
Quality Evaluation of Health Services Using the Kano Model in Two Hospitals in Peru


 ,
, 
Abstract
:1. Introduction
2. Theoretical Model
- (1)
- Delivering a promise: This is the central element of the model and is what makes it different to the traditional concepts of excellence in service. The organization is trustworthy, as it does what it says and does not disappoint the customer.
- (2)
- Providing a personal touch: This makes the client feel privileged, since the organization cares about the client and offers a personalized service.
- (3)
- Going the extra mile: This consists of dedicating extra effort, that is, going further and trying to anticipate the clients’ needs.
- (4)
- Dealing well with problems and queries: The organization’s ability to react to a failed service is an important element for customers.
- (1)
- Service leadership: The existence of a service leader who is in charge of motivating and helping to meet the needs of employees in their work environment is key. It is necessary to communicate a vision of service, that is, an attitude of offering quality service.
- (2)
- Service encounters: These are the employee’s interactions with customers in the so-called “moments of truth”. Thus, how customers are treated has a direct impact on their perception of the service provided and their satisfaction. Therefore, the organization must carry out practices that create positive customer perceptions of service performance. It is also necessary to give employees the power to make decisions in this area (empowerment). In this way, staff members feel more responsible, are more motivated, and are more productive, so they respond quicker to complaints or problems that the client raises.
- (3)
- Service systems: It is necessary to develop an integrated system of practices and procedures to achieve the provision of a quality service. This system must include practices for preventing and recovering from service failures and for communication with the customer.
- (4)
- Human resources management: The organization must develop training measures, as the training and reward of workers are related to improvements in the provision of customer service.
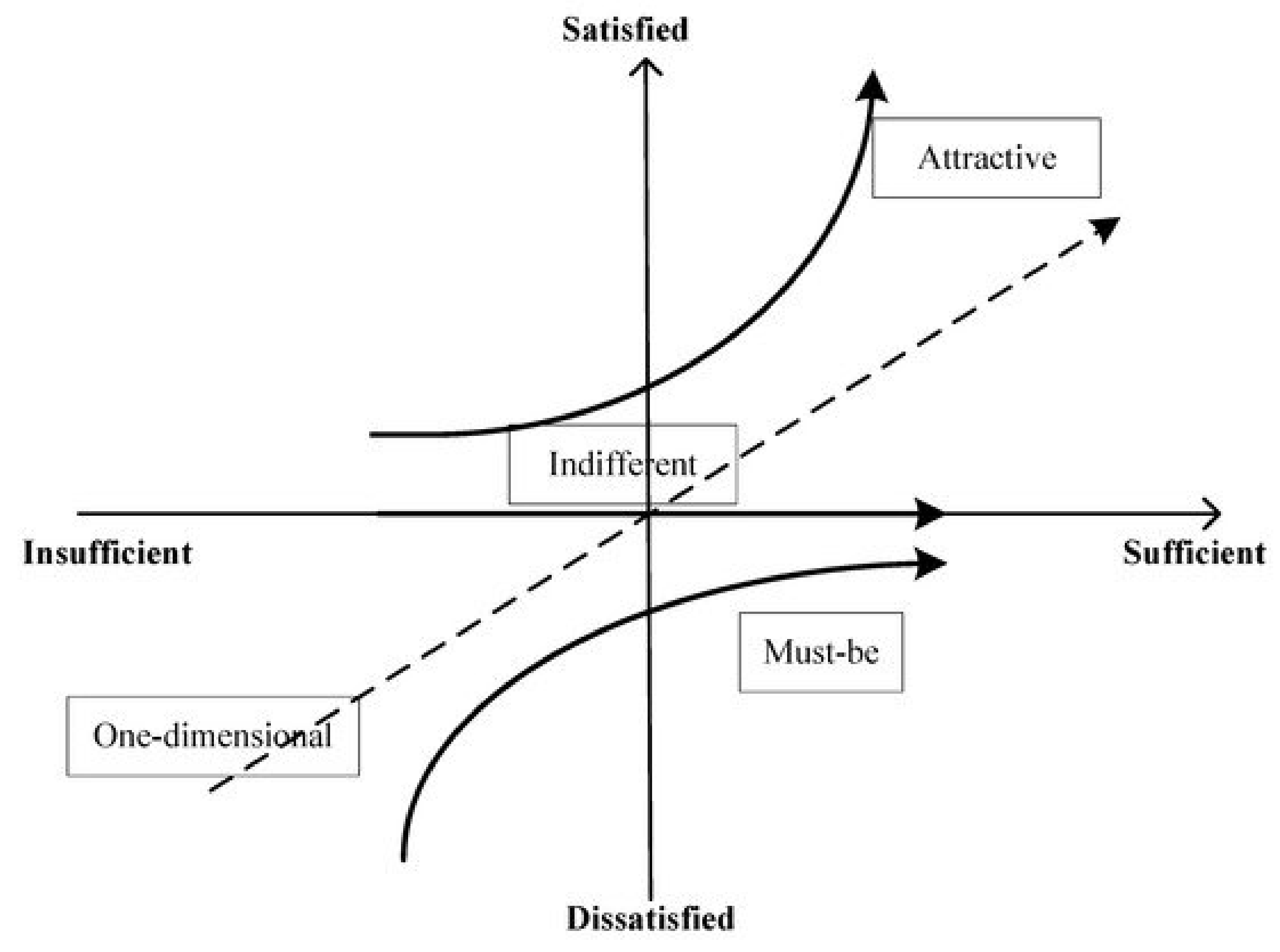
- Mandatory or “must-be” (M): This characteristic is a basic requirement, so its absence leads to extreme customer dissatisfaction. The customer takes this requirement for granted; therefore, its fulfillment does not increase their level of satisfaction. Compliance with this requirement leads to a status of “satisfied”.
- One-dimensional (O): This characteristic is a linear-type requirement; when it is met, customer satisfaction increases, but when it is not met, the level of customer satisfaction decreases, that is, their dissatisfaction increases. This characteristic is what customers expect from the proposed service; it is a performance requirement that is typically demanded by customers.
- Attractive (A): This feature has the greatest impact on the level of customer satisfaction. The client may not express or expect this feature explicitly; however, its presence increases satisfaction more than proportionally. Moreover, if not met, satisfaction does not diminish. Consequently, attractive requirements make it possible to differentiate the product/service from the competition. This feature comprises the attributes related to customer delight.
- Indifferent (I): This characteristic presents a requirement of no preference, which implies that the customer is indifferent to the characteristic.
- Reverse (R): This characteristic is one that creates customer satisfaction when absent and dissatisfaction when it occurs.
3. Materials and Methods
3.1. Participants
3.2. Instrument
3.3. Methods and Data Analysis
Kano Questionnaire Reliability
4. Results
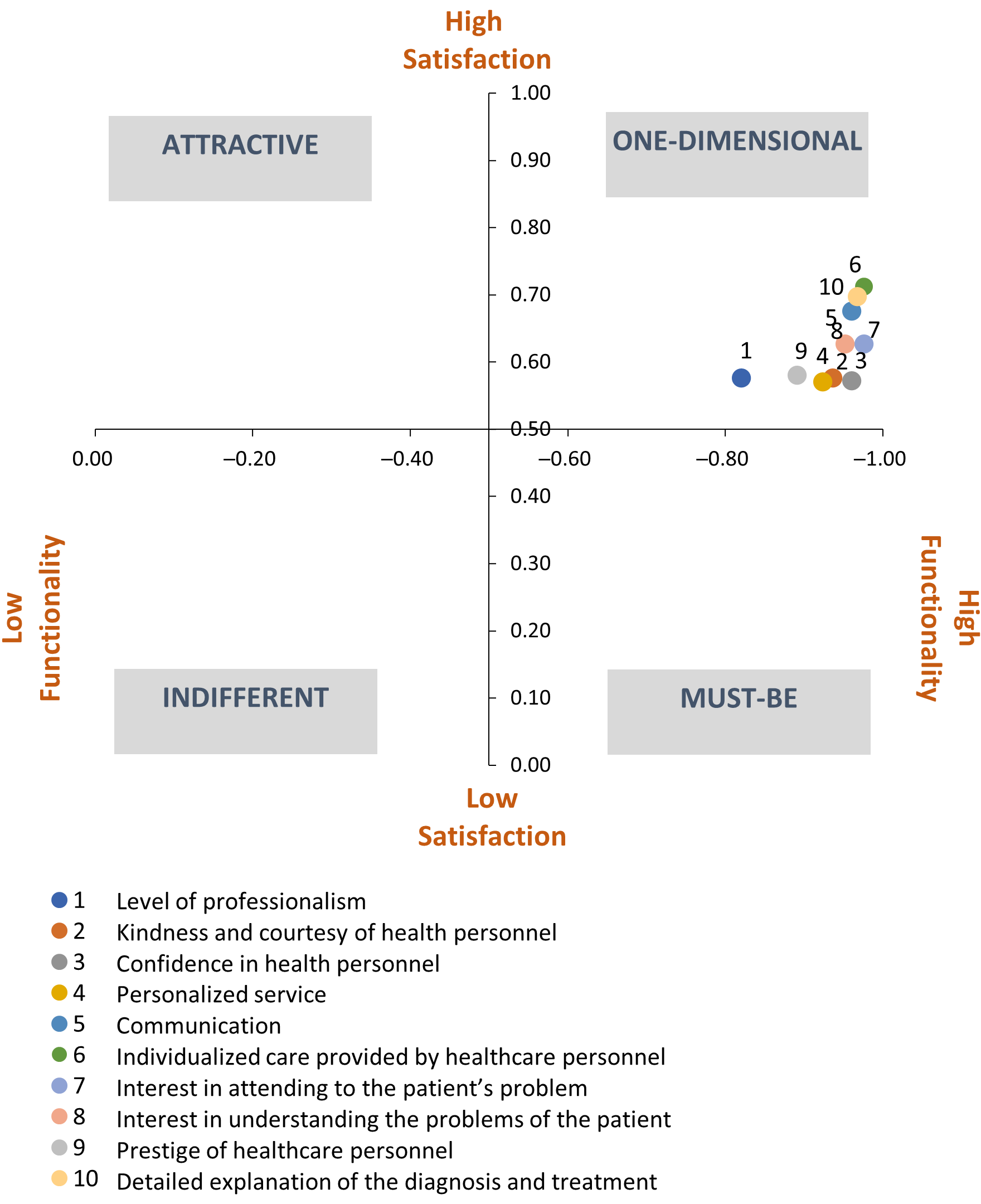
4.1. Health Personnel (PS)
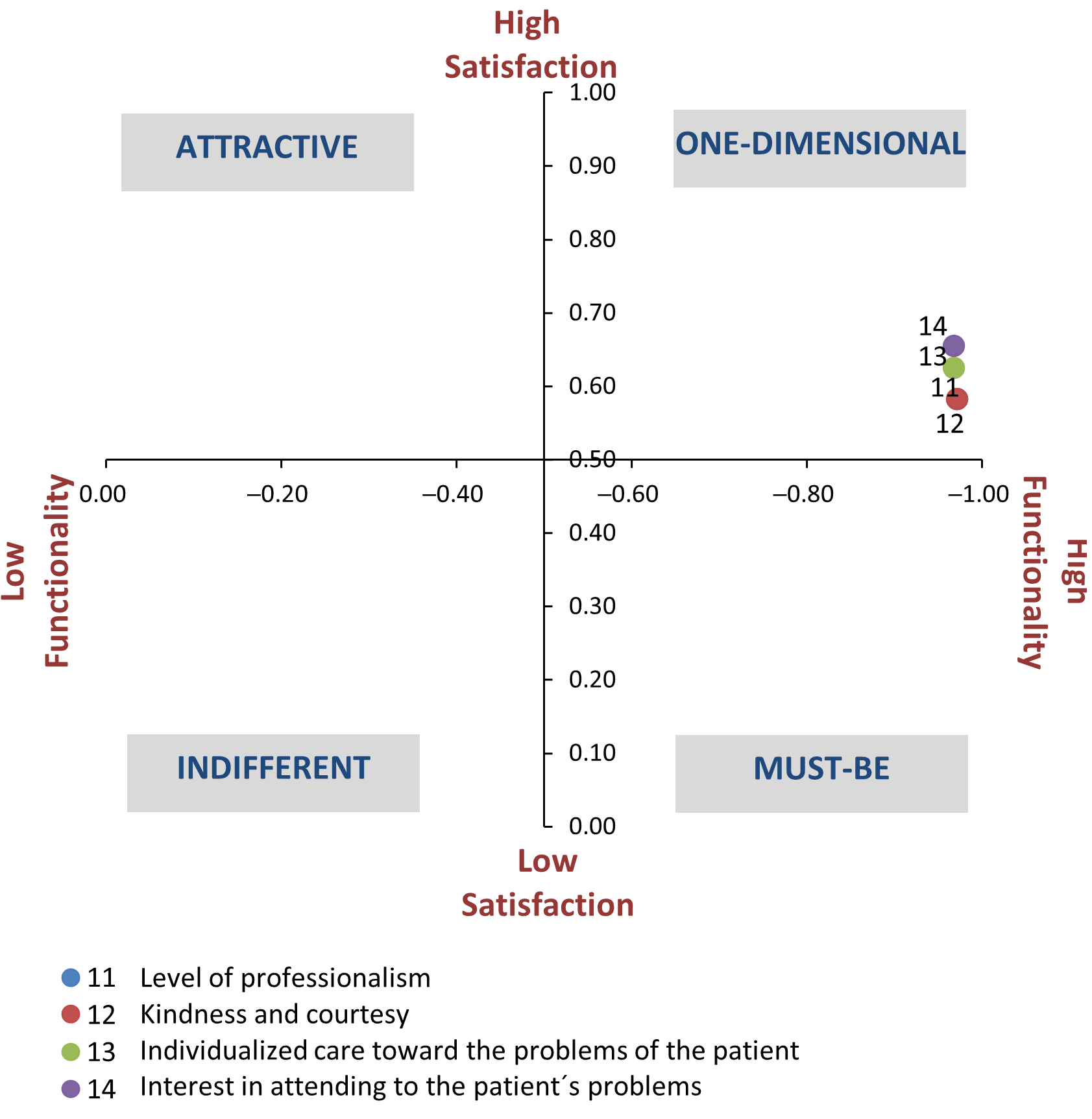
4.2. Non-Health Personnel (PNS)
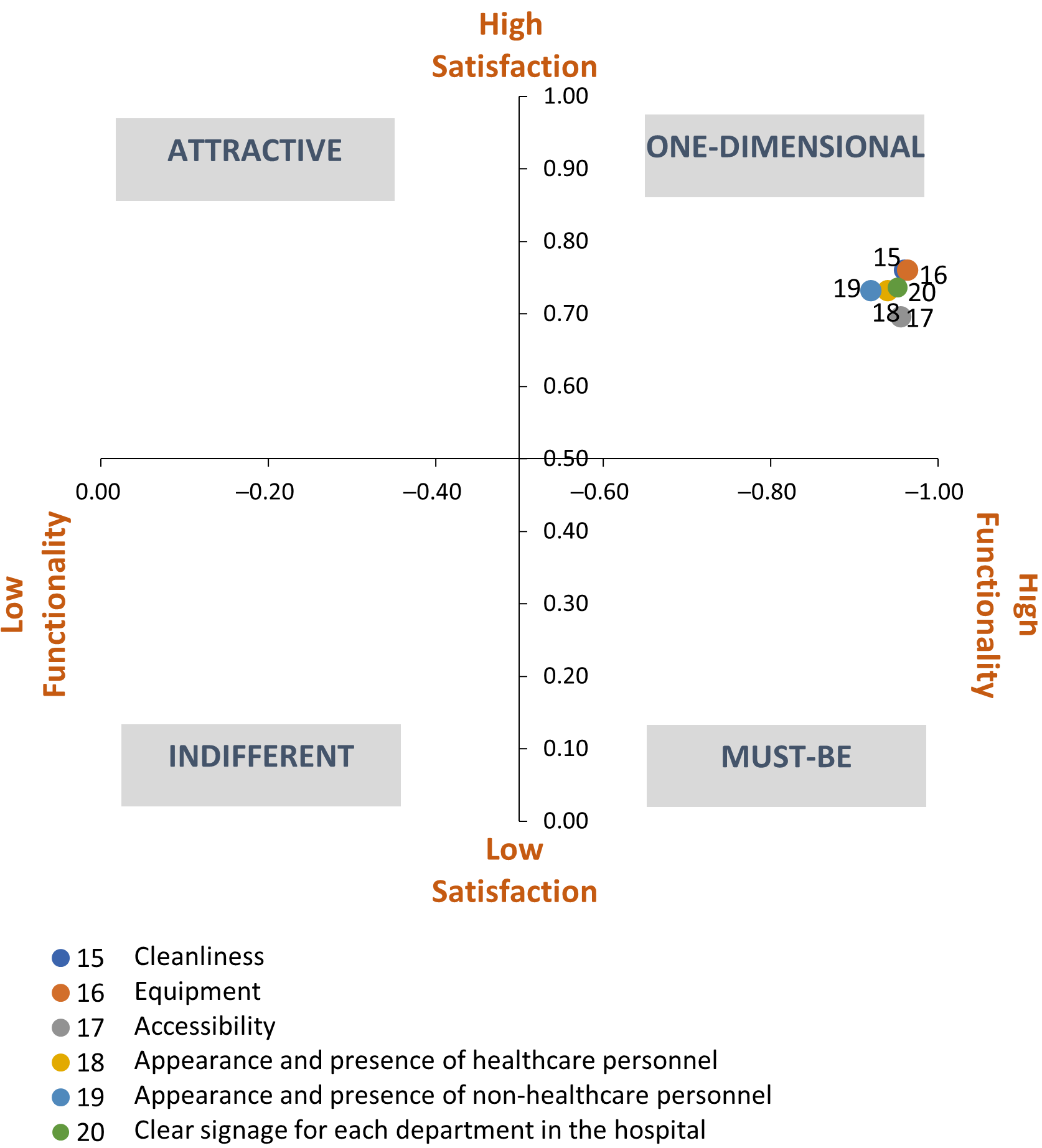
4.3. Facilities, Equipment, and Tangibles (IEET)
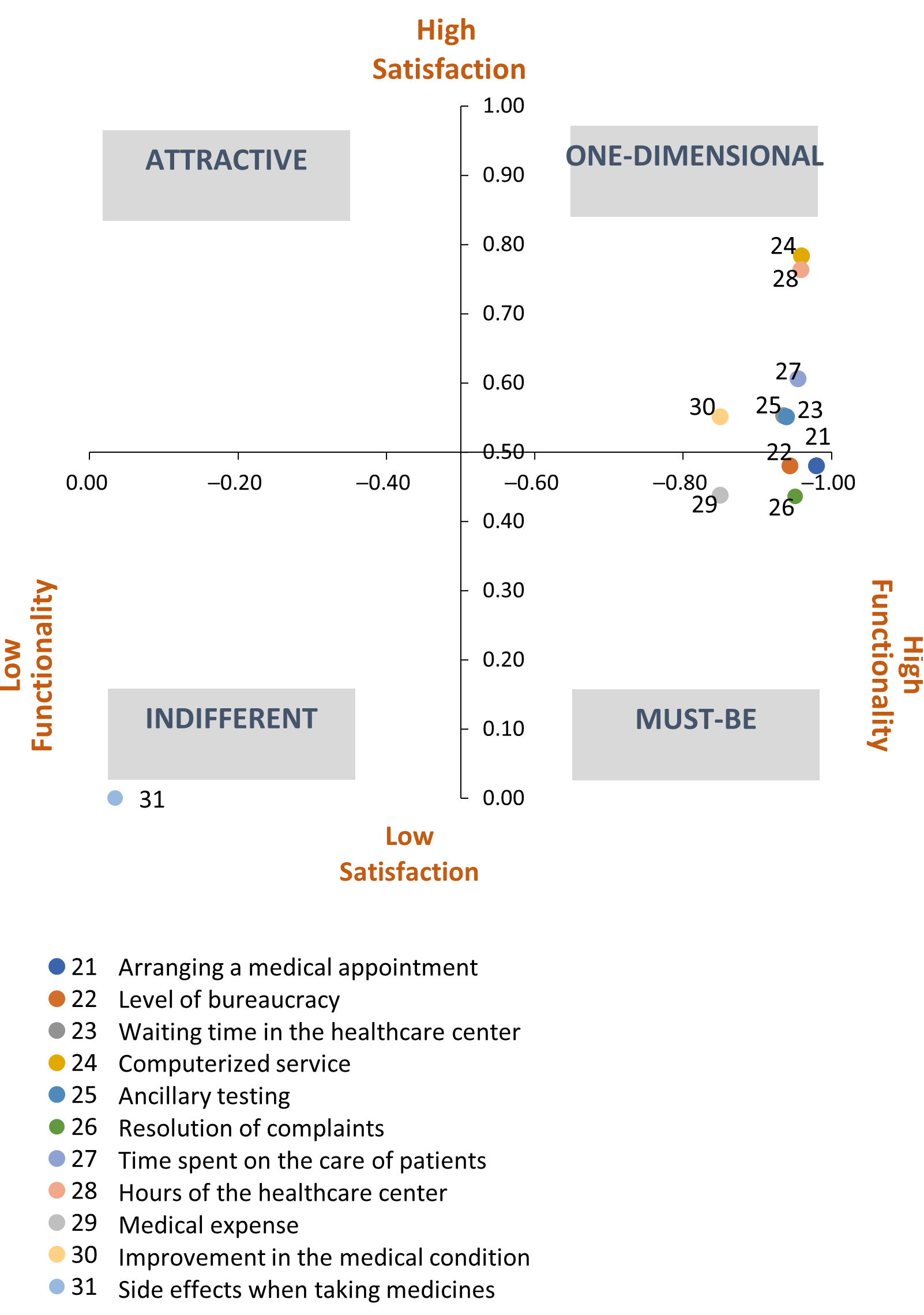
4.4. Efficiency (E)
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Javed, S.A.; Liu, S.; Mahmoudi, A.; Nawaz, M. Patients’ satisfaction and public and private sectors’ health care service quality in Pakistan: Application of grey decision analysis approaches. Int. J. Health Plan. Manag. 2019, 34, e168–e182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forrellat-Barrios, M. Calidad en los servicios de salud: Un reto ineludible. Rev. Cuba. Hematol. Inmunol. Hemoter. 2014, 30, 179–183. Available online: http://scielo.sld.cu/pdf/hih/v30n2/hih11214 (accessed on 27 January 2021).
- Bleich, S.N.; Özaltin, E.; Murray, C.J. How does satisfaction with the health-care system relate to patient experience? Bull. World Health Organ. 2009, 87, 271–278. [Google Scholar] [CrossRef]
- Sullivan, E.E.; Ellner, A. Strong Patient-Provider Relationships Drive Healthier Outcomes. Harv. Bus. Rev. 2015. Available online: https://hbr.org/2015/10/strong-patient-provider-relationships-drive-healthier-outcomes (accessed on 27 January 2021).
- Khan, N.; Puthussery, S. Stakeholder perspectives on public-private partnership in health service delivery in Sindh province of Pakistan: A qualitative study. Public Health 2019, 170, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Broadbent, J.; Laughlin, R. Public private partnerships: An introduction. Account. Audit. Account. J. 2003, 16, 322–341. [Google Scholar] [CrossRef] [Green Version]
- Moro Visconti, R.; Morea, D. Healthcare digitalization and pay-for-performance incentives in smart hospital project financing. Int. J. Environ. Res. Public Health 2020, 17, 2318. [Google Scholar] [CrossRef] [Green Version]
- Morea, D.; Gebennini, E. New Project Financing and Eco-Efficiency Models for Investment Sustainability. Sustainability 2021, 13, 786. [Google Scholar] [CrossRef]
- Visconti, R.M.; Doś, A.; Gurgun, A.P. Public–Private Partnerships for Sustainable Healthcare in Emerging Economies. In The Emerald Handbook of Public–Private Partnerships in Developing and Emerging Economies; Leitão, J., de Morais Sarmento, E., Aleluia, J., Eds.; Emerald Publishing Limited: London, UK, 2017; pp. 407–437. [Google Scholar]
- Greve, C.; Christensen, L.T.; Tvarnø, C.; Nielsen, S.N.; Denta, S.M. Public-private partnerships in the healthcare sector: Limited policy guidelines, but active project development in Denmark. J. Econ. Policy Reform. 2021, 1–15. [Google Scholar] [CrossRef]
- Cruz, C.O.; Marques, R.C. Flexible contracts to cope with uncertainty in public–private partnerships. Int. J. Proj. Manag. 2013, 31, 473–483. [Google Scholar] [CrossRef]
- De Marco, A.; Mangano, G. Risk and value in privately financed health care projects. J. Constr. Eng. Manag. 2013, 139, 918–926. [Google Scholar] [CrossRef] [Green Version]
- Möller-Leimkühler, A.M.; Dunkel, R.; Müller, P.; Pukies, G.; de Fazio, S.; Lehmann, E. Is patient satisfaction a unidimensional construct? Factor analysis of the Munich Patient Satisfaction Scale (MPSS-24). Eur. Arch. Psychiatry Clin. Neurosci. 2002, 252, 19–23. [Google Scholar] [CrossRef]
- Donabedian, A. Explorations in Quality Assessment and Monitoring; Health Administration Press: Chicago, IL, USA, 1980. [Google Scholar]
- Oliveira, D.F.; Arieta, C.E.; Temporini, E.R.; Kara-José, N. Quality of health care: Patient satisfaction in a university hospital. Arq. Bras. Oftalmol. 2006, 69, 731–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, P.W.; Smith, K.L.; Ghushchyan, V.H.; Globe, D.R.; Lin, S.L.; Globe, G. Asthma in USA: Its impact on health-related quality of life. J. Asthma 2013, 50, 891–899. [Google Scholar] [CrossRef]
- Shahin, A.; Akasheh, S. Classifying customer requirements using Kano model and Kano map: The case of hospital services. Int. J. Product. Qual. Manag. 2017, 21, 500–515. [Google Scholar] [CrossRef]
- Lotfizadeh, M.; Wang, S.; Taylor, J.; Slusher, K. Assessment of patient satisfaction and experience through correlation analysis and Kano model. In Proceedings of the IIE Annual Conference, Norcross, GA, USA, 2017; pp. 2033–2038. [Google Scholar]
- Gustavsson, S.; Gremyr, I.; Kenne Sarenmalm, E. Using an adapted approach to the Kano model to identify patient needs from various patient roles. TQM J. 2016, 28, 151–162. [Google Scholar] [CrossRef]
- Kohn, L.T.; Corrigan, J.M.; Donaldson, M.S. To Err is Human: Building a Safer Health system. In Institute of Medicine (US) Committee on Quality of Health Care in America; National Academies Press: Washington, DC, USA, 2000; Available online: https://www.nap.edu/catalog/9728/to-err-is-human-building-a-safer-health-system (accessed on 27 January 2021).
- Mitrabasu, N. Integrating Kano model and Herzberg two factor theory to unveil the third quality factor of patient satisfaction in a multispecialty outdoor medical centre. Int. J. Emerg. Sci. Eng. 2013, 1, 1–5. [Google Scholar]
- Gupta, P.; Srivastava, R.K. Customer satisfaction for designing attractive qualities of healthcare service in India using Kano model and quality function deployment. MIT Int. J. Mech. Eng. 2011, 1, 101–107. [Google Scholar]
- Kano, N.; Seraku, N.; Takahashi, F.; Tsuji, S. Attractive Quality and Must-Be Quality. J. Jpn. Soc. Qual. Control 1984, 41, 39–48. [Google Scholar]
- Kuo, T.C.; Ma, H.-Y.; Huang, S.H.; Hu, A.H.; Huang, C.S. Barrier analysis for product service system using interpretive structural model. Int. J. Adv. Manuf. Technol. 2010, 49, 407–417. [Google Scholar] [CrossRef]
- Materla, T.; Cudney, E.A.; Hopen, D. Evaluating factors affecting patient satisfaction using the Kano model. Int. J. Health Care Qual. Assur. 2019, 32, 137–151. [Google Scholar] [CrossRef]
- Chiou, C.C.; Cheng, Y.S. An integrated method of Kano model and QFD for designing impressive qualities of healthcare service. In Proceedings of the 2008 IEEE International Conference on Industrial Engineering and Engineering Management, Singapore, 6 January 2008; pp. 590–594. [Google Scholar]
- Sulisworo, D.; Maniquiz, N. Integrating Kano’s Model and Servqual to Improve Healthcare Service Quality. In Proceedings of the International Conference on Green World in Business and Technology, Yogyakarta, Indonesia, 21–24 March 2012. [Google Scholar]
- Pawitra, T.A.; Tan, K.C. Tourist satisfaction in Singapore–a perspective from Indonesian tourists. Manag. Serv. Qual. 2003, 13, 399–411. [Google Scholar] [CrossRef]
- Sahney, S. Delighting customers of management education in India: A student perspective, part I. TQM J. 2011, 23, 644–658. [Google Scholar] [CrossRef]
- Chen, L.H.; Kuo, Y.F. Understanding e-learning service quality of a commercial bank by using Kano’s model. Total Qual. Manag. Bus. 2011, 22, 99–116. [Google Scholar] [CrossRef]
- Hejaili, F.F.; Assad, L.; Shaheen, F.A.; Moussa, D.H.; Karkar, A.; AlRukhaimi, M. Culture-related service expectations: A comparative study using the Kano model. Qual. Manag. Health Care 2009, 18, 48–58. [Google Scholar] [CrossRef]
- Huang, J.C. Application of Kano model and IPA on improvement of service quality of mobile healthcare. Int. J. Mob. Commun. 2018, 16, 227–246. [Google Scholar] [CrossRef]
- Sanakulov, N.; Karjaluoto, H. Consumer adoption of mobile technologies: A literature review. Int. J. Mob. Commun. 2015, 13, 244–275. [Google Scholar] [CrossRef]
- Barrios-Ipenza, F.; Calvo-Mora, A.; Velicia-Martín, F.; Criado-García, F.; Leal-Millán, A. Patient Satisfaction in the Peruvian Health Services: Validation and Application of the HEALTHQUAL Scale. Int. J. Environ. Res. Public Health 2020, 17, 5111. [Google Scholar] [CrossRef]
- Lam, S.S. SERVQUAL: A tool for measuring patients’ opinions of hospital service quality in Hong Kong. Total Qual. Manag. 1997, 8, 145–152. [Google Scholar] [CrossRef]
- Davies, B.; Baron, S.; Gear, T.; Read, M. Measuring and Managing Service Quality. Mark. Intell. Plan. 1999, 17, 33–40. [Google Scholar] [CrossRef]
- Gouthier, M.; Giese, A.; Bartl, C. Service excellence models: A critical discussion and comparison. Manag. Serv. Qual. 2012, 22, 447–464. [Google Scholar] [CrossRef]
- AENOR. UNE-CEN/TS 16880 Service Excellence. Creating Outstanding Customer Experiences through Service Excellence. Spain. Available online: https://www.aenor.com/normas-y-libros/buscador-de-normas/une?c=N0055921 (accessed on 27 January 2021).
- Asif, M. A critical review of service excellence models: Towards developing an integrated framework. Qual. Quant. 2015, 49, 763–783. [Google Scholar] [CrossRef]
- Schneider, B.; Bowen, D.E. Understanding customer delight and outrage. Sloan Manag. Rev. 1999, 41, 35–45. [Google Scholar]
- Berman, B. How to delight your customers. Calif. Manag. Rev. 2005, 48, 129–151. [Google Scholar] [CrossRef]
- Johnston, R. Towards a better understanding of service excellence. Manag. Serv. Qual. 2004, 14, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Johnston, R. Insights into service excellence. In Service Excellence als Impulsgeber; Gouthier, M.H.J., Coenen, C., Schulze, H.S., Wegmann, C., Eds.; Gabler Verlag: Wiesbaden, Germany, 2007; pp. 17–35. [Google Scholar]
- Lytle, R.S.; Hom, P.W.; Mokwa, M.P. SERV*OR: A managerial measure of organizational service-orientation. J. Retail. 1998, 74, 455–489. [Google Scholar] [CrossRef]
- EFQM Excellence Model. European Foundation for Quality Management, Brussels. Available online: https://www.efqm.org/index.php/efqm-model/ (accessed on 27 January 2021).
- Asif, M.; Gouthier, M.H.J. What service excellence can learn from business excellence models? Total Qual. Manag. Bus. Excell. 2014, 25, 511–531. [Google Scholar] [CrossRef]
- NIST. Malcolm Baldrige National Quality Award. Available online: https://www.nist.gov/baldrige/baldrige-award (accessed on 27 January 2021).
- Periañez-Cristobal, R.; Calvo-Mora, A.; Rey-Moreno, M.; Suárez, E. Organisational profiles: Key factors and results from the EFQM model perspective. Total Qual. Manag. Bus. Excell. 2020, 1–24. [Google Scholar] [CrossRef]
- Rezaei, S.; Hajizadeh, M.; Zandian, H.; Fathi, A.; Nouri, B. Service quality in Iranian hospitals: A systematic review and meta-analysis. Med J. Islamic Repub. Iran 2018, 32, 59. [Google Scholar] [CrossRef]
- Rose, R.C.; Uli, J.; Abdul, M.; Ng, K.L. Hospital service quality: A managerial challenge. Int. J. Health Care Qual. Assur. 2004, 17, 146–159. [Google Scholar] [CrossRef]
- Go, M.; Kim, I. In-flight NCCI management by combining the Kano model with the service blueprint: A comparison of frequent and infrequent flyers. Tour. Manag. 2018, 69, 471–486. [Google Scholar] [CrossRef]
- Jané, A.C.; Domínguez, S.M. Citizens’ Role in Health Services: Satisfaction Behavior: Kano’s Model, Part 1. Qual Manag. Healthc. 2003, 12, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Park, Y.; Yu, J. An Assessment Model for Evaluating Asymmetric Effects of Attribute-Level Performance on Satisfaction. Sustainability 2019, 11, 4323. [Google Scholar] [CrossRef] [Green Version]
- Lengnick-Hall, C.A. The patient as the pivot point for quality in health care delivery. J. Healthc. Manag. 1995, 40, 25–39. [Google Scholar]
- Vassiliadis, C.A.; Fotiadis, A.K.; Tavlaridou, E. The effect of creating new secondary health services on patients’ perceptions: A Kano service quality analysis approach. Total Qual. Manag. Bus. Excell. 2014, 25, 897–907. [Google Scholar] [CrossRef]
- Sulisworo, D. Integrating Kano’s Model and SERVQUAL to Improve Healthcare Service Quality. Ahmad Dahlan University. Available online: http://eprints.uad.ac.id/1354/ (accessed on 27 May 2021).
- Berger, C.; Blauth, R.; Boger, D. Kano’s Methods for understanding customer-defined quality. Center Qual. Manag. J. 1993, 2, 3–36. [Google Scholar]
- Cabello, E.; Chirinos, J.L. Validación y aplicabilidad de encuestas SERVQUAL modificadas para medir la satisfacción de usuarios externos en servicios de salud. Rev. Médica Herediana 2012, 23, 88–95. [Google Scholar] [CrossRef] [Green Version]
- Zevallos, L.; Salas, V.; y Robles, L. Asociaciones público-privadas para servicio de salud: ¿la solución al sistema de salud peruano? Rev. Peru Med. Exp. Salud Pública 2014, 31, 769–774. [Google Scholar] [CrossRef] [Green Version]
- Bravo-Orellana, S. Asociaciones Público Privadas en el sector salud. Círculo. Derecho Adm. 2013, 13, 123–140. Available online: http://revistas.pucp.edu.pe/index.php/derechoadministrativo/article/view/13472/14099 (accessed on 27 January 2021).
- Hashim, H.A.; Sapri, M.; Low, S.-T. Public private partnership (PPP) facilities management for healthcare services in Malaysia: The challenges of implementation. J. Facil. Manag. 2016, 14, 350–362. [Google Scholar] [CrossRef]
- Hashim, H.A.; Sapri, M.; Shazmin, S.S.A. Strategic facilities management functions for public private partnership (PPP) healthcare services in Malaysia. Plan. Malays. 2019, 17, 25–47. [Google Scholar]
- Öge, H.; Bas, T. Public–private Partnership Healthcare Projects in Turkey. J. Bus. Sci. 2016, 4, 105–119. [Google Scholar]
- Ramakrishnan, D. Public Private Partnership (PPP) in Indian Health Care. SSRN. Available online: http://ssrn.com/abstract=2186897 (accessed on 27 January 2021).
- Velásquez, A.; Suarez, D.; y Nepo-Linares, E. Reforma del sector salud en el Perú: Derecho, gobernanza, cobertura universal y respuesta contra riesgos sanitarios. Rev. Peru Med. Exp. Salud Pública 2016, 33, 546–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wongrukmit, P.; Thawesaengskulthai, N. Hospital service quality preferences among culture diversity. Total Qual. Manag. Bus. Excell. 2014, 25, 908–922. [Google Scholar] [CrossRef]
- Reddick, C.G.; Enriquez, R.; Harris, R.J.; Sharma, B. Determinants of broadband access and affordability: An analysis of a community survey on the digital divide. Cities 2020, 106, 102904. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dimension | Service Attribute |
|---|---|
| Health personnel | 1. Level of professionalism |
| 2. Kindness and courtesy of health personnel | |
| 3. Confidence in health personnel | |
| 4. Personalized service | |
| 5. Communication | |
| 6. Individualized care provided by healthcare personnel | |
| 7. Interest in attending to the patient’s problem | |
| 8. Interest in understanding the problems of the patient | |
| 9. Prestige of healthcare personnel | |
| 10. Detailed explanation of the diagnosis and treatment | |
| Non-health personnel | 11. Level of professionalism |
| 12. Kindness and courtesy | |
| 13. Individualized care toward the problems of the patient | |
| 14. Interest in attending to the patient´s problems | |
| Facilities, equipment, and tangibles | 15. Cleanliness |
| 16. Equipment | |
| 17. Accessibility | |
| 18. Appearance and presence of healthcare personnel | |
| 19. Appearance and presence of non-healthcare personnel | |
| 20. Clear signage for each department in the hospital | |
| Efficiency | 21. Arranging a medical appointment |
| 22. Level of bureaucracy | |
| 23. Waiting time in the healthcare center | |
| 24. Computerized service | |
| 25. Ancillary testing | |
| 26. Resolution of complaints | |
| 27. Time spent on the care of patients | |
| 28. Hours of the healthcare center | |
| 29. Medical expense | |
| 30. Improvement in the medical condition | |
| 31. Side effects when taking medicines |
| Features | Calculation |
|---|---|
| Degree of satisfaction (CS) | Attractive + one-dimensional Attractive + one-dimensional + mandatory + indifferent |
| Degree of dissatisfaction (DS) | Mandatory + one-dimensional Attractive + one-dimensional + mandatory + indifferent |
| Variables | n | % | |
|---|---|---|---|
| Age | 18–34 | 67 | 27% |
| 35–54 | 101 | 40% | |
| 55–74 | 60 | 24% | |
| 75+ | 22 | 9% | |
| Gender | Male | 122 | 49% |
| Female | 128 | 51% | |
| Hospital | Barton Thomson | 128 | 51% |
| Guillermo Kaelin | 122 | 49% | |
| Question | Attributes | Quality Levels 1 | Classif. | CS 2 | DS 3 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| A | Q | I | R | M | O | |||||
| 1 | How do you feel about the level of professionalism of the healthcare personnel? | 24 | 0 | 21 | 0 | 85 | 120 | O | 0.58 | −0.82 |
| 2 | If the healthcare staff are kind and courteous, how do you feel? | 12 | 0 | 4 | 0 | 74 | 160 | O | 0.69 | −0.94 |
| 3 | If the healthcare staff are confident, how do you feel? | 2 | 0 | 8 | 0 | 99 | 141 | O | 0.57 | −0.96 |
| 4 | If the health personnel provide a personalized service, how do you feel? | 10 | 1 | 9 | 0 | 98 | 132 | O | 0.57 | −0.92 |
| 5 | How do you feel if the communication with the healthcare personnel is good? | 7 | 0 | 3 | 0 | 78 | 162 | O | 0.68 | −0.96 |
| 6 | How do you feel if the individualized care of the healthcare personnel is good? | 4 | 0 | 2 | 0 | 70 | 174 | O | 0.71 | −0.98 |
| 7 | How do you feel if the healthcare personnel show interest in solving your problems? | 4 | 1 | 2 | 0 | 91 | 152 | O | 0.63 | −0.98 |
| 8 | How do you feel if the health staff show interest in understanding your problems? | 8 | 0 | 4 | 1 | 89 | 148 | O | 0.63 | −0.95 |
| 9 | If the medical staff are prestigious, how do you feel? | 17 | 0 | 10 | 2 | 94 | 127 | O | 0.58 | −0.89 |
| 10 | If doctors explain in detail the diagnoses and treatment of a disease, how do you feel? | 5 | 0 | 3 | 2 | 72 | 168 | O | 0.70 | −0.97 |
| Question | Attributes | Quality Levels 1 | Classif. | CS 2 | DS 3 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| A | Q | I | R | M | O | |||||
| 11 | If non-healthcare personnel act professionally, how do you feel? | 1 | 0 | 6 | 1 | 98 | 144 | O | 0.58 | −0.97 |
| 12 | If non-healthcare staff are kind and courteous, how do you feel? | 5 | 0 | 2 | 1 | 75 | 167 | O | 0.69 | −0.97 |
| 13 | How do you feel if non-healthcare personnel attend to your problems? | 3 | 0 | 5 | 2 | 88 | 152 | O | 0.63 | −0.97 |
| 14 | How do you feel if non-healthcare personnel show interest in solving your problems? | 8 | 0 | 0 | 1 | 86 | 155 | O | 0.65 | −0.97 |
| Question | Attributes | Quality Levels 1 | Classif. | CS 2 | DS 3 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| A | Q | I | R | M | O | |||||
| 15 | How do you feel about the cleanliness of the facilities? | 6 | 0 | 4 | 0 | 56 | 184 | O | 0.76 | −0.96 |
| 16 | If the healthcare center equipment is adequate, how do you feel? | 8 | 0 | 1 | 0 | 81 | 160 | O | 0.67 | −0.96 |
| 17 | If the accessibility to the healthcare center is adequate, how do you feel? | 7 | 0 | 4 | 0 | 72 | 167 | O | 0.70 | −0.96 |
| 18 | If the appearance and presence of the healthcare personnel are adequate, how do you feel? | 10 | 0 | 5 | 0 | 62 | 173 | O | 0.73 | −0.94 |
| 19 | If the appearance and presence of non-healthcare personnel are adequate, how do you feel? | 11 | 0 | 9 | 0 | 58 | 172 | O | 0.73 | −0.92 |
| 20 | Given the existence of clear signage for each department in the hospital, how do you feel? | 9 | 0 | 3 | 0 | 63 | 175 | O | 0.74 | −0.95 |
| Question | Attributes | Quality Levels 1 | Classif. | CS 2 | DS 3 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| A | Q | I | R | M | O | |||||
| 21 | Given the many facilities to arrange a medical appointment, how do you feel? | 2 | 0 | 3 | 0 | 127 | 118 | M | 0.48 | −0.98 |
| 22 | If the level of bureaucracy is low, how do you feel? | 3 | 0 | 11 | 0 | 122 | 114 | M | 0.47 | −0.94 |
| 23 | Given the adequate waiting time before entering a medical consultation, how do you feel? | 2 | 0 | 14 | 0 | 98 | 136 | O | 0.55 | −0.94 |
| 24 | If the hospital provides a very good computerized service, how do you feel? | 8 | 0 | 2 | 1 | 52 | 187 | O | 0.78 | −0.96 |
| 25 | Given the adequate speed of ancillary testing, how do you feel? | 5 | 1 | 10 | 2 | 101 | 131 | O | 0.55 | −0.94 |
| 26 | Faced with the proper resolution of complaints, how do you feel? | 3 | 0 | 9 | 2 | 131 | 105 | M | 0.44 | −0.95 |
| 27 | Given the adequate time of care of each patient, how do you feel? | 4 | 1 | 7 | 3 | 90 | 145 | O | 0.61 | −0.96 |
| 28 | Given the appropriate hours of attention at the healthcare center, how do you feel? | 5 | 0 | 5 | 5 | 53 | 182 | O | 0.76 | −0.96 |
| 29 | Given the adequate medical expenses made by the patient, how do you feel? | 2 | 0 | 35 | 3 | 104 | 106 | O | 0.44 | −0.85 |
| 30 | If there is an improvement in the medical condition as a result of the efforts and treatment by medical personnel, how do you feel? | 14 | 1 | 23 | 2 | 88 | 122 | O | 0.55 | −0.85 |
| 31 | Given the occurrence of side effects when taking medicines, how do you feel? | 0 | 1 | 28 | 220 | 1 | 0 | R | 0.00 | −0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barrios-Ipenza, F.; Calvo-Mora, A.; Criado-García, F.; Curioso, W.H. Quality Evaluation of Health Services Using the Kano Model in Two Hospitals in Peru. Int. J. Environ. Res. Public Health 2021, 18, 6159. https://doi.org/10.3390/ijerph18116159
Barrios-Ipenza F, Calvo-Mora A, Criado-García F, Curioso WH. Quality Evaluation of Health Services Using the Kano Model in Two Hospitals in Peru. International Journal of Environmental Research and Public Health. 2021; 18(11):6159. https://doi.org/10.3390/ijerph18116159
Chicago/Turabian StyleBarrios-Ipenza, Fernando, Arturo Calvo-Mora, Fernando Criado-García, and Walter H. Curioso. 2021. "Quality Evaluation of Health Services Using the Kano Model in Two Hospitals in Peru" International Journal of Environmental Research and Public Health 18, no. 11: 6159. https://doi.org/10.3390/ijerph18116159
APA StyleBarrios-Ipenza, F., Calvo-Mora, A., Criado-García, F., & Curioso, W. H. (2021). Quality Evaluation of Health Services Using the Kano Model in Two Hospitals in Peru. International Journal of Environmental Research and Public Health, 18(11), 6159. https://doi.org/10.3390/ijerph18116159