
Mental Health Crisis and Stress Coping among Healthcare College Students Momentarily Displaced from Their Campus Community Because of COVID-19 Restrictions in Japan



Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Demographic Characteristics
3.2. Severity of Mental Health Problems and Associated Factors
3.3. Resilience Factors for Mental Health Outcomes
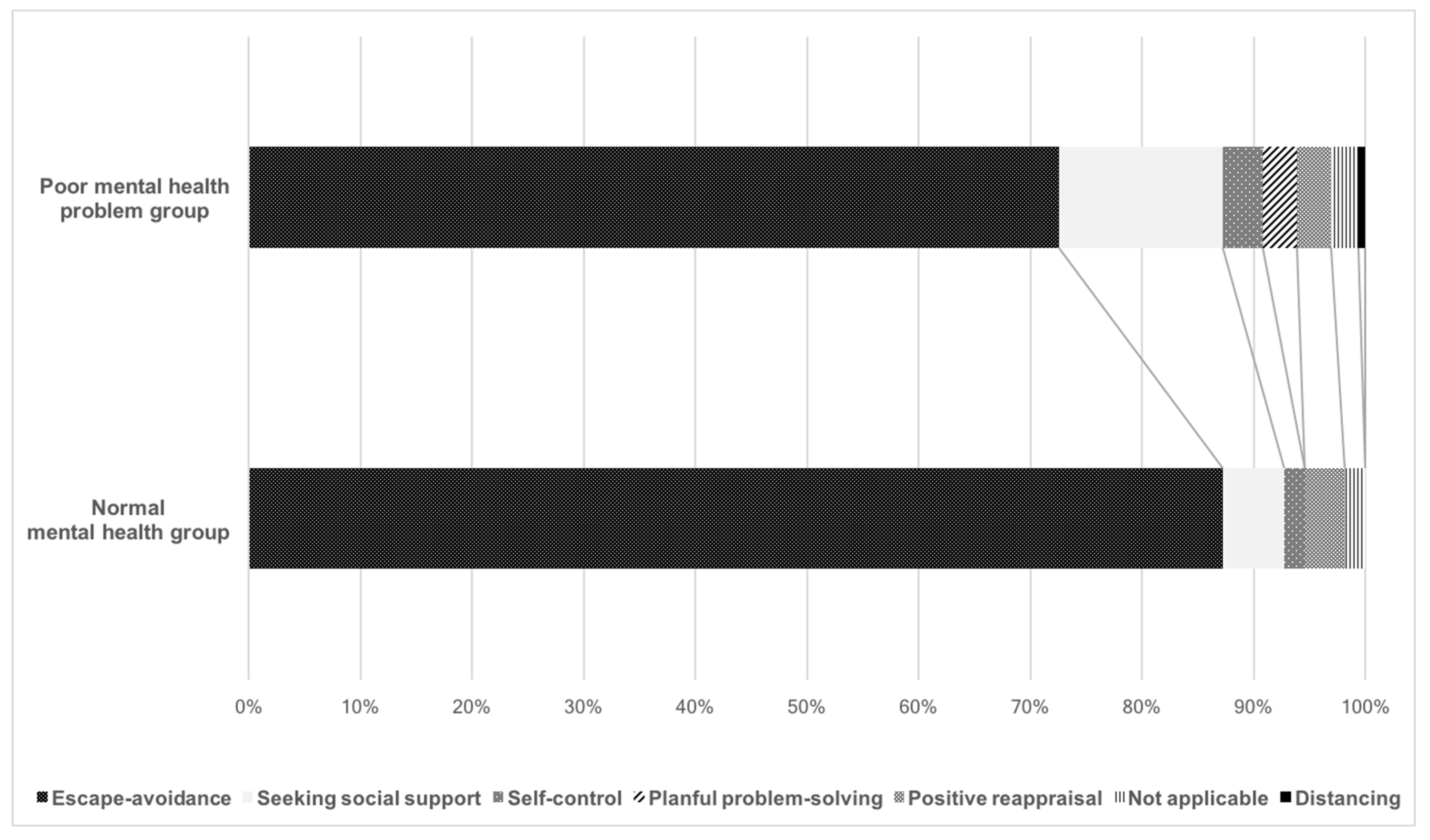
3.4. Coping Strategies: New Activities Initiated since Social Distancing Began
4. Discussion
4.1. Factors Contributing to Mental Health Decline among Healthcare College Students
4.2. Risk and Resilience Factors
4.3. Stress Coping Strategies
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef]
- Rose, S. Medical Student Education in the Time of COVID-19. JAMA 2020, 323, 2131. [Google Scholar] [CrossRef] [PubMed]
- Marelli, S.; Castelnuovo, A.; Somma, A.; Castronovo, V.; Mombelli, S.; Bottoni, D.; Leitner, C.; Fossati, A.; Ferini-Strambi, L. Impact of COVID-19 lockdown on sleep quality in university students and administration staff. J. Neurol. 2021, 268, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Odriozola-González, P.; Planchuelo-Gómez, Á.; Irurtia, M.J.; de Luis-García, R. Psychological effects of the COVID-19 outbreak and lockdown among students and workers of a Spanish university. Psychiatry Res. 2020, 290, 113108. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV). Available online: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 31 March 2020).
- The Case of the Coronavirus 31 March 2020. Updates on COVID-19 in Japan. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/newpage_00032.html (accessed on 31 March 2020).
- Tanaka, K.; Tahara, M.; Mashizume, Y.; Takahashi, K. Effects of Lifestyle Changes on the Mental Health of Healthcare Workers with Different Sense of Coherence Levels in the Era of COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 2801. [Google Scholar] [CrossRef] [PubMed]
- D’Aloja, E.; Finco, G.; Demontis, R.; Napoli, P.E.; Fossarello, M.; Nioi, M. COVID-19 and medical liability: Italy denies the shield to its heroes. EClinicalMedicine 2020, 25, 100470. [Google Scholar] [CrossRef] [PubMed]
- Nioi, M.; Napoli, P.E.; Lobina, J.; Fossarello, M.; D’Aloja, E. COVID-19 and Italian Healthcare Workers from the Initial Sacrifice to the mRNA Vaccine: Pandemic Chrono-History, Epidemiological Data, Ethical Dilemmas, and Future Challenges. Front. Public Health 2021, 8, 591900. [Google Scholar] [CrossRef]
- Napoli, P.E.; Nioi, M.; Fossarello, M. The “Quarantine Dry Eye”: The Lockdown for Coronavirus Disease 2019 and Its Implications for Ocular Surface Health. Health Policy 2021, ume 14, 1629–1636. [Google Scholar] [CrossRef]
- Folkman, S.; Lazarus, R.S. An Analysis of Coping in a Middle-Aged Community Sample. J. Health Soc. Behav. 1980, 21, 219. [Google Scholar] [CrossRef]
- Folkman, S.; Lazarus, R.S. Stress, Appraisal and Coping. In Health Psychology: A Handbook; Springer Publishing Company: New York, NY, USA, 1984. [Google Scholar]
- Goldberg, D.P.; Gater, R.; Sartorius, N.; Ustun, T.B.; Piccinelli, M.; Gureje, O.; Rutter, C. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol. Med. 1997, 27, 191–197. [Google Scholar] [CrossRef]
- Goldberg, D.P.; Oldehinkel, T.; Ormel, J. Why GHQ threshold varies from one place to another. Psychol. Med. 1998, 28, 915–921. [Google Scholar] [CrossRef]
- Nagasu, M.; Kogi, K.; Yamamoto, I. Association of socioeconomic and lifestyle-related risk factors with mental health conditions: A cross-sectional study. BMC Public Health 2019, 19, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Tahara, M.; Mashizume, Y.; Takahashi, K. Coping Mechanisms: Exploring Strategies Utilized by Japanese Healthcare Workers to Reduce Stress and Improve Mental Health during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 18, 131. [Google Scholar] [CrossRef]
- Carswell, A.; McColl, M.A.; Baptiste, S.; Law, M.; Polatajko, H.; Pollock, N. The Canadian Occupational Performance Measure: A Research and Clinical Literature Review. Can. J. Occup. Ther. 2004, 71, 210–222. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Baptiste, S.; McColl, M.; Opzoomer, A.; Polatajko, H.; Pollock, N. The Canadian Occupational Performance Measure: An Outcome Measure for Occupational Therapy. Can. J. Occup. Ther. 1990, 57, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.R. Intrinsic, extrinsic, and amotivational orientations: Their role in university adjustment, stress, well-being, and subsequent academic performance. Curr. Psychol. 2004, 23, 189–202. [Google Scholar] [CrossRef]
- Folkman, S.; Lazarus, R.S.; Dunkel-Schetter, C.; DeLongis, A.; Gruen, R.J. Dynamics of a stressful encounter: Cognitive ap-praisal, coping, and encounter outcomes. J. Personal. Soc. Psychol. 1986, 50, 992. [Google Scholar] [CrossRef]
- Li, Y.; Wang, Y.; Jiang, J.; Valdimarsdóttir, U.A.; Fall, K.; Fang, F.; Song, H.; Lu, D.; Zhang, W. Psychological distress among health professional students during the COVID-19 outbreak. Psychol. Med. 2020, 42, 1–3. [Google Scholar] [CrossRef]
- Assadi, S.M.; Nakhaei, M.R.; Najafi, F.; Fazel, S. Mental health in three generations of Iranian medical students and doctors. Soc. Psychiatry Psychiatr. Epidemiol. 2006, 42, 57–60. [Google Scholar] [CrossRef]
- Ohtsu, T.; Kaneita, Y.; Osaki, Y.; Kokaze, A.; Ochiai, H.; Shirasawa, T.; Nanri, H.; Ohida, T. Mental health status among Japanese medical students: A cross-sectional survey of 20 universities. Acta Med. Okayama 2014, 68, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Dyrbye, L.N.; Thomas, M.R.; Shanafelt, T.D. Systematic Review of Depression, Anxiety, and Other Indicators of Psychological Distress among U.S. and Canadian Medical Students. Acad. Med. 2006, 81, 354–373. [Google Scholar] [CrossRef] [PubMed]
- Hooper, M.W.; Nápoles, A.M.; Pérez-Stable, E.J. COVID-19 and Racial/Ethnic Disparities. JAMA 2020, 323, 2466. [Google Scholar] [CrossRef]
- Ng, Q.X.; Lim, D.Y.; Chee, K.T. Not all trauma is the same. Proc. Natl. Acad. Sci. USA 2020, 117, 25200. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, K.; Yagi, T. Happiness and Self-Determination—An Empirical Study in Japan. Rev. Behav. Econ. 2019, 6, 385–419. [Google Scholar] [CrossRef]
- Orsini, C.; Binnie, V.I.; Wilson, S.L. Determinants and outcomes of motivation in health professions education: A systematic review based on self-determination theory. J. Educ. Eval. Health Prof. 2016, 13, 19. [Google Scholar] [CrossRef] [PubMed]
- Nioi, M.; Napoli, P.E.; Finco, G.; Demontis, R.; Fossarello, M.; D’aloja, E. Fear of the COVID-19 and medical liability. Insights from a series of 130 consecutives medico-legal claims evaluated in a single insti-tution during SARS-CoV-2-related pandemic. Signa Vitae 2021, 17, 79–85. [Google Scholar]
- Mushtaq, R. Relationship Between Loneliness, Psychiatric Disorders and Physical Health ? A Review on the Psychological Aspects of Loneliness. J. Clin. Diagn. Res. 2014, 8, WE01–WE04. [Google Scholar] [CrossRef]
- Puyat, J.H.; Kazanjian, A.; Wong, H.; Goldner, E. Comorbid Chronic General Health Conditions and Depression Care: A Population-Based Analysis. Psychiatr. Serv. 2017, 68, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Shek, D. A longitudinal study of perceived family functioning and adolescent adjustment in Chinese adolescents with economic disadvantage. J. Fam. 2005, 26, 518–543. [Google Scholar] [CrossRef]
- Yang, J.; Yang, Y.; Liu, X.; Tian, J.; Zhu, X.; Miao, D. Self-efficacy, social support, and coping strate-gies of adolescent earthquake survivors in China. Soc. Behav. Personal. Int. J. 2010, 38, 1219–1228. [Google Scholar] [CrossRef]
- Hoare, E.; Milton, K.; Foster, C.; Allender, S. The associations between sedentary behaviour and mental health among adolescents: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–22. [Google Scholar] [CrossRef] [Green Version]
- McNicol, M.L.; Thorsteinsson, E.B. Internet Addiction, Psychological Distress, and Coping Responses Among Adolescents and Adults. Cyberpsychol. Behav. Soc. Netw. 2017, 20, 296–304. [Google Scholar] [CrossRef] [Green Version]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Foubert, J.; Nixon, M.L.; Sisson, V.S.; Barnes, A.C. A longitudinal study of chickering and Reisser’s vectors: Exploring gender differences and implications for refining the theory. J. Coll. Stud. Dev. 2005, 46, 461–471. [Google Scholar] [CrossRef]
- Ng, Q.X.; Chee, K.T.; De Deyn, M.L.Z.Q.; Chua, Z. Staying connected during the COVID-19 pandemic. Int. J. Soc. Psychiatry 2020, 66, 519–520. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Number | Percentage |
|---|---|---|
| Gender | ||
| Male | 48 | 21.5 |
| Female | 175 | 78.5 |
| Age, years | ||
| 20 | 92 | 41.3 |
| 21 | 103 | 46.2 |
| 22 | 24 | 10.8 |
| 23 | 3 | 1.3 |
| 24 | 1 | 0.4 |
| Year of university | ||
| Third | 121 | 54.3 |
| Fourth | 102 | 45.7 |
| Place of residence | ||
| alert region * | 197 | 88.3 |
| Non-alert region | 26 | 11.7 |
| Household members | ||
| One | 81 | 36.3 |
| Two or more | 142 | 63.7 |
| Economic situation | ||
| Same as usual | 112 | 50.2 |
| Worse than usual | 91 | 40.8 |
| Better than usual | 20 | 9.0 |
| Communication with family | ||
| Same as usual | 86 | 38.6 |
| Less than usual | 11 | 4.9 |
| More than usual | 126 | 56.5 |
| Communication with friends | ||
| Same as usual | 22 | 9.9 |
| Less than usual | 192 | 86.1 |
| More than usual | 9 | 4.0 |
| Total | Gender | Year of University | Household Members | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Measurements | Male | Female | p Value | Third | Fourth | p Value | One | Two or More | p Value | |
| GHQ-12 | 5 (3-8) | 5 (2–7) | 6 (3–8) | 0.26 | 5 (2–8) | 6 (3–8) | 0.22 | 6 (3–8) | 5 (3–8) | 0.25 |
| Anxiety over COVID-19 | 8 (7–10) | 7 (5.75–9) | 8 (7–10) | 0.001 | 8 (7–10) | 8 (7–9) | 0.19 | 8 (7–9) | 8 (7–10) | 0.35 |
| Health condition | 8 (6–10) | 8 (7–10) | 8 (6–9) | 0.15 | 8 (6–9) | 8 (7–10) | 0.49 | 7 (5–8) | 7 (5–9) | 0.80 |
| Self-determination score | 7 (5–9) | 7 (4.75–9) | 7 (5–9) | 0.33 | 8 (5–9) | 7 (5–9) | 0.44 | 7 (5–9) | 7 (5–9) | 0.67 |
| Satisfaction with daily life | ||||||||||
| Leisure | 3 (1–4) | 2.5 (1–5) | 3 (1–4) | 0.72 | 3 (2–5) | 2 (1–4) | 0.02 | 3 (1–4) | 3 (2–5) | 0.21 |
| Study | 4 (2–6) | 4 (2–7) | 4 (2–6) | 0.46 | 4 (2–7) | 3.5 (2–5) | 0.15 | 3 (2–6) | 4 (2.25–6) | 0.03 |
| Daily-life activities | 4 (3–7) | 6 (3–7) | 4 (3–6) | 0.04 | 4 (3–7) | 4 (3–6.75) | 0.92 | 4 (3–6) | 4 (3–7) | 0.46 |
| New activities | 6 (2–8) | 6 (3–8) | 6 (2–8) | 0.24 | 7 (3–8) | 6 (1–8) | 0.08 | 6(1–8) | 7 (3.25–8) | 0.03 |
| Normal (n = 65) | Poor (n = 158) | |
|---|---|---|
| Gender | ||
| Male | 18 (27.7) | 30 (19.0) |
| Female | 47 (72.3) | 128 (81.0) |
| Age, years | ||
| 20 | 30 (46.2) | 62 (39.2) |
| 21 | 27 (41.5) | 76 (48.1) |
| 22 | 6 (9.2) | 18 (11.4) |
| 23 | 2 (3.1) | 1 (0.6) |
| 24 | 0 (0.0) | 1 (0.6) |
| Year of university | ||
| Third | 38 (58.5) | 83 (52.5) |
| Fourth | 27 (41.5) | 75 (47.5) |
| Place of residence | ||
| Alert region * | 54 (83.1) | 144 (91.1) |
| Non-alert region | 11 (16.9) | 14 (8.9) |
| Household members | ||
| One | 21 (32.3) | 60 (38.0) |
| Two or more | 44 (67.7) | 98 (62.0) |
| Economic situation | ||
| Same as usual | 39 (60.0) | 73 (46.2) |
| Worse than usual | 20 (30.8) | 71 (44.9) |
| Better than usual | 6 (9.2) | 14 (8.9) |
| Communication with family | ||
| Same as usual | 28 (43.1) | 58 (36.7) |
| Less than usual | 2 (3.1) | 9 (5.7) |
| More than usual | 35 (53.8) | 91 (57.6) |
| Communication with friends | ||
| Same as usual | 15 (23.1) | 7 (4.4) |
| Less than usual | 48 (73.8) | 144 (91.1) |
| More than usual | 2 (3.1) | 7 (4.4) |
| Normal Mental Health Status | Poor Mental Health Status | p Value | |
|---|---|---|---|
| GHQ-12 score | 2 (0–2) | 7 (5–9) | <0.001 |
| Anxiety about COVID-19 | 8 (6–9) | 8 (7–10) | 0.03 |
| Health status | 9 (8–10) | 8 (5–9) | <0.001 |
| Self-determination score | 8 (6–9) | 7 (5–9) | 0.04 |
| Satisfaction with daily life | |||
| Leisure | 4 (3–7) | 2 (1–3) | <0.001 |
| Study | 5 (3–7) | 4 (2–6) | 0.001 |
| Daily-life activities | 6 (4–8) | 4 (3–6) | <0.001 |
| New activities | 7 (6–9) | 6 (1–8) | <0.001 |
| p Value | ||||
|---|---|---|---|---|
| Number of Respondents with Poor Mental Health/Number of Responses (%) | Adjusted OR (95%CI) | Category | Overall | |
| Communication with friends | 0.03 | |||
| Same as usual | 7/22 (31.8) | 1 [Reference] | NA | |
| Less than usual | 144/152 (94.7) | 5.38 (1.54–18.83) | 0.008 | |
| More than usual | 7/9 (77.8) | 5.45 (0.69–43.32) | 0.11 | |
| Health condition | 0.68 (0.55–0.83) | <0.001 | ||
| Satisfaction with leisure | 0.68 (0.58–0.79) | <0.001 | ||
| Satisfaction with new activities | 0.88 (0.78–0.99) | 0.04 | ||
| Adjusted for health condition, satisfaction with leisure, satisfaction with study, satisfaction with daily-life activities, satisfaction with new activities, communication with friends, communication with family, anxiety about COVID-19, self-determination score, household members, gender, age, year of university, and economic situation, as appropriate. | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tahara, M.; Mashizume, Y.; Takahashi, K. Mental Health Crisis and Stress Coping among Healthcare College Students Momentarily Displaced from Their Campus Community Because of COVID-19 Restrictions in Japan. Int. J. Environ. Res. Public Health 2021, 18, 7245. https://doi.org/10.3390/ijerph18147245
Tahara M, Mashizume Y, Takahashi K. Mental Health Crisis and Stress Coping among Healthcare College Students Momentarily Displaced from Their Campus Community Because of COVID-19 Restrictions in Japan. International Journal of Environmental Research and Public Health. 2021; 18(14):7245. https://doi.org/10.3390/ijerph18147245
Chicago/Turabian StyleTahara, Masatoshi, Yuki Mashizume, and Kayoko Takahashi. 2021. "Mental Health Crisis and Stress Coping among Healthcare College Students Momentarily Displaced from Their Campus Community Because of COVID-19 Restrictions in Japan" International Journal of Environmental Research and Public Health 18, no. 14: 7245. https://doi.org/10.3390/ijerph18147245
APA StyleTahara, M., Mashizume, Y., & Takahashi, K. (2021). Mental Health Crisis and Stress Coping among Healthcare College Students Momentarily Displaced from Their Campus Community Because of COVID-19 Restrictions in Japan. International Journal of Environmental Research and Public Health, 18(14), 7245. https://doi.org/10.3390/ijerph18147245