
Whether Public Hospital Reform Affects the Hospital Choices of Patients in Urban Areas: New Evidence from Smart Card Data

Abstract
:1. Introduction
2. Literature Review
2.1. Hospital Allocation and Health Reforms
2.2. Reforms for Optimizing Hospital Utilization in China since 2009
3. Study Design
3.1. Case Study—Beijing’s Public Hospital Reform in 2017
3.2. Data Collection
3.3. Method for Inferring Health-Seeking Trips from Smart Card Data
4. Effects of Beijing’s 2017 Public Hospital Reform on Patients’ Hospital Choices
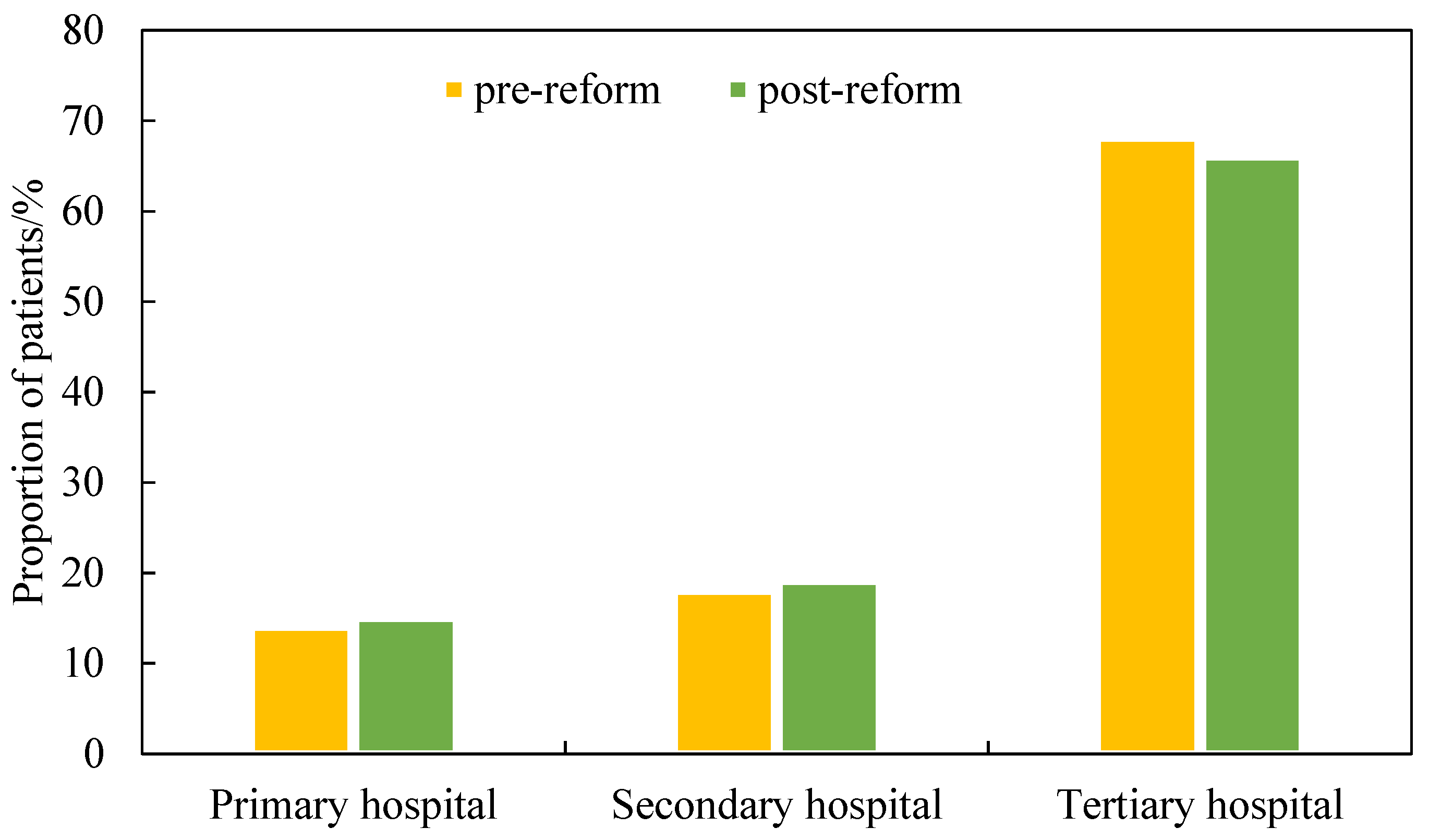
4.1. Tertiary Hospital Preference
4.2. Hospital Bypass
4.3. Efficiency of Patients’ Health-Seeking
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reform | Year | Measures on Medical Services | Measures on Drug Supply |
|---|---|---|---|
| Opinions on deepening the healthcare system reform. | 2009 | Completed the primary healthcare system and constructed primary healthcare facilities. | Introduced production, circulation, price, usage, and reimbursement policies for essential drugs. |
| Opinions on the pilot of public hospital reform. | 2010 | Completed the plan of the construction of primary healthcare facilities and implemented public hospital reform in pilot cities. | Implemented an essential drugs system in 60% of primary healthcare facilities and prioritized essential drugs in other healthcare facilities. |
| Opinions on the pilot of public hospital reform in urban areas. | 2015 | Built a compensation mechanism for reduced drug markups and implemented a relevant reform in pilot cities. | Removed drug price addition and reduced price of medical investigations. |
| Guiding opinions of the general office of the state council on pushing forward the formation of a hierarchical medical system. | 2015 | Differentiated the functions at different levels of hospital, enhanced the primary healthcare services, and promoted IT application in the medical system. | -- |
| Notice on promoting the pilot of a hierarchical medical system. | 2016 | Selected 266 cities as pilot cities to implement a hierarchical medical system, enhanced the primary healthcare services, established a family doctor system, and built a health service consortium. | -- |
| Notice on the implementation of a comprehensive public hospital reform. | 2017 | All cities should have issued a plan of comprehensive public hospital reform before 31 July 2017, and implemented it until 30 September 2017. | Removed drug markups (except Chinese Herbal Medicines) in all public hospitals until 30 September 2017. |
References
- Li, X.; Lu, J.; Hu, S.; Cheng, K.; Maeseneer, D.J.; Meng, Q.; Mossialos, E.; Xu, D.R.; Yip, W.; Zhang, H.; et al. The primary health-care system in China. Lancet 2017, 390, 2584–2594. [Google Scholar] [CrossRef]
- Liu, Y.; Kong, Q.; Esther, W.B. Public preferences for health care facilities in rural China: A discrete choice experiment. Soc. Sci. Med. 2019, 237, 112396. [Google Scholar] [CrossRef]
- Liaropoulos, L.; Tragakes, E. Public/private financing in the Greek health care system: Implications for equity. Health Policy 1998, 43, 153–169. [Google Scholar] [CrossRef]
- Wong, M.; Chau, P.H.; Goggins, W.; Woo, J. A geographical study of health services utilization among the elderly in Hong Kong: From spatial variations to health care implications. Health Serv. Insights 2009, 2, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Laksono, D.A.; Wulandari, D.R.; Soedirham, O. Urban and rural disparities in hospital utilization among Indonesian adults. Iran. J. Public Health 2019, 48, 247–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, P.H.; Theoharides, C. Health-seeking behavior and hospital choice in China’s New Cooperative Medical System. Health Econ. 2009, 18, S47–S64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, D.; Lam, T.; Lam, K.; Zhou, X.; Sun, K. Health reforms in China: The public’s choices for first-contact care in urban areas. Fam. Pract. 2017, 34, 194–200. [Google Scholar] [CrossRef] [Green Version]
- Jiang, S.; Min, R.; Fang, P. The impact of healthcare reform on the efficiency of public county hospitals in China. BMC Health Serv. Res. 2017, 17, 838. [Google Scholar] [CrossRef] [Green Version]
- Pan, X.; Kwan, M.P.; Yang, L.; Zhou, S.; Zuo, Z.; Wan, B. Evaluating the accessibility of healthcare facilities using an integrated catchment area approach. Int. J. Environ. Res. Public Health 2018, 15, 2051. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Du, F.; Huang, J.; Liu, Y. Access to hospitals: Potential vs. observed. Cities 2020, 100, 102671. [Google Scholar] [CrossRef]
- Kong, X.; Liu, Y.; Wang, Y.; Tong, D.; Zhang, J. Investigating public facility characteristics from a spatial interaction perspective: A case study of Beijing hospitals using taxi data. ISPRS Int. J. Geo-Inf. 2017, 6, 38. [Google Scholar] [CrossRef]
- Pelletier, M.P.; Trépanier, M.; Morency, C. Smart card data use in public transit: A literature review. Transp. Res. Part C Emerg. Technol. 2011, 19, 557–568. [Google Scholar] [CrossRef]
- Du, F.; Mao, L.; Wang, J.; Jin, H. Inferring transit-based health seeking patterns from smart card data—A case study in Beijing, China. Health Place 2020, 65, 102405. [Google Scholar] [CrossRef]
- Deng, J.; Sun, Y.; Lei, R.; Guo, Y.; Liu, J.; Yang, T. Status of healthcare workers after comprehensive reform of urban public hospitals in Beijing, China: Sustainable supply, psychological perception, and work outcomes. Hum. Resour. Health 2019, 17, 77. [Google Scholar] [CrossRef] [PubMed]
- Carli, R.; Dotoli, M.; Pellegrino, R.; Ranieri, L. Measuring and managing the smartness of cities: A framework for classifying performance indicators. In Proceedings of the 2013 IEEE International Conference on Systems, Man, and Cybernetics, Manchester, UK, 13–16 October 2013; pp. 1288–1293. [Google Scholar]
- Jiang, S.; Gu, Y.; Yang, F.; Wu, T.; Wang, H.; Cutler, H.; Zhang, L. Tertiary hospitals or community clinics? An enquiry into the factors affecting patients’ choice for healthcare facilities in urban China. China Econ. Rev. 2020, 63, 101538. [Google Scholar] [CrossRef]
- McGuirk, A.M.; Porell, W.F. Spatial patterns of hospital utilization: The impact of distance and time. Inquiry 1984, 21, 84–95. [Google Scholar]
- Rechel, B.; Džakul, A.; Duran, A.; Fattore, G.; Edwards, N.; Grignon, M.; Haas, M.; Habicht, T.; Marchildon, P.G.; Moreno, A.; et al. Hospitals in rural or remote areas: An exploratory review of policies in 8 high-income countries. Health Policy 2016, 120, 758–769. [Google Scholar] [CrossRef]
- Herberholz, C.; Phuntsho, S. Social capital, outpatient care utilization and choice between different levels of health facilities in rural and urban areas of Bhutan. Soc. Sci. Med. 2018, 211, 102–113. [Google Scholar] [CrossRef]
- Garrido, V.M.; Zentner, A.; Busse, R. The effects of gatekeeping: A systematic review of the literature. Scand. J. Prim. Health Care 2011, 29, 28–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godert, W.J.J.; Theodoor, J.P.P.; Maria, V.L.; Assendelft, W.J.J.; Westert, G.P.; Faber, M.J. Is the role as gatekeeper still feasible? A survey among Dutch general practitioners. Fam. Pract. 2014, 31, 538–544. [Google Scholar]
- Meng, Q.; Mills, A.; Wang, L.; Han, Q. What can we learn from China’s health system reform? BMJ 2019, 365, l2349. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Z.; Zhao, Y.; Shen, C.; Lai, S.; Nawaz, R.; Gao, J. Evaluating the effect of hierarchical medical system on health seeking behavior: A difference-in-differences analysis in China. Soc. Sci. Med. 2021, 268, 113372. [Google Scholar] [CrossRef]
- State Council of the People’s Republic of China. Opinions on Deepening the Healthcare System Reform. 2009. Available online: http://www.china.org.cn/government/scio-press-conferences/2009-04/09/content_17575378.htm (accessed on 1 April 2021).
- Ministry of Public Health of China; State Commission Office of Public Sectors Reform; State Development and Reform Commission; Ministry of Finance of the People’s Republic of China; Ministry of Human Resources and Social Security. Opinions on the Pilot of Public Hospital Reform. 2010. Available online: http://www.gov.cn/gzdt/2010-02/24/content_1540062.htm (accessed on 1 April 2021).
- State Council of The People’s Republic of China. Opinions on the Pilot of Public Hospital Reform in Urban Areas. 2015. Available online: http://www.gov.cn/zhengce/content/2015-05/17/content_9776.htm (accessed on 1 April 2021).
- National Health and Family Planning Commission; State Administration of Traditional Chinese Medicine. Notice on Promoting the Pilot of a Hierarchical Medical System. Available online: http://www.nhc.gov.cn/yzygj/s3593g/201608/7d264b533a3b403cb8348d40cfb9a9d3.shtml (accessed on 1 April 2021).
- State Council of The People’s Republic of China. Guiding Opinions of the General Office of the State Council on Pushing forward the Formation of a Hierarchical Medical System. 2016. Available online: http://www.gov.cn/zhengce/content/2015-09/11/content_10158.htm (accessed on 1 April 2021).
- National Health and Family Planning Commission; Ministry of Finance of The People’s Republic of China; State Commission Office of Public Sectors Reform; State Development and Reform Commission; Ministry of Human Resources and Social Security; State Administration of Chinese Traditional Medicine; Medical Reform Office of the State Council. Notice on the Implementation of a Comprehensive Public Hospital Reform. 2017. Available online: http://www.hnwsjsw.gov.cn/contents/409/30637.shtml (accessed on 1 April 2021).
- Lu, C.; Zhang, Z.X.; Lan, X.T. Impact of China’s referral reform on the equity and spatial accessibility of healthcare resources: A case study of Beijing. Soc. Sci. Med. 2019, 235, 112386. [Google Scholar] [CrossRef]
- Zeng, Y.; Xu, W.; Chen, L.; Chen, F.; Fang, Y. The Influencing factors of health-seeking preference and community health service utilization among patients in primary care reform in Xiamen, China. Patient Prefer. Adherence 2020, 14, 653–662. [Google Scholar] [CrossRef] [Green Version]
- Zhou, S.; Zhuang, Y.; Yang, S.; Ma, X.; Yuan, B.; Xu, J.; Fang, H.; Liu, X.; Meng, Q. The comprehensive reform of separating drug sales from medical services and its impact on outpatients and emergency medical flow in Beijing. Chin. J. Health Policy 2018, 11, 37–41. [Google Scholar]
- People’s Government of Beijing Municipality. Implementation Plan for Comprehensive Reform on Separating Drug Sales from Hospital Revenues. 2017. Available online: http://www.beijing.gov.cn/zhengce/zhengcefagui/201905/t20190522_60088.html (accessed on 1 April 2021).
- National Health Commission. China’s Health Statistics Yearbook 2018; Peking Union Medical College Press: Beijing, China, 2008.
- Baidu Map [GS (2015) 5218]. 2015. Available online: https://api.map.baidu.com/lbsapi/getpoint/index.html (accessed on 1 April 2015).
- Akin, J.; Hutchinson, P. Health-care facility choice and the phenomenon of bypassing. Health Policy Plan. 1999, 14, 135–151. [Google Scholar] [CrossRef] [Green Version]
- Sivey, P. The effect of waiting time and distance on hospital choice for English cataract patients. Health Econ. 2012, 21, 444–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, C.L.; Bundorf, K.M.; Kessler, P.D. The effect of hospital/physician integration on hospital choice. J. Health Econ. 2016, 50, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Bellamy, R.G.; McCormick, M. Patient bypass behavior and critical access hospitals: Implications for patient retention. J. Rural Health 2007, 23, 17–24. [Google Scholar] [CrossRef]
- Yang, G.; Song, C.; Shu, H.; Zhang, J.; Pei, T.; Zhou, C.H. Assessing patient bypass behavior using taxi trip origin-destination (OD) data. ISPRS Int. J. Geo-Inf. 2016, 5, 157. [Google Scholar] [CrossRef] [Green Version]
- Du, F.; Mao, L.; Wang, J. Determinants of travel mode choice for seeking healthcare: A comparison between elderly and non-elderly patients. J. Transp. Geogr. 2021, 92, 103023. [Google Scholar] [CrossRef]




| Tertiary Hospital | Secondary Hospital | Primary Hospital | ||||
|---|---|---|---|---|---|---|
| RF | MSF | RF | MSF | RF | MSF | |
| Junior physicians | 5 | 50 | 5 | 30 | 5 | 20 |
| Associate chief physician | 7 | 60 | 7 | 50 | 7 | 40 |
| Chief physician | 9 | 80 | 9 | 70 | 9 | 60 |
| Senior physicians | 14 | 100 | 14 | 90 | 14 | 80 |
| Card ID | Trip Leg ID | Operating Date | Boarding Stop | Alighting Stop | ||||
|---|---|---|---|---|---|---|---|---|
| Latitude | Longitude | Time | Latitude | Longitude | Time | |||
| 0101 | 1 | 11 April 2015 | 116.402 | 39.942 | 07:00:00 | 116.453 | 39.956 | 07:36:00 |
| 0101 | 2 | 11 April 2015 | 116.453 | 39.956 | 09:08:00 | 116.468 | 39.952 | 10:12:00 |
| 0101 | 3 | 11 April 2015 | 116:468 | 39.952 | 17:25:10 | 116.402 | 39.942 | 18:10:20 |
| 0012 | 1 | 6 June 2017 | 116.470 | 39.867 | 8:10:00 | 116.450 | 39.856 | 8:30:20 |
| 0012 | 2 | 6 June 2017 | 116.450 | 39.856 | 12:30:43 | 116.470 | 39.867 | 12:46:53 |
| 0050 | 1 | 7 June 2017 | 116.398 | 39.975 | 11:30:35 | 116.444 | 39.711 | 12:30:40 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Du, F.; Wang, J.; Jin, H. Whether Public Hospital Reform Affects the Hospital Choices of Patients in Urban Areas: New Evidence from Smart Card Data. Int. J. Environ. Res. Public Health 2021, 18, 8037. https://doi.org/10.3390/ijerph18158037
Du F, Wang J, Jin H. Whether Public Hospital Reform Affects the Hospital Choices of Patients in Urban Areas: New Evidence from Smart Card Data. International Journal of Environmental Research and Public Health. 2021; 18(15):8037. https://doi.org/10.3390/ijerph18158037
Chicago/Turabian StyleDu, Fangye, Jiaoe Wang, and Haitao Jin. 2021. "Whether Public Hospital Reform Affects the Hospital Choices of Patients in Urban Areas: New Evidence from Smart Card Data" International Journal of Environmental Research and Public Health 18, no. 15: 8037. https://doi.org/10.3390/ijerph18158037