Shyr, Y.; Johnson, K.D. Length of Operative Procedures: Reamed Femoral Intramedullary Nailing Performed with and Without a Fracture Table. J. Orthop. Trauma 1998, 12, 485–495. [Google Scholar] [CrossRef]
- Sanders, R.; Koval, K.J.; DiPasquale, T.; Helfet, D.L.; Frankle, M. Retrograde Reamed Femoral Nailing. J. Orthop. Trauma 1993, 7, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Neradi, D.; Kansal, R.; Aggarwal, S.; Kumar, V.; Dhillon, M.S. Greater trochanteric versus piriformis fossa entry nails for femur shaft fractures: Resolving the controversy. Injury 2019, 50, 1715–1724. [Google Scholar] [CrossRef] [PubMed]
- Ricci, W.M.; Schwappach, J.; Tucker, M.; Coupe, K.; Brandt, A.; Sanders, R.; Leighton, R. Trochanteric versus piriformis entry portal for the treatment of femoral shaft fractures. J. Orthop. Trauma 2006, 20, 663–667. [Google Scholar] [CrossRef] [PubMed]
- Ansari Moein, C.M.; Verhofstad, M.H.; Bleys, R.L.; van der Werken, C. Soft tissue injury related to choice of entry point in antegrade femoral nailing: Piriform fossa or greater trochanter tip. Injury 2005, 36, 1337–1342. [Google Scholar] [CrossRef]
- Andalib, A.; Tahririan, M.A. Is there a place for open intramedullary nailing in femoral shaft fractures? Adv. Biomed. Res. 2014, 3, 157. [Google Scholar] [CrossRef] [PubMed]
- Burç, H.; Atay, T.; Demirci, D.; Baykal, Y.B.; Kirdemir, V.; Yorgancigil, H. The Intramedullary Nailing of Adult Femoral Shaft Fracture by the Way of Open Reduction is a Disadvantage or Not? Indian J. Surg. 2013, 77, 583–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lieurance, R.; Benjamin, J.B.; Rappaport, W.D. Blood Loss and Transfusion in Patients with Isolated Femur Fractures. J. Orthop. Trauma 1992, 6, 175–179. [Google Scholar] [CrossRef]
- Ponnusamy, K.E.; Kim, T.J.; Khanuja, H.S. Perioperative Blood Transfusions in Orthopaedic Surgery. J. Bone Jt. Surgery-Am. 2014, 96, 1836–1844. [Google Scholar] [CrossRef]
- Oliveira, P.R.; Leonhardt, M.C.; Carvalho, V.C.; Kojima, K.E.; Silva, J.S.; Rossi, F.; Lima, A.L.L. Incidence and risk factors associated with infection after intramedullary nailing of femoral and tibial diaphyseal fractures: Prospective study. Injury 2018, 49, 1905–1911. [Google Scholar] [CrossRef] [PubMed]
- Young, S.; Lie, S.A.; Hallan, G.; Zirkle, L.G.; Engesæter, L.B.; Havelin, L.I. Risk Factors for Infection after 46,113 Intramedullary Nail Operations in Low- and Middle-income Countries. World J. Surg. 2013, 37, 349–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.-J.; Choi, D.-H.; Ahn, S.; Sohn, C.H.; Seo, D.-W.; Kim, W.Y. Timing of pulmonary embolisms in femur fracture patients. J. Trauma Acute Care Surg. 2016, 80, 952–956. [Google Scholar] [CrossRef]
- Bosse, M.J.; MacKenzie, E.J.; Riemer, B.L.; Brumback, R.J.; McCarthy, M.L.; Burgess, A.R.; Gens, D.R.; Yasui, Y. Adult Respiratory Distress Syndrome, Pneumonia, and Mortality following Thoracic Injury and a Femoral Fracture Treated Either with Intramedullary Nailing with Reaming or with a Plate. A Comparative Study *. J. Bone Jt. Surgery-Am. 1997, 79, 799–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Made, W.J.; Smit, E.J.; van Luyt, P.A.; van Vugt, A.B. Intramedullary femoral osteosynthesis: An additional cause of ARDS in multiply injured patients? Injury 1996, 27, 391–393. [Google Scholar] [CrossRef]
- Bone, L.B.; Anders, M.J.; Rohrbacher, B.J. Treatment of Femoral Fractures in the Multiply Injured Patient with Thoracic Injury. Clin. Orthop. Relat. Res. 1998, 347, 57–61. [Google Scholar] [CrossRef]
- Nahm, N.J.; Como, J.J.; Wilber, J.H.; Vallier, H.A. Early Appropriate Care: Definitive Stabilization of Femoral Fractures Within 24 Hours of Injury Is Safe in Most patients with multiple Injuries. J. Trauma Inj. Infect. Crit. Care 2011, 71, 175–185. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variable | Value | Variable | Value |
|---|---|---|---|
| Age (mean ± SD) | 30.7 ± 16.2 | Associated injuries | |
| Males | 541 (89.4%) | Tibia | 106 (17.5%) |
| Mechanism of Injury | Fibula | 68 (11.2%) | |
| MVC | 264 (43.6%) | Ankle | 46 (7.6%) |
| Pedestrian | 81 (13.4%) | Knee | 39 (6.4%) |
| Motorcycle/bike crash | 32 (5.3%) | Pelvis | 109 (18.0%) |
| ATV | 16 (2.6%) | Head | 98 (16.2%) |
| Fall from height | 157 (26.0%) | Chest | 146 (24.1%) |
| Fall of a heavy object | 36 (6.0%) | Abdomen | 96 (15.9%) |
| Others | 19 (3.1%) | Spine | 120 (19.8%) |
| Comorbidities | Initial lab results | ||
| Hypertension | 42 (6.9%) | Hemoglobin level (n = 509) | 13.0 ± 2.2 |
| Diabetes mellitus | 39 (6.4%) | White blood cell count (n = 488) | 15.2 ± 6.4 |
| Bronchial asthma | 36 (6.0%) | Neutrophil count (n = 255) | 14.7 ± 13.8 |
| Coronary artery disease | 14 (2.3%) | Platelet count (n = 499) | 259.5 ± 92.3 |
| Initial assessment | International normalized ratio (n = 466) | 1.07 ± 0.14 | |
| Initial heart rate | 96.3 ± 21.4 | ||
| Initial SBP | 125.9 ± 20.4 | ||
| Respiratory rate | 20.3 ± 5.9 | ||
| Injury severity score | 14.8 ± 8.1 |
| Variable | Value |
|---|---|
| DVT prophylaxis (n = 489) | 374 (76.5%) |
| Pre-operative heparin (n = 410) | 30 (7.3%) |
| Unilateral femur fracture | 584 (96.7%) |
| Bilateral femur fracture | 20 (3.3%) |
| Type of Femur Fracture | |
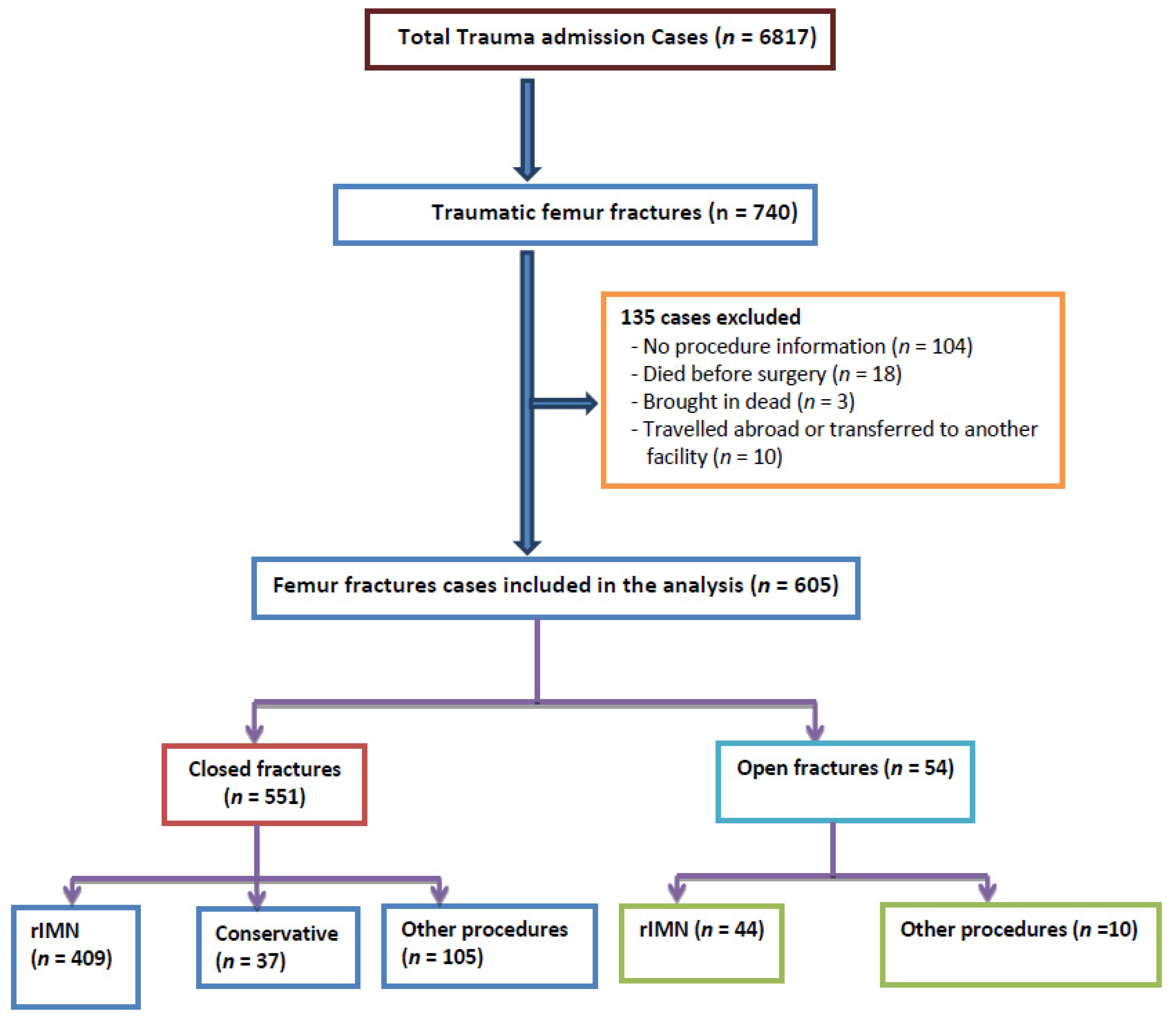
| Close fracture | 551 (91.1%) |
| Open fracture | 54 (8.9%) |
| Reamed intramedullary nailing | 453 (74.9%) |
| Time to IMN (hours) (n = 400) | 20 (1–4382) |
| Early (≤12 h) | 137 (34.3%) |
| Late (>12 h) | 267 (66.8%) |
| External fixation | 45 (8.9%) |
| Conservative management | 37 (6.1%) |
| Implant type (n = 408) | |
| Antegrade nail | 327 (80.1%) |
| Retrograde nail | 81 (19.9%) |
| Site of entry (n = 342) | |
| Piriformis | 245 (71.6%) |
| Trochanteric | 97 (28.4%) |
| Procedure (n = 439) | |
| Open | 145 (33.0%) |
| Closed | 294 (67.0%) |
| Duration of Surgery (hours) | 2.6 ± 1.7 |
| Locking | 453 (100%) |
| Number of procedures (n = 423) | 1 (1–7) |
| Bleeding on admission (n = 432) | 38 (8.8%) |
| Wound Infection (n = 461) | 58 (12.6%) |
| Blood transfusion | 239 (39.5%) |
| Blood units transfused | 4 (1–51) |
| Complications | |
| Pneumonia | 44 (7.3%) |
| Pulmonary embolism | 7 (1.2%) |
| Acute respiratory distress syndrome | 7 (1.2%) |
| Sepsis | 24 (4.0%) |
| Acute renal failure | 13 (2.1%) |
| Hospital length of stay in days | 10 (1–157) |
| ICU stay in days | 7 (1–88) |
| Mortality | 13 (2.1%) |
| Variable | Time to Intramedullary Nailing * | p Value | ||
|---|---|---|---|---|
| Group I: < 6 h (n = 31; 7.7%) | Group II: 6–12 h (n = 106; 26.2%) | Group III: >12 h (n = 267; 66.1%) | ||
| Timing to IMN, median (IQR) h | 4.5 (4.0–5.5) | 10 (8.4–11.0) | 24 (20–72) | 0.001 |
| Site of entry (n = 301) | ||||
| Piriformis | 23 (82.1%) | 70 (82.4%) | 124 (66.0%) | 0.009 for all |
| Trochanteric | 5 (17.9%) | 15 (17.6%) | 64 (34.0%) | |
| Implant type (n = 364) | ||||
| Antegrade nail | 26 (96.3%) | 76 (77.6%) | 186 (77.8%) | 0.07 for all |
| Retrograde nail | 1 (3.7%) | 22 (22.4%) | 53 (22.2%) | |
| Duration of Surgery (h) | 3.2 ± 1.6 | 2.7 ± 1.6 | 2.6 ± 1.5 | 0.17 |
| Complications | ||||
| Wound Infection (n = 312) | 3 (12.5%) | 12 (13.3%) | 27 (13.6%) | 0.97 |
| DVT prophylaxis (n = 320) | 19 (79.2%) | 67 (79.8%) | 159 (75.0%) | 0.65 |
| Sepsis | 2 (6.5%) | 3 (2.9%) | 9 (3.4%) | 0.91 |
| Pulmonary Embolism | 0 (0.0%) | 0 (0.0%) | 6 (2.2%) | 0.52 |
| Acute Respiratory Distress Syndrome | 1 (3.2%) | 1 (1.0%) | 3 (1.1%) | 0.96 |
| Pneumonia | 2 (6.5%) | 4 (3.9%) | 21 (7.9%) | 0.51 |
| Mortality | 0 (0.0%) | 1 (1.0%) | 4 (1.5%) | 0.96 |
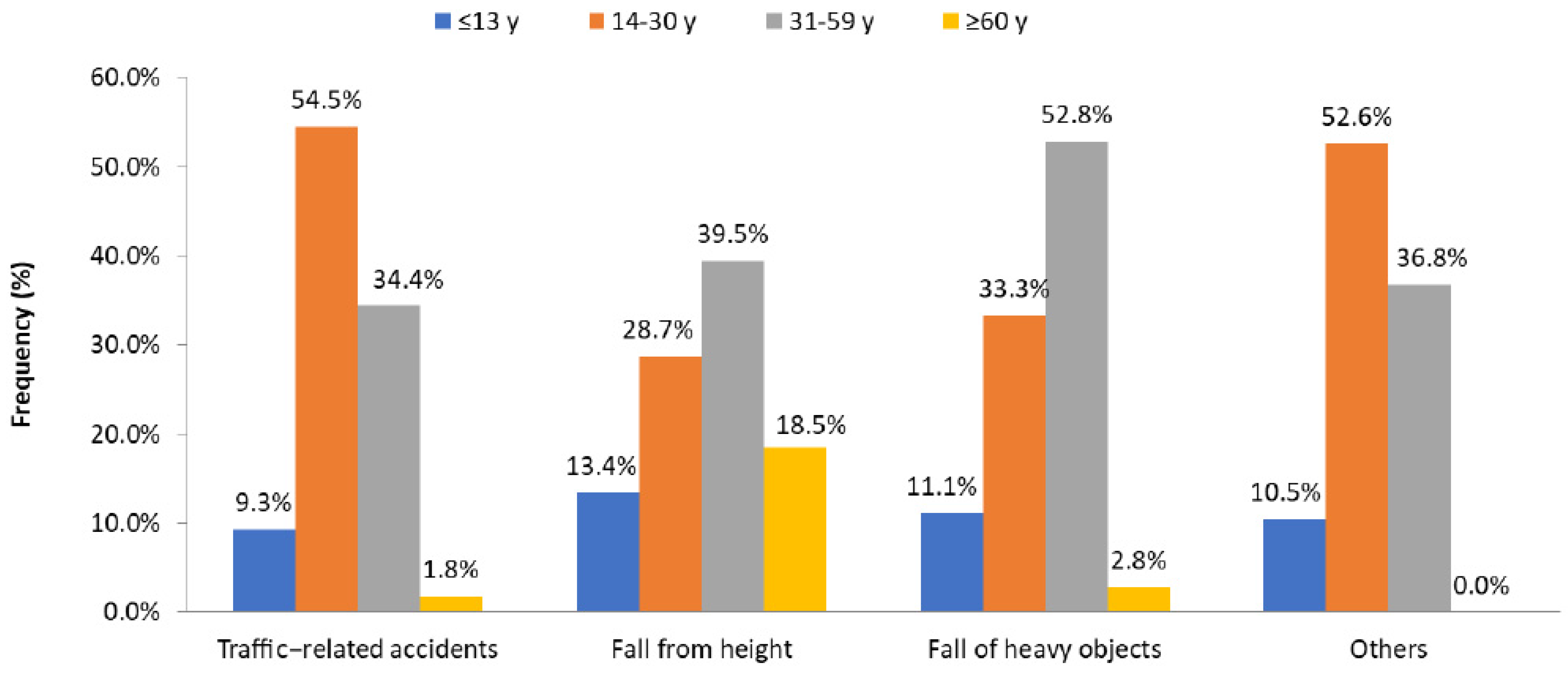
| Variable | Traffic-Related Injury (n = 393) | Fall from Height (n = 157) | Fall of Heavy Object (n = 36) | p Value |
|---|---|---|---|---|
| Age (mean ± SD) | 27.8 ± 12.7 | 37.9 ± 21.6 | 31.7 ± 13.9 | 0.001 |
| Males | 359 (91.3%) | 132 (84.1%) | 34 (94.4%) | 0.05 |
| Injury Severity Score (ISS) | 15.8 ± 8.7 | 12.9 ± 6.3 | 14.1 ± 6.5 | 0.001 |
| ISS > 15 | 138 (35.1%) | 39 (24.8%) | 11 (30.6%) | 0.02 |
| Associated injuries | ||||
| Tibia | 83 (21.1%) | 14 (8.9%) | 7 (19.4%) | 0.006 |
| Fibula | 55 (14.0%) | 11 (7.0%) | 1 (2.8%) | 0.02 |
| Ankle | 31 (7.9%) | 9 (5.7%) | 3 (8.3%) | 0.44 |
| Knee | 29 (7.4%) | 8 (5.1%) | 1 (2.8%) | 0.59 |
| Pelvis | 72 (18.3%) | 23 (14.6%) | 10 (27.8%) | 0.29 |
| Head | 70 (17.8%) | 23 (14.6%) | 3 (8.3%) | 0.37 |
| Chest | 99 (25.2%) | 33 (21.0%) | 10 (27.8%) | 0.69 |
| Abdomen | 70 (17.8%) | 14 (8.9%) | 7 (19.4%) | 0.03 |
| Spine | 80 (20.4%) | 26 (16.6%) | 10 (27.8%) | 0.46 |
| Management | ||||
| Reamed IMN | 307 (78.1%) | 102 (65.0%) | 28 (77.8%) | 0.005 for all |
| Conservative | 16 (4.1%) | 15 (9.6%) | 5 (13.9%) | |
| Other procedures | 70 (17.8%) | 40 (25.5%) | 3 (8.3%) | |
| Time to IMN (hours) | ||||
| Early (<12 h) | 76 (28.6%) | 23 (24.7%) | 8 (30.8%) | 0.88 |
| Late (≥12 h) | 190 (71.4%) | 70 (75.3%) | 18 (69.2%) | |
| Site of entry | ||||
| Piriformis | 166 (72.2%) | 53 (67.1%) | 16 (76.2%) | 0.60 |
| Trochanteric | 64 (27.8%) | 26 (32.9%) | 5 (23.8%) | |
| Implant type | ||||
| Antegrade nail | 215 (77.6%) | 79 (84.9%) | 21 (84.0%) | 0.27 |
| Retrograde nail | 62 (22.4%) | 14 (15.1%) | 4 (16.0%) | |
| Procedure | ||||
| Open | 196 (66.4%) | 70 (69.3%) | 18 (66.7%) | 0.93 |
| Closed | 99 (33.6%) | 31 (30.7%) | 9 (33.3%) | |
| Complications | ||||
| Wound Infection | 46 (15.1%) | 8 (6.7%) | 2 (8.3%) | 0.11 |
| DVT prophylaxis | 249 (78.5%) | 95 (72.5%) | 21 (72.4%) | 0.53 |
| Blood transfusion | 172 (43.8%) | 49 (31.2%) | 16 (44.4%) | 0.002 |
| Blood units transfused | 4 (1–51) | 2 (1–22) | 2 (1–16) | 0.009 |
| Sepsis | 19 (4.8%) | 3 (1.9%) | 2 (5.6%) | 0.31 |
| Pulmonary embolism | 3 (0.8%) | 4 (2.5%) | 0 (0.0%) | 0.28 |
| Acute respirtory distresss syndrome | 6 (1.5%) | 1 (0.6%) | 0 (0.0%) | 0.68 |
| Pneumonia | 35 (8.9%) | 4 (2.5%) | 3 (8.3%) | 0.06 |
| Hospital length of stay | 10 (1–157) | 9 (1–117) | 11 (3–104) | 0.07 |
| Mortality | 12 (3.1%) | 1 (0.6%) | 0 (0.0%) | 0.21 |
| Variable | ≤13 Years (n = 63; 10.5%) | 14–30 Years (n = 279; 46.4%) | 31–59 Years (n = 222; 36.9%) | ≥60 Years (n = 37; 6.2%) | p Value |
|---|---|---|---|---|---|
| Age (mean ± SD) years | 5.9 ± 3.7 | 23.3 ± 4.5 | 40.1 ± 7.4 | 71.9 ± 7.5 | 0.001 |
| Males | 50 (79.4%) | 256 (91.8%) | 211 (95.0%) | 20 (54.1%) | 0.001 |
| ISS mean ± SD | 12.2 ± 6.1 | 16.2 ± 8.9 | 14.2 ± 7.2 | 12.8 ± 7.7 | 0.001 |
| ISS >15 | 10 (15.9%) | 104 (37.3%) | 66 (29.7%) | 9 (24.3%) | 0.005 |
| Associated injuries | |||||
| Tibia | 5 (7.9%) | 48 (17.2%) | 47 (21.2%) | 5 (13.5%) | 0.09 |
| Fibula | 4 (6.3%) | 28 (10.0%) | 32 (14.4%) | 3 (8.1%) | 0.20 |
| Ankle | 3 (4.8%) | 22 (7.9%) | 19 (8.6%) | 1 (2.7%) | 0.50 |
| Knee | 5 (7.9%) | 17 (6.1%) | 15 (6.8%) | 2 (5.4%) | 0.94 |
| Pelvis | 10 (15.9%) | 55 (19.7%) | 38 (17.1%) | 3 (8.1%) | 0.34 |
| Head | 6 (9.5%) | 49 (17.6%) | 38 (17.1%) | 3 (8.1%) | 0.22 |
| Chest | 11 (17.5%) | 73 (26.2%) | 57 (25.7%) | 4 (10.8%) | 0.11 |
| Abdomen | 10 (15.9%) | 53 (19.30%) | 31 (14.0%) | 1 (2.7%) | 0.05 |
| Spine | 4 (6.3%) | 66 (23.7%) | 46 (20.7%) | 3 (8.1%) | 0.004 |
| Management | |||||
| Reamed IMN | 37 (58.7%) | 234 (83.9%) | 161 (72.5%) | 18 (48.6%) | 0.001 for all |
| Conservative | 17 (27.0%) | 7 (2.5%) | 10 (4.5%) | 3 (8.1%) | |
| Other procedures | 9 (14.3%) | 38 (13.6%) | 51 (23.0%) | 16 (43.2%) | |
| Time to IMN (hours) | |||||
| Early (<12 h) | 8 (24.2%) | 55 (26.7%) | 44 (30.6%) | 4 (25.0%) | 0.81 for all |
| Late (≥12 h) | 25 (75.8%) | 151 (73.3%) | 100 (69.4%) | 12 (75.0%) | |
| Site of entry | |||||
| Piriformis | 16 (57.1%) | 135 (75.4%) | 87 (71.3%) | 5 (50.0%) | 0.09 for all |
| Trochanteric | 12 (42.9%) | 44 (24.6%) | 35 (28.7%) | 5 (50.0%) | |
| Implant type | |||||
| Antegrade nail | 22 (64.7%) | 176 (83.0%) | 113 (77.9%) | 14 (93.3%) | 0.04 for all |
| Retrograde nail | 12 (35.3%) | 36 (17.0%) | 32 (22.1%) | 1 (6.7%) | |
| Complications | |||||
| Wound Infection | 2 (4.3%) | 26 (12.6%) | 30 (16.8%) | 0 (0.0%) | 0.02 |
| DVT prophylaxis | 14 (28.0%) | 181 (80.8%) | 154 (84.2%) | 22 (75.9%) | 0.001 |
| Blood transfusion | 7 (11.1%) | 122 (43.7%) | 86 (38.7%) | 22 (59.5%) | 0.001 |
| Blood units transfused | 2 (1–10) | 4 (1–51) | 4 (1–24) | 3 (1–8) | 0.03 |
| Sepsis | 1 (1.6%) | 12 (4.3%) | 8 (3.6%) | 3 (8.1%) | 0.43 |
| Pulmonary Embolism | 2 (3.2%) | 3 (1.1%) | 1 (0.5%) | 1 (2.7%) | 0.26 |
| Acute respiratory distress syndrome | 0 (0.0%) | 4 (1.4%) | 3 (1.4%) | 0 (0.0%) | 0.70 |
| Pneumonia | 3 (4.8%) | 21 (7.5%) | 19 (8.6%) | 1 (2.7%) | 0.51 |
| Hospital length of stay | 6 (1–43) | 10 (1–157) | 10 (1–123) | 15 (4–115) | 0.001 |
| Mortality | 0 (0.0%) | 7 (2.5%) | 3 (1.4%) | 1 (2.7%) | 0.50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghouri, S.I.; Asim, M.; Mustafa, F.; Kanbar, A.; Ellabib, M.; Al Jogol, H.; Muneer, M.; Abdurraheim, N.; Goel, A.P.; Abdelrahman, H.; et al. Patterns, Management, and Outcome of Traumatic Femur Fracture: Exploring the Experience of the Only Level 1 Trauma Center in Qatar. Int. J. Environ. Res. Public Health 2021, 18, 5916. https://doi.org/10.3390/ijerph18115916
Ghouri SI, Asim M, Mustafa F, Kanbar A, Ellabib M, Al Jogol H, Muneer M, Abdurraheim N, Goel AP, Abdelrahman H, et al. Patterns, Management, and Outcome of Traumatic Femur Fracture: Exploring the Experience of the Only Level 1 Trauma Center in Qatar. International Journal of Environmental Research and Public Health. 2021; 18(11):5916. https://doi.org/10.3390/ijerph18115916
Chicago/Turabian StyleGhouri, Syed Imran, Mohammad Asim, Fuad Mustafa, Ahad Kanbar, Mohamed Ellabib, Hisham Al Jogol, Mohammed Muneer, Nuri Abdurraheim, Atirek Pratap Goel, Husham Abdelrahman, and et al. 2021. "Patterns, Management, and Outcome of Traumatic Femur Fracture: Exploring the Experience of the Only Level 1 Trauma Center in Qatar" International Journal of Environmental Research and Public Health 18, no. 11: 5916. https://doi.org/10.3390/ijerph18115916