
Assessing Caregivers’ Skills in Assisting People with Dementia during Mealtime: Portuguese Cultural Adaptation of the Feeding Skills Checklist



Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Translation and Adaptation Procedures
2.3. Assessment of the Psychometric Properties of the FSC-PT
2.4. Statistical Analysis
3. Results
3.1. Content Validity
3.2. Participants
3.3. Interobserver Reliability
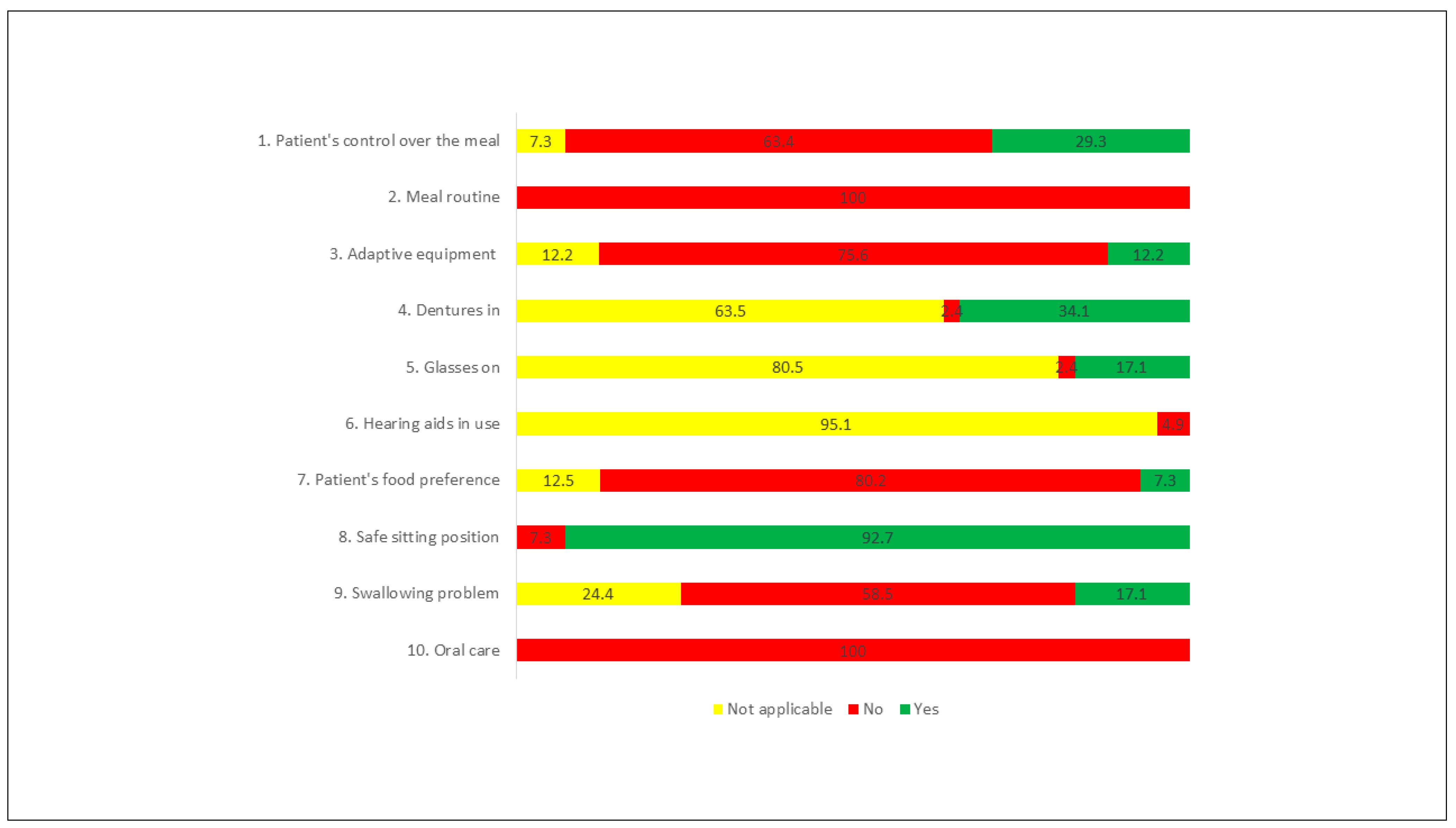
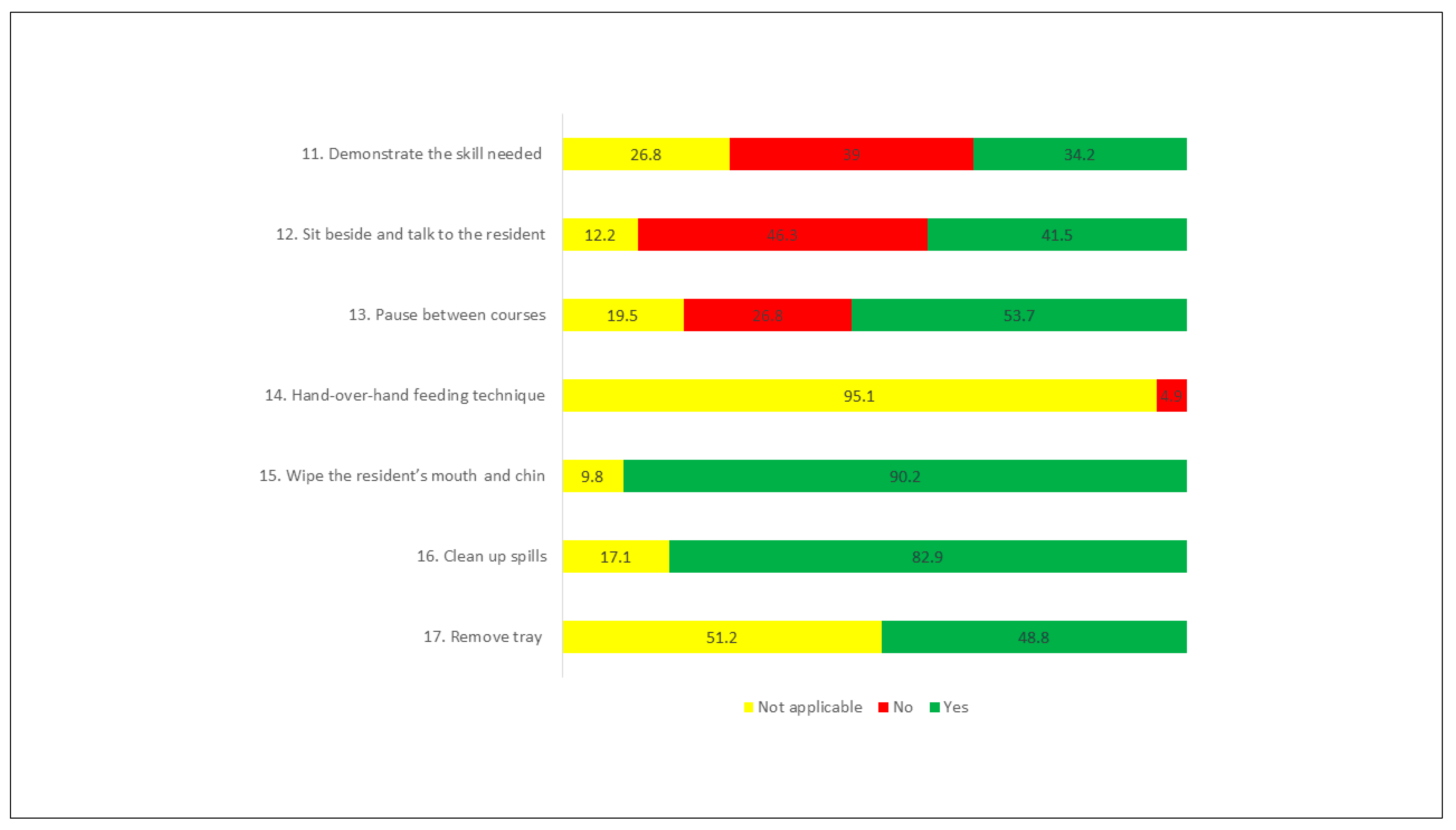
3.4. Study of the Good Practices in Feeding
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Cintra, M.T.G.; de Rezende, N.A.; de Torres, H.O.G. Qual a via mais adequada para a alimentação de idosos com demência avançada: Oral ou enteral? Geriatr. Gerontol. Aging 2013, 7, 308–317. [Google Scholar]
- Batchelor-Murphy, M.; Crowgey, S. Mealtime Difficulties in Dementia. In Evidence-Based Geriatric Nursing Protocols for Best Practice; Springer Publish Company: New York, NY, USA, 2016. [Google Scholar]
- Stone, L. Eating/Feeding Issues in Demenita: Improving the Dining Experience. End Life J. 2014, 4, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Morris, J.N.; Fries, B.E.; Morris, S.A. Scaling ADLs Within the MDS. J. Gerontol. Ser. A 1999, 54, M546–M553. [Google Scholar] [CrossRef]
- Palese, A.; Grassetti, L.; Bandera, D.; Zuttion, R.; Ferrario, B.; Ponta, S.; Hayter, M.; Watson, R. High feeding dependence prevalence in residents living in Italian nursing homes requires new policies: Findings from a regionally based cross-sectional study. Health Policy N. Y. 2018, 122, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Martins, A.S.; de Rezende, N.A.; da Torres, H.O.G. Occurrence of complications and survival rates in elderly with neurological disorders undergoing enteral nutrition therapy. Rev. Assoc. Med. Bras. 2012, 58, 691–697. [Google Scholar] [CrossRef] [Green Version]
- American Geriatrics Society Ethics Committee and Clinical Practice and Models of Care Committee. American Geriatrics Society Ethics Committee American Geriatrics Society Feeding Tubes in Advanced Dementia Position Statement. J. Am. Geriatr. Soc. 2014, 62, 1590–1593. [Google Scholar] [CrossRef] [PubMed]
- Barrocas, A.; Geppert, C.; Durfee, S.M.; Maillet, S.R.; Monturo, C.; Mueller, C.; Stratton, K.; Valentine, C.; Aspen, T. ASPEN Ethics Position Paper. Nutr. Clin. Pract. 2010, 25, 672–679. [Google Scholar]
- Volkert, D.; Chourdakis, M.; Faxen-Irving, G.; Frühwald, T.; Landi, F.; Suominen, M.H.; Vandewoude, M.; Wirth, R.; Schneider, S.M. ESPEN guidelines on nutrition in dementia. Clin. Nutr. 2015, 34, 1052–1073. [Google Scholar] [CrossRef] [Green Version]
- Royal College of Physicians. Oral Feeding Difficulties and Dilemmas. A Guide to Practical Care, Particularly Towards the End of Life; Royal College of Physicians: London, UK, 2010; ISBN 9781860163739. [Google Scholar]
- Gonçalves, J.T.M.; Horie, L.M.; Elisa, S.; Batista, A.; Bacchi, M.K.; Bailer, M.C.; Barbosa-silva, T.G.; Paula, A.; Barrére, N.; Barreto, P.A.; et al. Diretriz BRASPEN de Terapia Nutricional no Envelhecimento. Braspen J. 2019, 34, 2–58. [Google Scholar]
- Goldberg, L.S.; Altman, K.W. The role of gastrostomy tube placement in advanced dementia with dysphagia: A critical review. Clin. Interv. Aging 2014, 9, 1733–1739. [Google Scholar] [CrossRef] [Green Version]
- Alzheimer Europe: The Prevalence of Dementia in Europe. Available online: https://www.alzheimer-europe.org/Policy-in-Practice2/Country-comparisons/2013-The-prevalence-of-dementia-in-Europe (accessed on 15 April 2019).
- OECD. Care Needed: Improving the Lives of People with Dementia; OECD Health Policy Studies; OECD: Paris, France, 2018; ISBN 9789264085091. [Google Scholar]
- Rodrigues, I.B.; Adachi, J.D.; Beattie, K.A.; MacDermid, J.C. Development and validation of a new tool to measure the facilitators, barriers and preferences to exercise in people with osteoporosis. BMC Musculoskelet. Disord. 2017, 18, 540. [Google Scholar] [CrossRef] [Green Version]
- Kuske, B.; Luck, T.; Hanns, S.; Matschinger, H.; Angermeyer, M.C.; Behrens, J.; Riedel-Heller, S.G. Training in dementia care: A cluster-randomized controlled trial of a training program for nursing home staff in Germany. Int. Psychogeriatr. 2009, 21, 295–308. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, A.L.; Cruz, J.; Figueiredo, D.; Marques, A.; Sousa, L. Cuidar de idosos com demência em instituições: Competências, dificuldades e necessidades percepcionadas pelos cuidadores formais. Psicol. Saúde Doenças 2011, 12, 119–129. [Google Scholar] [CrossRef]
- Chang, C.-C.; Wykle, M.L.; Madigan, E.A. The Effect of A Feeding Skills Training Program for Nursing Assistants Who Feed Dementia Patients in Taiwanese Nursing Homes. Geriatr. Nurs. Minneap. 2006, 27, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Kuo, S.; Rhodes, R.L.; Mitchell, S.L.; Mor, V.; Teno, J.M. Natural History of Feeding-Tube Use in Nursing Home Residents With Advanced Dementia. J. Am. Med. Dir. Assoc. 2009, 10, 264–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amella, E.J. Resistance at mealtimes for persons with dementia. J. Nutr. Health Aging 2002, 6, 117–122. [Google Scholar] [PubMed]
- Simmons, S.F.; Osterweil, D.; Schnelle, J.F. Improving food intake in nursing home residents with feeding assistance: A staffing analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M790–M794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batchelor-Murphy, M.; Amella, E.J.; Zapka, J.; Mueller, M.; Beck, C. Feasibility of a web-based dementia feeding skills training program for nursing home staff. Geriatr. Nurs. Minneap. 2015, 36, 212–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amella, E.J.; Batchelor-Aselage, M.B. Facilitating ADLs by caregivers of persons with dementia: The C3P model. Occup. Ther. Health Care 2014, 28, 51–61. [Google Scholar] [CrossRef] [Green Version]
- Golden, S.D.; Earp, J.A.L. Social Ecological Approaches to Individuals and Their Contexts: Twenty Years of Health Education & Behavior Health Promotion Interventions. Health Educ. Behav. 2012, 39, 364–372. [Google Scholar] [CrossRef]
- Shune, S.E.; Linville, D. Understanding the dining experience of individuals with dysphagia living in care facilities: A grounded theory analysis. Int. J. Nurs. Stud. 2019, 92, 144–153. [Google Scholar] [CrossRef]
- Liu, W.; Williams, K.; Batchelor-Murphy, M.; Perkhounkova, Y.; Hein, M. Eating performance in relation to intake of solid and liquid food in nursing home residents with dementia: A secondary behavioral analysis of mealtime videos. Int. J. Nurs. Stud. 2019, 96, 18–26. [Google Scholar] [CrossRef]
- Amella Krug, E.J.; Qanungo, S.; Martin, K.L.; Mueller, M.; Madisetti, M.; Kelechi, T.J. A cluster randomized controlled trial to assess the efficacy of a telehealth-based train-the-trainer mealtime intervention delivered by respite care center volunteers to caregivers of persons with dementia to improve nutritional outcomes and quality of li. BMC Nutr. 2020, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Wild, D.; Alyson, G.; Mona, M.; Sonya, E.; Sandra, M.; Verjee-Lorenz, A.; Erikson, P. Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes (PRO) Measures. Value Health 2005, 8, 95–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polit, D.F.; Beck, C.T. The content validity index: Are you sure you know what’s being reported? Critique and recommendations. Res. Nurs. Health 2006, 29, 489–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamanzadeh, V.; Ghahramanian, A.; Rassouli, M.; Abbaszadeh, A.; Alavi-Majd, H.; Nikanfar, A.-R. Design and Implementation Content Validity Study: Development of an instrument for measuring Patient-Centered Communication. J. Caring Sci. 2015, 4, 165–178. [Google Scholar] [CrossRef]
- Zamanzadeh, V.; Rassouli, M.; Abbaszadeh, A.; Majd, H.A.; Nikanfar, A.; Ghahramanian, A. Details of content validity and objectifying it in instrument development. Nurs. Pract. Today 2014, 1, 163–171. [Google Scholar]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Yang, Y.; Hsiao, C.; Kuo, H.; Wang, J. Development and psychometric testing of a dementia care competence scale for nurses working in acute care setting. Scand. J. Caring Sci. 2020. [Google Scholar] [CrossRef]
- Suvanich, R.; Chatchawan, U.; Jariengprasert, C.; Yimtae, K.; Hunsawong, T.; Emasithi, A. Development and validation of the dizziness symptoms questionnaire in Thai-outpatients. Braz. J. Otorhinolaryngol. 2021. [Google Scholar] [CrossRef]
- Wong, F.M.F. First Data in the Process of Validating a Tool to Evaluate Knowledge, Attitude, and Practice of Healthcare Providers in Oral Care of Institutionalized Elderly Residents: Content Validity, Reliability and Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 4145. [Google Scholar] [CrossRef]
- Lynn, M.R. Determination and quantification of content validity. Nurs. Res. 1986, 35, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Haynes, S.N.; Richard, D.C.S.; Kubany, E.S. Content validity in psychological assessment: A functional approach to concepts and methods. Psychol. Assess. 1995, 7, 238–247. [Google Scholar] [CrossRef]
- Sireci, S. The construct of content validity. Soc. Indic. Res. 1998, 45, 83–117. [Google Scholar] [CrossRef]
- Sireci, S.; Faulkner-Bond, M. Validity evidence based on test content. Psicothema 2014, 26, 100–107. [Google Scholar] [CrossRef]
- Shrotryia, V.K.; Dhanda, U. Content Validity of Assessment Instrument for Employee Engagement. SAGE Open 2019, 9, 215824401882175. [Google Scholar] [CrossRef] [Green Version]
- Alexandre, N.M.C.; Coluci, M.Z.O. Validade de conteúdo nos processos de construção e adaptação de instrumentos de medidas. Ciência Saúde Coletiva 2011, 16, 3061–3068. [Google Scholar] [CrossRef]
- Pilatti, L.A.; Pedroso, B.; Gutierrez, G.L. Propriedades Psicométricas de Instrumentos de Avaliação: Um debate necessário. Rev. Bras. Ensino Ciênc. Tecnol. 2010, 3. [Google Scholar] [CrossRef] [Green Version]
- Sarvimäki, A.; Stenbock-Hult, B. The meaning of vulnerability to older persons. Nurs. Ethics 2016, 23, 372–383. [Google Scholar] [CrossRef]
- Batchelor-Murphy, M.; Mcconnell, E.S.; Amella, E.J.; Anderson, R.A.; Bales, C.W.; Silva, S.; Barnes, A.; Beck, C.; Colon-Emeric, C.S. Experimental Comparison of Efficacy for Three Handfeeding Techniques in Dementia. J. Am. Geriatr. Soc. 2017, 65, 89–94. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| FSC Dimension | Item | I-CVI | PC | κ | Interpretation | ||||
|---|---|---|---|---|---|---|---|---|---|
| 1st Round | 2nd Round | 1st Round | 2nd Round | 1st Round | 2nd Round | 1st Round | 2nd Round | ||
| Person with dementia | 1. Patient’s control over the meal | 0.625 | 1 | 0.218 | 0.004 | 0.52 | 1 | Fair | Excellent |
| 2. Meal routine | 0.625 | 1 | 0.218 | 0.004 | 0.52 | 1 | Fair | Excellent | |
| 3. Adaptive equipment | 0.625 | 0.85 | 0.218 | 0.12 | 0.52 | 0.72 | Fair | Good | |
| 4. Dentures in | 1 | - | 0.004 | - | 1 | - | Excellent | Excellent | |
| 5. Glasses in | 1 | - | 0.004 | - | 1 | - | Excellent | Excellent | |
| 6. Hearing aids in use | 0.75 | 1 | 0.12 | 0.004 | 0.72 | 1 | Good | Excellent | |
| 7. Patient’s food preference | 0.625 | 1 | 0.218 | 0.004 | 0.52 | 1 | Fair | Excellent | |
| 8. Safe sitting position | 0.625 | 1 | 0.218 | 0.004 | 0.52 | 1 | Fair | Excellent | |
| 9. Swallowing problem | 0.625 | 0.875 | 0.218 | 0.0313 | 0.52 | 0.87 | Fair | Excellent | |
| 10. Oral care | 0.875 | - | 0.0313 | - | 0.87 | - | Excellent | Excellent | |
| Caregiver | 11. Demonstrate the skill needed | 0.75 | 0.875 | 0.12 | 0.0313 | 0.72 | 0.87 | Good | Excellent |
| 12. Sit beside and talk to the resident | 0.875 | - | 0.0313 | - | 0.87 | - | Excellent | Excellent | |
| 13. Pause between courses | 0.75 | 0.875 | 0.12 | 0.0313 | 0.72 | 0.87 | Good | Excellent | |
| 14. Hand-over-hand feeding technique | 0.875 | - | 0.0313 | - | 0.87 | - | Excellent | Excellent | |
| 15. Wipe the resident’s mouth and chin | 0.75 | 0.875 | 0.12 | 0.0313 | 0.72 | 0.87 | Good | Excellent | |
| 16. Clean up spills | 0.625 | 1 | 0.218 | 0.004 | 0.52 | 1 | Fair | Excellent | |
| 17. Remove tray | 0.75 | 1 | 0.12 | 0.004 | 0.72 | 1 | Good | Excellent | |
| Environment | 18. Monitoring noise level | 1 | - | 0.004 | - | 1 | - | Excellent | Excellent |
| 19. Limiting traffic in the room | 1 | - | 0.004 | - | 1 | - | Excellent | Excellent | |
| 20. Resident sitting in same area | 0.875 | - | 0.0313 | - | 0.87 | - | Excellent | Excellent | |
| 21. Adequate lighting | 1 | - | 0.004 | - | 1 | - | Excellent | Excellent | |
| 22. Present foods one at a time | 0.875 | - | 0.0313 | - | 0.87 | - | Excellent | Excellent | |
| 23. Contrasting placemat | 1 | - | 0.004 | - | 1 | - | Excellent | Excellent | |
| 24. Set up the patient’s tray | 0.875 | - | 0.0313 | - | 0.87 | - | Excellent | Excellent | |
| Mean | 0.807 | 0.945 | |||||||
| Variable | n = 23 |
|---|---|
| Age [years] Mean (SD) | 44.73 (10.42) |
| Profession time [years] Mean (SD) | 10.28 (10.46) |
| Time in the NH [years] Mean (SD) | 7.81 (8.96) |
| Sex n (%) | |
| Female | 23 (100) |
| Education n (%) | |
| Primary school | 2 (8.8) |
| Secondary school | 14 (60.8) |
| High school | 4 (17.4) |
| University | 3 (13.0) |
| Marital Status n (%) | |
| Single | 2 (8.7) |
| Married | 19 (82.6) |
| Divorced | 2 (8.7) |
| Weekly workload [hours] Mean (SD) | 38.17 (1.46) |
| Weekly workload n (%) | |
| 37 h | 14 (60.9) |
| 40 h | 9 (39.1) |
| Specific training n (%) | |
| Yes | 13 (56.5) |
| No | 10 (43.5) |
| Observer 1 n (%) | Observer 2 n (%) | K | p Value | C | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| FSC Dimension | Item | Yes | No | Not Applicable | Yes | No | Not Applicable | |||
| Person with dementia | 1. Patient’s control over the meal | 11 (36.7) | 16 (53.3) | 3 (10) | 11 (36.7) | 16 (53.3) | 3 (10) | 1 | <0.01 | 100 |
| 2. Meal routine | - | 30 (100) | - | - | 30 (100) | - | * | * | 100 | |
| 3. Adaptive equipment | 4 (13.3) | 22 (73.3) | 4 (13.3) | 4 (13.3) | 20 (66.7) | 6 (20) | 0.857 | <0.01 | 93.3 | |
| 4. Dentures in | 10 (33.3) | 1 (3.3) | 19 (63.3) | 10 (33.3) | 7 (23.3) | 13 (43.3) | 0.670 | <0.01 | 80 | |
| 5. Glasses in | 7 (23.3) | 1 (3.3) | 22 (73.3) | 7 (23.3) | 9 (30) | 14 (46.7) | 0.551 | <0.01 | 73.3 | |
| 6. Hearing aids in use | - | 2 (6.7) | 28 (93.3) | - | 12 (40) | 18 (6) | 0.193 | 0.73 | 66.6 | |
| 7. Patient’s food preference | 3 (10) | 23 (76.7) | 4 (13.3) | 2 (6.7) | 24 (80) | 4 (13.3) | 0.724 | <0.01 | 90 | |
| 8. Safe sitting position | 27 (90) | 3 (10) | - | 28 (93.3) | 2 (6.7) | - | 0.783 | <0.01 | 96.6 | |
| 9. Swallowing problem | 4 (13.3) | 19 (63.3) | 7 (23.3) | 5 (16.7) | 16 (53.3) | 9 (30) | 0.825 | <0.01 | 90 | |
| 10. Oral care | - | 30 (100) | - | - | 30 (100) | - | * | * | 100 | |
| Caregiver | 11. Demonstrate the skill needed | 7 (23.3) | 13 (43.3) | 10 (33.3) | 7 (23.3) | 15 (50) | 8 (26.7) | 0.896 | <0.01 | 93.3 |
| 12. Sit beside and talk to the resident | 9 (30) | 17 (56.7) | 4 (13.3) | 9 (30) | 19 (63.3) | 2 (6.7) | 0.877 | <0.01 | 93.3 | |
| 13. Pause between courses | 15 (50) | 11 (36.7) | 4 (13.3) | 14 (46.7) | 12 (40) | 4 (13.3) | 0.945 | <0.01 | 96.6 | |
| 14. Hand-over-hand feeding technique | - | 2 (6.7) | 28 (93.3) | - | 1 (3.3) | 29 (96.7) | 0.651 | <0.01 | 96.6 | |
| 15. Wipe the resident’s mouth and chin | 26 (86.7) | - | 4 (13.3) | 26 (86.7) | - | 4 (13.3) | 1 | <0.01 | 100 | |
| 16. Clean up spills | 24 (80) | - | 6 (20) | 25 (83.3) | - | 5 (16.7) | 0.889 | <0.01 | 96.6 | |
| 17. Remove tray | 17 (56.7) | - | 13 (43.3) | 15 (50) | - | 15 (50) | 0.867 | <0.01 | 93.3 | |
| Environment | 18. Monitoring noise level | 11 (36.7) | 1 (3.3) | 18 (60) | 11 (36.7) | 1 (3.3) | 18 (60) | 1 | <0.01 | 100 |
| 19. Limiting traffic in the room | 2 (6.7) | 1 (3.3) | 27 (90) | 2 (6.7) | 1 (3.3) | 27 (90) | 1 | <0.01 | 100 | |
| 20. Resident sitting in same area | 29 (96.7) | - | 1 (3.3) | 29 (96.7) | - | 1 (3.3) | 1 | <0.01 | 100 | |
| 21. Adequate lighting | 30 (100) | - | - | 30 (100) | - | - | * | * | 100 | |
| 22. Present foods one at a time | 27 (90) | 2 (6.7) | 1 (3.3) | 27 (90) | 2 (6.7) | 1 (3.3) | 1 | <0.01 | 100 | |
| 23. Contrasting placemat | 1 (3.3) | 12 (40) | 17 (56.7) | 1 (3.3) | 12 (40) | 17 (56.7) | 1 | <0.01 | 100 | |
| 24. Set up the patients’ tray | 4 (13.3) | 1 (3.3) | 25 (83.3) | 4 (13.3) | 1 (3.3) | 25 (83.3) | 1 | <0.01 | 100 | |
| Mean | 0.844 | 94.14 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Passos, L.; Tavares, J.; Figueiredo, D. Assessing Caregivers’ Skills in Assisting People with Dementia during Mealtime: Portuguese Cultural Adaptation of the Feeding Skills Checklist. Int. J. Environ. Res. Public Health 2021, 18, 6467. https://doi.org/10.3390/ijerph18126467
Passos L, Tavares J, Figueiredo D. Assessing Caregivers’ Skills in Assisting People with Dementia during Mealtime: Portuguese Cultural Adaptation of the Feeding Skills Checklist. International Journal of Environmental Research and Public Health. 2021; 18(12):6467. https://doi.org/10.3390/ijerph18126467
Chicago/Turabian StylePassos, Lígia, João Tavares, and Daniela Figueiredo. 2021. "Assessing Caregivers’ Skills in Assisting People with Dementia during Mealtime: Portuguese Cultural Adaptation of the Feeding Skills Checklist" International Journal of Environmental Research and Public Health 18, no. 12: 6467. https://doi.org/10.3390/ijerph18126467