
Effectiveness of Simulation-Based Empathy Enhancement Program for Caregivers (SEE-C) Evaluated by Older Adults Receiving Care


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
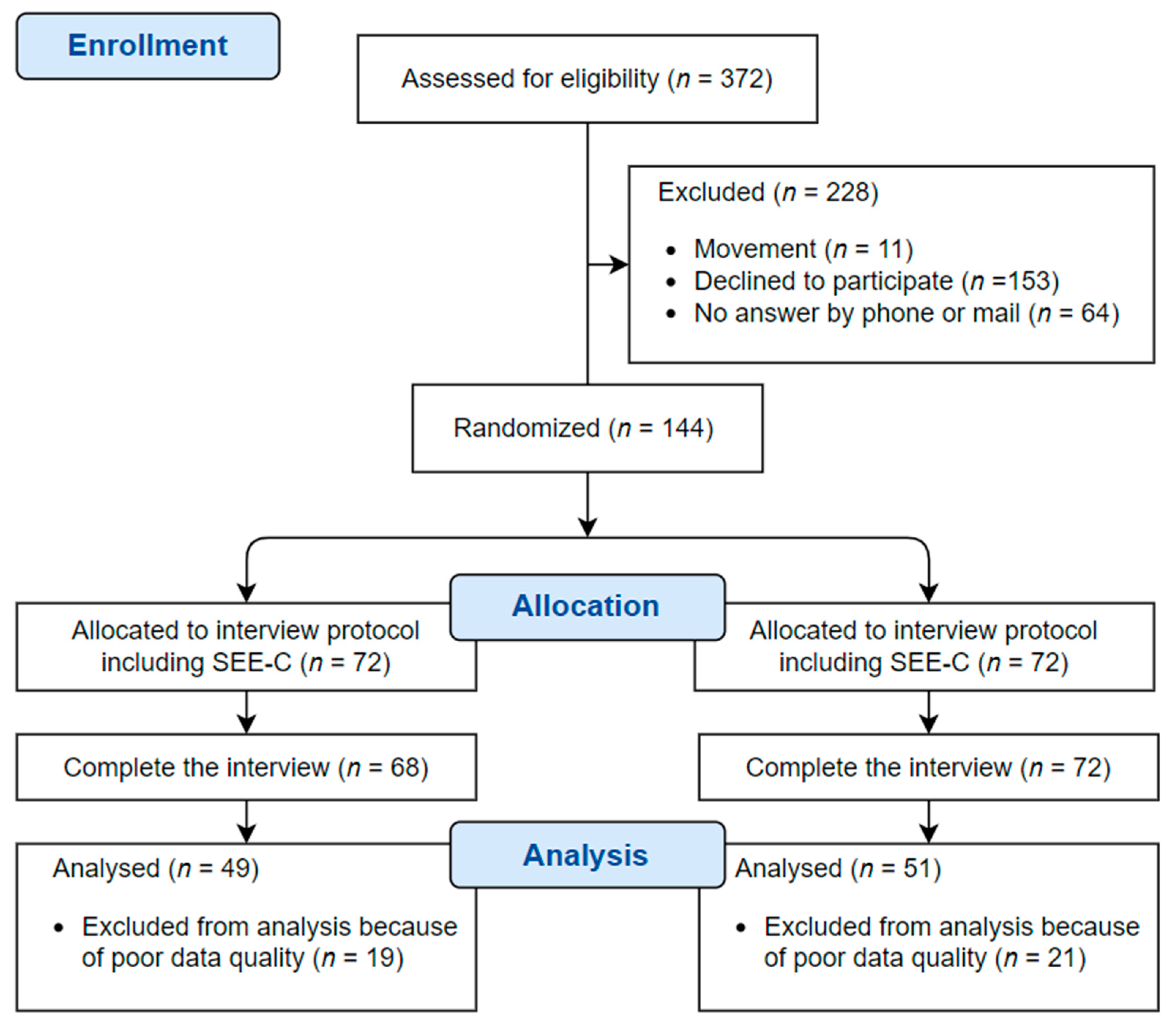
2.2. Sample Size Calculation and Recruitment
2.3. Ethics
2.4. Measurement
2.4.1. Health Status Evaluation
2.4.2. Interview Session Evaluation
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barua, A.; Ghosh, M.K.; Kar, N.; Basilio, M.A. Socio-demographic Factors of Geriatric Depression. Indian J. Psychol. Med. 2010, 32, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Wiktorsson, S.; Runeson, B.; Skoog, I.; Östling, S.; Waern, M. Attempted Suicide in the Elderly: Characteristics of Suicide Attempters 70 Years and Older and a General Population Comparison Group. Am. J. Geriatr. Psychiatry 2010, 18, 57–67. [Google Scholar] [CrossRef]
- Lee, H.-Y.; Choi, J.-H.; Yi, N.-Y.; Lee, M.-J.; Chang, H.-J.; Choi, E.-H.; Chung, M.-J.; Gang, G.-O.; Lee, H.-L.; Lee, K.-E.; et al. Development of Materials for Food Safety and Nutrition Management Program for Single Seniors with a Life Manager -by Focus Group Interview and Delphi Technique. J. Korean Soc. Food Sci. Nutr. 2018, 47, 195–206. [Google Scholar] [CrossRef]
- Lyu, I. A study of life satisfaction level concerning the life management assistant dispatch project for the elderly. Korean J. 21 Century Soc. Welf. 2008, 5, 159–180. [Google Scholar]
- Song, S.; Kim, T.; Park, M.; Um, T. A Study on Empathy Experiences of Welfare Practitioners of Single-Household Elderly Support Center. Korean J. Gerontol. Soc. Welf. 2019, 74, 61–85. [Google Scholar] [CrossRef]
- Gerdes, K.E.; Segal, E. Importance of Empathy for Social Work Practice: Integrating New Science. Soc. Work. 2011, 56, 141–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanafelt, T.D.; West, C.; Zhao, X.; Novotny, P.; Kolars, J.; Habermann, T.; Sloan, J. Relationship between increased personal well-being and enhanced empathy among. J. Gen. Intern. Med. 2005, 20, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Clark, K.B. Empathy: A neglected topic in psychological research. Am. Psychol. 1980, 35, 187. [Google Scholar] [CrossRef]
- Stephan, W.G.; Finlay, K. The Role of Empathy in Improving Intergroup Relations. J. Soc. Issues 1999, 55, 729–743. [Google Scholar] [CrossRef]
- Miller, P.A.; Eisenberg, N. The relation of empathy to aggressive and externalizing/antisocial behavior. Psychol. Bull. 1988, 103, 324. [Google Scholar] [CrossRef] [PubMed]
- Mercer, S.W.; Reynolds, W.J. Empathy and quality of care. Br. J. Gen. Pract. 2002, 52, S9–S12. [Google Scholar]
- Hojat, M. Ten approaches for enhancing empathy in health and human services cultures. J. Health Hum. Serv. Adm. 2009, 31, 412–450. [Google Scholar]
- Bayne, H.B.; Hays, D.G. Examining Conditions for Empathy in Counseling: An Exploratory Model. J. Humanist. Couns. 2017, 56, 32–52. [Google Scholar] [CrossRef]
- van Berkhout, E.T.; Malouff, J.M. The efficacy of empathy training: A meta-analysis of randomized controlled trials. J. Couns. Psychol. 2016, 63, 32. [Google Scholar] [CrossRef]
- Cheng, A.; Palaganas, J.; Eppich, W.; Rudolph, J.; Robinson, T.; Grant, V. Co-debriefing for simulation-based education: A primer for facilitators. Simul. Healthc. 2015, 10, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Fox, R.; Walker, J.; Draycott, T.J. Medical simulation for professional development-science and practice. BJOG Int. J. Obstet. Gynaecol. 2011, 118, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Han, A.; Kim, T.H. Effectiveness of empathy enhancement programs for social workers working with older adults: A quasi-experimental study. J. Soc. Work. 2020, 21, 913–930. [Google Scholar] [CrossRef]
- Han, A.; Kim, T.H. A Quasi-experimental Study Measuring the Effectiveness of Two Empathy Enhancement Programs on Caregivers Working with Older Adults Living Alone. Clin. Gerontol. 2020, 24, 1–10. [Google Scholar] [CrossRef]
- Morse, J.M.; Anderson, G.; Bottorff, J.L.; Yonge, O.; O’Brien, B.; Solberg, S.M.; McIlveen, K.H. Exploring empathy: A conceptual fit for nursing practice? Image J. Nurs. Scholarsh. 1992, 24, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Alzayer, Z.M.; Abdulkader, R.S.; Jeyashree, K.; Alselihem, A. Patient-rated physicians’ empathy and its determinants in Riyadh, Saudi Arabia. J. Fam. Community Med. 2019, 26, 199. [Google Scholar]
- Stephen, K.A.; Baernstein, A. Educating for Empathy. JGIM J. Gen. Intern. Med. 2006, 21, 524–530. [Google Scholar] [CrossRef]
- Bernardo, M.O.; Cecílio-Fernandes, D.; Costa, P.; Quince, T.A.; Costa, M.J.; Carvalho-Filho, M.A. Physicians’ self-assessed empathy levels do not correlate with patients’ assessments. PLoS ONE 2018, 13, e0198488. [Google Scholar] [CrossRef] [Green Version]
- Jeong, Y.-A. The Relationship between the Empathetic Ability of a Solitary Senior Citizen Life Manager and the Solitary Senior Citizens’s Emotional Stability; Industrial Graduate School at Myongji University: Seoul, Korea, 2017. [Google Scholar]
- Ageucate Training Institute. Available online: https://ageucate.com/ (accessed on 11 February 2021).
- Jeong, H.Y.; Kim, T.H.; Han, A.R. Effects of Korean Dementia Simulation Program for Caregivers of the Elderly with Dementia: A Pilot Study. Korean Assoc. Geriatr. Psychiatry 2019, 23, 65–71. [Google Scholar] [CrossRef]
- Han, A.; Kim, T.H.; Hong, H. Experiences of caregivers of people with dementia in a Korean dementia simulation program. Dementia 2019, 19, 2415–2429. [Google Scholar] [CrossRef]
- Bohecker, L.; Doughty Horn, E.A. Increasing students’ empathy and counseling self-efficacy through a mindfulness experiential small group. J. Spec. Group Work. 2016, 41, 312–333. [Google Scholar] [CrossRef]
- Lee, Y.-K.; Nam, H.-S.; Chuang, L.-H.; Kim, K.-Y.; Yang, H.-K.; Kwon, I.-S.; Kind, P.; Kweon, S.; Kim, Y.-T. South Korean Time Trade-Off Values for EQ-5D Health States: Modeling with Observed Values for 101 Health States. Value Health 2009, 12, 1187–1193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabin, R.; Oemar, M.; Oppe, M.; Janssen, B.; Herdman, M. EQ-5D-3L User Guide: Basic Information on How to Use the EQ-5D-3L Instrument; EuroQol Group: Rotterdam, The Netherlands, 2011; p. 22. [Google Scholar]
- Kim, O.S. Korean Version of the Revised UCLA Loneliness Scale: Reliability and Validity Test. J. Nurses Acad. Soc. 1997, 27, 871–879. [Google Scholar] [CrossRef]
- Kim, T.H.; Jhoo, J.H.; Park, J.H.; Kim, J.L.; Ryu, S.H.; Moon, S.W.; Choo, I.H.; Lee, D.W.; Yoon, J.C.; Do, Y.J.; et al. Korean Version of Mini Mental Status Examination for Dementia Screening and Its’ Short Form. Psychiatry Investig. 2010, 7, 102–108. [Google Scholar] [CrossRef]
- Bae, J.N.; Cho, M.J. Development of the Korean version of the Geriatric Depression Scale and its short form among elderly psychiatric patients. J. Psychosom. Res. 2004, 57, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Stiles, W. Use of the Session Evaluation Questionnaire; Miami University: Oxford, OH, USA, 1989. [Google Scholar]
- Lee, S.; Kim, K. Validation of Session Evaluation Questionnaire. Korean J. Couns. Psychol. 1993, 5, 30–47. [Google Scholar]
- Stiles, W.B.; Snow, J.S. Counseling session impact as viewed by novice counselors and their clients. J. Couns. Psychol. 1984, 31, 3. [Google Scholar] [CrossRef]
- Bearman, M.; Palermo, C.; Allen, L.M.; Williams, B. Learning empathy through simulation: A systematic literature review. Simul. Healthc. 2015, 10, 308–319. [Google Scholar] [CrossRef] [PubMed]
- Bunn, W.; Terpstra, J. Cultivating empathy for the mentally ill using simulated auditory hallucinations. Acad. Psychiatry 2009, 33, 457–460. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.W.; Ozier, A.D.; Johnson, A. Empathetic responses and attitudes about older adults: How experience with the aging game measures up. Educ. Gerontol. 2011, 37, 924–941. [Google Scholar] [CrossRef]
- Cuff, B.M.; Brown, S.J.; Taylor, L.; Howat, D.J. Empathy: A review of the concept. Emot. Rev. 2016, 8, 144–153. [Google Scholar] [CrossRef]
- Zaki, J.; Ochsner, K.N. The neuroscience of empathy: Progress, pitfalls and promise. Nat. Neurosci. 2012, 15, 675–680. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Category | Experimental Group (n = 49) | Control Group (n = 51) | p-Value |
|---|---|---|---|
| Age(years) | 73.02 ± 4.0 | 71.16 ± 3.8 | 0.020 * |
| Gender | |||
| Male | 19 (38) | 18 (36) | 0.718 |
| Female | 31 (62) | 32 (64) | |
| Years of Education | 6.78 ± 3.9 | 7.24 ± 4.1 | 0.729 |
| Years of Living Alone | 17.94 ± 11.7 | 20.75 ± 13.2 | 0.313 |
| EQ-5D-3L | 0.82 ± 0.2 | 0.83 ± 0.2 | 0.807 |
| RULS | 37.65 ± 10.2 | 39.75 ± 9.6 | 0.386 |
| MMSE-DS | 27.94 ± 2.4 | 27.90 ± 1.9 | 0.538 |
| SGDS | 2.45 ± 2.5 | 3.08 ± 2.9 | 0.208 |
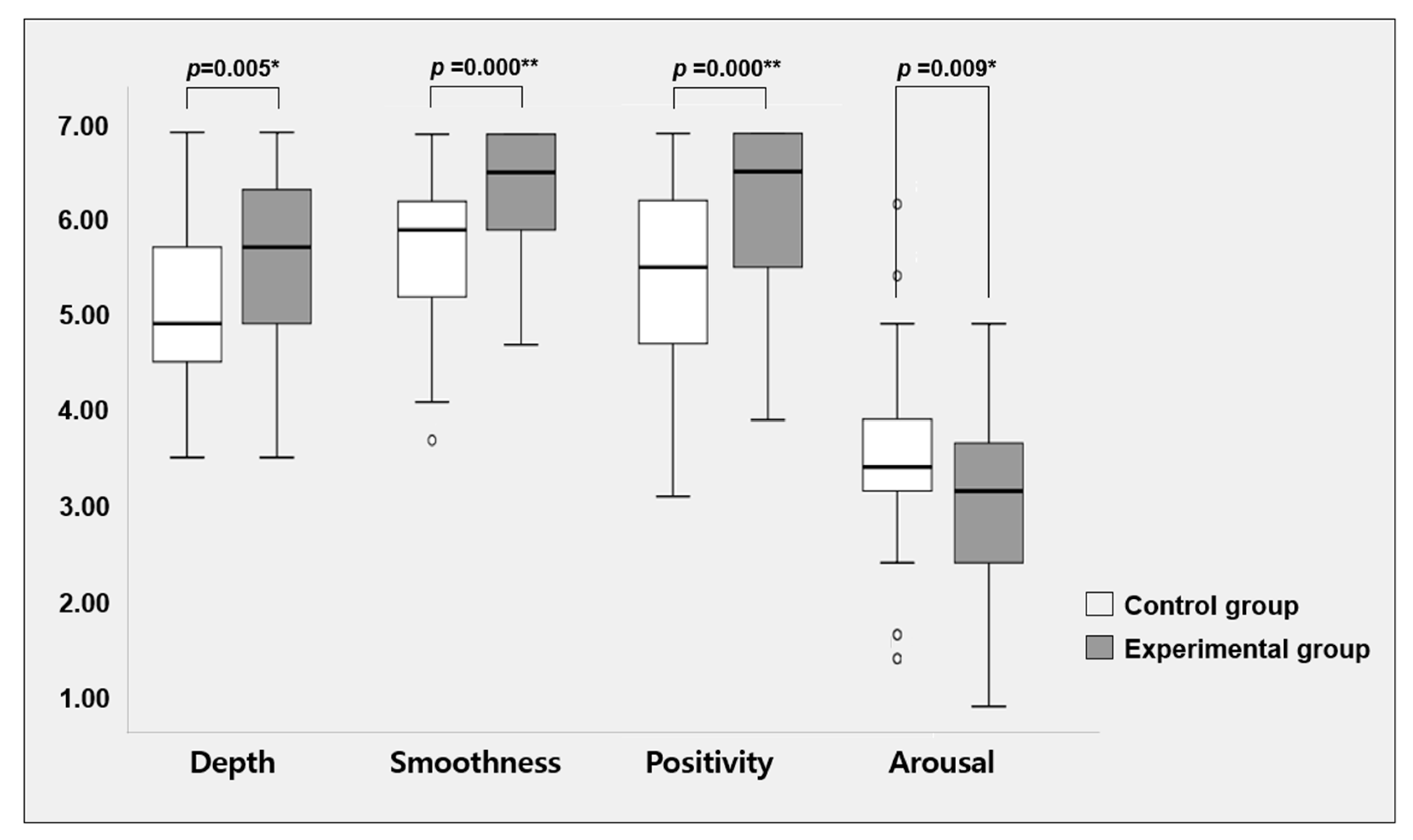
| Categories of SEQ | Experimental Group (n = 49) | Control Group (n = 51) | U-Value | p-Value | |
|---|---|---|---|---|---|
| Session evaluation | Depth | 5.70 ± 1.0 | 5.15 ± 0.9 | 1651.5 | 0.005 * |
| Smoothness | 6.45 ± 0.6 | 5.81 ± 0.9 | 1803.0 | 0.000 ** | |
| Post-session mood | Positivity | 6.26 ± 0.9 | 5.49 ± 1.1 | 1783.0 | 0.000 ** |
| Arousal | 3.03 ± 0.9 | 3.55 ± 0.9 | 873.5 | 0.009 * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.; Han, A.; Kim, T.H. Effectiveness of Simulation-Based Empathy Enhancement Program for Caregivers (SEE-C) Evaluated by Older Adults Receiving Care. Int. J. Environ. Res. Public Health 2021, 18, 7802. https://doi.org/10.3390/ijerph18157802
Lee K, Han A, Kim TH. Effectiveness of Simulation-Based Empathy Enhancement Program for Caregivers (SEE-C) Evaluated by Older Adults Receiving Care. International Journal of Environmental Research and Public Health. 2021; 18(15):7802. https://doi.org/10.3390/ijerph18157802
Chicago/Turabian StyleLee, Kyuwon, Areum Han, and Tae Hui Kim. 2021. "Effectiveness of Simulation-Based Empathy Enhancement Program for Caregivers (SEE-C) Evaluated by Older Adults Receiving Care" International Journal of Environmental Research and Public Health 18, no. 15: 7802. https://doi.org/10.3390/ijerph18157802
APA StyleLee, K., Han, A., & Kim, T. H. (2021). Effectiveness of Simulation-Based Empathy Enhancement Program for Caregivers (SEE-C) Evaluated by Older Adults Receiving Care. International Journal of Environmental Research and Public Health, 18(15), 7802. https://doi.org/10.3390/ijerph18157802