
Evaluation of Medicine Abuse Trends in Community Pharmacies: The Medicine Abuse Observatory (MAO) in a Region of Southern Europe

 ,
,  ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Medicine Abuse Observatory (MAO) Conceptualisation
2.2. Abuse Drugs Questionnaire (ADQ) Development
2.3. Pharmacies Selection
2.4. Pharmacist Training
2.5. Statistical Analysis
3. Results
3.1. Patient and Pharmacy Distribution Profile
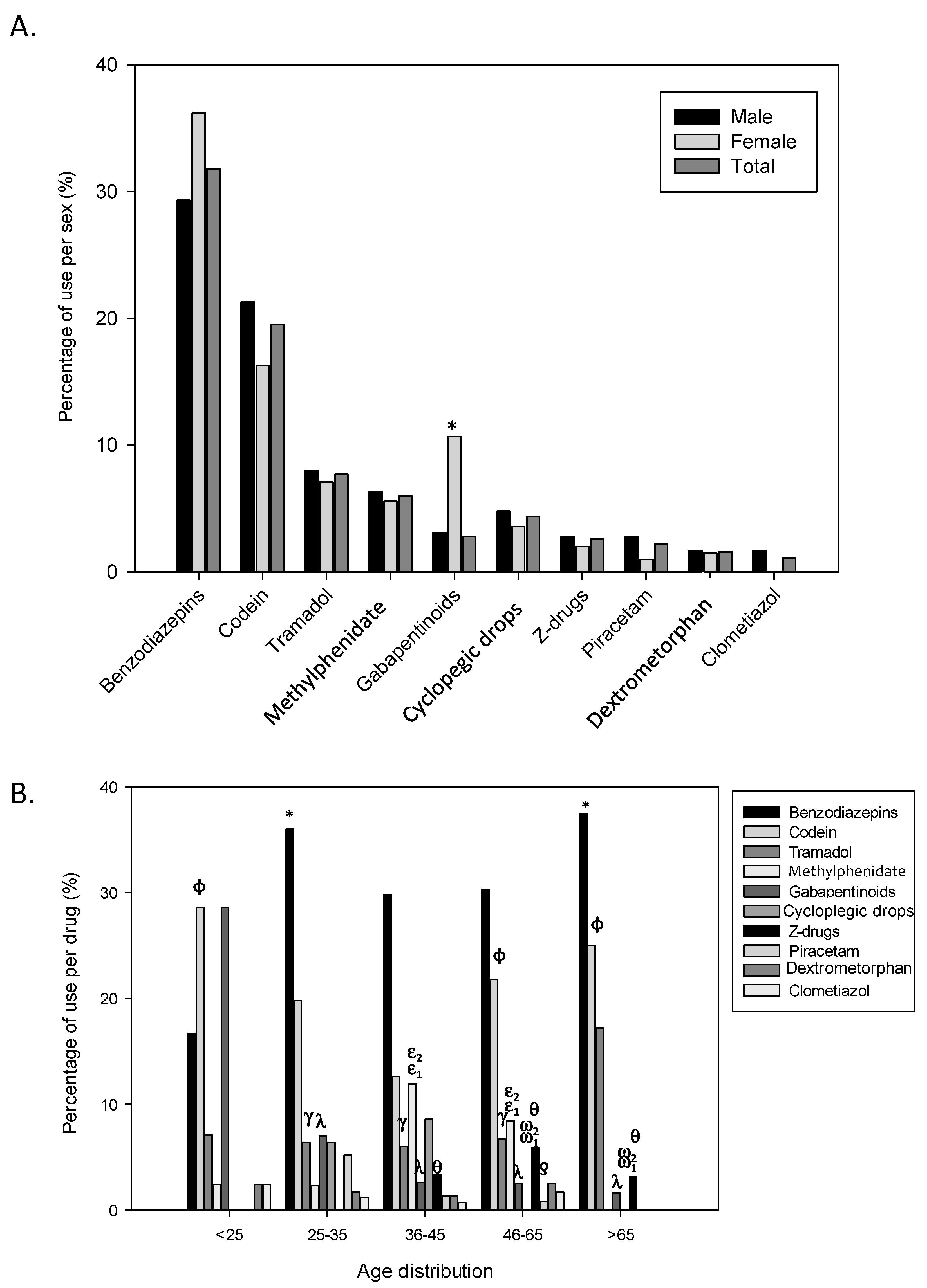
3.2. Involved Substances
3.3. Drug Request
3.4. Supply of Medicine
- i.
- the pharmacist knows the patient because that patient lives in the neighbourhood;
- ii.
- the requested medication is an over-the-counter product;
- iii.
- the pharmacist has detected that the prescription was false after dispensing the medication;
- iv.
- the patient presents multiple prescriptions but all of them are correct;
- v.
- the patient knows why and how the medicine is used and also expresses a need and the pharmacist gives the medication under pressure.
- i.
- the patient take more medication than prescribed;
- ii.
- the reason for the demand does not agree with the symptoms described;
- iii.
- it has been confirmed with the doctor that the prescription is false;
- iv.
- the patients insists forcefully for getting the drug;
- v.
- a first dispensation is made but then the following are denied.
3.5. Multidimensional Analysis of the Participants
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- NIDA. Prescription Drugs. In: NIDA Community Drug Alert Bulletin. 2005. Available online: https://archives.drugabuse.gov/publications/nida-community-drug-alert-bulletin-prescription-drugs (accessed on 8 January 2017).
- NIDA. Media Guide. In: National Institute on Drug Abuse; National Institutes of Health; U.S. Department of Health and Human Services. 2018. Available online: https://www.drugabuse.gov/sites/default/files/media_guide.pdf (accessed on 6 October 2018).
- Substance Abuse and Mental Health Services Administration. Key Substance Use and Mental Health Indicators in the United States: Results from the 2018 National Survey on Drug Use and Health. In: HHS Publication No. PEP19-5068, NSDUH Series H-54. Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. 2019. Available online: https://www.samhsa.gov/data/ (accessed on 9 September 2019).
- Centers for Disease Control and Prevention. Prescription Drug Monitoring Programs (PDMPs). In: Healthcare Providers & Systems. 2019. Available online: https://www.cdc.gov/drugoverdose/pdmp/providers.html (accessed on 9 September 2019).
- European Monitoring Centre for Drugs and Drug Addiction. Euro-DEN Plus Network Expands Reach by Welcoming Eight New Centres. In: Monitoring Hospital Emergencies and Acute Drug Toxicity in Europe. 2017. Available online: https://www.emcdda.europa.eu/news/2017/fs2/euro-den-expands_en (accessed on 5 June 2017).
- European Monitoring Centre for Drugs and Drug Addiction. Drug-Related Hospital Emergency Presentations in Europe: Update from the Euro-DEN Plus Expert Network. In: Hospital Emergencies. 2020. Available online: https://www.emcdda.europa.eu/system/files/publications/12725/TD02AY20001ENN.pdf (accessed on 19 March 2020).
- Casati, A.; Sedefov, R.; Pfeiffer-Gerschel, T. Misuse of Medicines in the European Union: A Systematic Review of the Literature. Eur. Addict. Res. 2012, 18, 228–245. [Google Scholar] [CrossRef]
- Observatorio Español de las Drogas y las Adicciones. Estadísticas 2019 Alcohol, Tabaco y Drogas Ilegales en España. In: Delegación del Gobierno Para el Plan Nacional Sobre Drogas. Ministerio de Sanidad, Consumo y Bienester Social. 2019. Available online: https://pnsd.sanidad.gob.es/profesionales/sistemasInformacion/informesEstadisticas/pdf/2019OEDA-ESTADISTICAS.pdf (accessed on 2 February 2020).
- WHO Regional Office for Europe. The Legal and Regulatory Framework for Community Pharmacies in the WHO European Region. In: Public Health Panorama. 2019. Available online: https://www.euro.who.int/en/publications/abstracts/the-legal-and-regulatory-framework-for-community-pharmacies-in-the-who-european-region-2019 (accessed on 9 September 2019).
- ASHP Statement on the Pharmacist’s Role in Substance Abuse Prevention, Education, and Assistance. Am. J. Health Pharm. 2014, 71, 243–246. [CrossRef]
- El-Aneed, A.; Alaghehbandan, R.; Gladney, N.; Collins, K.; Macdonald, D.; Fischer, B. Prescription drug abuse and methods of diversion: The potential role of a pharmacy network. J. Subst. Use 2009, 14, 75–83. [Google Scholar] [CrossRef]
- Finch, J. Prescription drug abuse. Prim. Care 1993, 20, 231–239. [Google Scholar] [CrossRef]
- Vega, A.T.; Zurriaga, O.; Galmés, A.; Lozano, J.E.; Paisán, L.; Gil, M.; Herrero, A.; Ramos, J.M. Guía de principios y métodos de las redes centinelas sanitarias en España. Gac. Sanit. 2006, 20, 52–60. [Google Scholar] [CrossRef] [Green Version]
- Bach, P.; Hartung, D. Leveraging the role of community pharmacists in the prevention, surveillance, and treatment of opioid use disorders. Addict. Sci. Clin. Pr. 2019, 14, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrot, S.; Cittée, J.; Louis, P.; Quentin, B.; Robert, C.; Milon, J.; Bismut, H.; Baumelou, A. Self-medication in pain management: The state of the art of pharmacists’ role for optimal Over-The-Counter analgesic use. Eur. J. Pain 2019, 23, 1747–1762. [Google Scholar] [CrossRef] [PubMed]
- Substance Abuse and Mental Health Services Administration. Preliminary Data from the Drug Abuse Warning Network. In: U.S. Department of Health and Human Services. 2020. Available online: https://www.samhsa.gov/data/sites/default/files/reports/rpt32809/DAWN%20Profile%20Expanded.pdf (accessed on 28 December 2020).
- Wazaify, M.; Hughes, C.M.; McElnay, J.C. The implementation of a harm minimisation model for the identification and treatment of over-the-counter drug misuse and abuse in community pharmacies in Northern Ireland. Patient Educ. Couns. 2006, 64, 136–141. [Google Scholar] [CrossRef]
- Mobrad, A.M.; Alghadeer, S.; Syed, W.; Al-Arifi, M.N.; Azher, A.; Almetawazi, M.S.; Babelghaith, S.D. Knowledge, Attitudes, and Beliefs Regarding Drug Abuse and Misuse among Community Pharmacists in Saudi Arabia. Int. J. Environ. Res. Public Health 2020, 17, 1334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleming, G.F.; McElnay, J.C.; Hughes, C.M. Development of a community pharmacy-based model to identify and treat OTC drug abuse/misuse: A pilot study. Pharm. World Sci. 2004, 26, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Abood, E.A.; Wazaify, M. Abuse and Misuse of Prescription and Nonprescription Drugs from Community Pharmacies in Aden City—Yemen. Subst. Use Misuse 2016, 51, 942–947. [Google Scholar] [CrossRef] [PubMed]
- Leong, C.; Alessi-Severini, S.; Sareen, J.; Enns, M.W.; Bolton, J. Community Pharmacists’ Perspectives on Dispensing Medications with the Potential for Misuse, Diversion, and Intentional Overdose: Results of a Province-Wide Survey of Community Pharmacists in Canada. Subst. Use Misuse 2016, 51, 1724–1730. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R. Surveillance and uncertainty: Community pharmacy responses to over the counter medicine abuse. Health Soc. Care Community 2013, 21, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Cochran, G.T.; Engel, R.J.; Hruschak, V.J.; Tarter, R.E. Prescription Opioid Misuse Among Rural Community Pharmacy Patients: Pilot Study for Screening and Implications for Future Practice and Research. J. Pharm. Pr. 2016, 30, 498–505. [Google Scholar] [CrossRef]
- Zaprutko, T.; Koligat, D.; Michalak, M.; Wieczorek, M.; Józiak, M.; Ratajczak, P.; Szydłowska, K.; Miazek, J.; Kus, K.; Nowakowska, E. Misuse of OTC drugs in Poland. Health Policy 2016, 120, 875–881. [Google Scholar] [CrossRef]
- Eickhoff, C.; Hämmerlein, A.; Griese, N.; Schulz, M. Nature and frequency of drug-related problems in self-medication (over-the-counter drugs) in daily community pharmacy practice in Germany. Pharmacoepidemiol. Drug Saf. 2011, 21, 254–260. [Google Scholar] [CrossRef]
- Albsoul-Younes, A.; Wazaify, M.; Yousef, A.-M.; Tahaineh, L. Abuse and Misuse of Prescription and Nonprescription Drugs Sold in Community Pharmacies in Jordan. Subst. Use Misuse 2010, 45, 1319–1329. [Google Scholar] [CrossRef]
- Cochran, G.; Rubinstein, J.; Bacci, J.L.; Ylioja, T.; Tarter, R. Screening Community Pharmacy Patients for Risk of Prescription Opioid Misuse. J. Addict. Med. 2015, 9, 411–416. [Google Scholar] [CrossRef] [Green Version]
- Boeuf, O.; Lapeyre-Mestre, M. Survey of Forged Prescriptions to Investigate Risk of Psychoactive Medications Abuse in France. Drug Saf. 2007, 30, 265–276. [Google Scholar] [CrossRef]
- Lapeyre-Mestre, M.; Gony, M.; Carvajal, A.; Macías, D.; Conforti, A.; D’Incau, P.; Heerdink, R.; Van Der Stichele, R.; Bergman, U. The OSIAP Europe Study Group. A European Community Pharmacy-Based Survey to Investigate Patterns of Prescription Fraud through Identification of Falsified Prescriptions. Eur. Addict. Res. 2014, 20, 174–182. [Google Scholar] [CrossRef]
- Orriols, L.; Gaillard, J.; Lapeyre-Mestre, M.; Roussin, A.; Roussin, P.A. Evaluation of Abuse and Dependence on Drugs Used for Self-Medication. Drug Saf. 2009, 32, 859–873. [Google Scholar] [CrossRef]
- NIDA. Substance Use in Women. In: Research Report. National Institute on Drug Abuse. 2020. Available online: https://www.drugabuse.gov/publications/research-reports/substance-use-in-women/summary (accessed on 28 December 2020).
- NIDA. Misuse of Prescription Drugs. In: Research Report. National Institute on Drug Abuse. 2018. Available online: https://www.drugabuse.gov/publications/research-reports/misuse-prescription-drugs/overview (accessed on 6 October 2018).
- European Monitoring Centre for Drugs and Drug Addiction. Addressing the Misuse of Medicines. In: Policy and Practice Briefings. Available online: https://www.emcdda.europa.eu/best-practice/briefings/addressing-misuse-medicines_en (accessed on 6 October 2018).
- Schifano, F.; Chiappini, S.; Corkery, J.M.; Guirguis, A. An Insight into Z-Drug Abuse and Dependence: An Examination of Reports to the European Medicines Agency Database of Suspected Adverse Drug Reactions. Int. J. Neuropsychopharmacol. 2019, 22, 270–277. [Google Scholar] [CrossRef] [Green Version]
- Lee, T.; Bonnici, A.; Tamblyn, R.; McDonald, E.G. Inpatient Z-drug use commonly exceeds safe dosing recommendations. PLoS ONE 2017, 12, e0177645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Medicines Agency. PRAC Recommends Restrictions on the Use of Codeine for Cough and Cold in Children. In: European Medicines Agency’s Pharmacovigilance Risk Assessment Committee. 2015. Available online: https://www.ema.europa.eu/en/news/prac-recommends-restrictions-use-codeine-cough-cold-children (accessed on 5 September 2019).
- Roussin, A.; Géniaux, H.; Halberer, C.; D’Ouince, O.D. Un exemple d’évaluation de l’abus et de la dépendance en addictovigilance: À propos du tramadol. Therapies 2015, 70, 203–211. [Google Scholar] [CrossRef]
- Zabihi, E.; Hoseinzaadeh, A.; Emami, M.; Mardani, M.; Mahmoud, B.; Akbar, M.A. Potential for Tramadol Abuse by Patients Visiting Pharmacies in Northern Iran. Subst. Abus. Res. Treat. 2011, 5, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Layne, K.A.; Dargan, P.I.; Dines, A.M.; Leaper, C.; Yates, C.; Hovda, K.E.; Heyerdahl, F.; Archer, J.R.; Giraudon, I.; Wood, D.M.; et al. Acute toxicity related to misuse (nonmedical use) of tramadol: Experience of the European Drug Emergencies Network Plus. Br. J. Clin. Pharmacol. 2021, 87, 1668–1675. [Google Scholar] [CrossRef]
- Ms, M.A.S.; Mph, M.D.E.; Buchholtz, C.; Dasgupta, N.; Schnoll, S.H. Surveillance of Diversion and Nonmedical Use of Extended-Release Prescription Amphetamine and Oral Methylphenidate in the United States. J. Addict. Dis. 2013, 32, 26–38. [Google Scholar] [CrossRef]
- Faraone, S.V.; Rostain, A.L.; Montano, C.B.; Mason, O.; Antshel, K.; Newcorn, J.H. Systematic Review: Nonmedical Use of Prescription Stimulants: Risk Factors, Outcomes, and Risk Reduction Strategies. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 100–112. [Google Scholar] [CrossRef] [Green Version]
- Millar, J.; Sadasivan, S.; Weatherup, N.; Lutton, S. Lyrica nights-recreational pregabalin abuse in an urban emergency department. Emerg. Med. J. 2013, 30, 874. [Google Scholar] [CrossRef]
- Hägg, S.; Jönsson, A.K.; Ahlner, J. Current Evidence on Abuse and Misuse of Gabapentinoids. Drug Saf. 2020, 43, 1235–1254. [Google Scholar] [CrossRef]
- Evoy, K.E.; Morrison, M.D.; Saklad, S. Abuse and Misuse of Pregabalin and Gabapentin. Drugs 2017, 77, 403–426. [Google Scholar] [CrossRef]
- Fonseca, F.; Lenahan, W.; Dart, R.C.; Papaseit, E.; Dargan, P.I.; Wood, D.M.; Guareschi, M.; Maremmani, I.; Auriacombe, M.; Farré, M.; et al. Non-medical Use of Prescription Gabapentinoids (Gabapentin and Pregabalin) in Five European Countries. Front. Psychiatry 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Al-Khalaileh, W.; Abu-Farha, R.; Wazaify, M.; Van Hout, M.C. Ophthalmic drug abuse: An observational study from community pharmacies. Res. Soc. Adm. Pharm. 2019, 15, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Ponté, C.; Pi, C.; Palmaro, A.; Jouanjus, E.; Lapeyre-Mestre, M. Early signal of diverted use of tropicamide eye drops in France. Br. J. Clin. Pharmacol. 2017, 83, 1791–1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question Number | Question Text | Answer |
|---|---|---|
| 1 | Pharmacy ID | |
| 2 | Pharmacist | |
| 3 | Patient age | <25/25–25/36–45/46–65/> 65 |
| 4 | Patient sex | Male/Female |
| 5 | Patient origin | Native/Not native |
| 6 | Substance involved | Benzodiazepines/Buprenorphine/Clomethiazole/Codeine/Dextromethorphan/Fentanyl and related compounds/Methadone/Methylphenidate/Misoprostol/Modafinil/Tramadol/Others |
| 7 | Drug request | Does not require a prescription/Requested with prescription/Requested without prescription/Probably forged prescription |
| 8 | Intimidation | Yes/No |
| 9 | Frequent request | Yes/No |
| 10 | Pharmacist management | Supplied/Not supplied |
| 11 | Why do you supply the medicine? | |
| 12 | Observations |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perelló, M.; Rio-Aige, K.; Guayta-Escolies, R.; Gascón, P.; Rius, P.; Jambrina, A.M.; Bagaria, G.; Armelles, M.; Pérez-Cano, F.J.; Rabanal, M. Evaluation of Medicine Abuse Trends in Community Pharmacies: The Medicine Abuse Observatory (MAO) in a Region of Southern Europe. Int. J. Environ. Res. Public Health 2021, 18, 7818. https://doi.org/10.3390/ijerph18157818
Perelló M, Rio-Aige K, Guayta-Escolies R, Gascón P, Rius P, Jambrina AM, Bagaria G, Armelles M, Pérez-Cano FJ, Rabanal M. Evaluation of Medicine Abuse Trends in Community Pharmacies: The Medicine Abuse Observatory (MAO) in a Region of Southern Europe. International Journal of Environmental Research and Public Health. 2021; 18(15):7818. https://doi.org/10.3390/ijerph18157818
Chicago/Turabian StylePerelló, Maria, Karla Rio-Aige, Rafel Guayta-Escolies, Pilar Gascón, Pilar Rius, Anna M. Jambrina, Guillermo Bagaria, Mercè Armelles, Francisco José Pérez-Cano, and Manel Rabanal. 2021. "Evaluation of Medicine Abuse Trends in Community Pharmacies: The Medicine Abuse Observatory (MAO) in a Region of Southern Europe" International Journal of Environmental Research and Public Health 18, no. 15: 7818. https://doi.org/10.3390/ijerph18157818
APA StylePerelló, M., Rio-Aige, K., Guayta-Escolies, R., Gascón, P., Rius, P., Jambrina, A. M., Bagaria, G., Armelles, M., Pérez-Cano, F. J., & Rabanal, M. (2021). Evaluation of Medicine Abuse Trends in Community Pharmacies: The Medicine Abuse Observatory (MAO) in a Region of Southern Europe. International Journal of Environmental Research and Public Health, 18(15), 7818. https://doi.org/10.3390/ijerph18157818