
Enhancing Teaching Recovery Techniques (TRT) with Parenting Skills: RCT of TRT + Parenting with Trauma-Affected Syrian Refugees in Lebanon Utilising Remote Training with Implications for Insecure Contexts and COVID-19 †


 ,
,
Abstract
:1. Introduction
The Current Study
2. Materials and Methods
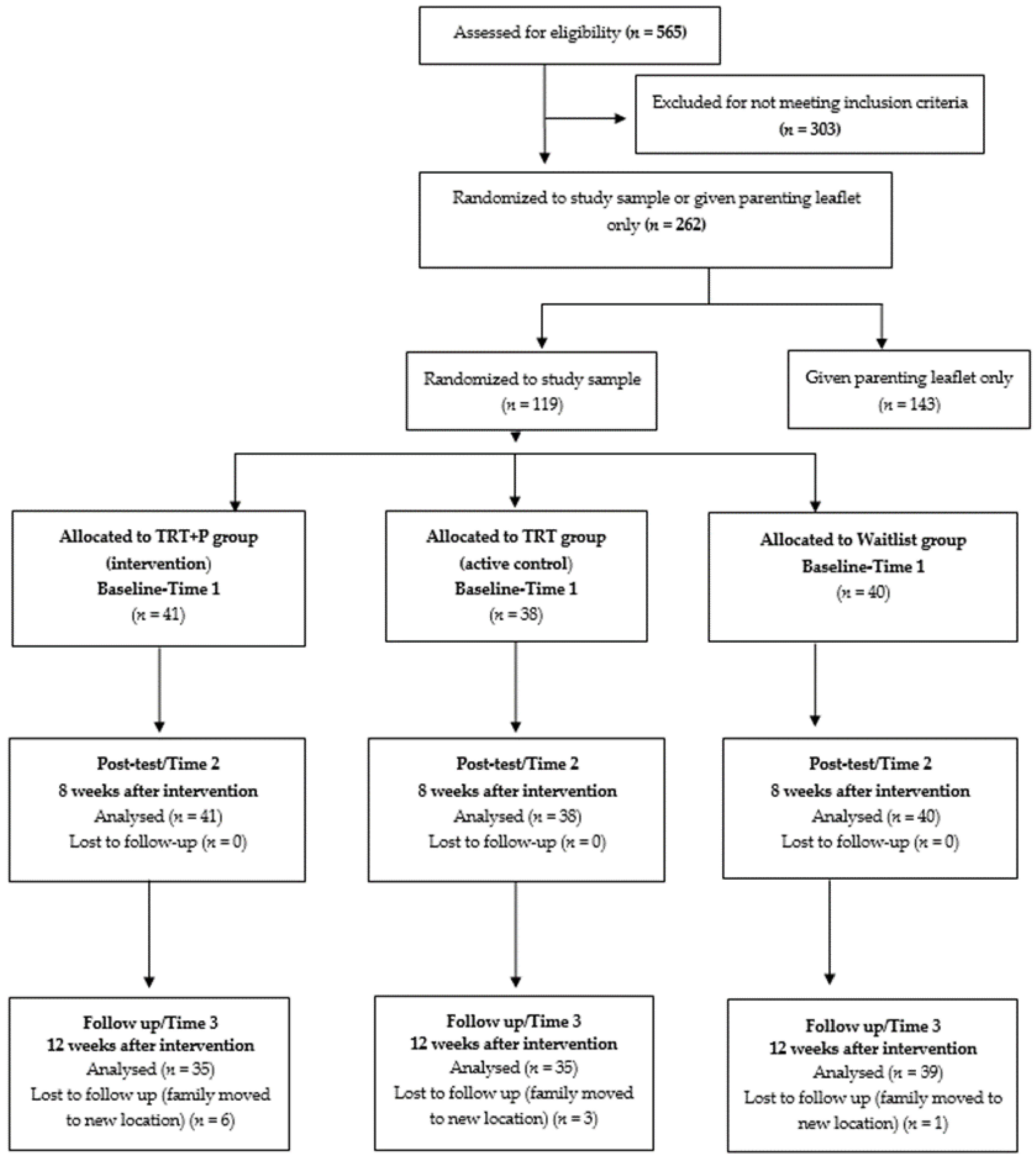
2.1. Study Design
2.2. Study Setting
2.3. Ethics and Governance
2.4. The Intervention
2.5. Participants and Eligibility Criteria
2.6. Recruitment of Participants and Consent Procedures
2.7. Randomisation
2.8. Programme Delivery and Fidelity
2.9. Recruitment of Staff for Intervention and Study Delivery
2.10. Outcomes and Measures
2.10.1. Child Mental Health
Post-Traumatic Stress
2.10.2. Depression and Anxiety
2.10.3. Parenting
2.10.4. Caregiver Mental Health
2.11. Methods
Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
3.2. Feasibility of Engaging and Retaining Families in the Study
3.3. Child Mental Health
3.3.1. Post-Traumatic Stress
3.3.2. Depression
3.3.3. Anxiety
The Screen for Childhood Anxiety Related Disorders (SCARED): Child Version
The Screen for Childhood Anxiety Related Disorders (SCARED): Parent Version
3.3.4. Parent-Administered Measures
The Strengths and Difficulties Questionnaire (SDQ)
3.4. Caregiver Mental Health
3.4.1. Post-Traumatic Stress
The Impact of Events Scale Revised (IES-R)
3.4.2. Depression, Anxiety, and Stress
The Depression–Anxiety–Stress Scale (DASS)
3.5. Parenting Skills and Confidence
3.5.1. The Parenting Scale (PS)
3.5.2. Parenting Confidence
Parenting Sense of Competence (PSOC)
4. Discussion
Implications for Utilising Remote Training during and after COVID-19
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| T1 | T2 | T3 | |
| Child Mental Health | |||
| Post-Traumatic Stress Scale (CRIES 13) | |||
| Intrusion | 0.304 | 0.651 | 0.766 |
| Avoidance | −0.012 * | 0.710 | 0.818 |
| Arousal | 0.557 | 0.640 | 0.728 |
| Depression Scale (Total DSRS) | 0.782 | 0.764 | 0.832 |
| Anxiety Scale (Total SCARED—child version) | 0.879 | 0.928 | 0.944 |
| Anxiety Scale (Total SCARED—parent version) | 0.886 | 0.895 | 0.935 |
| Aggression/Behavioural Problem Scale (Total SDQ) | 0.550 | 0.599 | 0.661 |
| Caregiver Mental Health | |||
| Post-Traumatic Stress Scale (Total IES-R) | 0.900 | 0.902 | 0.939 |
| Depression, Anxiety and Stress Scale | |||
| Stress | 0.793 | 0.847 | 0.847 |
| Anxiety | 0.862 | 0.841 | 0.858 |
| Depression | 0.831 | 0.835 | 0.837 |
| Parental Skills Confidence Scale (Total PS) | 0.408 | 0.221 | 0.365 |
| Parental Confidence Scale (Total PSOC) | 0.303 | 0.344 | 0.422 |
References
- UNHCR. Operational Portal Refugee Situations. 2020. Available online: http://data2.unhcr.org/en/situations/syria (accessed on 25 June 2021).
- Save the Children. Stop the War on Children: Protecting Children in 21st Century Conflict. Available online: https://www.savethechildren.org/content/dam/usa/reports/ed-cp/stop-the-war-on-children-2019.pdf (accessed on 25 June 2021).
- Ahmad, I.; Smetana, J.; Klimstra, T. Maternal Monitoring, adolescent disclosure and adolescent adjustment among Palestinian refugee youth in Jordan. J. Res. Adolescence 2015, 25, 403–411. [Google Scholar] [CrossRef]
- Eruyar, S.; Huemer, J.; Vostanis, P. How should child mental health services respond to the refugee crisis? Child Adolesc. Ment. Health 2018, 23, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Blackmore, R.; Gray, M.; Boyle, J.; Fazel, M.; Ranasinha, S.; Fitzgerald, G.; Gibson-Helm, M. Systematic review and meta-analysis: The prevalence of mental illness in child and adolescent refugees and asylum seekers. J. Am. Acad. Child Adolesc. Psychiatry 2019, 59, 705–714. [Google Scholar] [CrossRef]
- Hendrickx, M.; Woodward, A.; Fuhr, D.; Sondorp, E.; Roberts, B. The burden of mental disorders and access to mental health and psychosocial support services in Syria and among Syrian refugees in neighbouring countries: A systematic review. J. Public Health 2020, 42, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Barbui, C.; Purgato, M.; Abdulmalik, J.; Acarturk, C.; Eaton, J.; Gastaldon, C.; Nosè, M. Efficacy of psychosocial interventions for mental health outcomes in low-income and middle-income countries: An umbrella review. Lancet Psychiatry 2020, 7, 162–172. [Google Scholar] [CrossRef]
- Sim, A.; Fazel, M.; Bowes, L.; Gardner, F. Pathways linking war and displacement to parenting and child adjustment: A qualitative study with Syrian refugees in Lebanon. Soc. Sci. Med. 2018, 200, 19–26. [Google Scholar] [CrossRef]
- Betancourt, T.; McBain, R.; Newnham, E.; Brennan, R. The intergenerational impact of war: Longitudinal relationships between caregiver and child mental health in post conflict Sierra Leone. J. Child Psychol. Psychiatry 2015, 56, 1101–1107. [Google Scholar] [CrossRef]
- Newnham, E.; Kashyap, S.; Tearne, J.; Fazel, M. Child mental health in the context of war: An overview of risk factors and interventions for refugee and war-affected youth. In Mental Health of Refugee and Conflict-Affected Populations; Springer: Cham, Switzerland, 2018; pp. 37–63. [Google Scholar]
- Miller, K.; Koppenol-Gonzalez, G.; Arnous, M.; Tossyeh, F.; Chen, A.; Nahas, N.; Jordans, M. Supporting Syrian families displaced by armed conflict: A pilot randomized controlled trial of the caregiver support intervention. Child Abus. Negl. 2020, 106, 104–512. [Google Scholar] [CrossRef]
- Catani, C. Mental health of children living in war zones: A risk and protection perspective. World Psychiatry 2018, 17, 104–143. [Google Scholar] [CrossRef]
- Arenliu, A.; Bertelsen, N.; Saad, R.; Abdulaziz, H.; Weine, S. War and displacement stressors and coping mechanisms of Syrian urban refugee families living in Istanbul. J. Fam. Psychol. 2019, 7, 392–401. [Google Scholar] [CrossRef] [PubMed]
- Diab, M.; Peltonen, K.; Qouta, S.; Palosaari, E.; Punamäki, R. Effectiveness of psychosocial intervention enhancing resilience among war-affected children and the moderating role of family factors. Child Abus. Negl. 2015, 40, 24–35. [Google Scholar] [CrossRef]
- Fayyad, J.; Cordahi-Tabet, C.; Yeretzian, J.; Salamoun, M.; Najm, C.; Karam, E. Resilience-promoting factors in war-exposed adolescents: An epidemiologic study. Eur. Child Adolesc. Psychiatry 2017, 26, 191–200. [Google Scholar] [CrossRef]
- UNODC. Guide to Implementing Family skills Training Programmes for Drug Abuse Prevention; United Nations Office on Drugs and Crime: Vienna, Austria, 2009; Available online: https://www.unodc.org/documents/prevention/family-guidelines-E.pdf (accessed on 25 June 2021).
- Yoon, D.; Yoon, S.; Yoon, M.; Snyder, S. Developmental trajectories of deviant peer affiliation in adolescence: Associations with types of child maltreatment and substance use. Child. Youth Serv. Rev. 2019, 105, 104–121. [Google Scholar] [CrossRef]
- Denov, M.; Fennig, M.; Rabiau, M.; Shevell, M. Intergenerational resilience in families affected by war, displacement, and migration: “It runs in the family”. J. Fam. Soc. Work 2019, 22, 17–45. [Google Scholar] [CrossRef]
- Maalouf, W.; Campello, G. The influence of family skills programmes on violence indicators: Experience from a multi-site project of the United Nations Office on Drugs and Crime in low and middle income countries. Aggress. Violent Behav. 2014, 19, 616–624. [Google Scholar] [CrossRef]
- Vlahovicova, K.; Melendez-Torres, G.; Leijten, P.; Knerr, W.; Gardner, F. Parenting programs for the prevention of child physical abuse recurrence: A systematic review and meta-analysis. Clin. Child Fam. Psychol. Rev. 2017, 20, 351–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eltanamly, H.; Leijten, P.; Jak, S.; Overbeek, G. Parenting in times of war: A meta-analysis and qualitative synthesis of war exposure, parenting, and child adjustment. Trauma Violence Abus. 2021, 22, 146–160. [Google Scholar] [CrossRef] [PubMed]
- Murphy, K.M.; Rodrigues, K.; Costigan, J.; Annan, J. Raising children in conflict: An integrative model of parenting in war. Peace Confl. J. Peace Psychol. 2017, 23, 40–46. [Google Scholar] [CrossRef]
- El-Khani, A.; Maalouf, W.; Baker, D.A.; Zahra, N.; Noubani, A.; Cartwright, K. Caregiving for children through conflict and displacement: A pilot study testing the feasibility of delivering and evaluating a light touch parenting intervention for caregivers in the West Bank. Int. J. Psychol. 2019, 55, 26–39. [Google Scholar] [CrossRef]
- Lakkis, N.; Osman, M.; Aoude, L.; Maalouf, C.; Issa, H.G.; Issa, G.M. A pilot intervention to promote positive parenting in refugees from Syria in Lebanon and Jordan. Front. Psychiatry 2020, 11, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.E.; Ghalayini, H.; Arnous, M.; Tossyeh, F.; Chen, A.; van den Broek, M.; Jordans, M. Strengthening parenting in conflict-affected communities: Development of the caregiver support intervention. Glob. Ment. Health 2020, 7, e14. [Google Scholar] [CrossRef]
- UNHCR. The UN Refugee Agency. Global Trends Forced Displacement in 2019. 2020. Available online: https://www.unhcr.org/5ee200e37.pdf (accessed on 25 June 2021).
- Miles, E.; Narayan, A.; Watamura, S. Syrian caregivers in perimigration: A systematic review from an ecological systems perspective. Transl. Issues Psychol. Sci. 2019, 5, 78–86. [Google Scholar] [CrossRef]
- Scharpf, F.; Kaltenbach, E.; Nickerson, A.; Hecker, T. A systematic review of socio-ecological factors contributing to risk and protection of the mental health of refugee children and adolescents. Clin. Psychol. Rev. 2020, 83, 101930. [Google Scholar] [CrossRef]
- Silove, D.; Ventevogel, P.; Rees, S. The contemporary refugee crisis: An overview of mental health challenges. World Psychiatry 2017, 16, 130–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassan, G.; Kirmayer, L.; Mekki-Berrada, A.; Quosh, C.; El Chammay, R.; Deville-Stoetzel, J.; Song, S. Culture, Context and the Mental Health and Psychosocial Wellbeing of Syrians: A Review for Mental Health and Psychosocial Support Staff Working with Syrians Affected by Armed Conflict; UNHCR: Geneva, Switzerland, 2015; pp. 14–15. [Google Scholar]
- El-Khani, A.; Ulph, F.; Peters, S.; Calam, R. Syria: The challenges of parenting in refugee situations of immediate displacement. Intervention 2016, 14, 99–113. [Google Scholar] [CrossRef]
- El-Khani, A.; Cartwright, K.; Redmond, A.; Calam, R. Daily bread: A novel vehicle for dissemination and evaluation of psychological first aid for families exposed to armed conflict in Syria. Glob. Ment. Health 2016, 3, e15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yule, W.; Dyregrov, A.; Raundalen, M.; Smith, P. Children and war: The work of the Children and War Foundation. Eur. J. Psychotraumatol. 2013, 4, 18424. [Google Scholar] [CrossRef] [Green Version]
- Barron, I.; Abdallah, G.; Heltne, U. Randomized control trial of Teaching Recovery Techniques in rural occupied Palestine: Effect on adolescent dissociation. J. Aggress. Maltreat. Trauma 2016, 25, 955–973. [Google Scholar] [CrossRef] [Green Version]
- Qouta, S.; Palosaari, E.; Diab, M.; Punamäki, R. Intervention effectiveness among war-affected children: A cluster randomized controlled trial on improving mental health. J. Trauma. Stress 2012, 25, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Sarkadi, A.; Ådahl, K.; Stenvall, E.; Ssegonja, R.; Batti, H.; Gavra, P.; Salari, R. Teaching recovery techniques: Evaluation of a group intervention for unaccompanied refugee minors with symptoms of PTSD in Sweden. Eur. Child Adolesc. Psychiatry 2018, 27, 467–479. [Google Scholar] [CrossRef] [Green Version]
- Almoshmosh, N.; Mobayed, M.; Aljendi, M. Mental health and psychosocial needs of Syrian refugees and the role of Syrian non-governmental organisations. Br. J. Psychiatry Int. 2016, 3, 81–83. [Google Scholar] [CrossRef] [Green Version]
- Abbara, A.; Coutts, A.; Fouad, F.; Ismail, S.; Orcutt, M. Syria Public Health Network. Mental health among displaced Syrians: Findings from the Syria Public Health Network. J. R. Soc. Med. 2016, 109, 88–90. [Google Scholar] [CrossRef] [Green Version]
- Campello, G.; Heikkila, H.; Maalouf, W. International standards on drug use prevention. In The Cambridge Handbook of International Prevention Science; Cambridge University Press: Cambridge, UK, 2016; pp. 134–159. [Google Scholar]
- Bentovim, A.; Elliott, I. Hope for children and families: Targeting abusive parenting and the associated impairment of children. J. Clin. Child Adolesc. Psychol. 2014, 43, 270–285. [Google Scholar] [CrossRef]
- Perrin, S.; Meiser-Stedman, R.; Smith, P. The Children’s Revised Impact of Event Scale (CRIES): Validity as a screening instrument for PTSD. Behav. Cogn. Psychother. 2005, 33, 487–498. [Google Scholar] [CrossRef] [Green Version]
- Yule, W.; Smith, P.; Perrin, S. Training helpers for Bosnian children with PTSD. In Proceedings of the International Congress, Royal College of Psychiatrists, London, UK, 22–25 June 1998. [Google Scholar]
- Deeba, F.; Rapee, R.; Prvan, T. Psychometric properties of the Children’s Revised Impact of Events Scale (CRIES) with Bangladeshi children and adolescents. Peer J. 2014, 2, e536. [Google Scholar] [CrossRef] [Green Version]
- Birleson, P. The validity of depressive disorder in childhood and the development of a self-rating scale: A research report. Child Psychol. Psychiatry Allied Discip. 1981, 22, 73–88. [Google Scholar] [CrossRef]
- Ivarsson, T.; Gillberg, C.; Arvidsson, T.; Broberg, A. The Youth Self-Report (YSR) and the Depression Self-Rating Scale (DSRS) as measures of depression and suicidality among adolescents. Eur. Child Adolesc. Psychiatry 2002, 11, 31–37. [Google Scholar] [CrossRef]
- Birmaher, B.; Khetarpal, S.; Brent, D.; Cully, M.; Balach, L.; Kaufman, J.; Neer, S. The screen for child anxiety related emotional disorders (SCARED): Scale construction and psychometric characteristics. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Arab, A.; El Keshky, M.; Hadwin, J. Psychometric properties of the screen for child anxiety related emotional disorders (SCARED) in a non-clinical sample of children and adolescents in Saudi Arabia. Child Psychiatry Hum. Dev. 2016, 47, 554–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodman, R. The strengths and difficulties questionnaire: A research note. J. Child Psychol. Psychiatry Allied Discip. 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Goodman, R. Psychometric properties of the Strengths and Difficulties Questionnaire. J. Am. Acad. Child. Adolesc. Psychiatry 2001, 40, 1337–1345. [Google Scholar] [CrossRef]
- Mullick, M.; Goodman, R. Questionnaire screening for mental health problems in Bangladeshi children: A preliminary study. Soc. Psychiatry Epidemiol. 2001, 36, 94–99. [Google Scholar] [CrossRef]
- Arnold, D.; O’leary, S.; Wolff, L.; Acker, M. The Parenting Scale: A measure of dysfunctional parenting in discipline situations. Psychol. Assess. 1993, 5, 137–142. [Google Scholar] [CrossRef]
- Lorber, M.; Xu, S.; Slep, A.; Bulling, L.; Leary, S. A new look at the psychometrics of the Parenting Scale through the lens of item response theory. J. Clin. Child Adolesc. Psychol. 2014, 43, 613–626. [Google Scholar] [CrossRef] [Green Version]
- Christianson, S.; Marren, J. The impact of event scale-revised (IES-R). Medsurg. Nurs. 2012, 21, 321–322. [Google Scholar] [PubMed]
- Asukai, N.; Kato, H.; Kawamura, N.; Kim, Y.; Yamamoto, K.; Kishimoto, J.; Nishizono-Maher, A. Reliabiligy and validity of the Japanese-language version of the impact of event scale-revised (Ies-RJ): Four studies of different traumatic events. J. Nerv. Ment. Dis. 2002, 190, 175–182. [Google Scholar] [CrossRef]
- Beck, J.G.; Grant, D.; Read, J.; Clapp, J.; Coffey, S.; Miller, L.; Palyo, S. The impact of event scale-revised: Psychometric properties in a sample of motor vehicle accident survivors. J. Anxiety Disord. 2008, 22, 187–198. [Google Scholar] [CrossRef] [Green Version]
- Lovibond, P.; Lovibond, S. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, K.; De Boer, A.; Verbeek, J.; Blonk, R.; Van Dijk, F. The Depression Anxiety Stress Scales (DASS): Detecting anxiety disorder and depression in employees absent from work because of mental health problems. Occup. Environ. Med. 2003, 60 (Suppl. 1), i77–i82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barlow, J.; Smailagic, N.; Huband, N.; Roloff, V.; Bennett, C. Group-based parent training programmes for improving parental psychosocial health. Cochrane Database Syst. Rev. 2014, 5, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Hasha, W.; Fadnes, L.; Igland, J.; Vårdal, R.; Giusti, L.; Strømme, E.; Diaz, E. Two interventions to treat pain disorders and post-traumatic symptoms among Syrian refugees: Protocol for a randomized controlled trial. Trials 2019, 20, 784. [Google Scholar] [CrossRef] [PubMed]
- Fazel, M.; Betancourt, T. Preventive mental health interventions for refugee children and adolescents in high-income settings. Lancet Child Adolesc. Health 2018, 2, 121–132. [Google Scholar] [CrossRef] [Green Version]
- Cioffi, C.; Leve, L. Substance use disorder treatment, parenting, and COVID-19. J. Subst. Abus. Treat. 2020, 119, 108148. [Google Scholar] [CrossRef]
- El-Khani, A.; Haar, K.; AlKurdi, M.; Calam, R.; Maalouf, W. Testing the effectiveness of TRT Plus parenting responding to the Beirut port blast. 2021. in preparation. [Google Scholar]

| Personal Characteristics | TRT + P N (%) n = 41 | TRTN (%) n = 38 | Waitlist N (%) n = 40 | X2 | p-Value | |
|---|---|---|---|---|---|---|
| Gender of Caregiver | Male | 2 (1.7%) | 7 (5.9%) | 8 (6.7%) | 4.561 | 0.102 |
| Female | 39 (32.8%) | 31 (26.1%) | 32 (26.9%) | |||
| Marital Status of Caregiver | Married | 37 (31.1%) | 32 (26.9%) | 37 (31.1%) | 6.694 | 0.350 |
| Divorced/separated | 0 (0%) | 1 (0.8%) | 0 (0%) | |||
| Single | 0 (0%) | 2 (1.7%) | 0 (0%) | |||
| Cohabiting | 0 (0%) | 0 (0%) | 0 (0%) | |||
| Widow | 4 (3.4%) | 3 (2.5%) | 3 (2.5%) | |||
| Highest Education | Primary school or less | 24 (20.2%) | 13 (10.9%) | 27 (22.7%) | 11.798 | 0.067 |
| Some high school | 13 (10.9%) | 15 (12.6%) | 8 (6.7%) | |||
| Completed high school | 3 (2.5%) | 4 (3.4%) | 2 (1.7%) | |||
| Trade/technical school | 0 (0%) | 0 (0%) | 0 (0%) | |||
| University degree | 1 (0.8%) | 6 (5.0%) | 3 (2.5%) | |||
| Postgraduate degree | 0 (0%) | 0 (0%) | 0 (0%) | |||
| Current Employment | Not working | 34 (28.6%) | 22 (18.5%) | 30 (25.2%) | 8.695 | 0.191 |
| Full-time job | 1 (0.8%) | 6 (5.0%) | 5 (4.2%) | |||
| Part-time job | 2 (1.7%) | 4 (3.4%) | 3 (2.5%) | |||
| Looking for a job | 4 (3.4%) | 6 (5.0%) | 2 (1.7%) | |||
| Home-based paid work | 0 (0%) | 0 (0%) | 0 (0%) | |||
| N/A | 0 (0%) | 0 (0%) | 0 (0%) | |||
| Child Mental Health | ||||||||
| Post-Traumatic Stress | ||||||||
| CRIES 13 | t1 | t2 | t3 | Statistical Test Results | ||||
| N | Mean (SD) | N | Mean (SD) | N | Mean (SD) | |||
| Intrusion | TRT + P | 41 | 15.80 (3.41) | 41 | 7.68 (4.03) | 35 | 3.75 (2.53) | F(1.894,219.688) = 174.344 p < 0.001 □ ⬟ |
| TRT | 36 | 13.74 (3.76) | 38 | 8.92 (4.15) | 35 | 5.41 (4.25) | ||
| Waitlist | 40 | 13.45 (4.08) | 40 | 11.05 (3.92) | 38 | 8.71 (4.09) | ||
| Difference between groups | F(2,116) = 4.729 p = 0.011 † ⬟ | F(2,116) = 7.197 p = 0.001 ⬟ | χ2(2) = 30.314 p < 0.001 □ ⬟ | |||||
| Avoidance | TRT + P | 41 | 14.00 (3.76) | 40 | 8.43 (5.04) | 34 | 4.10 (3.14) | F(2,115) = 77.778 p < 0.001 ⬟ |
| TRT | 38 | 13.32 (3.76) | 38 | 9.74 (5.28) | 35 | 7.19 (5.95) | ||
| Waitlist | 40 | 12.75 (4.00) | 38 | 10.87 (3.94) | 37 | 8.90 (4.68) | ||
| Difference between groups | F(2,116) = 1.075 p = 0.345 | F(2,116) = 2.645 p = 0.075 | χ2(2) = 20.931 p < 0.001 † □ ⬟ | |||||
| Arousal | TRT + P | 41 | 13.76 (6.63) | 40 | 8.68 (3.90) | 34 | 4.98 (3.54) | F(1.798,208.608) = 42.762 p < 0.001 □ ⬟ |
| TRT | 38 | 12.00 (5.61) | 38 | 7.84 (5.26) | 35 | 6.22 (4.70) | ||
| Waitlist | 40 | 12.13 (5.68) | 39 | 12.98 (5.76) | 39 | 10.20 (4.66) | ||
| Difference between groups | F(2,116) = 1.071 p = 0.346 | F(2,116) = 11.894 p < 0.001 □ ⬟ | χ2(2) = 30.085 p < 0.001 □ ⬟ | |||||
| Depression | ||||||||
| DSRS | t1 | t2 | t3 | Statistical test results | ||||
| N | Mean (SD) | n | Mean (SD) | n | Mean (SD) | |||
| Total score | TRT + P | 37 | 13.62 (5.64) | 40 | 8.35 (5.28) | 32 | 8.73 (4.33) | F(1.806,209.472) = 11.74 p < 0.001 |
| TRT | 32 | 13.32 (5.86) | 36 | 9.67 (4.66) | 33 | 10.57 (5.60) | ||
| Waitlist | 37 | 11.34 (6.52) | 36 | 11.83 (4.09) | 36 | 12.86 (6.23) | ||
| Difference between groups | F(2,116) = 1.694 p = 0.188 | F(2,116) = 5.629 p = 0.005 ⬟ | F(2,116) = 5.586 p = 0.005 ⬟ | |||||
| Anxiety | ||||||||
| SCARED child version | t1 | t2 | t3 | Statistical test results | ||||
| Mean (SD) | Mean (SD) | Mean (SD) | ||||||
| Total score | TRT + P | 35.14 (12.11) | 22.98 (12.17) | 20.69 (8.59) | F(2,115) = 34.942 p < 0.001 | |||
| TRT | 34.15 (13.19) | 22.56 (14.25) | 22.71 (14.75) | |||||
| Waitlist | 34.66 (13.69) | 27.02 (13.30) | 31.99 (14.04) | |||||
| Difference between groups | F(2,116) = 0.058 p = 0.944 | χ2(2) = 4.778 p = 0.092 | F(2,116) = 9.042 p < 0.001 □ ⬟ | |||||
| SCARED parent version | t1 | t2 | t3 | Statistical test results | ||||
| N | Mean (SD) | n | Mean (SD) | n | Mean (SD) | |||
| Total score | TRT + P | 31 | 31.52 (13.53) | 34 | 18.51 (11.09) | 24 | 18.93 (7.65) | F(2,115) = 17.412 p < 0.001 |
| TRT | 26 | 29.63 (11.22) | 32 | 23.54 (11.67) | 32 | 22.05 (10.56) | ||
| Waitlist | 25 | 24.87 (10.37) | 35 | 24.34 (8.32) | 34 | 32.99 (14.73) | ||
| Difference between groups | F(2,116) = 3.396 p = 0.037 ⬟ | F(2,116) = 3.702 p = 0.028 ⬟ | F(2,116) = 17.013 p < 0.001 □ ⬟ | |||||
| Aggression/Behavioural problems | ||||||||
| SDQ | t1 | t2 | t3 | Statistical test results | ||||
| N | Mean (SD) | n | Mean (SD) | n | Mean (SD) | |||
| Total Difficulty score | TRT + P | 40 | 16.75 (5.22) | 38 | 12.75 (4.10) | 33 | 14.17 (5.09) | F(2,115) = 7.389 p = 0.001 |
| TRT | 37 | 15.60 (4.53) | 36 | 14.62 (4.68) | 32 | 13.89 (5.24) | ||
| Waitlist | 37 | 15.05 (3.63) | 37 | 14.35 (4.36) | 37 | 14.97 (4.13) | ||
| Difference between groups | F(2,116) = 1.485 p = 0.231 | F(2,116) = 2.132 p = 0.123 | F(2,116) = 0.526 p = 0.592 | |||||
| CAREGIVER MENTAL HEALTH | ||||||||
| Post-traumatic stress | ||||||||
| IES-R | t1 | t2 | t3 | Statistical test results | ||||
| N | Mean (SD) | n | Mean (SD) | n | Mean (SD) | |||
| Total sum | TRT + P | 39 | 41.27 (16.58) | 40 | 18.39 (8.47) | 32 | 18.54 (8.08) | F(2,115) = 119.064 p < 0.001 ⬟ |
| TRT | 32 | 40.62 (13.62) | 37 | 23.96 (10.12) | 35 | 18.80 (9.89) | ||
| Waitlist | 38 | 41.46 (12.50) | 32 | 27.12 (13.27) | 33 | 29.00 (14.29) | ||
| Difference between groups | F(2,116) = 0.037 p = 0.964 | F(2,116) = 6.800 p = 0.002 ⬟ | F(2,116) = 11.586 p < 0.001 □ ⬟ | |||||
| Depression, Anxiety and Stress | ||||||||
| DASS | t1 | t2 | t3 | Statistical test results | ||||
| n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | |||
| Stress | TRT + P | 41 | 24.88 (8.31) | 41 | 13.22 (7.92) | 34 | 12.44 (5.77) | F(2,115) = 49.400 p < 0.001 |
| TRT | 38 | 21.16 (9.60) | 37 | 15.59 (9.08) | 35 | 14.27 (6.89) | ||
| Waitlist | 38 | 23.08 (7.84) | 38 | 17.63 (7.42) | 38 | 17.56 (8.54) | ||
| Difference between groups | F(2,116) = 1.847 p = 0.162 | F(2,116) = 2.975 p = 0.055 | F(2,116) = 5.309 p = 0.006 ⬟ | |||||
| Anxiety | TRT + P | 41 | 17.46 (12.59) | 40 | 7.05 (8.04) | 34 | 8.48 (4.70) | F(1.814,210.463) = 33.777 p < 0.001 |
| TRT | 37 | 17.00 (10.67) | 38 | 9.89 (9.10) | 35 | 10.62 (8.44) | ||
| Waitlist | 39 | 16.22 (9.80) | 40 | 10.35 (6.70) | 39 | 12.46 (9.14) | ||
| Difference between groups | F(2,116) = 0.130 p = 0.879 | χ2(2) = 8.350 p = 0.015 ⬟ | χ2(2) = 2.130 p = 0.345 | |||||
| Depression | TRT + P | 39 | 24.40 (8.96) | 41 | 10.98 (7.56) | 35 | 10.50 (5.60) | F(1.850,214.655) = 75.631 p < 0.001 |
| TRT | 37 | 19.87 (10.56) | 37 | 12.68 (8.33) | 35 | 11.09 (7.32) | ||
| Waitlist | 37 | 23.60 (8.37) | 40 | 16.60 (7.95) | 38 | 15.70 (8.82) | ||
| Difference between groups | F(2,116) = 2.623 p = 0.077 | F(2,116) = 5.306 p = 0.006 ⬟ | F(2,116) = 5.997 p = 0.003 □ ⬟ | |||||
| PARENTING | ||||||||
| Parent Skills and Confidence | ||||||||
| PS | t1 | t2 | t3 | Statistical test results | ||||
| n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | |||
| Total score | TRT + P | 41 | 4.04 (0.48) | 40 | 3.66 (0.33) | 35 | 3.59 (0.38) | F(1.861,215.909) = 19.972 p < 0.001 |
| TRT | 38 | 3.83 (0.38) | 38 | 3.74 (0.35) | 35 | 3.57 (0.30) | ||
| Waitlist | 40 | 3.87 (0.39) | 40 | 3.74 (0.33) | 39 | 3.80 (0.38) | ||
| Difference between groups | F(2,116) = 2.762 p = 0.067 | F(2,116) = 0.858 p = 0.427 | F(2,116) = 4.825 p = 0.010 □ ⬟ | |||||
| Parenting confidence | ||||||||
| PSOC | t1 | t2 | t3 | Statistical test results | ||||
| n | Mean (SD) | n | Mean (SD) | n | Mean (SD) | |||
| Total score | TRT + P | 36 | 61.88 (6.56) | 39 | 64.02 (4.73) | 32 | 62.01 (4.50) | F(1.870,216.891) = 3.712 p = 0.029 |
| TRT | 36 | 63.27 (5.36) | 36 | 61.24 (5.61) | 30 | 61.29 (3.00) | ||
| Waitlist | 38 | 63.16 (5.22) | 37 | 60.20 (3.83) | 39 | 59.88 (6.19) | ||
| Difference between groups | F(2,116) = 0.720 p = 0.489 | χ2(2) = 15.166 p = 0.001 † ⬟ | χ2(2) = 13.413 p = 0.001 □ ⬟ | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Khani, A.; Cartwright, K.; Maalouf, W.; Haar, K.; Zehra, N.; Çokamay-Yılmaz, G.; Calam, R. Enhancing Teaching Recovery Techniques (TRT) with Parenting Skills: RCT of TRT + Parenting with Trauma-Affected Syrian Refugees in Lebanon Utilising Remote Training with Implications for Insecure Contexts and COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 8652. https://doi.org/10.3390/ijerph18168652
El-Khani A, Cartwright K, Maalouf W, Haar K, Zehra N, Çokamay-Yılmaz G, Calam R. Enhancing Teaching Recovery Techniques (TRT) with Parenting Skills: RCT of TRT + Parenting with Trauma-Affected Syrian Refugees in Lebanon Utilising Remote Training with Implications for Insecure Contexts and COVID-19. International Journal of Environmental Research and Public Health. 2021; 18(16):8652. https://doi.org/10.3390/ijerph18168652
Chicago/Turabian StyleEl-Khani, Aala, Kim Cartwright, Wadih Maalouf, Karin Haar, Nosheen Zehra, Gökçe Çokamay-Yılmaz, and Rachel Calam. 2021. "Enhancing Teaching Recovery Techniques (TRT) with Parenting Skills: RCT of TRT + Parenting with Trauma-Affected Syrian Refugees in Lebanon Utilising Remote Training with Implications for Insecure Contexts and COVID-19" International Journal of Environmental Research and Public Health 18, no. 16: 8652. https://doi.org/10.3390/ijerph18168652