
The Association between Loneliness, Mental Well-Being, and Self-Esteem among Adolescents in Four Nordic Countries

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Participants
2.3. Measures
2.4. Statistical Analysis
3. Results
3.1. Prevalence of Loneliness, Mental Wellbeing, and High Self-Esteem
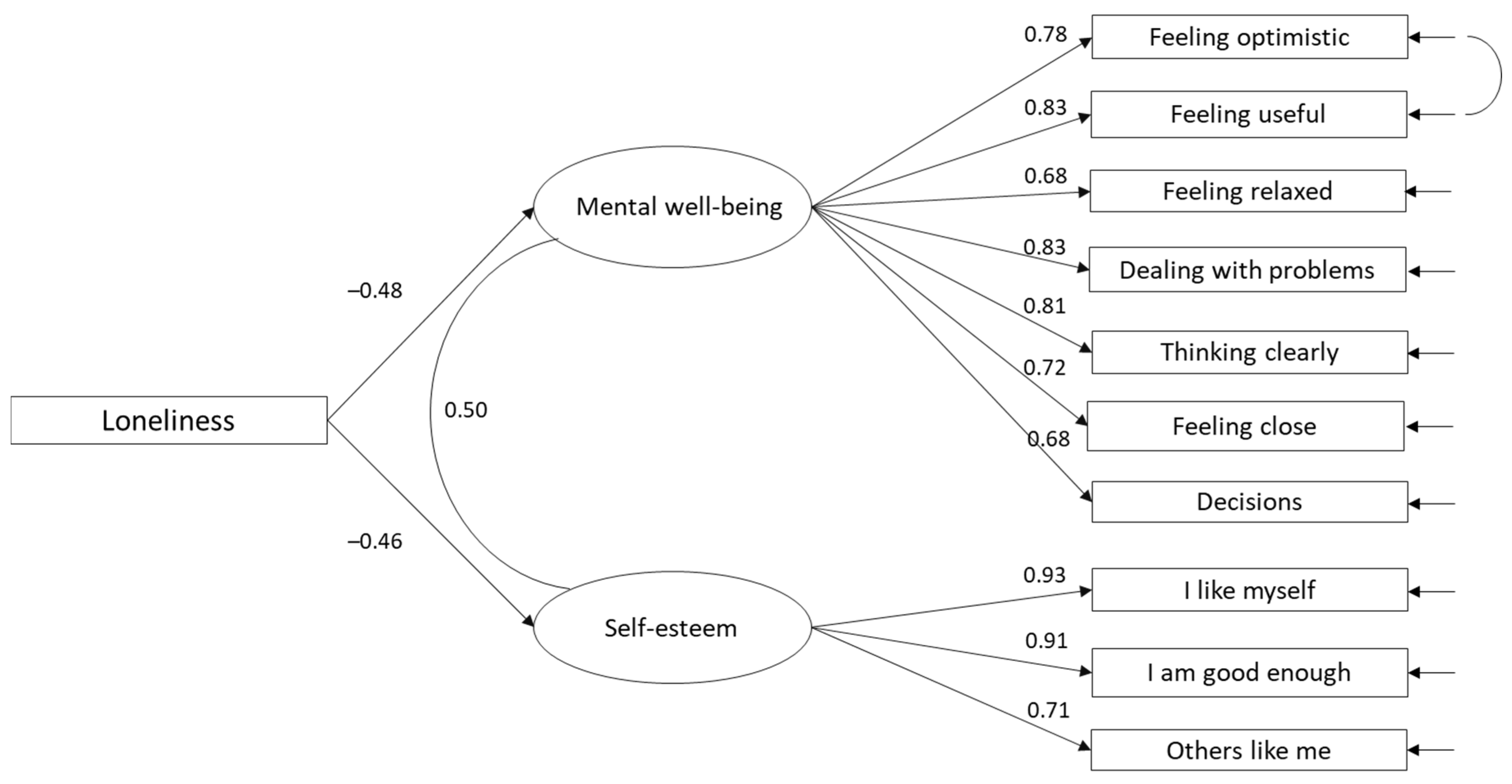
3.2. Relationships between Loneliness and Positive Mental Health
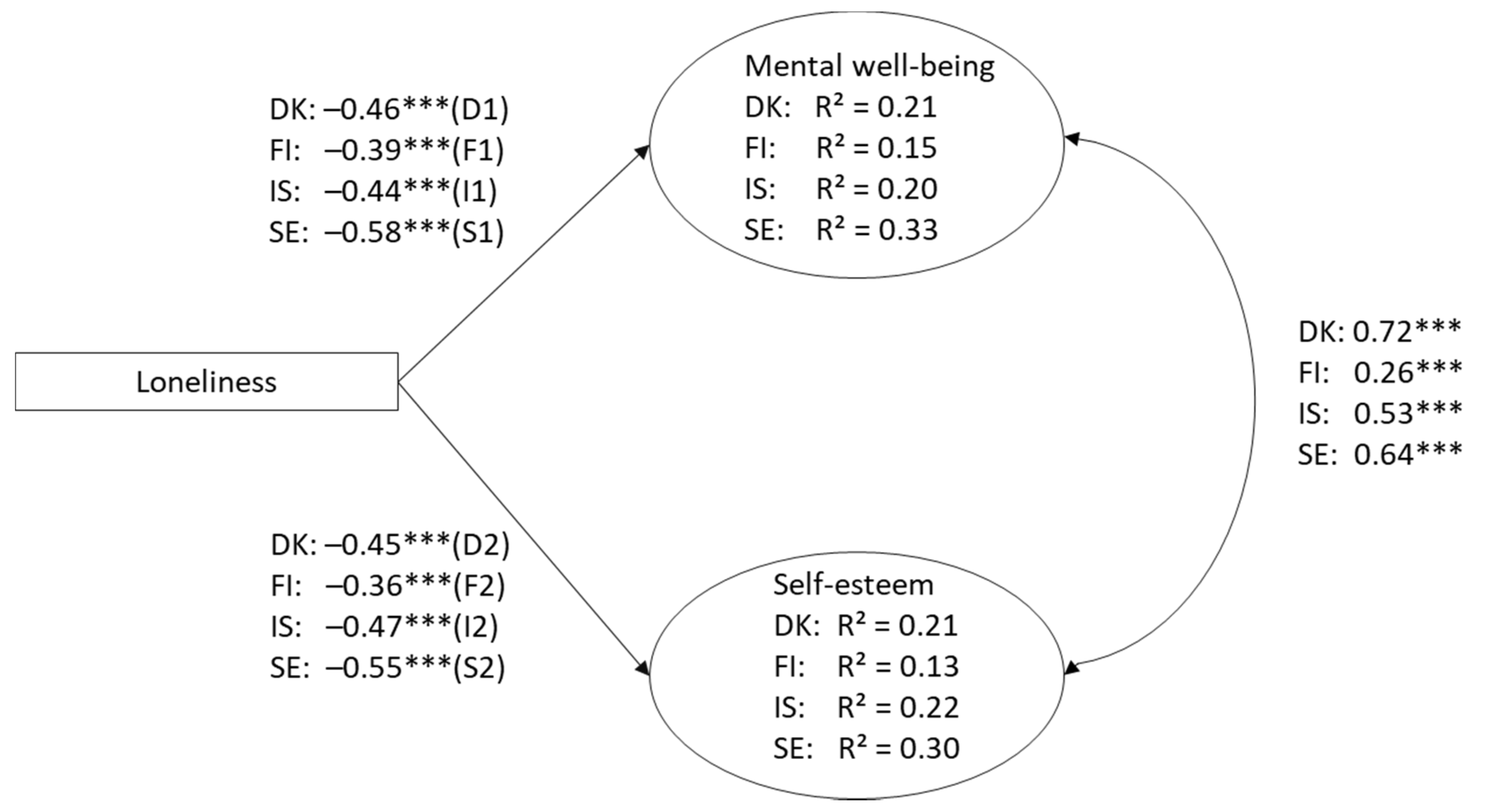
3.3. Country-Level Differences in Loneliness and Mental Health
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Qualter, P.; Brown, S.L.; Rotenberg, K.J.; Vanhalst, J.; Harris, R.A.; Goossens, L.; Bangee, M.; Munn, P. Trajectories of loneliness during childhood and adolescence: Predictors and health outcomes. J. Adolesc. 2013, 36, 1283–1293. [Google Scholar] [CrossRef] [PubMed]
- Orban, A.; Tomova, L.; Blakemore, S.-J. The effects of social deprivation on adolescent development and mental health. Lancet Child Adolesc. Health 2020, 4, 634–640. [Google Scholar] [CrossRef]
- Laursen, B.; Hartl, A.C. Understanding loneliness during adolescence: Developmental changes that increase the risk of perceived social isolation. J. Adolesc. 2013, 36, 1261–1268. [Google Scholar] [CrossRef]
- Peplau, L.A.; Perlman, D. Perspectives on loneliness. In Loneliness: A Sourcebook of Current Theory Research and Therapy; Peplau, L.A., Perlman, D., Eds.; John Wiley: New York, NY, USA, 1982; pp. 1–18. [Google Scholar]
- Cacioppo, S.; Grippo, A.J.; London, S.; Goossens, L.; Cacioppo, J.T. Loneliness: Clinical import and interventions. Perspect. Psychol. Sci. 2015, 10, 238–249. [Google Scholar] [CrossRef] [Green Version]
- Hawkley, L.C.; Cacioppo, J.T. Loneliness Matters: A Theoretical and Empirical Review of Consequences and Mechanisms. Ann. Behav. Med. 2010, 40, 218–227. [Google Scholar] [CrossRef] [Green Version]
- Van Dulmen, M.H.M.; Goossens, L. Loneliness trajectories. J. Adolesc. 2013, 36, 1247–1249. [Google Scholar] [CrossRef]
- Eccles, A.M.; Qualter, P.; Madsen, K.R.; Holstein, B.E. Loneliness in the lives of Danish adolescents: Associations with health and sleep. Scand. J. Public Health 2020, 48, 877–887. [Google Scholar] [CrossRef]
- Lyyra, N.; Välimaa, R.; Tynjälä, J. Loneliness and subjective health complaints among school-aged children. Scand. J. Public Health 2018, 40 (Suppl. 20), 87–93. [Google Scholar] [CrossRef] [Green Version]
- Ladd, G.W.; Ettekal, I. Peer-related loneliness across early to late adolescence: Normative trends, intra-individual trajectories, and links with depressive symptoms. J. Adolesc. 2013, 36, 1269–1282. [Google Scholar] [CrossRef]
- Danneel, S.; Nelemans, S.; Spithoven, A.; Bastin, M.; Bijttebier, P.; Colpin, H.; Van Den Noortgate, W.; Van Leeuwen, K.; Verschueren, K.; Goossens, L. Internalizing Problems in Adolescence: Linking Loneliness, Social Anxiety Symptoms, and Depressive Symptoms Over Time. J. Abnorm. Child Psychol. 2019, 47, 1691–1705. [Google Scholar] [CrossRef] [PubMed]
- Loades, M.E.; Chatburn, E.; Higson-Sweeney, N.; Reynolds, S.; Shafran, R.; Brigden, A.; Linney, C.; Niamh McManus, M.; Borwick, C. Rapid Systematic Review: The Impact of Social Isolation and Loneliness on the Mental Health of Children and Adolescents in the Context of COVID-19. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 1218–1239. [Google Scholar] [CrossRef]
- Moksnes, U.K.; Bjørnsen, H.; Eilertsen, M.E.B.; Espnes, G.E. The role of perceived loneliness and sociodemographic factors in association with subjective mental and physical health and well-being in Norwegian adolescents. Scand. J. Public Health 2021. [Google Scholar] [CrossRef]
- Mushtaq, R.; Shoib, S.; Shah, T.; Mushtaq, S. Relationship between loneliness, psychiatric disorders and physical health? A review on the psychological aspects of loneliness. J. Clin. Diagn. Res. 2014, 8, WE01–WE04. [Google Scholar] [CrossRef]
- Harris, R.; Qualter, P.; Robinson, S. Loneliness trajectories from middle childhood to pre-adolescence: Impact on perceived health and sleep disturbance. J. Adolesc. 2013, 36, 1295–1304. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Promoting Mental Health: Concepts Emerging Evidence and Practice; Summary Report; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- Barry, M. Addressing the determinants of positive mental health: Concepts, evidence and practice. Int. J. Ment. Health Promot. 2009, 11, 4–17. [Google Scholar] [CrossRef] [Green Version]
- Eriksson, C.; Arnarsson, A.M.; Damsgaard, M.T.; Löfstedt, P.; Potrebny, T.; Suominen, S.; Thorsteinsson, E.B.; Torsheim, T.; Välimaa, R.; Due, P. Towards Enhancing Research on Adolescent Positive Mental Health. Nord. Welf. Res. 2019, 4, 113–128. [Google Scholar] [CrossRef] [Green Version]
- Stewart-Brown, S. The Warwick-Edinburgh Mental Well-Being Scale (WEMWBS): Performance in different cultural and geographical groups. In Mental Well-Being. International Contributions to the Study of Positive Mental Health; Keyes, C.L.M., Ed.; Springer: Dordrecht, The Netherlands, 2013; pp. 133–150. [Google Scholar]
- Blakemore, S.-J. Adolescence and mental health. Lancet 2019, 393, 2030–2031. [Google Scholar] [CrossRef]
- Guo, C.; Tomson, G.; Keller, C.; Söderqvist, F. Prevalence and correlates of positive mental health in Chinese adolescents. BMC Public Health 2018, 18, 263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keyes, C.L.M. The nature and importance of positive mental health in America’s adolescents. In Handbook of Positive Psychology in Schools; Gilman, R., Huebner, E.S., Furlong, M.J., Eds.; Routledge: New York, NY, USA, 2009; pp. 9–23. [Google Scholar]
- Centers for Disease Control and Prevention. Youth Behaviour Survey Data Summary & Trends Report: 2009–2019. Available online: https://www.cdc.gov/healthyyouth/data/yrbs/pdf/YRBSDataSummaryTrendsReport2019-508.pdf (accessed on 14 April 2021).
- Boden, J.M.; Fergusson, D.M.; Horwood, L.J. Does adolescent self-esteem predict later life outcomes? A test of the causal role of self-esteem. Dev. Psychopathol. 2008, 20, 319–339. [Google Scholar] [CrossRef]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Birkeland, M.S.; Melkevik, O.; Holsen, I.; Wold, B. Trajectories of global self-esteem development during adolescence. J. Adolesc. 2012, 35, 43–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanhalst, J.; Luyckx, K.; Scholte, R.H.; Engels, R.C.; Goossens, L. Low Self-Esteem as a Risk Factor for Loneliness in Adolescence: Perceived—but not Actual—Social Acceptance as an Underlying Mechanism. J. Abnorm. Child Psychol. 2013, 41, 1067–1081. [Google Scholar] [CrossRef]
- Heinrich, L.M.; Gullone, E. The clinical significance of loneliness: A literature review. Clin. Psychol. Rev. 2006, 26, 695–718. [Google Scholar] [CrossRef]
- Potrebny, T.; Torsheim, T.; Due, P.; Välimaa, R.; Suominen, S.; Eriksson, C. Trends in excellent self-rated health among adolescents: A comparative Nordic study. Nord. Welf. Res. 2019, 4, 67–76. [Google Scholar] [CrossRef] [Green Version]
- Eriksson, C.; Arnarsson, A.M.; Damsgaard, M.T.; Potrebny, T.; Suominen, S.; Torsheim, T.; Due, P. Building Knowledge of Adolescent Mental Health in the Nordic Countries. An introduction to a Nordic research collaboration. Nord. Welf. Res. 2019, 4, 43–53. [Google Scholar] [CrossRef] [Green Version]
- Schnohr, C.W.; Molcho, M.; Rasmussen, M.; Samdal, O.; de Looze, M.; Levin, K.; Roberts, C.J.; Ehlinger, V.; Krølner, R.; Dalmasso, P. Trend analyses in the health behaviour in school-aged children study: Methodological considerations and recommendations. Eur. J. Public Health 2015, 25, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Cavanaugh, A.M.; Buehler, C. Adolescent loneliness and social anxiety: The role of multiple sources of support. J. Soc. Pers. Relat. 2016, 33, 149–170. [Google Scholar] [CrossRef]
- Clarke, A.; Friede, T.; Putz, R.; Ashdown, J.; Martin, S.; Blake, A.; Adi, Y.; Parkinson, J.; Flynn, P.; Platt, S.; et al. Warwick-Edinburgh Mental Well-being Scale (WEMWBS): Validated for teenage school students in England and Scotland. A mixed methods assessment. BMC Public Health 2011, 11, 487. [Google Scholar] [CrossRef] [Green Version]
- McKay, M.T.; Andretta, J.R. Evidence for the Psychometric Validity, Internal Consistency and Measurement Invariance of Warwick Edinburgh Mental Well-being Scale Scores in Scottish and Irish Adolescents. Psychiatry Res. 2017, 255, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Rose, T.; Joe, S.; Williams, A.; Harris, R.; Betz, G.; Stewart-Brown, S. Measuring mental wellbeing among adolescents: A systematic review of instruments. J. Child. Fam. Stud. 2017, 26, 2349–2362. [Google Scholar] [CrossRef]
- Stewart-Brown, S.; Tennant, A.; Tennant, R.; Platt, S.; Parkinson, J.; Weich, S. Internal construct validity of the Warwick-Edinburgh Mental Well-being Scale (WEMWBS): A rasch analysis using data from the Scottish Health Education Population Survey. Health Qual. Life Outcomes 2009, 7, 15. [Google Scholar] [CrossRef] [Green Version]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 7th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2012. [Google Scholar]
- Bentler, P.M.; Bonett, D.G. Significance Tests and Goodness of Fit in the Analysis of Covariance Structures. Psychol. Bull. 1980, 88, 555–606. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cut-off criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Chen, F. Sensitivity of Goodness of Fit Indexes to Lack of Measurement Invariance. Struct. Equ. Model. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- Satorra, A.; Bentler, P.N. A scaled difference chi-square test statistic for moment structure analysis. Psychometrika 2001, 66, 507–514. [Google Scholar] [CrossRef] [Green Version]
- Borys, S.; Perlman, D. Gender differences in loneliness. Personal. Soc. Psychol. Bull. 1985, 11, 63–74. [Google Scholar] [CrossRef]
- Kerr, N.A.; Stanley, T.B. Revisiting the social stigma of loneliness. Personal. Individ. Differ. 2021, 171, 110482. [Google Scholar] [CrossRef]
- Bell, S.L.; Audrey, S.; Gunnell, D.; Cooper, A.; Campbell, R. The relationship between physical activity, mental wellbeing and symptoms of mental health disorder in adolescents: A cohort study. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haugland, S.; Wold, B. Subjective health complaints in adolescence—Reliability and validity of survey methods. J. Adolesc. 2001, 24, 611–624. [Google Scholar] [CrossRef] [Green Version]
- Asher, S.R.; Paquette, J.A. Loneliness and peer relations in childhood. Curr. Dir. Psychol. Sci. 2003, 12, 75–78. [Google Scholar] [CrossRef]
- Eccles, A.M.; Qualter, P. Review: Alleviating loneliness in young people—A meta-analysis of interventions. Child Adolesc. Ment. Health 2021, 26, 17–33. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Measure | All | Denmark | Finland | Iceland | Sweden | p d |
|---|---|---|---|---|---|---|
| Loneliness c | ||||||
| Feeling lonely | 14.3 | 7.7 | 19.2 | 17.1 | 11.9 | <0.001 |
| Mental well-being a | ||||||
| Feeling optimistic about the future | 62.4 | 76.7 | 46.4 | 59.4 | 69.2 | <0.001 |
| Feeling useful | 57.9 | 67.4 | 47.8 | 55.7 | 62.0 | <0.001 |
| Feeling relaxed | 54.3 | 61.5 | 48.0 | 49.5 | 60.9 | <0.001 |
| Dealing with problems well | 58.4 | 71.2 | 46.0 | 53.9 | 65.7 | <0.001 |
| Thinking clearly | 63.4 | 74.4 | 55.8 | 59.8 | 67.1 | <0.001 |
| Feeling close to other people | 65.9 | 75.6 | 59.1 | 61.9 | 70.5 | <0.001 |
| Able to make up my own mind | 67.3 | 88.4 | 68.5 | 48.6 | 80.6 | <0.001 |
| Self-esteem b | ||||||
| I like myself | 70.5 | 72.4 | 66.8 | 70.0 | 72.0 | 0.001 |
| I am good enough as I am | 67.8 | 71.5 | 66.2 | 66.0 | 69.3 | 0.003 |
| Others my age like me | 68.7 | 72.5 | 60.4 | 68.0 | 72.7 | <0.001 |
| Measure | All | Denmark | Finland | Iceland | Sweden | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Boys | Girls | p | Boys | Girls | p | Boys | Girls | p | Boys | Girls | p | Boys | Girls | p | |
| Loneliness c | |||||||||||||||
| Feeling lonely | 10.7 | 17.9 | *** | 5.6 | 9.9 | *** | 12.5 | 25.5 | *** | 13.7 | 19.6 | *** | 8.3 | 14.8 | *** |
| Mental well-being a | |||||||||||||||
| Feeling optimistic about the future | 67.4 | 57.7 | *** | 85.5 | 68.4 | *** | 47.5 | 45.3 | 62.9 | 56.7 | ** | 78.1 | 61.5 | *** | |
| Feeling useful | 64.8 | 51.3 | *** | 76.1 | 59.0 | *** | 52.9 | 42.7 | ** | 61.9 | 50.4 | *** | 71.2 | 54.1 | *** |
| Feeling relaxed | 63.8 | 45.2 | *** | 73.0 | 50.7 | *** | 57.3 | 38.9 | *** | 55.8 | 43.7 | *** | 74.9 | 48.6 | *** |
| Dealing with problems well | 65.6 | 51.7 | *** | 77.4 | 65.4 | ** | 53.8 | 38.2 | *** | 60.2 | 48.6 | *** | 75.1 | 57.4 | *** |
| Thinking clearly | 69.6 | 57.5 | *** | 82.0 | 67.3 | *** | 60.9 | 50.4 | ** | 65.0 | 55.7 | *** | 75.7 | 59.4 | *** |
| Feeling close to other people | 67.4 | 64.5 | 78.0 | 73.2 | 53.7 | 64.2 | ** | 62.8 | 61.8 | 78.0 | 64.0 | *** | |||
| Able to make up my own mind | 73.0 | 61.8 | *** | 89.5 | 87.3 | 68.4 | 68.5 | 58.6 | 39.5 | *** | 87.9 | 74.0 | *** | ||
| Self-esteem b | |||||||||||||||
| I like myself | 81.0 | 60.5 | *** | 84.9 | 60.6 | *** | 77.3 | 56.5 | *** | 79.4 | 61.7 | *** | 83.7 | 61.5 | *** |
| I am good enough as I am | 76.5 | 59.6 | *** | 82.0 | 61.5 | *** | 75.5 | 57.1 | *** | 72.7 | 59.8 | *** | 79.5 | 60.1 | *** |
| Others my age like me | 74.5 | 63.1 | *** | 79.3 | 66.0 | *** | 68.3 | 52.6 | *** | 72.6 | 64.0 | *** | 79.1 | 67.3 | *** |
| Item | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Loneliness | − | ||||||||||
| 2. Feeling optimistic about the future | −0.36 * | - | |||||||||
| 3. Feeling useful | −0.42 * | 0.72 * | − | ||||||||
| 4. Feeling relaxed | −0.32 * | 0.50 * | 0.55 * | − | |||||||
| 5. Dealing with problems well | −0.39 * | 0.61 * | 0.66 * | 0.59 * | − | ||||||
| 6. Thinking clearly | −0.37 * | 0.61 * | 0.63 * | 0.56 * | 0.72 * | − | |||||
| 7. Feeling close to other people | −0.33 * | 0.55 * | 0.59 * | 0.48 * | 0.57 * | 0.59 * | − | ||||
| 8. Able to make up my own mind | −0.33 * | 0.51 * | 0.54 * | 0.46 * | 0.57 * | 0.58 * | 0.51 * | − | |||
| 9. I like myself | −0.42 * | 0.47 * | 0.53 * | 0.37 * | 0.44 * | 0.43 * | 0.39 * | 0.36 * | − | ||
| 10. I am good enough as I am | −0.42 * | 0.43 * | 0.52 * | 0.36 * | 0.43 * | 0.42 * | 0.38 * | 0.35 * | 0.85 * | − | |
| 11. Others my age like me | −0.41 * | 0.39 * | 0.46 * | 0.31 * | 0.39 * | 0.36 * | 0.41 * | 0.32 * | 0.66 * | 0.64 * | − |
| M | 3.29 | 2.33 | 2.41 | 2.49 | 2.40 | 2.30 | 2.24 | 2.19 | 2.13 | 2.18 | 2.17 |
| SD | 0.85 | 1.02 | 0.98 | 0.99 | 0.96 | 0.96 | 0.99 | 1.03 | 1.05 | 1.08 | 0.95 |
| N | 5861 | 5753 | 5727 | 5740 | 5737 | 5723 | 5726 | 5725 | 5767 | 5753 | 5717 |
| Model | χ2(df) | p | CFI | TLI | RMSEA | SRMR |
|---|---|---|---|---|---|---|
| Separate models | ||||||
| Denmark | χ2(41) = 240.38 | <0.001 | 0.95 | 0.93 | 0.08 | 0.05 |
| Finland | χ2(41) = 194.89 | <0.001 | 0.97 | 0.96 | 0.06 | 0.03 |
| Iceland | χ2(41) = 218.45 | <0.001 | 0.98 | 0.97 | 0.04 | 0.03 |
| Sweden | χ2(41) = 353.54 | <0.001 | 0.95 | 0.94 | 0.07 | 0.05 |
| Country invariance | ||||||
| M1 | χ2(164) = 1005.38 | <0.001 | 0.97 | 0.96 | 0.06 | 0.04 |
| M2 | χ2(188) = 1242.01 | <0.001 | 0.96 | 0.95 | 0.06 | 0.06 |
| M3 | χ2(194) = 1294.31 | <0.001 | 0.96 | 0.95 | 0.06 | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lyyra, N.; Thorsteinsson, E.B.; Eriksson, C.; Madsen, K.R.; Tolvanen, A.; Löfstedt, P.; Välimaa, R. The Association between Loneliness, Mental Well-Being, and Self-Esteem among Adolescents in Four Nordic Countries. Int. J. Environ. Res. Public Health 2021, 18, 7405. https://doi.org/10.3390/ijerph18147405
Lyyra N, Thorsteinsson EB, Eriksson C, Madsen KR, Tolvanen A, Löfstedt P, Välimaa R. The Association between Loneliness, Mental Well-Being, and Self-Esteem among Adolescents in Four Nordic Countries. International Journal of Environmental Research and Public Health. 2021; 18(14):7405. https://doi.org/10.3390/ijerph18147405
Chicago/Turabian StyleLyyra, Nelli, Einar Baldvin Thorsteinsson, Charli Eriksson, Katrine Rich Madsen, Asko Tolvanen, Petra Löfstedt, and Raili Välimaa. 2021. "The Association between Loneliness, Mental Well-Being, and Self-Esteem among Adolescents in Four Nordic Countries" International Journal of Environmental Research and Public Health 18, no. 14: 7405. https://doi.org/10.3390/ijerph18147405
APA StyleLyyra, N., Thorsteinsson, E. B., Eriksson, C., Madsen, K. R., Tolvanen, A., Löfstedt, P., & Välimaa, R. (2021). The Association between Loneliness, Mental Well-Being, and Self-Esteem among Adolescents in Four Nordic Countries. International Journal of Environmental Research and Public Health, 18(14), 7405. https://doi.org/10.3390/ijerph18147405