
Efficacy of Photobiomodulation in the Treatment of Cancer Chemotherapy-Induced Oral Mucositis: A Meta-Analysis with Trial Sequential Analysis

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Resources and Search Strategy
2.3. Study Selection
Inclusion Criteria
2.4. Data Extraction and Quality Assessment
2.5. Data Synthesis
3. Results
3.1. Study Selection
3.2. Characteristics of the Selected Studies
3.3. Risk of Bias
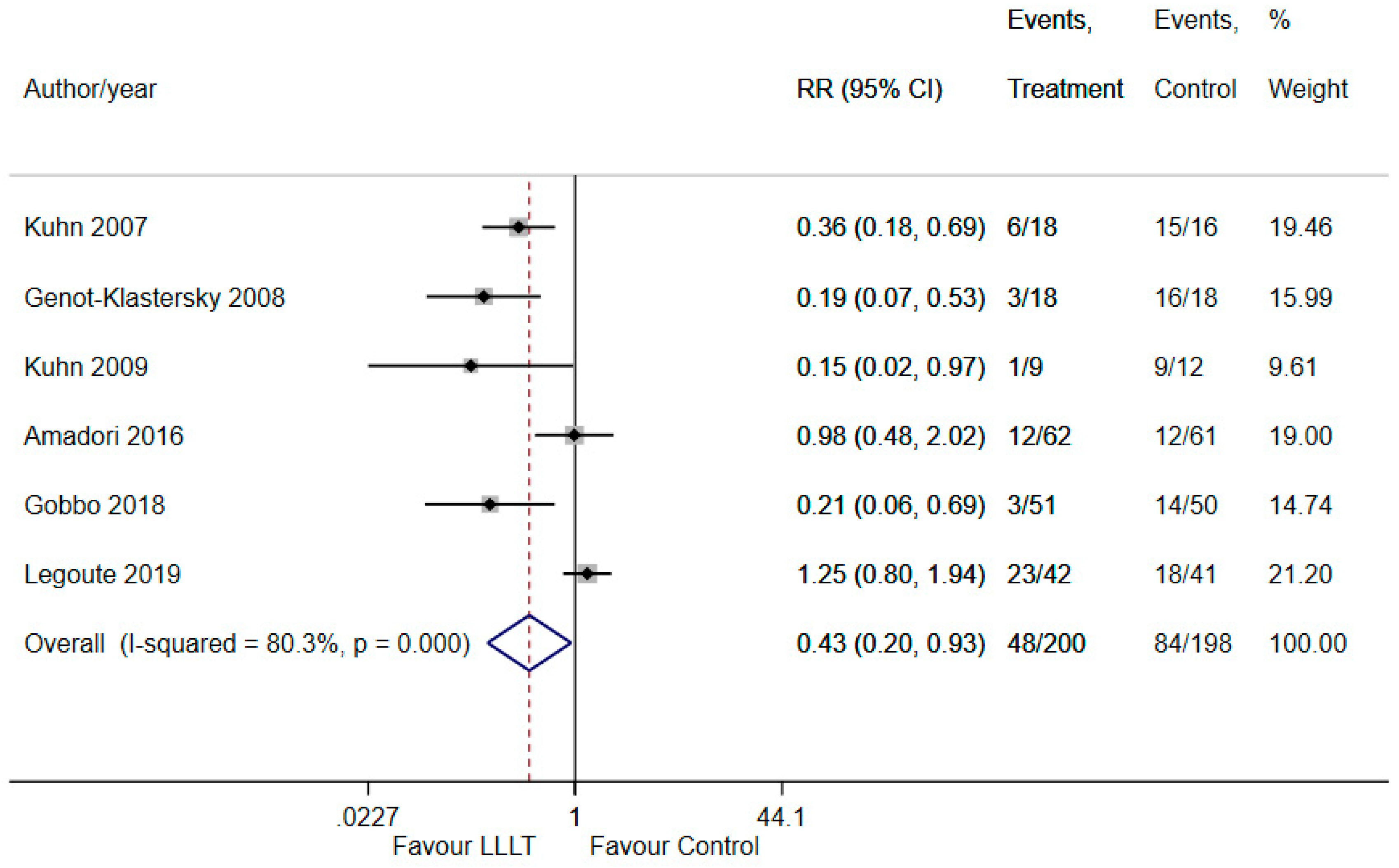
3.4. Reduction in the Severity of OM by PBM
3.5. Sensitivity Analysis
3.6. Trial Sequential Analysis
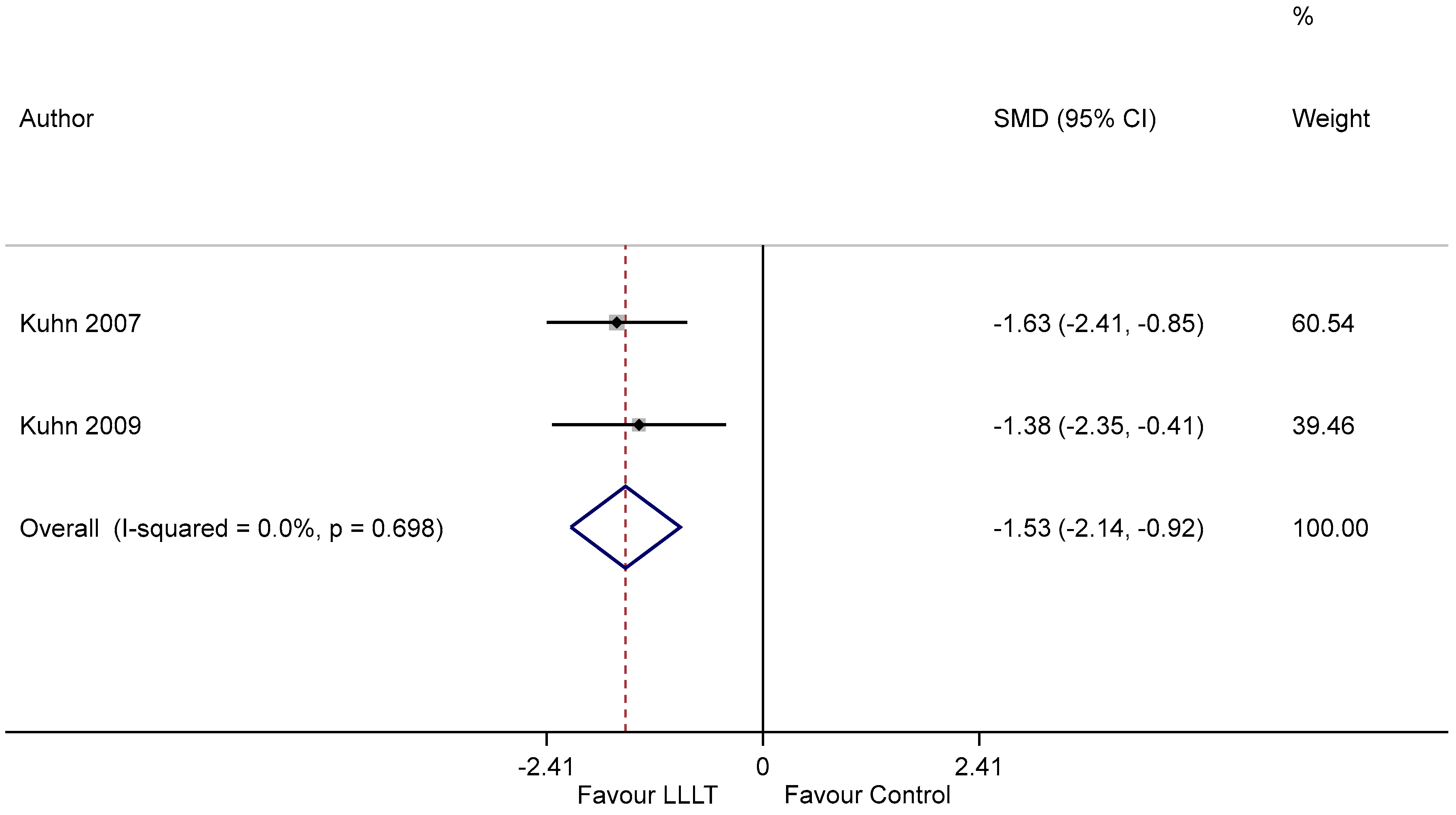
3.7. Duration of OM
3.8. Effect on Pain Relief
3.9. Adverse Effects
3.10. GRADE: Summary of Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Richardson, J.L.; Marks, G.; Levine, A. The Influence of Symptoms of Disease and Side Effects of Treatment on Compliance with Cancer Therapy. J. Clin. Oncol. 1988, 6, 1746–1752. [Google Scholar] [CrossRef]
- Keefe, D.M.; Schubert, M.M.; Elting, L.S.; Sonis, S.T.; Epstein, J.B.; Raber-Durlacher, J.E.; Migliorati, C.A.; McGuire, D.B.; Hutchins, R.D.; Peterson, D.E.; et al. Updated Clinical Practice Guidelines for the Prevention and Treatment of Mucositis. Cancer 2007, 109, 820–831. [Google Scholar] [CrossRef]
- Sonis, S.T.; Elting, L.S.; Keefe, D.; Peterson, D.E.; Schubert, M.; Hauer-Jensen, M.; Bekele, B.N.; Raber-Durlacher, J.; Donnelly, J.P.; Rubenstein, E.B.; et al. Perspectives on Cancer Therapy-Induced Mucosal Injury: Pathogenesis, Measurement, Epidemiology, and Consequences for Patients. Cancer 2004, 100, 1995–2025. [Google Scholar] [CrossRef]
- Pulito, C.; Cristaudo, A.; Porta, C.L.; Zapperi, S.; Blandino, G.; Morrone, A.; Strano, S. Oral Mucositis: The Hidden Side of Cancer Therapy. J. Exp. Clin. Cancer Res. 2020, 39, 210. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.-J.; Zhu, G.-P.; Guan, X.-Y. Comparison of the NCI-CTCAE Version 4.0 and Version 3.0 in Assessing Chemoradiation-Induced Oral Mucositis for Locally Advanced Nasopharyngeal Carcinoma. Oral Oncol. 2012, 48, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.H.L.; Gueiros, L.A.; Fulton, J.S.; Cheng, K.K.F.; Kandwal, A.; Galiti, D.; Fall-Dickson, J.M.; Johansen, J.; Ameringer, S.; Kataoka, T.; et al. Systematic Review of Basic Oral Care for the Management of Oral Mucositis in Cancer Patients and Clinical Practice Guidelines. Support. Care Cancer 2019, 27, 3949–3967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riley, P.; Glenny, A.-M.; Worthington, H.V.; Littlewood, A.; Clarkson, J.E.; McCabe, M.G. Interventions for Preventing Oral Mucositis in Patients with Cancer Receiving Treatment: Oral Cryotherapy. Cochrane Database Syst. Rev. 2015, CD011552. [Google Scholar] [CrossRef] [Green Version]
- Elad, S.; Cheng, K.K.F.; Lalla, R.V.; Yarom, N.; Hong, C.; Logan, R.M.; Bowen, J.; Gibson, R.; Saunders, D.P.; Zadik, Y.; et al. MASCC/ISOO Clinical Practice Guidelines for the Management of Mucositis Secondary to Cancer Therapy. Cancer 2020, 126, 4423–4431. [Google Scholar] [CrossRef]
- Chaveli-López, B.; Bagán-Sebastián, J.V. Treatment of Oral Mucositis Due to Chemotherapy. J. Clin. Exp. Dent. 2016, 8, e201–e209. [Google Scholar] [CrossRef]
- Zecha, J.A.E.M.; Raber-Durlacher, J.E.; Nair, R.G.; Epstein, J.B.; Sonis, S.T.; Elad, S.; Hamblin, M.R.; Barasch, A.; Migliorati, C.A.; Milstein, D.M.J.; et al. Low Level Laser Therapy/Photobiomodulation in the Management of Side Effects of Chemoradiation Therapy in Head and Neck Cancer: Part 1: Mechanisms of Action, Dosimetric, and Safety Considerations. Support. Care Cancer 2016, 24, 2781–2792. [Google Scholar] [CrossRef] [Green Version]
- Jadaud, E.; Bensadoun, R. low-level laser therapy: A Standard of Supportive Care for Cancer Therapy-Induced Oral Mucositis in Head and Neck Cancer Patients? Laser Ther. 2012, 21, 297–303. [Google Scholar] [CrossRef] [Green Version]
- Oberoi, S.; Zamperlini–Netto, G.; Beyene, J.; Treister, N.S.; Sung, L. Effect of Prophylactic Low Level Laser Therapy on Oral Mucositis: A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e107418. [Google Scholar] [CrossRef]
- Lai, C.-C.; Chen, S.-Y.; Tu, Y.-K.; Ding, Y.-W.; Lin, J.-J. Effectiveness of Low Level Laser Therapy versus Cryotherapy in Cancer Patients with Oral Mucositis: Systematic Review and Network Meta-Analysis. Crit. Rev. Oncol. Hematol. 2021, 160, 103276. [Google Scholar] [CrossRef] [PubMed]
- Anschau, F.; Webster, J.; Capra, M.E.Z.; de Azeredo da Silva, A.L.F.; Stein, A.T. Efficacy of Low-Level Laser for Treatment of Cancer Oral Mucositis: A Systematic Review and Meta-Analysis. Lasers Med. Sci. 2019, 34, 1053–1062. [Google Scholar] [CrossRef]
- Cochrane. Cochrane Handbook for Systematic Reviews of Intervention. Available online: Https://Community.Cochrane.Org/Book_pdf/764 (accessed on 20 November 2020).
- RoB 2.0: A Revised Tool to Assess the Risk of Bias in Randomized Trials [Webinar]|Cochrane Training [Internet]. Available online: Https://Training.Cochrane.Org/Resource/Rob-20-Webinar (accessed on 5 December 2020).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dersimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.0 (Updated July 2019); Cochrane: London, UK, 2019; Available online: www.Training.Cochrane.Org/Handbook (accessed on 20 November 2020).
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brok, J.; Thorlund, K.; Gluud, C.; Wetterslev, J. Trial Sequential Analysis Reveals Insufficient Information Size and Potentially False Positive Results in Many Meta-Analyses. J. Clin. Epidemiol. 2008, 61, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Puhan, M.A.; Schünemann, H.J.; Murad, M.H.; Li, T.; Brignardello-Petersen, R.; Singh, J.A.; Kessels, A.G.; Guyatt, G.H.; GRADE Working Group. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ 2014, 349, g5630. [Google Scholar] [CrossRef] [Green Version]
- Amadori, F.; Bardellini, E.; Conti, G.; Pedrini, N.; Schumacher, R.F.; Majorana, A. low-level laser therapy for Treatment of Chemotherapy-Induced Oral Mucositis in Childhood: A Randomized Double-Blind Controlled Study. Lasers Med. Sci. 2016, 31, 1231–1236. [Google Scholar] [CrossRef] [Green Version]
- Gobbo, M.; Verzegnassi, F.; Ronfani, L.; Zanon, D.; Melchionda, F.; Bagattoni, S.; Majorana, A.; Bardellini, E.; Mura, R.; Piras, A.; et al. Multicenter Randomized, Double-Blind Controlled Trial to Evaluate the Efficacy of Laser Therapy for the Treatment of Severe Oral Mucositis Induced by Chemotherapy in Children: LaMPO RCT. Pediatr. Blood Cancer 2018, 65, e27098. [Google Scholar] [CrossRef] [Green Version]
- Kuhn, A.; Vacaro, G.; Almeida, D.; Machado, Á.; Braghini, P.B.; Shilling, M.A.; Guerra, L.; Brunetto, A.L. Low-Level Infrared Laser Therapy for Chemo- or Radiotherapy-Induced Oral Mucositis: A Randomized, Placebo-Controlled Study. J. Oral Laser Appl. 2007, 7, 175. [Google Scholar]
- Kuhn, A.; Porto, F.A.; Miraglia, P.; Brunetto, A.L. Low-Level Infrared Laser Therapy in Chemotherapy-Induced Oral Mucositis: A Randomized Placebo-Controlled Trial in Children. J. Pediatr. Hematol. Oncol. 2009, 31, 33. [Google Scholar] [CrossRef]
- Legoute, F.; Bensadoun, R.-J.; Seegers, V.; Pointreau, Y.; Caron, D.; Lang, P.; Prevost, A.; Martin, L.; Schick, U.; Morvant, B.; et al. low-level laser therapy in Treatment of Chemoradiotherapy-Induced Mucositis in Head and Neck Cancer: Results of a Randomised, Triple Blind, Multicentre Phase III Trial. Radiat. Oncol. 2019, 14, 83. [Google Scholar] [CrossRef] [PubMed]
- Genot-Klastersky, M.T.; Klastersky, J.; Awada, F.; Awada, A.; Crombez, P.; Martinez, M.D.; Jaivenois, M.F.; Delmelle, M.; Vogt, G.; Meuleman, N.; et al. The Use of Low-Energy Laser (LEL) for the Prevention of Chemotherapy- and/or Radiotherapy-Induced Oral Mucositis in Cancer Patients: Results from Two Prospective Studies. Support. Care Cancer 2008, 16, 1381–1387. [Google Scholar] [CrossRef]
- WALT/NAALT Photobiomodulation: Mainstream Medicine and beyond. In Proceedings of the WALT Biennial Congress and NAALT Annual Conference, Arlington, VA, USA, 9–12 September 2014.
- Wong, T.Y.; Loo, Y.S.; Veettil, S.K.; Wong, P.S.; Divya, G.; Ching, S.M.; Menon, R.K. Efficacy and safety of posaconazole for the prevention of invasive fungal infections in immunocompromised patients: A systematic review with meta-analysis and trial sequential analysis. Sci. Rep. 2020, 10, 14575. [Google Scholar] [CrossRef] [PubMed]
- Migliorati, C.; Hewson, I.; Lalla, R.V.; Antunes, H.S.; Estilo, C.L.; Hodgson, B.; Lopes, N.N.; Schubert, M.M.; Bowen, J.; Elad, S. Systematic review of laser and other light therapy for the management of oral mucositis in cancer patients. Support. Care Cancer 2013, 21, 333–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karu, T.I. Molecular mechanism of the therapeutic effect of low-intensity laser radiation. Lasers Life Sci. 1988, 2, 53–74. [Google Scholar]
- Rizzi, C.F.; Mauriz, J.L.; Freitas Corrêa, D.S.; Moreira, A.J.; Zettler, C.G.; Filippin, L.I.; Marroni, N.P.; González-Gallego, J. Effects of low-level laser therapy (LLLT) on the Nuclear Factor (NF)-ΚB Signaling Pathway in Traumatized Muscle. Lasers Surg. Med. 2006, 38, 704–713. [Google Scholar] [CrossRef] [PubMed]
- Bensadoun, R.-J.; Nair, R.G. Efficacy of low-level laser therapy (LLLT) in Oral Mucositis: What Have We Learned from Randomized Studies and Meta-Analyses? Photomed Laser Surg 2012, 30, 191–192. [Google Scholar] [CrossRef]
- Huang, Y.-Y.; Chen, A.C.-H.; Carroll, J.D.; Hamblin, M.R. Biphasic Dose Response in Low Level Light Therapy. Dose-Response 2009, 7, dose-response.0. [Google Scholar] [CrossRef]
- Braverman, B.; McCarthy, R.J.; Ivankovich, A.D.; Forde, D.E.; Overfield, M.; Bapna, M.S. Effect of Helium-Neon and Infrared Laser Irradiation on Wound Healing in Rabbits. Lasers Surg. Med. 1989, 9, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Rupel, K.; Zupin, L.; Colliva, A.; Kamada, A.; Poropat, A.; Ottaviani, G.; Gobbo, M.; Fanfoni, L.; Gratton, R.; Santoro, M.; et al. Photobiomodulation at Multiple Wavelengths Differentially Modulates Oxidative Stress In Vitro and In Vivo. Oxid. Med. Cell. Longev. 2018, 2018, 6510159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basso, F.G.; Oliveira, C.F.; Kurachi, C.; Hebling, J.; de Souza Costa, C.A. Biostimulatory Effect of low-level laser therapy on Keratinocytes in Vitro. Lasers Med. Sci. 2013, 28, 367–374. [Google Scholar] [CrossRef]
- Hamblin, M.R.; Nelson, S.T.; Strahan, J.R. Photobiomodulation and Cancer: What Is the Truth? Photomed. Laser Surg. 2018, 36, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Al-Rudayni, A.H.M.; Gopinath, D.; Maharajan, M.K.; Menon, R.K. Impact of oral mucositis on quality of life in patients undergoing oncological treatment: A systematic review. Transl. Cancer Res. 2020, 9, 3126–3134. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Intervention | Control | PBM Duration | Irradiation Time | Primary Outcome | OM Assessment | Secondary Outcomes | Other Outcomes |
|---|---|---|---|---|---|---|---|---|
| Kuhn 2007 [25] | Laser 830 nm, 100 mW | Sham | 5 days | N/A | Reduction in severity (OM grade) | NCI-CTCAE | OM duration | Nil |
| Genot-Klastersky 2008 [28] | Visible laser + Infrared laser 100–500 mW | Sham | 3 days | 6 min | Reduction in severity (OM grade) | EORTC | OM progression | Esophageal OM |
| Kuhn 2009 [26] | Laser 830 nm, 100 mW | Sham | 5 days | N/A | Reduction in severity (OM grade) | NCI-CTCAE v2 | OM duration | Nil |
| Amadori 2016 [23] | Laser 830 nm, 150 mW | Sham | 4 days | 30 s | Reduction in severity (OM grade) | WHO | Pain score (VAS) | Nil |
| Gobbo 2018 [24] | Laser 970 nm, 250 mW | Sham | 4 days | 25 s | Reduction in severity (OM grade) | WHO | OM grade on day 4 and 11 | Pain/analgesic use |
| Legoute 2019 [27] | Laser 658 nm, 100 mW | Sham | 5 days | 40 s | Reduction in severity (OM grade) | WHO | Pain/consumption of analgesics | Nutritional status, compliance to cancer treatment, QoL |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Rudayni, A.H.M.; Gopinath, D.; Maharajan, M.K.; Veettil, S.K.; Menon, R.K. Efficacy of Photobiomodulation in the Treatment of Cancer Chemotherapy-Induced Oral Mucositis: A Meta-Analysis with Trial Sequential Analysis. Int. J. Environ. Res. Public Health 2021, 18, 7418. https://doi.org/10.3390/ijerph18147418
Al-Rudayni AHM, Gopinath D, Maharajan MK, Veettil SK, Menon RK. Efficacy of Photobiomodulation in the Treatment of Cancer Chemotherapy-Induced Oral Mucositis: A Meta-Analysis with Trial Sequential Analysis. International Journal of Environmental Research and Public Health. 2021; 18(14):7418. https://doi.org/10.3390/ijerph18147418
Chicago/Turabian StyleAl-Rudayni, Ali Hatem Manfi, Divya Gopinath, Mari Kannan Maharajan, Sajesh K. Veettil, and Rohit Kunnath Menon. 2021. "Efficacy of Photobiomodulation in the Treatment of Cancer Chemotherapy-Induced Oral Mucositis: A Meta-Analysis with Trial Sequential Analysis" International Journal of Environmental Research and Public Health 18, no. 14: 7418. https://doi.org/10.3390/ijerph18147418
APA StyleAl-Rudayni, A. H. M., Gopinath, D., Maharajan, M. K., Veettil, S. K., & Menon, R. K. (2021). Efficacy of Photobiomodulation in the Treatment of Cancer Chemotherapy-Induced Oral Mucositis: A Meta-Analysis with Trial Sequential Analysis. International Journal of Environmental Research and Public Health, 18(14), 7418. https://doi.org/10.3390/ijerph18147418