
Factors Associated with Clostridioides (Clostridium) Difficile Infection and Colonization: Ongoing Prospective Cohort Study in a French University Hospital

 ,
,  ,
, {kind=link}
Abstract
:1. Introduction
- −
- To estimate the proportion of asymptomatic colonization at admission.
- −
- To describe the association between colonization with either toxigenic or non-toxigenic strains of C. difficile and subsequent infection.
- −
- To calculate the delay between acquisition of C. difficile and the onset of symptoms related to CDI.
- −
- To identify the factors associated with colonization and infection.
2. Methods and Analysis
2.1. Study Design, Location and Patients
2.2. Sample Size
2.3. Expected Study Period
2.4. Participating Wards
2.5. Ethics and Dissemination
2.6. Patient and Public Involvement
2.7. Definitions
2.8. Clinical Data
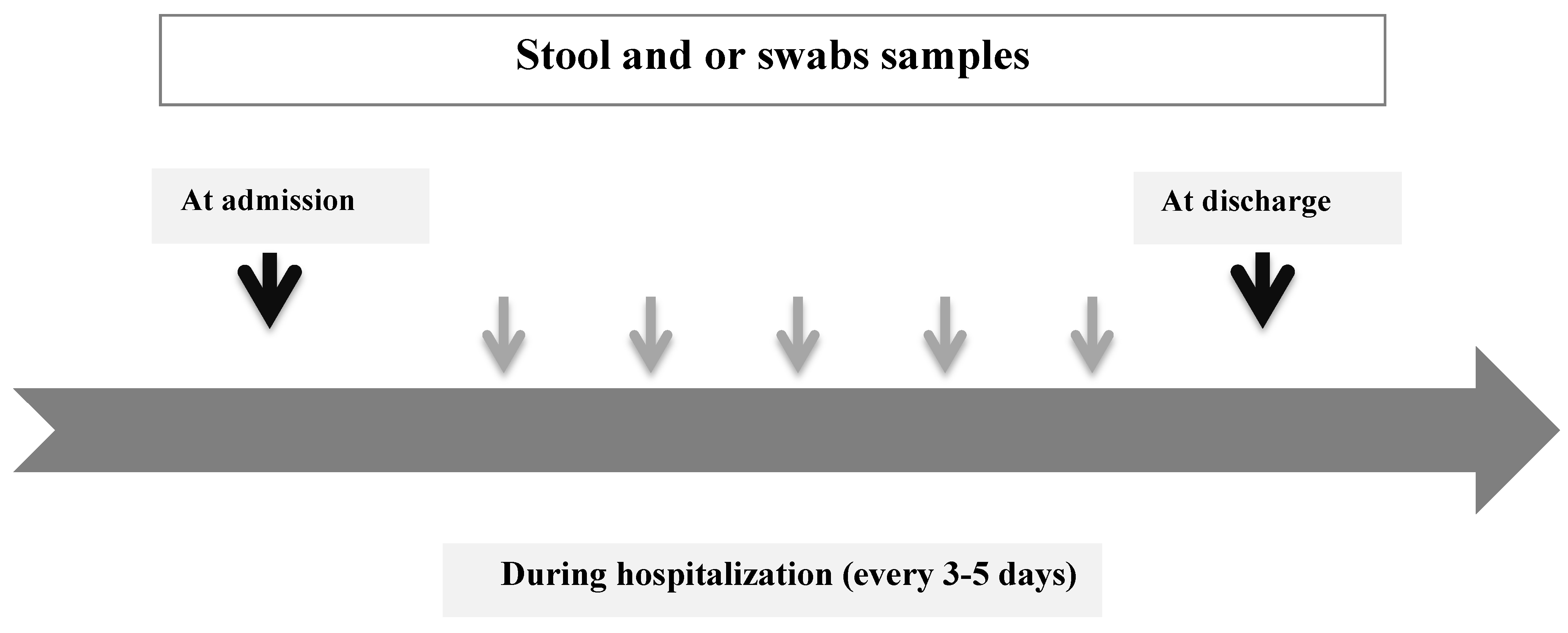
2.9. Clinical Samples
2.10. Laboratory Assays
2.11. Statistical Analysis
2.12. Data Entry
2.13. Descriptive Analysis
2.14. Rates of Colonization, CDI and Mortality
2.15. Estimation of Factors Associated with Colonization and/or CDI
2.16. Description of Prognosis of Included Patients and Survival Analyses
3. Discussion
4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Carroll, C.K.; Bartlett, J.G. Biology of Clostridium difficile: Implications for Epidemiology and Diagnosis. Annu. Rev. Microbiol. 2011, 65, 501–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surawicz, C.M.; Brandt, L.J.; Binion, D.G.; Ananthakrishnan, A.N.; Curry, S.R.; Gilligan, P.H.; McFarland, L.V.; Mellow, M.; Zuckerbraun, B.S. Guidelines for Diagnosis, Treatment, and Prevention of Clostridium difficile Infections. Am. J. Gastroenterol. 2013, 108, 478–498. [Google Scholar] [CrossRef]
- Bartlett, J.G. Antibiotic-Associated Diarrhea. N. Engl. J. Med. 2002, 346, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Loo, V.G.; Bourgault, A.-M.; Poirier, L.; Lamothe, F.; Michaud, S.; Turgeon, N.; Toye, B.; Beaudoin, A.; Frost, E.; Gilca, R.; et al. Host and Pathogen Factors for Clostridium difficile Infection and Colonization. N. Engl. J. Med. 2011, 365, 1693–1703. [Google Scholar] [CrossRef] [Green Version]
- Muto, C.A.; Pokrywka, M.; Shutt, K.; Mendelsohn, A.; Nouri, K.; Posey, K.; Roberts, T.; Croyle, K.; Krystoflak, S.; Patel-Brown, S.; et al. A Large Outbreak of Clostridium difficile–Associated Disease with an Unexpected Proportion of Deaths and Colectomies at a Teaching Hospital Following Increased Fluoroquinolone Use. Infect. Control Hosp. Epidemiol. 2005, 26, 273–280. [Google Scholar] [CrossRef] [Green Version]
- Pépin, J.; Valiquette, L.; Cossette, B. Mortality attributable to nosocomial Clostridium difficile-associated disease during an epidemic caused by a hypervirulent strain in Quebec. Can. Med. Assoc. J. 2005, 173, 1037–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbut, F.; Jones, G.; Eckert, C. Epidemiology and control of Clostridium difficile infections in healthcare settings. Curr. Opin. Infect. Dis. 2011, 24, 370–376. [Google Scholar] [CrossRef]
- Rodríguez-Pardo, D.; Almirante, B.; Bartolomé, R.M.; Pomar, V.; Mirelis, B.; Navarro, F.; Soriano, A.; Sorlí, L.; Martínez-Montauti, J.; Molins, M.T.; et al. Epidemiology of Clostridium difficile Infection and Risk Factors for Unfavorable Clinical Outcomes: Results of a Hospital-Based Study in Barcelona, Spain. J. Clin. Microbiol. 2013, 51, 1465–1473. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Kang, J.O.; Kim, H.; Seo, M.-R.; Choi, T.Y.; Pai, H.; Kuijper, E.; Sanders, I.; Fawley, W. Epidemiology of Clostridium difficile infections in a tertiary-care hospital in Korea. Clin. Microbiol. Infect. 2013, 19, 521–527. [Google Scholar] [CrossRef] [Green Version]
- Mascart, G.; Delmée, M.; Van Broeck, J.; Cytryn, E.; Karmali, R.; Cherifi, S. Impact of ribotype 027 on Clostridium difficile infection in a geriatric department. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 1177–1182. [Google Scholar] [CrossRef]
- Bartlett, J.G. Narrative review, the new epidemic of Clostridium difficile-associated enteric disease. Ann. Intern. Med. 2006, 145, 758–764. [Google Scholar] [CrossRef]
- Nanwa, N.; Kendzerska, T.; Krahn, M.; Kwong, J.C.; Daneman, N.; Witteman, W.; Mittmann, N.; Cadarette, S.; Rosella, L.; Sander, B. The Economic Impact of Clostridium difficile Infection: A Systematic Review. Am. J. Gastroenterol. 2015, 110, 511–519. [Google Scholar] [CrossRef]
- Best, E.L.; Fawley, W.N.; Parnell, P.; Wilcox, M.H. The Potential for Airborne Dispersal of Clostridium difficile from Symptomatic Patients. Clin. Infect. Dis. 2010, 50, 1450–1457. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.H.; Gerding, D.N.; Johnson, S.; Kelly, C.P.; Loo, V.G.; McDonald, L.C.; Pépin, J.L.; Wilcox, M.H. Clinical Practice Guidelines for Clostridium difficile Infection in Adults: 2010 Update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect. Control Hosp. Epidemiol. 2010, 31, 431–455. [Google Scholar] [CrossRef] [PubMed]
- Donskey, C.J. Preventing Transmission of Clostridium difficile: Is the Answer Blowing in the Wind? Clin. Infect. Dis. 2010, 50, 1458–1461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.-H.; Fekety, R.; Batts, D.H.; Brown, D.; Cudmore, M.; Silva, J.; Waters, D. Isolation of Clostridium difficile from the Environment and Contacts of Patients with Antibiotic-Associated Colitis. J. Infect. Dis. 1981, 143, 42–50. [Google Scholar] [CrossRef]
- Zacharioudakis, I.M.; Zervou, F.N.; Pliakos, E.; Ziakas, P.; Mylonakis, E. Colonization With Toxinogenic C. difficile Upon Hospital Admission, and Risk of Infection: A Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2015, 110, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.K.; Johnson, S.; Samore, M.H.; Bliss, D.Z.; Gerding, D.N. Primary symptomless colonisation by Clostridium difficile and decreased risk of subsequent diarrhoea. Lancet 1998, 351, 633–636. [Google Scholar] [CrossRef]
- Lim, S.K.; Stuart, R.L.; Mackin, K.E.; Carter, G.; Kotsanas, D.; Francis, M.J.; Easton, M.; Dimovski, K.; Elliott, B.; Riley, T.V.; et al. Emergence of a Ribotype 244 Strain of Clostridium difficile Associated With Severe Disease and Related to the Epidemic Ribotype 027 Strain. Clin. Infect. Dis. 2014, 58, 1723–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quesada-Gómez, C.; López-Ureña, D.; Acuña-Amador, L.; Villalobos-Zúñiga, M.; Du, T.; Freire, R.; Guzman-Verri, C.; Gamboa-Coronado, M.D.M.; Lawley, T.D.; Moreno, E.; et al. Emergence of an Outbreak-Associated Clostridium difficile Variant with Increased Virulence. J. Clin. Microbiol. 2015, 53, 1216–1226. [Google Scholar] [CrossRef] [Green Version]
- Peláez, T.; Alcalá, L.; Blanco, J.L.; Álvarez-Pérez, S.; Marín, M.; Martín-López, A.; Catalán, P.; Reigadas, E.; García, M.E.; Bouza, E. Characterization of swine isolates of Clostridium difficile in Spain: A potential source of epidemic multidrug resistant strains? Anaerobe 2013, 22, 45–49. [Google Scholar] [CrossRef]
- Janezic, S.; Zidaric, V.; Pardon, B.; Indra, A.; Kokotovic, B.; Blanco, J.L.; Seyboldt, C.; Diaz, C.R.; Poxton, I.R.; Perreten, V.; et al. International Clostridium difficile animal strain collection and large diversity of animal associated strains. BMC Microbiol. 2014, 14, 173. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, C.; Taminiau, B.; Avesani, V.; Van Broeck, J.; Delmée, M.; Daube, G. Multilocus sequence typing analysis and antibiotic resistance of Clostridium difficile strains isolated from retail meat and humans in Belgium. Food Microbiol. 2014, 42, 166–171. [Google Scholar] [CrossRef]
- Barbut, F.; Surgers, L.; Eckert, C.; Visseaux, B.; Cuingnet, M.; Mesquita, C.; Pradier, N.; Thiriez, A.; Ait-Ammar, N.; Aifaoui, A.; et al. Does a rapid diagnosis of Clostridium difficile infection impact on quality of patient management? Clin. Microbiol. Infect. 2014, 20, 136–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, K.A.; Longshaw, C.; Davis, G.L.; Bouza, E.; Barbut, F.; Barna, Z.; Delmée, M.; Fitzpatrick, F.; Ivanova, K.; Kuijper, E.; et al. Underdiagnosis of Clostridium difficile across Europe: The European, multicentre, prospective, biannual, point-prevalence study of Clostridium difficile infection in hospitalised patients with diarrhoea (EUCLID). Lancet Infect. Dis. 2014, 14, 1208–1219. [Google Scholar] [CrossRef]
- Kutty, P.K.; Beekmann, S.E.; Sinkowitz-Cochran, R.L.; Dubberke, E.R.; Kuhar, D.T.; McDonald, L.C.; Polgreen, P.M. A national survey of testing and management of asymptomatic carriage of C. difficile. Infect. Control Hosp. Epidemiol. 2019, 40, 801–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baron, S.W.; Ostrowsky, B.E.; Nori, P.; Drory, D.Y.; Levi, M.H.; Szymczak, W.; Rinke, M.L.; Southern, W.N. Screening ofClostridioides difficilecarriers in an urban academic medical center: Understanding implications of disease. Infect. Control Hosp. Epidemiol. 2019, 41, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Poirier, D.; Gervais, P.; Fuchs, M.; Roussy, J.-F.; Paquet-Bolduc, B.; Trottier, S.; Longtin, J.; Loo, V.G.; Longtin, Y. Predictors of Clostridioides difficile Infection Among Asymptomatic, Colonized Patients: A Retrospective Cohort Study. Clin. Infect. Dis. 2019, 70, 2103–2210. [Google Scholar] [CrossRef]
- Gilboa, M.; Houri-Levi, E.; Cohen, C.; Tal, I.; Rubin, C.; Feld-Simon, O.; Brom, A.; Eden-Friedman, Y.; Segal, S.; Rahav, G.; et al. Environmental shedding of toxigenic Clostridioides difficile by asymptomatic carriers: A prospective observational study. Clin. Microbiol. Infect. 2020, 26, 1052–1057. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khanafer, N.; Vanhems, P.; Bennia, S.; Martin-Gaujard, G.; Juillard, L.; Rimmelé, T.; Argaud, L.; Martin, O.; Huriaux, L.; Marcotte, G.; et al. Factors Associated with Clostridioides (Clostridium) Difficile Infection and Colonization: Ongoing Prospective Cohort Study in a French University Hospital. Int. J. Environ. Res. Public Health 2021, 18, 7528. https://doi.org/10.3390/ijerph18147528
Khanafer N, Vanhems P, Bennia S, Martin-Gaujard G, Juillard L, Rimmelé T, Argaud L, Martin O, Huriaux L, Marcotte G, et al. Factors Associated with Clostridioides (Clostridium) Difficile Infection and Colonization: Ongoing Prospective Cohort Study in a French University Hospital. International Journal of Environmental Research and Public Health. 2021; 18(14):7528. https://doi.org/10.3390/ijerph18147528
Chicago/Turabian StyleKhanafer, Nagham, Philippe Vanhems, Sabrina Bennia, Géraldine Martin-Gaujard, Laurent Juillard, Thomas Rimmelé, Laurent Argaud, Olivier Martin, Laetitia Huriaux, Guillaume Marcotte, and et al. 2021. "Factors Associated with Clostridioides (Clostridium) Difficile Infection and Colonization: Ongoing Prospective Cohort Study in a French University Hospital" International Journal of Environmental Research and Public Health 18, no. 14: 7528. https://doi.org/10.3390/ijerph18147528
APA StyleKhanafer, N., Vanhems, P., Bennia, S., Martin-Gaujard, G., Juillard, L., Rimmelé, T., Argaud, L., Martin, O., Huriaux, L., Marcotte, G., Hernu, R., Floccard, B., Cassier, P., & Group, S. (2021). Factors Associated with Clostridioides (Clostridium) Difficile Infection and Colonization: Ongoing Prospective Cohort Study in a French University Hospital. International Journal of Environmental Research and Public Health, 18(14), 7528. https://doi.org/10.3390/ijerph18147528