
Is the Clinical Delivery of Cardiac Rehabilitation in an Australian Setting Associated with Changes in Physical Capacity and Cardiovascular Risk and Are Any Changes Maintained for 12 Months?



Abstract
:1. Introduction
2. Materials and Methods
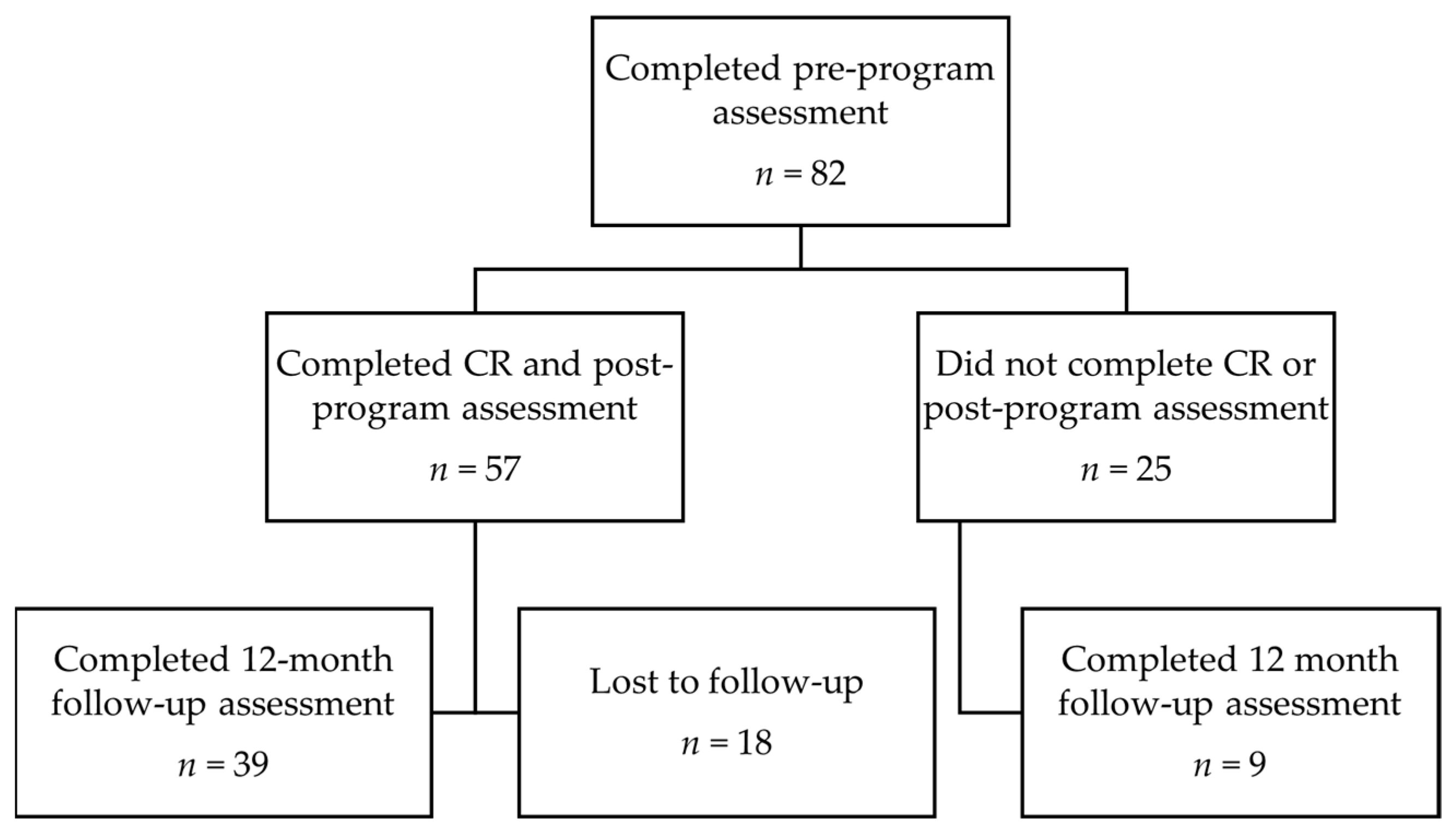
2.1. Participants and Study Design
2.2. Physical Capacity Testing
2.3. Assessment of Cardiovascular Risk Factors
2.4. Exercise Training
2.5. Statistical Analysis
3. Results
3.1. Participant Baseline Demographics
3.2. Short-Term Changes (12 Exercise Sessions)
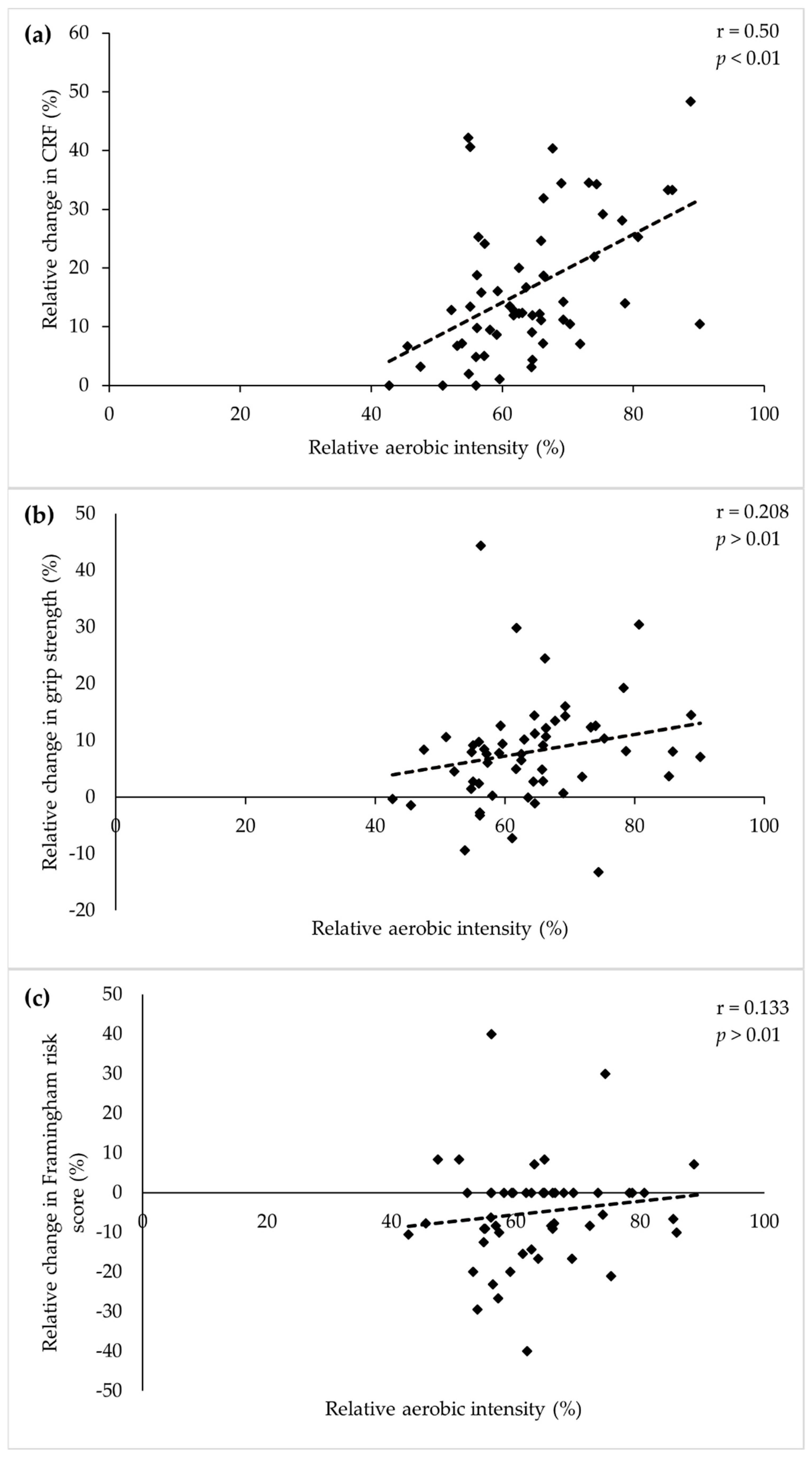
3.3. Influence of Relative Aerobic Exercise Intensity
3.4. Maintenance of Changes (12-Month Follow-Up)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anderson, L.; Oldridge, N.; Thompson, D.R.; Zwisler, A.D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease: Cochrane systematic review and meta-analysis. J. Am. Coll. Cardiol. 2016, 67, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Ades, P.A.; Savage, P.D.; Brawner, C.A.; Lyon, C.E.; Ehrman, J.K.; Bunn, J.Y.; Keteyian, S.J. Aerobic capacity in patients entering cardiac rehabilitation. Circulation 2006, 113, 2706–2712. [Google Scholar] [CrossRef] [Green Version]
- Baum, K.; Hildebrandt, U.; Edel, K.; Bertram, R.; Hahmann, H.; Bremer, F.J.; Bohmen, S.; Kammerlander, C.; Serafin, M.; Ruther, T.; et al. Comparison of skeletal muscle strength between cardiac patients and age-matched healthy controls. Int. J. Med. Sci. 2009, 6, 184–191. [Google Scholar] [CrossRef] [Green Version]
- Kim, A.R.; Nam, T.-W.; Oh, H.-M.; Park, E.; Huh, J.-W.; Yang, W.-J.; Yang, D.H.; Park, H.S.; Lee, Y.-S.; Jung, T.-D. Effect of hospital-based cardiac rehabilitation on quality of life and physical capacity in acute myocardial infarction patients: 2 years follow up. J. Clin. Exp. Cardiol. 2018, 9, 1000573. [Google Scholar] [CrossRef] [Green Version]
- Price, K.J.; Gordon, B.A.; Bird, S.R.; Benson, A.C. A review of guidelines for cardiac rehabilitation exercise programmes: Is there an international consensus? Eur. J. Prev. Cardiol. 2016, 23, 1715–1733. [Google Scholar] [CrossRef] [PubMed]
- National Heart Foundation of Australia; Australian Cardiac Rehabilitation Association. Recommended Framework for Cardiac Rehabilitation. Australia: National Heart Foundation of Australia; National Heart Foundation of Australia: Sydney, Australia; Australian Cardiac Rehabilitation Association: Sydney, Australia, 2004; Available online: http://www.heartfoundation.org.au/SiteCollectionDocuments/Recommended-framework.pdf (accessed on 11 February 2015).
- Abell, B.; Glasziou, P.; Briffa, T.; Hoffmann, T. Exercise training characteristics in cardiac rehabilitation programmes: A cross-sectional survey of Australian practice. Open Heart 2016, 3, e000374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandercock, G.; Hurtado, V.; Cardoso, F. Changes in cardiorespiratory fitness in cardiac rehabilitation patients: A meta-analysis. Int. J. Cardiol. 2013, 167, 894–902. [Google Scholar] [CrossRef] [PubMed]
- Sandercock, G.R.; Cardoso, F.; Almodhy, M.; Pepera, G. Cardiorespiratory fitness changes in patients receiving comprehensive outpatient cardiac rehabilitation in the UK: A multicentre study. Heart 2013, 99, 785–790. [Google Scholar] [CrossRef] [Green Version]
- Nichols, S.; Taylor, C.; Goodman, T.; Page, R.; Kallvikbacka-Bennett, A.; Nation, F.; Clark, A.L.; Birkett, S.T.; Carroll, S.; Ingle, L. Routine exercise-based cardiac rehabilitation does not increase aerobic fitness: A CARE CR study. Int. J. Cardiol. 2020, 305, 25–34. [Google Scholar] [CrossRef] [Green Version]
- Hald, K.; Nielsen, K.M.; Nielsen, C.V.; Meillier, L.K.; Larsen, F.B.; Christensen, B.; Larsen, M.L. Expanded cardiac rehabilitation in socially vulnerable patients with myodardial infarction: A 10-year follow-up study focusing on mortality and non-fatal events. BMJ Open Sport Exerc. Med. 2018, 8, e019307. [Google Scholar] [CrossRef]
- Doimo, S.; Fabris, F.; Piepoli, M.; Barbati, G.; Antonini-Canterin, F.; Bernardi, G.; Maras, P.; Sinagra, G. Impact of ambulatory cardiac rehabilitation on cardiovascular outcomes: A long-term follow-up study. Eur. Heart J. 2019, 40, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Sumner, J.; Harrison, A.; Doherty, P. The effectiveness of modern cardiac rehabilitation: A systematic review of recent observational studies in non-attenders versus attenders. PLoS ONE 2017, 12, e0177658. [Google Scholar] [CrossRef] [PubMed]
- Heran, B.S.; Chen, J.M.; Ebrahim, S.; Moxham, T.; Oldridge, N.; Rees, K.; Thompson, D.R.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2011, 7, CD001800. [Google Scholar] [CrossRef]
- Singh, S.J.; Morgan, M.D.L.; Scott, S.; Walters, D.; Hardman, A. Development of a shuttle walking test of disability in patients with chronic airways obstruction. Thorax 1992, 47, 1019–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowler, S.J.; Singh, S.J.; Revill, S. Reproducibility and validity of the incremental shuttle walking test in patients following coronary artery bypass surgery. Physiotherapy 2005, 91, 22–27. [Google Scholar] [CrossRef]
- American Association of Cardiovascular and Pulmonary Rehabilitation. Guidelines for Cardiac Rehabilitation and Secondary Prevention Programs, 5th ed.; Human Kinetics: Champaign, IL, USA, 2013. [Google Scholar]
- Gore, C.J. Physiological Tests for Elite Athletes; Human Kinetics: Champaign, IL, USA, 2000. [Google Scholar]
- Riebe, D.; Ehrman, J.K.; Liguori, G.; Magal, M. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2018. [Google Scholar]
- National Cholesterol Education Program (NCEP). Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) Expert Panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Bell, K.; Shaw, J.E.; Maple-Brown, L.; Ferris, W.; Gray, S.; Murfet, G.; Flavei, R.; Maynard, B.; Ryrie, H.; Pritchard, B.; et al. A postition statement on screening and management of prediabetes in adults in primary care in Australia. Diabetes Res. Clin. Pract 2020, 164, 108188. [Google Scholar] [CrossRef]
- D’Agostino, R.B.; Russell, M.W.; Huse, D.M.; Ellison, R.C.; Silbershatz, H.; Wilson, P.W.F.; Hartz, S.C. Primary and subsequent coronary risk appraisal: New results from The Framingham Study. Am. Heart J. 2000, 139, 272–281. [Google Scholar] [CrossRef]
- Borg, G.A.V. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988; pp. 79–81. [Google Scholar]
- Arena, R.; Myers, J.; Williams, M.A.; Gulati, M.; Kligfield, P.; Balady, G.J.; Collins, E.; Fletcher, G. Assessment of functional capacity in clinical and research settings: A scientific statement from the American Heart Association Committee on Exercise, Rehabilitation, and Prevention of the Council on Clinical Cardiology and the Council on Cardiovascular Nursing. Circulation 2007, 116, 329–343. [Google Scholar] [CrossRef]
- Kaminsky, L.A.; Arena, R.; Myers, J. Reference standards for cardiorespiratory fitness measured with cardiopulmonary exercise testing: Data from the Fitness Registry and the Importance of Exercise National Database. Mayo Clin. Proc. 2015, 90, 1515–1523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alley, D.E.; Shardell, M.D.; Peters, K.W.; McLean, R.R.; Dam, T.L.; Kenny, A.M.; Fragala, M.S.; Harris, T.B.; Kiel, D.P.; Guralnik, J.M.; et al. Grip strength cutpoint for the identification of clinically relevant weakness. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 559–566. [Google Scholar] [CrossRef]
- Massy-Westropp, N.M.; Gill, T.K.; Taylor, A.W.; Bohannon, R.W.; Hill, C.L. Hand Grip Strength: Age and gender stratified normative data in a population-based study. BMC Res. Notes 2011, 4, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balady, G.J.; Williams, M.A.; Ades, P.A.; Bittner, V.; Comoss, P.; Foody, J.M.; Franklin, B.; Sanderson, B.; Southard, D. Core components of cardiac rehabilitation/secondary prevention programs: 2007 update: A scientific statement from the American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee, the Council on Clinical Cardiology; the Councils on Cardiovascular Nursing, Epidemiology and Prevention, and Nutrition, Physical Activity, and Metabolism; and the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation 2007, 115, 2675–2682. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Corra, U.; Benzer, W.; Bjarnason-Wehrens, B.; Dendale, P.; Gaita, D.; McGee, H.; Mendes, M.; Niebauer, J.; Zwisler, A.D.; et al. Secondary prevention through cardiac rehabilitation: From knowledge to implementation. A position paper from the Cardiac Rehabilitation Section of the European Association of Cardiovascular Prevention and Rehabilitation. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.; Corra, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and other societies on Cardiovascular Disease Prevention in Clinical Practice. Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Eckel, R.H.; Jakicic, J.M.; Ard, J.D.; de Jesus, J.M.; Housten Miller, N.; Hubbard, V.S.; Lee, I.M.; Lichtenstein, A.H.; Loria, C.M.; Millen, B.E.; et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, S76–S99. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boire, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Vermeulen, J.; Neyens, J.C.L.; van Rossum, E.; Spreeuwenberg, M.D.; de Witte, L.P. Predicting ADL disability in community-dwelling elderly people using physical frailty indicators: A systematic review. BMC Geriatr. 2011, 11, 33. [Google Scholar] [CrossRef] [Green Version]
- Mroszczyk-McDonald, A.; Savage, P.D.; Ades, P.A. Handgrip strength in cardiac rehabilitation: Normative values, interaction with physical function, and response to training. J. Cardiopulm. Rehabil. Prev. 2007, 27, 298–302. [Google Scholar] [CrossRef]
- Sumide, T.; Shimada, K.; Ohmura, H.; Onishi, T.; Kawakami, K.; Masaki, Y.; Fukao, K.; Nishitani, M.; Kume, A.; Sato, H.; et al. Relationship between exercise tolerance and muscle strength following cardiac rehabilitation: Comparison of patients after cardiac surgery and patients with myocardial infarction. J. Cardiol. 2009, 54, 273–281. [Google Scholar] [CrossRef] [Green Version]
- Fagard, R.H. Exercise characteristics and the blood pressure response to dynamic physical training. Med. Sci. Sports Exerc. 2001, 33, S484–S492. [Google Scholar] [CrossRef]
- Pescatello, L.S.; Franklin, B.A.; Fagard, R.; Farquhar, W.B.; Kelley, G.A.; Ray, C.A. American College of Sports Medicine position stand. Exercise and hypertension. Med. Sci. Sports Exerc. 2004, 36, 533–553. [Google Scholar] [CrossRef]
- Wasfy, M.M.; Baggish, A.L. Exercise dose in clinical practice. Circulation 2016, 133, 2297–2313. [Google Scholar] [CrossRef] [Green Version]
- O’Donovan, G.; Owen, A.; Bird, S.R.; Kearney, E.M.; Nevill, A.M.; Jones, D.W.; Woolf-May, K. Changes in cardiorespiratory fitness and coronary heart disease risk factors following 24 wk of moderate- or high-intensity exercise of equal energy cost. J. Appl. Physiol. 2005, 98, 1619–1625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, R.; Dagnone, D.; Jones, P.J.H.; Smith, H.; Paddags, A.; Hudson, R.; Janssen, I. Reduction in obesity and related comorbid conditions after diet-induced weight loss or exercise-induced weight loss in men. Ann. Intern. Med. 2000, 133, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.; Janssen, I.; Dawson, J.; Kungl, A.; Kuk, J.L.; Wong, S.L.; Nguyen-Duy, T.; Lee, S.; Kilpatrick, K.; Hudson, R. Exercise-induced reduction in obesity and insulin resistance in women: A randomized controlled trial. Obes. Res. 2004, 12, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. American College of Sports Medicine position stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]
- Porcari, J.P.; Foster, C.; Cress, M.L.; Larson, R.; Lewis, H.; Cortis, C.; Doberstein, S.; Donahue, M.; Fusco, A.; Radtke, K. Prediction of exercise capacity and training prescription from the 6-minute walk test and rating of perceived exertion. J. Funct. Morphol. Kinesiol. 2021, 6, 52. [Google Scholar] [CrossRef] [PubMed]
- Volaklis, K.A.; Douda, H.T.; Kokkinos, P.F.; Tokmakidis, S.P. Physiological alterations to detraining following prolonged strength and aerobic training in cardiac patients. Eur. J. Cardiovasc. Prev. Rehabil. 2006, 13, 375–380. [Google Scholar] [CrossRef]
- Tokmakidis, S.P.; Volaklis, K.A. Training and detraining effects of a combined-strength and aerobic exercise program on blood lipids in patients with coronary artery disease. J. Cardiopulm. Rehabil. 2003, 23, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Han, D.; Lee, S.; Wee, S.; Oh, M.; Jeong, I. Effects of exercise-based cardiac rehabilitation and detraining on exercise capacity and cardiac function in patients with atrial fibrillation: A randomized controlled trial with 1-year follow-up. EP Eur. 2020, 22, euaa162.242. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristic | All Participants (n = 57) |
|---|---|
| Sex—Males/Females (n) | 55/2 |
| Non-surgical a/Surgical treatment b (n) | 35/22 |
| Age (years) | 61.4 ± 10.8 |
| Height (cm) | 172.8 ± 7.9 |
| Body mass (kg) | 83.3 ± 13.2 |
| Time to commencement (days) | 48 ± 35 (range 15–267) |
| Length of program (weeks) | 9.1 ± 4.6 (range 5–14) |
| Outcome | Target Value | Assessment | ||
|---|---|---|---|---|
| Pre-Program (n = 57) | Post-Program (n = 57) | 12-Month Follow-Up (n = 39) | ||
| Physical capacity | ||||
| CRF [25] | 5 METs | 88% | 96% | 95% |
| Age-based norms [26] | At or above population mean values | 4% | 21% | 33% |
| Grip strength [27] | Men: 32 kg Women: 20 kg | 79% | 88% | 90% |
| Age-based norms [28] | At or above population mean values | 45% | 63% | 59% |
| Blood pressure [29,30] | ||||
| Systolic | <140 mmHg | 77% | 82% | 77% |
| Diastolic | <90 mmHg | 86% | 93% | 85% |
| Body composition [31,32] | ||||
| Waist circumference | Men: <94 cm Women: <80 cm | 26% | 42% | 33% |
| BMI | <25 kg m2 | 14% | 18% | 13% |
| Blood profile [31] | ||||
| LDL-cholesterol | <2.6 mmol/L | 82% | 91% | 81% |
| Lower target | <1.8 mmol/L | 53% | 62% | 44% |
| Total cholesterol | <4.5 mmol/L | 89% | 87% | 75% |
| HDL-cholesterol | Men: >1.0 mmol/L Women: >1.2 mmol/L | 55% | 74% | 81% |
| Triglycerides | <1.7 mmol/L | 85% | 91% | 84% |
| Fasting blood glucose | <5.6 mmol/L | 67% | 71% | 77% |
| Outcome | Effect of CR Program (n = 57) | Maintenance Following CR Program (n = 39) | ||
|---|---|---|---|---|
| Pre | Post | Post | Follow-Up | |
| Framingham risk score | 13.7 (12.7–14.7) | 12.9 * (12.0–13.8) | 13.3 (12.2–14.4) | 13.4 (12.1–14) |
| Physical capacity | ||||
| CRF (METs) | 6.5 (6.1–6.8) | 7.4 * (7.1–7.8) | 7.4 (7.0–7.8) | 7.7 (7.2–8.2) |
| Grip strength (kg) | 37.7 (35.6–39.9) | 40.6 * (38.3–42.8) | 40.2 (37.3–43.1) | 40.4 (37.7–43.1) |
| Body composition | ||||
| BMI (kg/m2) | 28.0 (27.1–28.9) | 27.9 (27.0–28.8) | 28.0 (26.9–29.0) | 28.5 (27.4–29.7) |
| Waist circumference (cm) | 98.6 (95.9–101.2) | 97.0 * (94.4–99.6) | 97.6 (94.3–100.8) | 99.1 (95.6–102.7) |
| Blood pressure | ||||
| Diastolic BP (mmHg) | 75.5 (72.4–78.6) | 76.3 (74.0–78.6) | 76.9 (74.1–79.6) | 77.2 (73.5–80.9) |
| Systolic BP (mmHg) | 126.8 (122.6–131.0) | 128.2 (125.0–131.4) | 129.2 (125.2–133.3) | 133.6 (128.7–138.5) |
| Blood profile | ||||
| HDL-cholesterol (mmol/L) | 1.11 (1.04–1.19) | 1.22 * (1.14–1.30) | 1.23 (1.13–1.34) | 1.33 (1.22–1.45) |
| LDL-cholesterol (mmol/L) | 1.8 (1.6–2.0) | 1.6 (1.4–1.8) | 1.6 (1.4–1.8) | 2.0 (1.6–2.4) |
| Total cholesterol (mmol/L) | 3.5 (3.3–3.7) | 3.4 (3.1–3.6) | 3.4 (3.1–3.7) | 3.9 (3.5–4.4) |
| Triglycerides (mmol/L) | 1.3 (1.2–1.4) | 1.1 (0.9–1.3) | 1.2 (0.9–1.5) | 1.3 (0.8–1.7) |
| Blood glucose (mmol/L) | 5.4 (5.1–5.6) | 5.2 (5.1–5.4) | 5.2 (5.1–5.5) | 5.2 (5.0–5.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Price, K.J.; Gordon, B.A.; Bird, S.R.; Benson, A.C. Is the Clinical Delivery of Cardiac Rehabilitation in an Australian Setting Associated with Changes in Physical Capacity and Cardiovascular Risk and Are Any Changes Maintained for 12 Months? Int. J. Environ. Res. Public Health 2021, 18, 8950. https://doi.org/10.3390/ijerph18178950
Price KJ, Gordon BA, Bird SR, Benson AC. Is the Clinical Delivery of Cardiac Rehabilitation in an Australian Setting Associated with Changes in Physical Capacity and Cardiovascular Risk and Are Any Changes Maintained for 12 Months? International Journal of Environmental Research and Public Health. 2021; 18(17):8950. https://doi.org/10.3390/ijerph18178950
Chicago/Turabian StylePrice, Kym Joanne, Brett Ashley Gordon, Stephen Richard Bird, and Amanda Clare Benson. 2021. "Is the Clinical Delivery of Cardiac Rehabilitation in an Australian Setting Associated with Changes in Physical Capacity and Cardiovascular Risk and Are Any Changes Maintained for 12 Months?" International Journal of Environmental Research and Public Health 18, no. 17: 8950. https://doi.org/10.3390/ijerph18178950
APA StylePrice, K. J., Gordon, B. A., Bird, S. R., & Benson, A. C. (2021). Is the Clinical Delivery of Cardiac Rehabilitation in an Australian Setting Associated with Changes in Physical Capacity and Cardiovascular Risk and Are Any Changes Maintained for 12 Months? International Journal of Environmental Research and Public Health, 18(17), 8950. https://doi.org/10.3390/ijerph18178950