Abstract
Natural resource extraction projects are often accompanied by complex environmental and social-ecological changes. In this paper, we evaluated the association between commodity extraction and the incidence of diseases. We retrieved council (district)-level outpatient data from all public and private health facilities from the District Health Information System (DHIS2). We combined this information with population data from the 2012 national population census and a geocoded list of resource extraction projects from the Geological Survey of Tanzania (GST). We used Poisson regression with random effects and cluster-robust standard errors to estimate the district-level associations between the presence of three types of commodity extraction (metals, gemstone, and construction materials) and the total number of patients in each disease category in each year. Metal extraction was associated with reduced incidence of several diseases, including chronic diseases (IRR = 0.61, CI: 0.47–0.80), mental health disorders (IRR = 0.66, CI: 0.47–0.92), and undernutrition (IRR = 0.69, CI: 0.55–0.88). Extraction of construction materials was associated with an increased incidence of chronic diseases (IRR = 1.47, CI: 1.15–1.87). This study found that the presence of natural resources commodity extraction is significantly associated with changes in disease-specific patient volumes reported in Tanzania’s DHIS2. These associations differed substantially between commodities, with the most protective effects shown from metal extraction.
1. Introduction
Implementation of natural resource extraction projects often triggers a series of complex environmental and social–ecological changes [1,2,3,4]. These changes include increased population growth and urbanization, infrastructure improvements, movement and installation of heavy machinery, changes in land use, increased business and economic opportunities, and household resettlement [5,6,7]. Such changes can positively or negatively affect the health status of communities in proximity of resource extraction activities [8,9,10,11,12]. Studies have linked activities of the resource extraction with increased incidence of respiratory diseases [13,14]; sexually transmitted infections, including HIV/AIDS [15]; malnutrition [16]; vector-related diseases [17,18,19]; mental health [20,21]; and cancer diseases [9]. On the other hand, resource extraction projects can positively contribute to population health through improved labor market opportunities and corporate social responsibility (CSR) activities that support local health systems or contribute to general health and education programs [22,23,24,25].
Even though a growing literature has highlighted the importance of comprehensive health impact assessments (HIA) of mining projects [26,27,28], evidence on the impact of large-scale mining projects on population health remains limited. One of the key challenges for such projects is the lack of reliable data sources for local population health [4,29,30]. Due to major international efforts, such population-level health data are increasingly becoming available at the health facility level in low- and middle-income countries, often supported by new digital systems. DHIS2 (District Health Information Systems) is one such web-based software application that can be integrated into the national health management information system (HMIS) to facilitate data collection, data use, data management, and archiving of routine data [31]. DHIS2 has been installed in over 73 countries worldwide [32], allowing researchers and policy makers to collect and aggregate data across the health system [33,34,35].
In this study, we used the data from Tanzania’s DHIS2 to evaluate the association between the presence of different types of natural resource extraction projects and disease incidence at the district level.
2. Materials and Methods
2.1. Study Setting
Tanzania has an estimated total population of 57 million people [36] and ranks 163 out of 189 countries and territories with a human development index value of 0.529 [37]. Tanzania has a decentralized health system with administrative units in the mainland area extending to 26 regions, 184 districts and municipal councils, and 8941 health facilities (including both private and public health facilities). According to the Institute of Health Metrics’ (IHME) Global Burden of Diseases estimates, the top three Disability Adjusted Life Years (DALYs) per 100,000 population in Tanzania between 2015 and 2019 were consistently shown as (1) neonatal disorders, (2) lower respiratory infections, and (3) HIV/AIDS [38].
Tanzania has a long history of resource extraction activities [39] and was one of the earliest DHIS2 implementers after the platform was developed in 2007 [40,41].
2.2. Study Design
This is a multi-year cross-sectional study that aims to assess the associations between the presence of district-level commodity extraction and disease diagnoses reported in Tanzania’s DHIS2.
2.3. Data
Disease diagnoses data come from the DHIS2 outpatient department (OPD) dataset indicators and one additional indicator (i.e., total clients tested and found positive for HIV) from the HIV testing and counselling dataset. As part of national HMIS, disease diagnoses made during health facility visits are captured and summarized in HMIS books, and summary information is entered into the DHIS2. We extracted annual aggregated data at the district level covering the period from 2015 to 2019. The data contain counts of disease diagnoses from health facility visits (both public and private). We excluded laboratories, maternity homes, and all facilities that do not provide general OPD services. We excluded the region of Dar-es-Salaam (with 5 administrative districts) due to the high density of population and health facilities and the absence of large-scale resource extraction projects. We merged data from the Ifakara town district and Kilombero District to accommodate available shapefiles in the geographical information system (GIS), whereby Ifakara town District was formally part of Kilombero District until 2016. Our final dataset contained a total of 178 districts.
Data on natural resource extraction activities were accessed via the mineral occurrence map of Tanzania [42], which was based on the Geological Survey of Tanzania (GST) conducted in 2015 [43]. The GST lists a total of 480 resource extraction projects with location coordinates and commodity types. In this list, 42% of the projects are marked prospective, 20% active, and 38% inactive. We restricted our analysis to natural resource extraction projects that were classified as active in the GST as of 2015 (at the beginning of our sample period).
2.4. Variables
2.4.1. Exposure Variables
The primary exposure variable of interest was the presence of a given commodity extraction in the district. We considered three types of commodity extraction: (1) construction materials, (2) gemstone, and (3) metals. As shown in Figure 1, most districts contain only one type of extraction project; multiple types of extraction projects were found in only seven districts. Given that coal was identified in only one district and hydrocarbons are mostly located offshore, these two groups were excluded from our analysis. A complete list of the specific commodities extracted is available in Appendix A (Table A1).
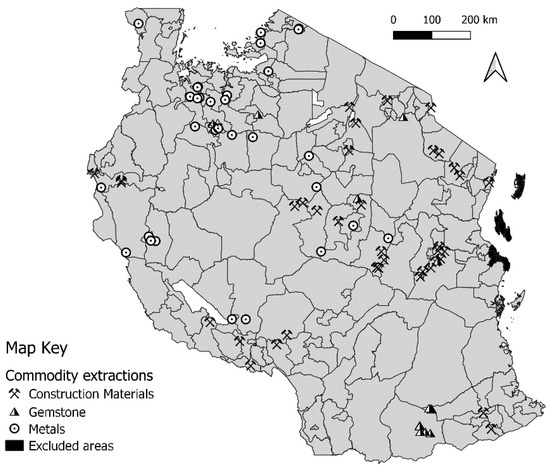
Figure 1.
Location of selected commodity extraction projects in Tanzania.
2.4.2. Outcome variables
We selected and grouped disease indicators based on the environmental health areas (EHA) framework defined in the HIA guidelines developed by the International Finance Corporation (IFC) [44]. The EHA framework provides a conceptual linkage between resource extraction activities and potential community-level impacts, incorporating a variety of biomedical and key social determinants of health [45]. For this study, we divided all reported health programs in the DHIS2 into disease groups based on the EHA framework. These groups, as well as the OPD indicators falling into each group, are summarized in Table 1.

Table 1.
List of disease groups and included outpatient department (OPD) indicators from DHIS2.
2.5. Statistical Analysis
To assess the association between the presence of commodity extraction projects and disease incidence, we used Poisson regression models controlling for period (in years), population, region fixed effects, and number of health facilities by time in the district. We assumed all commodity extraction projects to remain active over the full sample period. We employed cluster-robust standard errors to correct for residual correlation at the district level over time as well as over dispersion. We report incidence rate ratios (IRR) and corresponding 95% confidence intervals (CI) from the final models. All analyses were implemented using the STATA 15.0 statistical software package [46].
2.6. Ethical Considerations
This study obtained ethical approval from Ifakara Health Institute Review Board and the National Institute for Medical Research (NIMR) in Tanzania; the Ethics Committee of Northwestern and Central Switzerland (Ethikkommission Nordwest- und Zentralschweiz, EKNZ); and the institutional review board of the Swiss Tropical and Public Health Institute (Swiss TPH) in Switzerland.
3. Results
Participants: Overall Characteristics
A summary overview of the number and type of health facilities and commodity extraction projects in districts in Tanzania is shown in Table 2. On average, a district contained 1 hospital, 5 health centers, 36 dispensaries, and 1 health clinic. A total of 2 districts were exposed to all 3 types of commodity extraction, 5 districts were exposed to 2 types of commodity extraction, and 38 districts exposed to only 1 type of commodity extraction.
Table 2.
Overview of the number and type of health facilities and commodity extraction projects per district in Tanzania.
Extraction of construction materials occurred in 14% (N = 25) of all districts, metals in 12% (N = 22), and gemstone in 4% (N = 7). A total of 1% (N = 2) of the districts had all of the three types of commodity extraction, and 4% (N = 7) had at least two types of commodity extractions. A total of 45 districts (25%) were exposed to at least one type of commodity extraction. The distribution of health facilities by type of extractive activity is similar across the three types of commodity extraction (Table A2 in the Appendix A).
Table 3 summarizes the annual number of disease diagnoses per 100,000 inhabitants for different groups of diseases. Out of the main disease categories analyzed, the most common were respiratory infections and malaria, with an average of 52,704 and 33,981 cases across the five years, respectively. The least commonly diagnosed health problems were cancer and tuberculosis, with an average of 127 and 266 cases per year, respectively.
Table 3.
Number of disease diagnoses per 100,000 population by year.
Table 4 shows the association between the type of commodity extraction and disease groups. In the fully adjusted models, we found that the presence of construction material extraction was associated with an increased incidence of chronic diseases (IRR = 1.4795% CI = 1.15–1.87). The presence of metals extraction was associated with a reduced incidence of chronic diseases (0.61, 0.47–0.80), mental health disorders (0.66, 0.47–0.92), undernutrition (0.69, 0.55–0.88), parasitic infections (0.84, 0.72–0.98), sexually transmitted diseases (0.85, 0.74–0.97), and diarrhea diseases (0.88, 0.77–0.10). No association was found between gemstone extraction and any of the main disease categories. The outputs of the crude model are available in Table A3.
Table 4.
Relationship (adjusted model) between disease groups and type of commodity extraction.
Table 5 shows the results for disaggregated disease categories. Extraction of construction materials was associated with an increased incidence of hypertension (IRR = 1.49, CI: 1.11–2.01), neoplasms/cancer diseases (IRR = 1.46, CI: 1.07–1.99), bronchitis asthma (1.38, 1.14–1.66), and other cardiovascular diseases (1.72, 1.27–2.32). Gemstone extraction was associated with a significant increase in the incidence of malaria (blood slide microscopy method) (2.08, CI: 1.06–4.07), non-severe pneumonia (1.40, 1.04–1.87), diarrhea with some dehydration (IRR: 1.38, 1.11–1.73), and severe pneumonia (1.25, 1.01–1.54). Protective effects were found for metal extraction projects in the majority of disease-specific indicators.
Table 5.
Relationship (adjusted model) between disease-specific indicators and type of commodity extraction.
4. Discussion
In this paper, we evaluated the relationship between the district-level presence of natural resource extraction activities and the disease-specific patient volumes reported across all health facilities in Tanzania in a given district and year.
Our results show that the districts’ health infrastructure across the three types of commodity extraction is relatively the same (Table A3). In addition, the presence of commodity extraction projects is associated with significant changes in the incidence of diseases reported in the routine national HMIS of Tanzania. The changes in disease incidence appear to differ substantially by the type of commodity extracted; in districts where metal resources are extracted (most typically Gold in Tanzania), we observed a significant decrease in the incidence of chronic diseases (−39%), mental health disorders (−34%), undernutrition (−31%), parasitic infections (−26%), sexually transmitted diseases (−15%), and diarrheal diseases (−13%). On the other hand, the presence of construction material extractions was associated with a significant increase in the incidence of chronic diseases (+47%), including hypertension (+49%), neoplasms/cancer (+46%), bronchitis asthma (+38%), and other cardiovascular diseases (+72%). Gemstone extraction was not associated with any of the aggregated disease categories but showed positive associations with severe and non-severe pneumonia (+40% and +25%, respectively), as well as diarrhea with dehydration (+38%).
The consistent inverse association between the metal extraction industry and disease incidence was rather striking and could be due to several factors. The observed decreased incidence of chronic diseases can partially be explained by the in-migration of young and healthy mining workers and other job seekers [47,48,49], who are at lower risk for chronic diseases, such as hypertension and diabetes mellitus [50]. In addition, the majority of large-scale metal industries in Tanzania are led by transnational corporations [51], which are more likely to adhere to international environmental and social standards (e.g., Performance Standards of the International Finance Corporation (IFC) [52]) and recommended industry practices (e.g., International Council on Mining and Metals (ICMM) [53] and Extractive Industries Transparency Initiative (EITI) [54]). Hence, it seems plausible that metal extraction projects are, on average, more able to support local health systems and community-level interventions [55] or socio-economic development programs [56]. This may also explain why, in contrast to previous studies that reported elevated levels of sexually transmitted diseases in regions where metals are extracted [15,18,57,58], our results show that districts that are exposed to metal extractions activities generally have lower incidences of sexually transmitted diseases, including HIV/AIDS, even though these differences were not statistically significant.
It is also important to highlight that our study covered the period 2015–2019, which followed two major national-level government interventions. The first intervention was the Tanzania Mineral Policy 2009 Revision, which intended to increase the mineral sector contribution to income generation [59], and the second was the re-enactment of the Mining Act 2010, which requires mining companies to have a plan to increase Tanzania’s citizens’ participation in mining activities through employment and expatriate succession plans, as well as a plan for procurement of goods and services through the available local market in the United Republic of Tanzania [60]. It is likely that these measures had a particularly positive effect on the districts with the presence of metal extractions activities, which are, in general, larger operations than construction and gemstone commodity extraction projects.
In contrast to metal extraction, increased levels of disease incidence were observed for districts with construction material or gemstone extraction activities. Extraction of construction materials covers commodities such as cement, silicate, carbonate hard rocks, decorative stones (i.e., dolomite and limestone), and industrial minerals (i.e., gypsum, clay, halite, phosphate, and mica). The observed increase in the incidence of chronic diseases appears consistent with the risk factors for such projects described by IFC, namely, high exposures to dust, vibration, noise, and unhealthy lifestyle (related to cigarette smoking and excessive alcohol intake) [61]. Studies have also shown that exposure to particulate matter (PM) from construction dust can significantly influence the appearance of diseases such as cancer and cardiovascular and respiratory diseases [62,63]. Studies from the construction and building materials literature report that there is a growing demand for construction material commodities, and they equally draw attention to the environmental and health effects this demand imposes on the livelihoods of affected communities [64,65,66]. In our study sample, 40% of the commodities extraction projects were categorized as construction materials, highlighting the need to further scrutinize this sector in terms of environmental and social responsibility, including the mitigation of potential adverse health impacts.
Strength and Limitations
To our knowledge, this is the first large-scale study of the relationship between mining and disease incidence in Tanzania using the complete national HMIS database. The dataset covers—by definition—the entire country and allowed us to analyze a range of different mines at the same time. Having five years of data also allowed us to reduce the risk of specific results being driven by misreporting in a given month or year. The study also has several limitations. First, DHIS2 and routine HMIS data have known data quality issues [67], including concerns regarding completeness, consistency, coverage, and disease coding [68,69,70,71]. In our analysis, we did not account for potentially different data quality across districts. If such differences in quality exist, they would only bias our results if reporting was systematically correlated with the presence of mines. This is possible in principle if mines directly contribute to the health system capacity and could potentially bias results against mines. We also did not distinguish between missing data and the true zero values in our analysis, which means that the reported case numbers may underestimate the true burden of disease and patient numbers. Due to the unavailability of good data, we did not account for district per capita income, nor for the number of job seekers who migrated into mining areas. The OPD diagnoses consist of both clinical and non-clinical indicators. Non-clinical indicators can be influenced by physician’s opinion and are subject to reporting bias. As long as these biases are not correlated with the presence of mines, this should not introduce any systematic bias to our analysis. In addition, we used district boundaries to link mining operations to patient volumes. Even though districts are relatively large, it is possible that some of the mines—particularly when located near district boundaries—also affect patient volumes in neighboring districts. This exposure misclassification would likely result in less precise estimates but could also lead to an underestimation of the true causal effects if there are systematic spillovers into districts considered unexposed in our analysis. Lastly, OPD indicators represent counts of people who sought care at health facilities and do not represent actual case numbers in the population.
5. Conclusions
The results of this study suggest that the health impact of mining operations may not only depend on the specific health outcome but also on the types of mines. While metal extraction projects display consistent protective effects against a range of disease indicators, extraction of construction materials and gemstones is associated with increased incidence of chronic and diarrheal diseases, respectively. More research is needed to understand the underlying factors of the differences observed across the types of commodity extracted.
Author Contributions
Conceptualization: I.L., G.W.L., G.F. and M.S.W.; methodology: I.L., G.L., A.F., G.F. and M.S.W.; formal analysis: I.L.; writing—original draft preparation: I.L. and M.S.W.; writing—review and editing: all. All authors have read and agreed to the published version of the manuscript.
Funding
This research received funding from the Swiss Programme for Research on Global Issues for Development (r4d Programme, www.r4d.ch (accessed on 10 February 2021)), which is a joint funding initiative of the Swiss Agency for Development and Cooperation (SDC) and the Swiss National Science Foundation (SNSF) (grant number 169461).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of the Ifakara Health Institute (No: 32-2018, Date: 28 September 2018), Tanzania National Institute for Medical Research — NIMR (ID: NIMR/HQ/R.8a/Vol.IX/2969, Date: 3 December 2018) and the Ethics Committee of the Northwest and Central Switzerland — EKNZ (EKNZ Req-2018-00386, Date: 23 May 2018).
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the Ministry of Health Community Development, Gender, Elderly and Children (MoHCDGEC). The data are not publicly available due to local restrictions.
Acknowledgments
The authors thank the Tanzanian Ministry of Health, Community Development, Gender, Elderly and Children who allowed the use of DHIS2 data from Tanzania.
Conflicts of Interest
The authors declare that they have no conflict of interest. The funders had no role in the design of the study, data collection, analyzes and findings´ interpretation, the writing of the manuscript, or in the decision to publish the results.
Appendix A
Table A1.
List of commodities extracted in Tanzania.
Table A1.
List of commodities extracted in Tanzania.
| Commodity Groups | Commodity Subgroup | Example |
|---|---|---|
| Construction materials | Construction raw materials | Pozzolana (cement), silicate hard rock, carbonate hard rock |
| Decorative stones | Dolomite, limestone, quartzite, travertine | |
| Industrial minerals | Gypsum, halite, kaolin and kaolin clay, clay minerals, mica, phosphate, sylvinite | |
| Gemstone | Gemstone | Chrysoprase, diamond, sapphire, tanzanite |
| Metals | Precious metals | Gold |
| Rate metals | Tin | |
| Base metals | Copper | |
| Coal 1 | Coal | Coal |
| Hydrocarbons 1 | Hydrocarbons | Natural gas |
1 excluded in the analysis due to limited exposure.
Table A2.
Distribution of health facilities by type of commodity extraction.
Table A2.
Distribution of health facilities by type of commodity extraction.
| Facility Type | Type of Commodity Extraction | ||
|---|---|---|---|
| Construction Material | Gemstone | Metals | |
| Hospital | 28% | 27% | 26% |
| Health centers | 32% | 32% | 33% |
| Dispensaries | 32% | 32% | 33% |
| Clinics | 9% | 9% | 8% |
Table A3.
Crude model of relationship between disease groups and type of commodity extraction.
Table A3.
Crude model of relationship between disease groups and type of commodity extraction.
| Type of Commodity Extraction | ||||||
|---|---|---|---|---|---|---|
| Disease Groups | Construction Materials | Gemstone | Metals | |||
| IRR | CI | IRR | CI | IRR | CI | |
| Chronic diseases | 1.472 ** | 1.023–2.118 | 0.669 * | 0.417–1.073 | 0.632 ** | 0.425–0.940 |
| Respiratory infections | 1.012 | 0.891–1.148 | 1.050 | 0.870–1.267 | 0.898 * | 0.802–1.006 |
| Tuberculosis (TB) | 1.075 | 0.757–1.528 | 0.890 | 0.532–1.491 | 0.797 | 0.543–1.171 |
| Diarrhea | 0.932 | 0.804–1.081 | 1.180 | 0.928–1.499 | 0.875 ** | 0.770–0.994 |
| Undernutrition | 0.860 | 0.661–1.119 | 0.880 | 0.547–1.415 | 0.678 *** | 0.529–0.869 |
| Malaria | 0.927 | 0.641–1.341 | 1.235 | 0.872–1.750 | 1.073 | 0.840–1.370 |
| Parasitic diseases | 1.025 | 0.865–1.215 | 0.961 | 0.710–1.300 | 0.818 ** | 0.695–0.962 |
| Sexually transmitted diseases | 1.103 | 0.852–1.428 | 0.850 | 0.627–1.153 | 0.848 | 0.697–1.032 |
| Road traffic accidents | 1.112 | 0.843–1.465 | 0.953 | 0.608–1.494 | 0.939 | 0.703–1.255 |
| Mental health | 0.927 | 0.633–1.357 | 1.165 | 0.486–2.789 | 0.587 *** | 0.404–0.852 |
Note: estimates are adjusted for cluster robust; *** p < 0.01, ** p < 0.05, * p < 0.1.
References
- Watson, A.P.; Down, C.G.; Stocks, J. Environmental Impact of Mining. Ecology 1978, 59, 203. [Google Scholar] [CrossRef]
- Akabzaa, T.; Darimani, A. Impact of Mining Sector Investment in Ghana: A Study of the Tarkwa Mining Region; SAPRI: Accra, Ghana, 2001. [Google Scholar]
- Steinberg, J. Mines, Communities, and States: The Local Politics of Natural Resource Extraction in Africa; Cambridge University Press: Cambridge, UK, 2019. [Google Scholar]
- Winkler, M.S.; Divall, M.J.; Krieger, G.R.; Schmidlin, S.; Magassouba, M.L.; Knoblauch, A.M.; Singer, B.H.; Utzinger, J. Assessing health impacts in complex eco-epidemiological settings in the humid tropics: Modular baseline health surveys. Environ. Impact Assess. Rev. 2012, 33, 15–22. [Google Scholar] [CrossRef]
- Dietler, D.; Farnham, A.; De Hoogh, K.; Winkler, M.S. Quantification of Annual Settlement Growth in Rural Mining Areas Using Machine Learning. Remote Sens. 2020, 12, 235. [Google Scholar] [CrossRef]
- Cust, J.; Poelhekke, S. The Local Economic Impacts of Natural Resource Extraction. Annu. Rev. Resour. Econ. 2015, 7, 251–268. [Google Scholar] [CrossRef]
- Jäger, P.F. Flows of oil, flows of people: Resource-extraction industry, labour market and migration in western Kazakhstan. Cent. Asian Surv. 2014, 33, 500–516. [Google Scholar] [CrossRef]
- Leuenberger, A.; Farnham, A.; Azevedo, S.; Cossa, H.; Dietler, D.; Nimako, B.; Adongo, P.B.; Merten, S.; Utzinger, J.; Winkler, M.S. Health impact assessment and health equity in sub-Saharan Africa: A scoping review. Environ. Impact Assess. Rev. 2019, 79, 106288. [Google Scholar] [CrossRef]
- Fernández-Navarro, P.; García-Pérez, J.; Ramis, R.; Boldo, E.; Lopez-Abente, G. Proximity to mining industry and cancer mortality. Sci. Total Environ. 2012, 435-436, 66–73. [Google Scholar] [CrossRef]
- Kitula, A. The environmental and socio-economic impacts of mining on local livelihoods in Tanzania: A case study of Geita District. J. Clean. Prod. 2006, 14, 405–414. [Google Scholar] [CrossRef]
- Leuenberger, A.K.F.; Lyatuu, I.; Kengiad, J.T.; Farnham, A.; Winkler, M.S.; Merten, S. Health impacts of industrial gold mining on local communities in Tanzania: A gender-focused qualitative study. Impact Assess. Proj. Apprais. 2021, 39, 118–126. [Google Scholar] [CrossRef]
- Winkler, M.S.; Adongo, P.B.; Binka, F.; Brugger, F.; Diagbouga, S.; Macete, E.; Munguambe, K.; Okumu, F. Health impact assessment for promoting sustainable development: The HIA4SD project. Impact Assess. Proj. Apprais. 2019, 38, 225–232. [Google Scholar] [CrossRef]
- Ogola, J.S.; Mitullah, W.V.; Omulo, M.A. Impact of Gold mining on the Environment and Human Health: A Case Study in the Migori Gold Belt, Kenya. Environ. Geochem. Health 2002, 24, 141–157. [Google Scholar] [CrossRef]
- Nkosi, V.; Wichmann, J.; Voyi, K. Chronic respiratory disease among the elderly in South Africa: Any association with proximity to mine dumps? Environ. Health 2015, 14, 33. [Google Scholar] [CrossRef]
- de Soysa, I.; Gizelis, T.-I. The natural resource curse and the spread of HIV/AIDS, 1990–2008. Soc. Sci. Med. 2013, 77, 90–96. [Google Scholar] [CrossRef]
- Long, R.N.; Renne, E.P.; Basu, N. Understanding the Social Context of the ASGM Sector in Ghana: A Qualitative Description of the Demographic, Health, and Nutritional Characteristics of a Small-Scale Gold Mining Community in Ghana. Int. J. Environ. Res. Public Health 2015, 12, 12679–12696. [Google Scholar] [CrossRef]
- Winkler, M.S.; Divall, M.J.; Krieger, G.R.; Balge, M.Z.; Singer, B.H.; Utzinger, J. Assessing health impacts in complex eco-epidemiological settings in the humid tropics: The centrality of scoping. Environ. Impact Assess. Rev. 2011, 31, 310–319. [Google Scholar] [CrossRef]
- Eisler, R. Health Risks of Gold Miners: A Synoptic Review. Environ. Geochem. Health 2003, 25, 325–345. [Google Scholar] [CrossRef] [PubMed]
- Knoblauch, A.M.; Winkler, M.S.; Archer, C.; Divall, M.J.; Owuor, M.; Yapo, R.M.; Yao, P.; Utzinger, J. The epidemiology of malaria and anaemia in the Bonikro mining area, central Côte d’Ivoire. Malar. J. 2014, 13, 194. [Google Scholar] [CrossRef] [PubMed]
- Hossain, D.; Gorman, D.; Chapelle, B.; Mann, W.; Saal, R.; Penton, G. Impact of the mining industry on the mental health of landholders and rural communities in southwest Queensland. Australas. Psychiatry 2013, 21, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Shandro, J.; Jokinen, L.; Stockwell, A.; Mazzei, F.; Winkler, M.S. Risks and Impacts to First Nation Health and the Mount Polley Mine Tailings Dam Failure. Int. J. Indig. Health 2017, 12, 84–102. [Google Scholar] [CrossRef]
- Anaf, J.; Baum, F.; Fisher, M.; London, L. The health impacts of extractive industry transnational corporations: A study of Rio Tinto in Australia and Southern Africa. Glob. Health 2019, 15, 13. [Google Scholar] [CrossRef] [PubMed]
- Leuenberger, A.; Dietler, D.; Lyatuu, I.; Farnham, A.; Kihwele, F.; Brugger, F.; Winkler, M.S. Water infrastructure and health in mining settings: A mixed-methods geospatial visualization. Geospat. Health 2021. In Press. [Google Scholar] [CrossRef] [PubMed]
- Knoblauch, A.M.; Divall, M.J.; Owuor, M.; Nduna, K.; Ng’Uni, H.; Musunka, G.; Pascall, A.; Utzinger, J.; Winkler, M.S. Experience and lessons from health impact assessment guiding prevention and control of HIV/AIDS in a copper mine project, northwestern Zambia. Infect. Dis. Poverty 2017, 6, 1–11. [Google Scholar] [CrossRef]
- Knoblauch, A.M.; Farnham, A.; Zabré, H.R.; Owuor, M.; Archer, C.; Nduna, K.; Chisanga, M.; Zulu, L.; Musunka, G.; Utzinger, J.; et al. Community Health Impacts of the Trident Copper Mine Project in Northwestern Zambia: Results from Repeated Cross-Sectional Surveys. Int. J. Environ. Res. Public Health 2020, 17, 3633. [Google Scholar] [CrossRef] [PubMed]
- Thondoo, M.; Gupta, J. Health impact assessment legislation in developing countries: A path to sustainable development? Rev. Eur. Comp. Int. Environ. Law 2020, 30, 107–117. [Google Scholar] [CrossRef]
- Winkler, M.S.; Krieger, G.R.; Divall, M.J.; Cissé, G.; Wielga, M.; Singer, B.H.; Tanner, M.; Utzinger, J. Untapped potential of health impact assessment. Bull. World Health Organ. 2013, 91, 298–305. [Google Scholar] [CrossRef]
- Winkler, M.S.; Furu, P.; Viliani, F.; Cave, B.; Divall, M.; Ramesh, G.; Harris-Roxas, B.; Knoblauch, A.M. Current Global Health Impact Assessment Practice. Int. J. Environ. Res. Public Health 2020, 17, 2988. [Google Scholar] [CrossRef]
- Brisbois, B.W.; Reschny, J.; Fyfe, T.M.; Harder, H.G.; Parkes, M.W.; Allison, S.; Buse, C.G.; Fumerton, R.; Oke, B. Mapping research on resource extraction and health: A scoping review. Extr. Ind. Soc. 2019, 6, 250–259. [Google Scholar] [CrossRef]
- Thondoo, M.; Rojas-Rueda, D.; Gupta, J.; De Vries, D.H.; Nieuwenhuijsen, M.J. Systematic Literature Review of Health Impact Assessments in Low and Middle-Income Countries. Int. J. Environ. Res. Public Health 2019, 16, 2018. [Google Scholar] [CrossRef]
- DHIS2. District Health Informatoin System—Overview. Available online: https://dhis2.org/overview/ (accessed on 22 April 2021).
- Braa, J.; Sahay, S. The DHIS2 open source software platform: Evolution over time and space. Global Health Inf. 2017, 451. [Google Scholar]
- Plotkin, M.; Bishanga, D.; Kidanto, H.; Jennings, M.C.; Ricca, J.; Mwanamsangu, A.; Tibaijuka, G.; Lemwayi, R.; Ngereza, B.; Drake, M.; et al. Tracking facility-based perinatal deaths in Tanzania: Results from an indicator validation assessment. PLoS ONE 2018, 13, e0201238. [Google Scholar] [CrossRef]
- Bhattacharya, A.A.; Umar, N.; Audu, A.; Felix, H.; Allen, E.; Schellenberg, J.R.M.; Marchant, T. Quality of routine facility data for monitoring priority maternal and newborn indicators in DHIS2: A case study from Gombe State, Nigeria. PLoS ONE 2019, 14, e0211265. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, J.A.; Qiu, M.; Paina, L.; Colantuoni, E.; Mukuru, M.; Ssengooba, F.; Bennett, S. The impact of PEPFAR transition on HIV service delivery at health facilities in Uganda. PLoS ONE 2019, 14, e0223426. [Google Scholar] [CrossRef] [PubMed]
- NBS. Tanzania National Bureau of Statistics. Available online: https://www.nbs.go.tz/index.php/en/census-surveys/population-and-housing-census (accessed on 22 April 2021).
- UNDP. Global Human Development Indicators. Available online: http://hdr.undp.org/en/countries/profiles/TZA (accessed on 22 April 2021).
- Institute for Health Metrics and Evaluation (IHME). GBD Compare. Available online: https://vizhub.healthdata.org/gbd-compare/ (accessed on 22 April 2021).
- Pedersen, R.H.; Jacob, T.; Maganga, F.; Kweka, O. Rights to Land and Extractive Resources in Tanzania (1/2): The History; Danish Institute for International Studies: Copenhagen, Danmark, 2016. [Google Scholar]
- Lungo, J.H. The reliability and usability of district health information software: Case studies from Tanzania. Tanzan. J. Health Res. 2008, 10, 39–45. [Google Scholar] [CrossRef] [PubMed]
- DHIS2. Tanzania: Integrated Health Information Architecture. Available online: https://docs.dhis2.org/2.34/en/user_stories_book/tanzania-integrated-health-information-architecture_B.html (accessed on 22 April 2021).
- Geological Survey of Tanzania (GST). Tanzania Geological and Mineral Information System. Available online: https://www.gmis-tanzania.com/ (accessed on 12 April 2020).
- Leger, C.; Barth, A.; Falk, D.; Mruma, A.; Magigita, M.; Boniface, N.; Manya, S.; Kagya, M.; Stanek, K. Explanatory Notes for the Minerogenic Map of Tanzania; Geological Survey of Tanzania (GST): Dar-es-Salaam, United Republic of Tanzania, 2015; Available online: http://hdl.handle.net/123456789/3985 (accessed on 10 February 2021).
- International Finance Corporation (IFC). Introduction to Health Impact Assessment. Available online: https://www.ifc.org/wps/wcm/connect/topics_ext_content/ifc_external_corporate_site/sustainability-at-ifc/publications/publications_handbook_healthimpactassessment__wci__1319578475704 (accessed on 22 April 2021).
- Winkler, M.S.; Divall, M.J.; Krieger, G.R.; Balge, M.Z.; Singer, B.H.; Utzinger, J. Assessing health impacts in complex eco-epidemiological settings in the humid tropics: Advancing tools and methods. Environ. Impact Assess. Rev. 2010, 30, 52–61. [Google Scholar] [CrossRef]
- STATA Corp. STATA IC 15.0; STATA Corp.: College Station, TX, USA, 2017. [Google Scholar]
- Fennelly, K. The “healthy migrant” effect. Minn. Med. 2007, 90, 51–53. [Google Scholar]
- McDonald, J.T.; Kennedy, S. Insights into the ‘healthy immigrant effect’: Health status and health service use of immi-grants to Canada. Soc. Sci. Med. 2004, 59, 1613–1627. [Google Scholar] [CrossRef]
- Stedman, R.C.; Jacquet, J.B.; Filteau, M.R.; Willits, F.K.; Brasier, K.J.; McLaughlin, D.K. Environmental Reviews and Case Studies: Marcellus Shale Gas Development and New Boomtown Research: Views of New York and Pennsylvania Residents. Environ. Pract. 2012, 14, 382–393. [Google Scholar] [CrossRef]
- Booth, F.W.; Roberts, C.K.; Laye, M. Lack of Exercise Is a Major Cause of Chronic Diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar] [CrossRef]
- Tumemadini. Mining Commission Annual Report 2018/2019; The United Republic of Tanzania Ministry of Minerals: Dar-es-Salaam, United Republic of Tanzania, 2019; p. 39. [Google Scholar]
- International Finance Corporation (IFC). Performance Standards on Environmental and Social Sustainability; World Bank Group: Washington, DC, USA, 2012. [Google Scholar]
- The International Council on Mining and Metals (ICMM). Mining Principles. Available online: https://www.icmm.com/ (accessed on 14 March 2021).
- The Extractive Industries Transparency Initiative (EITI). Guide to Implementing the EITI Standard. Available online: https://eiti.org/ (accessed on 15 March 2021).
- Calain, P. Oil for health in sub-Saharan Africa: Health systems in a ‘resource curse’ environment. Glob. Health 2008, 4, 10. [Google Scholar] [CrossRef]
- Fleming, D.A.; Measham, T.G. Disentangling the Natural Resources Curse: National and Regional Socioeconomic Impacts of Resource Windfalls. In Proceedings of the 2013 Annual Meeting, Washington, DC, USA, 4–6 August 2013. [Google Scholar]
- Corno, L.; De Walque, D. Mines, Migration and HIV/AIDS in Southern Africa. J. Afr. Econ. 2012, 21, 465–498. [Google Scholar] [CrossRef]
- Clift, S.; Anemona, A.; Watson-Jones, D.; Kanga, Z.; Ndeki, L.; Changalucha, J.; Gavyole, A.; Ross, D. Variations of HIV and STI prevalences within communities neighbouring new goldmines in Tanzania: Importance for intervention design. Sex. Transm. Infect. 2003, 79, 307–312. [Google Scholar] [CrossRef]
- United Republic of Tanzania. The Mineral Policy of Tanzania 2009. Available online: https://www.tanzania.go.tz/egov_uploads/documents/0014_11032013_Mineral_Policy_of_Tanzania_2009_sw.pdf (accessed on 22 February 2021).
- United Republic of Tanzania. The Mining Act, No 14. 2010. Available online: http://parliament.go.tz/polis/uploads/bills/acts/1452071244-ActNo-14-2010.pdf (accessed on 22 February 2021).
- International Finance Corporation (IFC). Environmental, Health, and Safety Guidelines for Construction Materials Extraction; International Finance Corporation: Washington, DC, USA, 2007. [Google Scholar]
- Pope, C.A.; Burnett, R.T.; Thurston, G.D.; Thun, M.J.; Calle, E.E.; Krewski, D.; Godleski, J.J. Cardiovascular Mortality and Long-Term Exposure to Particulate Air Pollution. Circulation 2004, 109, 71–77. [Google Scholar] [CrossRef]
- Patra, A.K.; Gautam, S.; Kumar, P. Emissions and human health impact of particulate matter from surface mining operation—A review. Environ. Technol. Innov. 2016, 5, 233–249. [Google Scholar] [CrossRef]
- Allwood, J.M.; Ashby, M.F.; Gutowski, T.G.; Worrell, E. Material efficiency: A white paper. Resour. Conserv. Recycl. 2011, 55, 362–381. [Google Scholar] [CrossRef]
- Pacheco-Torgal, F.; Labrincha, J. The future of construction materials research and the seventh UN Millennium Development Goal: A few insights. Constr. Build. Mater. 2013, 40, 729–737. [Google Scholar] [CrossRef]
- Horvath, A. Construction Materials and the Environment. Annu. Rev. Environ. Resour. 2004, 29, 181–204. [Google Scholar] [CrossRef]
- Farnham, A.; Utzinger, J.; Kulinkina, A.V.; Winkler, M.S. Using district health information to monitor sustainable development. Bull. World Health Organ. 2020, 98, 69–71. [Google Scholar] [CrossRef]
- Chaulagai, C.N.; Moyo, C.M.; Koot, J.; Moyo, H.B.M.; Sambakunsi, T.C.; Khunga, F.M.; Naphini, P.D. Design and implementation of a health management information system in Malawi: Issues, innovations and results. Health Policy Plan. 2005, 20, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Gething, P.W.; Noor, A.M.; Gikandi, P.W.; Ogara, E.A.A.; Hay, S.; Nixon, M.S.; Snow, R.; Atkinson, P.M. Improving Imperfect Data from Health Management Information Systems in Africa Using Space–Time Geostatistics. PLoS Med. 2006, 3, e271. [Google Scholar] [CrossRef]
- Mate, K.S.; Bennett, B.; Mphatswe, W.; Barker, P.; Rollins, N. Challenges for Routine Health System Data Management in a Large Public Programme to Prevent Mother-to-Child HIV Transmission in South Africa. PLoS ONE 2009, 4, e5483. [Google Scholar] [CrossRef]
- Mpimbaza, A.; Chang, M.; Staedke, S.G.; Miles, M.; Kapella, B.K.; Dorsey, G.; Kigozi, R.; Nasr, S.; Rubahika, D.; Sserwanga, A.; et al. Comparison of Routine Health Management Information System Versus Enhanced Inpatient Malaria Surveillance for Estimating the Burden of Malaria Among Children Admitted to Four Hospitals in Uganda. Am. J. Trop. Med. Hyg. 2015, 92, 18–21. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).