
High Risk of Hip and Spinal Fractures after Distal Radius Fracture: A Longitudinal Follow-Up Study Using a National Sample Cohort


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Study Design
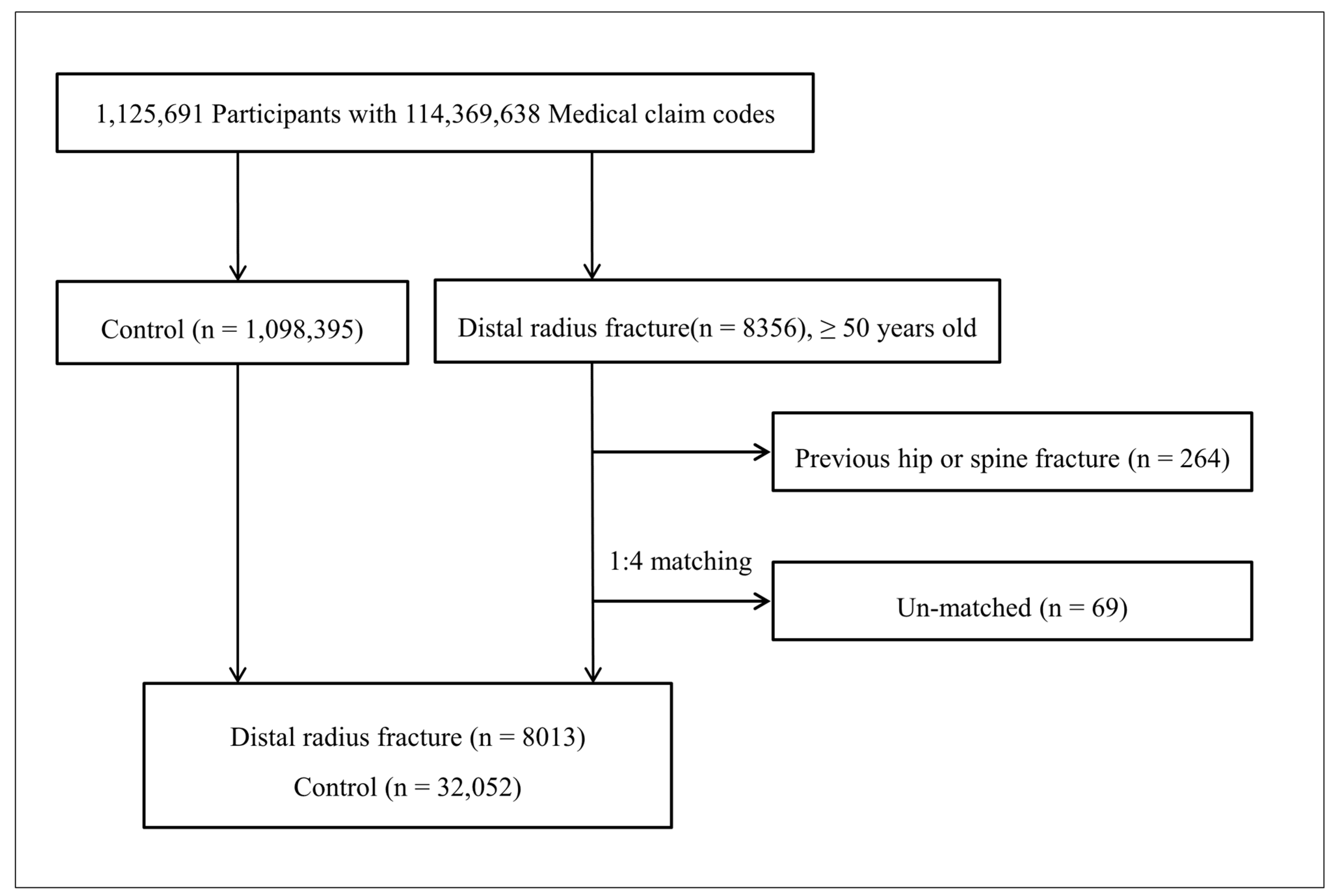
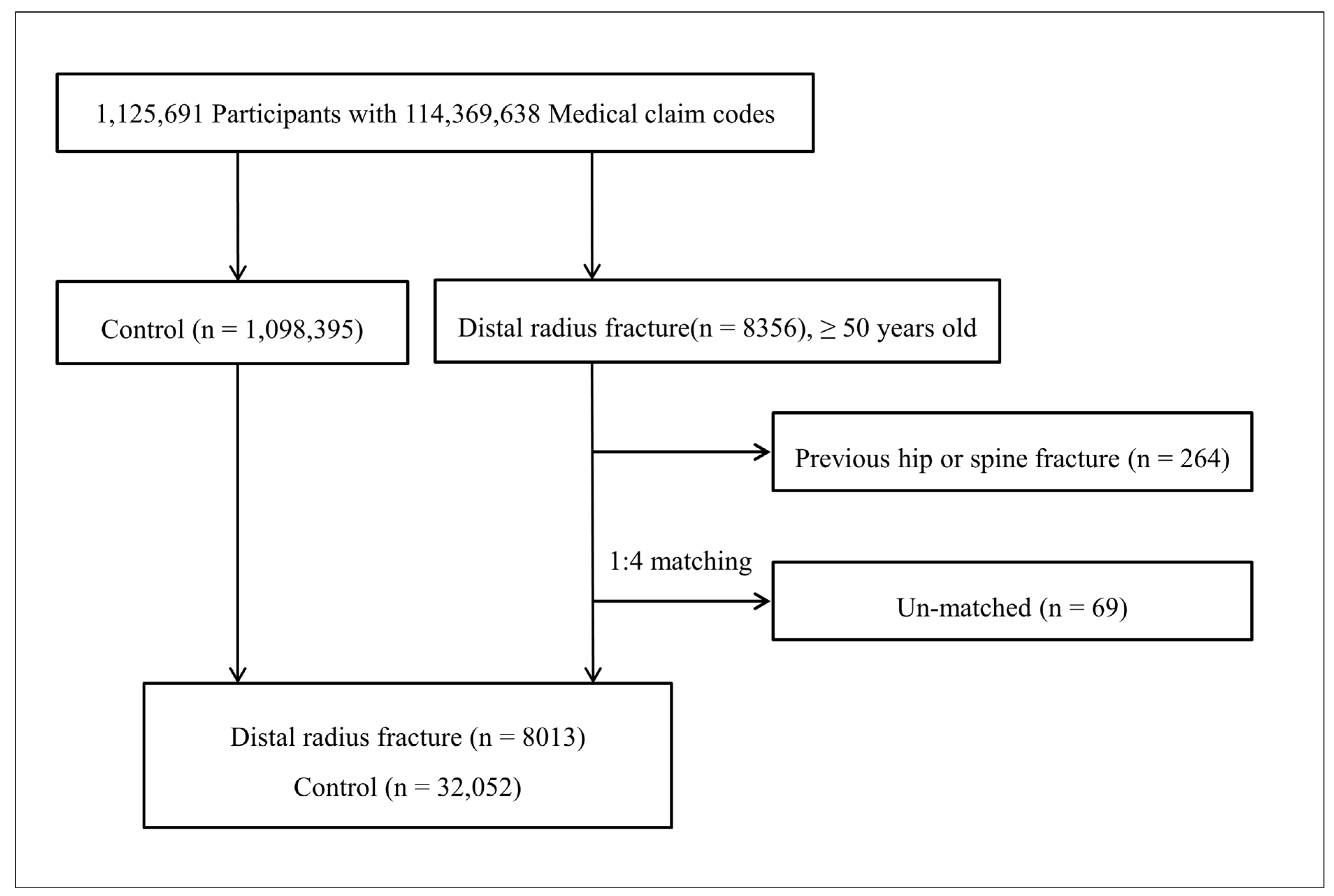
2.3. Participant Selection
2.4. Variables
2.4.1. Independent Variable
2.4.2. Covariate Analysis
2.4.3. Dependent Variable
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nellans, K.W.; Kowalski, E.; Chung, K.C. The epidemiology of distal radius fractures. Hand Clin. 2012, 28, 113–125. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.Y.; Ha, Y.-C.; Kim, T.-Y.; Cho, H.; Lee, Y.-K.; Baek, J.-Y.; Jang, S. Healthcare costs of osteoporotic fracture in Korea: Information from the national health insurance claims database, 2008–2011. J. Bone Metab. 2017, 24, 125–133. [Google Scholar] [CrossRef] [Green Version]
- Edwards, B.J.; Song, J.; Dunlop, D.D.; Fink, H.A.; Cauley, J.A. Functional decline after incident wrist fractures--Study of osteoporotic fractures: Prospective cohort study. Bmj 2010, 341, c3324. [Google Scholar] [CrossRef] [Green Version]
- Rozental, T.D.; Branas, C.C.; Bozentka, D.J.; Beredjiklian, P.K. Survival among elderly patients after fractures of the distal radius. J. Hand Surg. 2002, 27, 948–952. [Google Scholar] [CrossRef]
- Johnell, O.; Kanis, J.A.; Oden, A.; Sernbo, I.; Redlund-Johnell, I.; Petterson, C.; De Laet, C.; Jönsson, B. Mortality after osteoporotic fractures. Osteoporos. Int. 2004, 15, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Kwon, G.-D.; Jang, S.; Lee, A.; Park, C.-M.; Lee, Y.-K.; Kim, T.-Y.; Kim, H.-Y.; Park, E.-J.; Ha, Y.-C. Incidence and mortality after distal radius fractures in adults aged 50 years and older in Korea. J. Korean Med. Sci. 2016, 31, 630–634. [Google Scholar] [CrossRef]
- Øyen, J.; Diamantopoulos, A.P.; Haugeberg, G. Mortality after distal radius fracture in men and women aged 50 years and older in southern Norway. PLoS ONE 2014, 9, e112098. [Google Scholar] [CrossRef] [PubMed]
- Morin, S.; Lix, L.M.; Azimaee, M.; Metge, C.; Caetano, P.; Leslie, W.D. Mortality rates after incident non-traumatic fractures in older men and women. Osteoporos. Int. 2011, 22, 2439–2448. [Google Scholar] [CrossRef]
- Lyles, K.W.; Schenck, A.P.; Colón-Emeric, C.S. Hip and other osteoporotic fractures increase the risk of subsequent fractures in nursing home residents. Osteoporos. Int. 2008, 19, 1225–1233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanis, J.A.; Johnell, O.; De Laet, C.; Johansson, H.; Odén, A.; Delmas, P.; Eisman, J.; Fujiwara, S.; Garnero, P.; Kroger, H.; et al. A meta-analysis of previous fracture and subsequent fracture risk. Bone 2004, 35, 375–382. [Google Scholar] [CrossRef]
- Hodsman, A.B.; Leslie, W.D.; Tsang, J.F.; Gamble, G.D. 10-year probability of recurrent fractures following wrist and other osteoporotic fractures in a large clinical cohort: An analysis from the Manitoba Bone Density Program. Arch. Intern. Med. 2008, 168, 2261–2267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bynum, J.P.W.; Bell, J.-E.; Cantu, R.V.; Wang, Q.; McDonough, C.M.; Carmichael, D.; Tosteson, T.D.; Tosteson, A.N.A. Second fractures among older adults in the year following hip, shoulder, or wrist fracture. Osteoporos. Int. 2016, 27, 2207–2215. [Google Scholar] [CrossRef] [PubMed]
- Haentjens, P.; Autier, P.; Collins, J.; Velkeniers, B.; Vanderschueren, D.; Boonen, S. Colles fracture, spine fracture, and subsequent risk of hip fracture in men and women: A meta-analysis. JBJS 2003, 85, 1936–1943. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-W.; Huang, T.-L.; Su, L.-T.; Kuo, Y.-C.; Wu, S.-C.; Li, C.-Y.; Chen, K.-B.; Sung, F.-C. Incidence of subsequent hip fractures is significantly increased within the first month after distal radius fracture in patients older than 60 years. J. Trauma Acute Care Surg. 2013, 74, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Lauritzen, J.B.; Schwarz, P.; McNair, P.; Lund, B.; Transbøl, I. Radial and humeral fractures as predictors of subsequent hip, radial or humeral fractures in women, and their seasonal variation. Osteoporos. Int. 1993, 3, 133–137. [Google Scholar] [CrossRef]
- Owen, R.A.; Melton, L.J., 3rd; Ilstrup, D.M.; Johnson, K.A.; Riggs, B.L. Colles’ fracture and subsequent hip fracture risk. Clin. Orthop. Relat. Res. 1982, 171, 37–43. [Google Scholar] [CrossRef]
- Mallmin, H.; Ljunghall, S.; Persson, I.; Naessén, T.; Krusemo, U.B.; Bergström, R. Fracture of the distal forearm as a forecaster of subsequent hip fracture: A population-based cohort study with 24 years of follow-up. Calcif. Tissue. Int. 1993, 52, 269–272. [Google Scholar] [CrossRef]
- Robinson, C.M.; Royds, M.; Abraham, A.; McQueen, M.M.; Court-Brown, C.M.; Christie, J. Refractures in patients at least forty-five years old: A prospective analysis of twenty-two thousand and sixty patients. JBJS 2002, 84, 1528–1533. [Google Scholar] [CrossRef] [Green Version]
- Cummings, S.R.; Nevitt, M.C.; Browner, W.S.; Stone, K.; Fox, K.M.; Ensrud, K.E.; Cauley, J.; Black, D.; Vogt, T.M.; M.P.H. for the Study of Osteoporotic Fractures Research Group. Risk factors for hip fracture in white women. N. Engl. J. Med. 1995, 332, 767–773. [Google Scholar] [CrossRef]
- Schousboe, J.T.; Fink, H.A.; Taylor, B.C.; Stone, K.L.; Hillier, T.A.; Nevitt, M.C.; Ensrud, K.E. Association between self-reported prior wrist fractures and risk of subsequent hip and radiographic vertebral fractures in older women: A prospective study. J. Bone Miner. Res. 2005, 20, 100–106. [Google Scholar] [CrossRef]
- Cuddihy, M.-T.; Gabriel, S.E.; Crowson, C.S.; O’Fallon, W.M.; Melton, L.J., 3rd. Forearm fractures as predictors of subsequent osteoporotic fractures. Osteoporo. Int. 1999, 9, 469–475. [Google Scholar] [CrossRef]
- Gunnes, M.; Mellström, D.; Johnell, O. How well can a previous fracture indicate a new fracture? A questionnaire study of 29,802 postmenopausal women. Acta Orthop. Scand. 1998, 69, 508–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crandall, C.J.; Hovey, K.M.; Cauley, J.A.; Andrews, C.A.; Curtis, J.R.; Wactawski-Wende, J.; Wright, N.C.; Li, W.; LeBoff, M.S. Wrist fracture and risk of subsequent fracture: Findings from the women’s health initiative study. J. Bone Miner. Res. 2015, 30, 2086–2095. [Google Scholar] [CrossRef] [PubMed]
- Barrett-Connor, E.; Sajjan, S.G.; Siris, E.S.; Miller, P.D.; Chen, Y.T.; Markson, L.E. Wrist fracture as a predictor of future fractures in younger versus older postmenopausal women: Results from the National Osteoporosis Risk Assessment (NORA). Osteoporos. Int. 2008, 19, 607–613. [Google Scholar] [CrossRef]
- Van Staa, T.P.; Leufkens, H.G.M.; Cooper, C. Does a fracture at one site predict later fractures at other sites? A British cohort study. Osteoporos. Int. 2002, 13, 624–629. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Kong, I.G.; Lim, H.; Choi, H.G. Increased risk of sudden sensory neural hearing loss in osteoporosis: A longitudinal follow-up study. J. Clin. Endocrinol. Metab. 2018, 103, 3103–3109. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Lee, J.K.; Oh, D.J.; Kong, I.G.; Choi, H.G. Depression and incident hip fracture: A longitudinal follow-up study using a national sample cohort. Medicine 2019, 98, e16268. [Google Scholar] [CrossRef]
- Lee, J.; Lee, J.S.; Park, S.-H.; Shin, S.A.; Kim, K. Cohort Profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef]
- Lee, S.-Y.; Kong, I.G.; Oh, D.J.; Choi, H.G. Increased risk of sudden sensory neural hearing loss in patients with rheumatoid arthritis: A longitudinal follow-up study using a national sample cohort. Clin. Rheumatol. 2019, 38, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.G.; Kim, J.-H.; Park, J.-Y.; Hwang, Y.I.; Jang, S.H.; Jung, K.-S. Association between asthma and depression: A national cohort study. J. Allergy Clin. Immunol. Pract. 2019, 7, 1239–1245.e1231. [Google Scholar] [CrossRef]
- Park, B.; Min, C.; Choi, H.G. Neck dissection does not increases the risk of stroke in thyroid cancer: A national cohort study. PLoS ONE 2018, 13, e0195074. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Lee, J.K.; Sim, S.; Choi, H.G. Hearing impairment increases the risk of distal radius, hip, and spine fractures: A longitudinal follow-up study using a national sample cohort. PLoS ONE 2018, 13, e0192820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasnich, R.D.; Davis, J.W.; Ross, P.D. Spine fracture risk is predicted by non-spine fractures. Osteoporos. Int. 1994, 4, 1–5. [Google Scholar] [CrossRef]
- Haentjens, P.; Johnell, O.; Kanis, J.A.; Bouillon, R.; Cooper, C.; Lamraski, G.; Vanderschueren, D.; Kaufman, J.M.; Boonen, S. Evidence from data searches and life-table analyses for gender-related differences in absolute risk of hip fracture after Colles’ or spine fracture: Colles’ fracture as an early and sensitive marker of skeletal fragility in white men. J. Bone Miner. Res. 2004, 19, 1933–1944. [Google Scholar] [CrossRef] [PubMed]
- Klotzbuecher, C.M.; Ross, P.D.; Landsman, P.B.; Abbott, T.A., III; Berger, M. Patients with prior fractures have an increased risk of future fractures: A summary of the literature and statistical synthesis. J. Bone Miner. Res. 2000, 15, 721–739. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.W.; Lee, Y.B.; Kwon, B.C.; Yoo, J.H.; Choi, H.G. Mortality and cause of death in distal radius fracture patients: A longitudinal follow-up study using a national sample cohort. Medicine 2019, 98, e18604. [Google Scholar] [CrossRef]
- Sharifi, M.D.; Mohebbi, M.; Farrokhfar, M.; Farzaneh, R.; Disfani, H.F.; Hashemian, A.M. Analysis of correlation between estradiol and fracture of femur neck. Eur. J. Transl. Myol. 2018, 28, 7379. [Google Scholar] [CrossRef] [PubMed]
- Behrouzi, A.; Hejazi, H.; Kamali, A.; Hadi, H. Investigation of the outcome of patients with hip fractures using vitamin D3. Eur. J. Transl. Myol. 2018, 28, 7372. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.-Y.; Park, Y.-J.; Park, J.-S. A meta-analysis of studies of volar locking plate fixation of distal radius fractures: Conventional versus minimally invasive plate osteosynthesis. Clin. Orthop. Surg. 2019, 11, 208–219. [Google Scholar] [CrossRef]
- Kanis, J.A.; Johansson, H.; Odén, A.; Harvey, N.C.; Gudnason, V.; Sanders, K.M.; Sigurdsson, G.; Siggeirsdottir, K.; Fitzpatrick, L.A.; Borgström, F.; et al. Characteristics of recurrent fractures. Osteoporos. Int. 2018, 29, 1747–1757. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Distal Radius Fracture | ||||
|---|---|---|---|---|---|
| Fracture (n, %) | Control (n, %) | p-Value | |||
| Age (years) | 1.000 | ||||
| 50–54 | 1297 (16.2) | 5188 (16.2) | |||
| 55–59 | 1598 (19.9) | 6392 (19.9) | |||
| 60–64 | 1469 (18.3) | 5876 (18.3) | |||
| 65–69 | 1423 (17.8) | 5692 (17.8) | |||
| 70–74 | 1035 (12.9) | 4140 (12.9) | |||
| 75–79 | 581 (7.3) | 2324 (7.3) | |||
| 80–84 | 385 (4.8) | 1540 (4.8) | |||
| 85+ | 225 (2.8) | 900 (2.8) | |||
| Sex | 1.000 | ||||
| Male | 1533 (19.1) | 6132 (19.1) | |||
| Female | 6480 (80.9) | 25,920 (80.9) | |||
| Income | 1.000 | ||||
| 1 (lowest) | 84 (1.0) | 336 (1.0) | |||
| 2 | 722 (9.0) | 2888 (9.0) | |||
| 3 | 578 (7.2) | 2312 (7.2) | |||
| 4 | 557 (7.0) | 2228 (7.0) | |||
| 5 | 545 (6.8) | 2180 (6.8) | |||
| 6 | 662 (8.3) | 2648 (8.3) | |||
| 7 | 687 (8.6) | 2748 (8.6) | |||
| 8 | 788 (9.8) | 3152 (9.8) | |||
| 9 | 977 (12.2) | 3908 (12.2) | |||
| 10 | 1136 (14.2) | 4544 (14.2) | |||
| 11 (highest) | 1277 (15.9) | 5108 (15.9) | |||
| Region of residence | 1.000 | ||||
| Urban | 3592 (44.8) | 14,368 (44.8) | |||
| Rural | 4421 (55.2) | 17,684 (55.2) | |||
| Hypertension | 4673 (58.3) | 18,692 (58.3) | 1.000 | ||
| Diabetes mellitus | 2225 (27.8) | 8900 (27.8) | 1.000 | ||
| Dyslipidemia | 2855 (35.6) | 11,420 (35.6) | 1.000 | ||
| Ischemic heart disease | 780 (9.7) | 3152 (9.8) | 0.788 | ||
| Cerebral stroke | 1526 (19.0) | 5741 (17.9) | 0.018 * | ||
| Depression | 1099 (13.7) | 3833 (12.0) | <0.001 * | ||
| Osteoporosis | 3946 (49.2) | 12,981 (40.5) | <0.001 * | ||
| Hip fracture | 262 (3.3) | 661 (2.1) | <0.001 * | ||
| Age 50–59 y | 22 (0.8) | 42 (0.4) | 0.004 * | ||
| Age 60–69 y | 52 (1.8) | 163 (1.4) | 0.122 | ||
| Age 70+ y | 188 (8.4) | 456 (5.1) | <0.001 * | ||
| Spinal fracture | 812 (10.1) | 2167 (6.8) | <0.001 * | ||
| Age 50–59 y | 141 (4.9) | 261 (2.3) | <0.001 * | ||
| Age 60–69 y | 310 (10.7) | 846 (7.3) | <0.001 * | ||
| Age 70+ y | 361 (16.2) | 1060 (11.9) | <0.001 * | ||
| Fracture | Distal Radius Fracture | ||||
|---|---|---|---|---|---|
| Crude † | p-Value | Adjusted †‡ | p-Value | ||
| Hip fracture | <0.001 * | <0.001 * | |||
| Yes | 1.61 (1.40–1.86) | 1.51 (1.30–1.74) | |||
| No | 1.00 | 1.00 | |||
| Spinal fracture | <0.001 * | <0.001 * | |||
| Yes | 1.55 (1.43–1.6) | 1.40 (1.29–1.52) | |||
| No | 1.00 | 1.00 | |||
| Fracture | Distal Radius Fracture | ||||||
|---|---|---|---|---|---|---|---|
| 50–59 y (n = 3470) | 60–69 y (n = 2570) | 70+ y (n = 1625) | |||||
| Adjusted †‡ | p-value | Adjusted †‡ | p-value | Adjusted †‡ | p-value | ||
| Hip fracture | |||||||
| Male | 0.002 * | <0.001 * | <0.001 * | ||||
| Yes | 5.81 (1.94–17.36) | 3.23 (1.70–6.16) | 3.42 (1.95–6.00) | ||||
| No | 1.00 | 1.00 | 1.00 | ||||
| Female | 0.198 | 0.521 | <0.001 * | ||||
| Yes | 1.51 (0.80–2.84) | 0.88 (0.60–1.29) | 1.45 (1.21–1.74) | ||||
| No | 1.00 | 1.00 | 1.00 | ||||
| Spinal fracture | |||||||
| Male | <0.001 * | <0.001 * | 0.229 | ||||
| Yes | 3.00 (1.71–5.23) | 2.37 (1.48–3.80) | 1.35 (0.83–2.18) | ||||
| No | 1.00 | 1.00 | 1.00 | ||||
| Female | <0.001 * | <0.001 * | <0.001 * | ||||
| Yen | 1.78 (1.41–2.23) | 1.33 (1.16–1.53) | 1.27 (1.12–1.44) | ||||
| No | 1.00 | 1.00 | 1.00 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, H.-G.; Kim, D.-S.; Lee, B.; Youk, H.; Lee, J.-W. High Risk of Hip and Spinal Fractures after Distal Radius Fracture: A Longitudinal Follow-Up Study Using a National Sample Cohort. Int. J. Environ. Res. Public Health 2021, 18, 7391. https://doi.org/10.3390/ijerph18147391
Choi H-G, Kim D-S, Lee B, Youk H, Lee J-W. High Risk of Hip and Spinal Fractures after Distal Radius Fracture: A Longitudinal Follow-Up Study Using a National Sample Cohort. International Journal of Environmental Research and Public Health. 2021; 18(14):7391. https://doi.org/10.3390/ijerph18147391
Chicago/Turabian StyleChoi, Hyo-Geun, Doo-Sup Kim, Bumseok Lee, Hyun Youk, and Jung-Woo Lee. 2021. "High Risk of Hip and Spinal Fractures after Distal Radius Fracture: A Longitudinal Follow-Up Study Using a National Sample Cohort" International Journal of Environmental Research and Public Health 18, no. 14: 7391. https://doi.org/10.3390/ijerph18147391
APA StyleChoi, H.-G., Kim, D.-S., Lee, B., Youk, H., & Lee, J.-W. (2021). High Risk of Hip and Spinal Fractures after Distal Radius Fracture: A Longitudinal Follow-Up Study Using a National Sample Cohort. International Journal of Environmental Research and Public Health, 18(14), 7391. https://doi.org/10.3390/ijerph18147391