
Systolic Blood Pressure and Outcomes in Stable Outpatients with Recent Symptomatic Artery Disease: A Population-Based Longitudinal Study

 , , and
, , and
Abstract
:1. Introduction
2. Methods
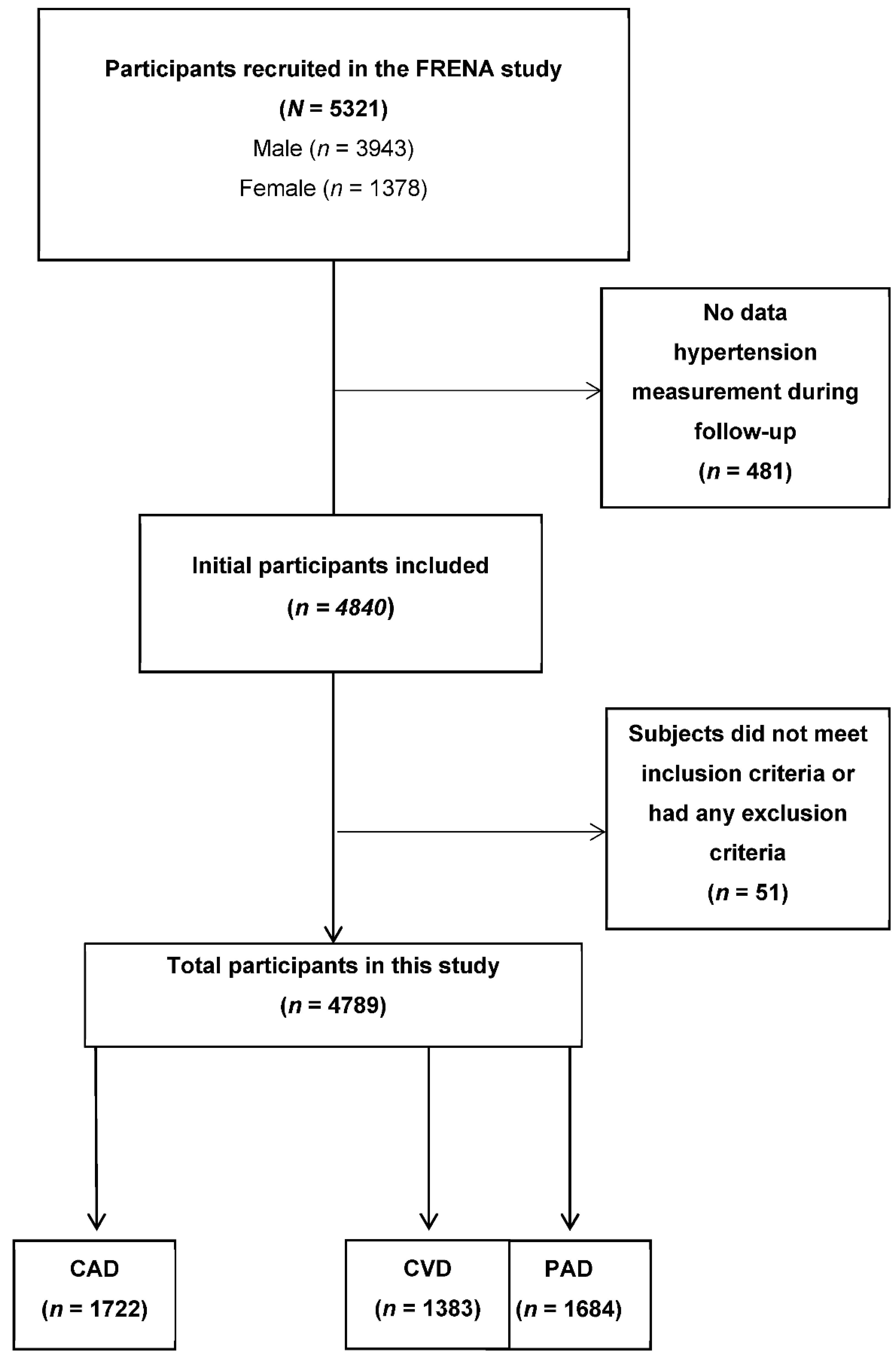
2.1. Inclusion Criteria
2.2. Study Design
2.3. Follow-up
2.4. Data Collection
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A
References
- Ettehad, D.; Emdin, C.A.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Blood pressure lowering for prevention of cardiovascular disease and death: A systematic review and meta-analysis. Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef] [Green Version]
- Thomopoulos, C.; Parati, G.; Zanchetti, A. Effects of blood pressure lowering on outcome incidence in hypertension. 1. Overview, meta-analyses, and meta-regression analyses of randomized trials. J. Hypertens. 2014, 32, 2285–2295. [Google Scholar] [CrossRef] [Green Version]
- Brugts, J.J.; Boersma, E.; Chonchol, M.; Deckers, J.W.; Bertrand, M.; Remme, W.J.; Ferrari, R.; Fox, K.; Simoons, M.L. The cardioprotective effects of the angiotensin-converting enzyme inhibitor perindopril in patients with stable coronary artery disease are not modified by mild to moderate renal insufficiency: Insights from the EUROPA trial. J. Am. Coll. Cardiol. 2007, 50, 2148–2155. [Google Scholar] [CrossRef] [Green Version]
- Nissen, S.E.; Tuzcu, E.M.; Libby, P.; Thompson, P.D.; Ghali, M.; Garza, D.; Berman, L.; Shi, H.; Buebendorf, E.; Topol, E.J. Effect of antihypertensive agents on cardiovascular events in patients with coronary disease and normal blood pressure: The CAMELOT study: A randomized controlled trial. JAMA 2004, 292, 2217–2225. [Google Scholar] [CrossRef] [Green Version]
- Braunwald, E.; Domanski, M.J.; Fowler, S.E.; Geller, N.L.; Gersh, B.J.; Hsia, J.; Pfeffer, M.A.; Rice, M.M.; Rosenberg, Y.D.; Rouleau, J.L. Angiotensin-converting-enzyme inhibition in stable coronary artery disease. N. Engl. J. Med. 2004, 351, 2058–2068. [Google Scholar] [PubMed]
- Boan, A.D.; Lackland, D.T.; Ovbiagele, B. Lowering of blood pressure for recurrent stroke prevention. Stroke 2014, 45, 2506–2513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, K.M. Efficacy of perindopril in reduction of cardiovascular events among patients with stable coronary artery disease: Randomised, double-blind, placebo-controlled, multicentre trial (the EUROPA study). Lancet 2003, 362, 782–788. [Google Scholar]
- Lonn, E.M.; Bosch, J.; Lopez-Jaramillo, P.; Zhu, J.; Liu, L.; Pais, P.; Diaz, R.; Xavier, D.; Sliwa, K.; Dans, A.; et al. Blood-Pressure Lowering in Intermediate-Risk Persons without Cardiovascular Disease. N. Engl. J. Med. 2016, 374, 2009–2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benavente, O.R.; Coffey, C.S.; Conwit, R.; Hart, R.G.; McClure, L.A.; Pearce, L.A.; Pergola, P.E.; Szychowski, J.M. Blood-pressure targets in patients with recent lacunar stroke: The SPS3 randomised trial. Lancet 2013, 382, 507–515. [Google Scholar] [PubMed] [Green Version]
- Mant, J.; McManus, R.J.; Roalfe, A.; Fletcher, K.; Taylor, C.J.; Martin, U.; Virdee, S.; Greenfield, S.; Hobbs, F.D.R. Different systolic blood pressure targets for people with history of stroke or transient ischaemic attack: PAST-BP (Prevention After Stroke—Blood Pressure) randomised controlled trial. BMJ 2016, 352, i708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arima, H.; Chalmers, J.; Woodward, M.; Anderson, C.; Rodgers, A.; Davis, S.; Macmahon, S.; Neal, B. Lower target blood pressures are safe and effective for the prevention of recurrent stroke: The PROGRESS trial. J. Hypertens. 2006, 24, 1201–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostergren, J.; Sleight, P.; Dagenais, G.; Danisa, K.; Bosch, J.; Qilong, Y.; Yusuf, S. Impact of ramipril in patients with evidence of clinical or subclinical peripheral arterial disease. Eur. Heart J. 2004, 25, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Thomas Manapurathe, D.; Moxon, J.V.; Krishna, S.M.; Rowbotham, S.; Quigley, F.; Jenkins, J.; Bourke, M.; Bourke, B.; Jones, R.E.; Golledge, J. Cohort Study Examining the Association Between Blood Pressure and Cardiovascular Events in Patients with Peripheral Artery Disease. J. Am. Heart Assoc. 2019, 8, e010748. [Google Scholar] [CrossRef] [Green Version]
- Bernaudo, D.; Coll, R.; Sanchez Munoz-Torrero, J.F.; Pascual, M.T.; Garcia-Diaz, A.M.; Alvarez, L.R.; Monreal, M. Renal function and short-term outcome in stable outpatients with coronary, cerebrovascular or peripheral artery disease. Atherosclerosis 2013, 229, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Barba, R.; Bisbe, J.; Pedrajas, J.N.A.; Toril, J.; Monte, R.; Munoz-Torrero, J.F.S.; Monreal, M. Body mass index and outcome in patients with coronary, cerebrovascular, or peripheral artery disease: Findings from the FRENA registry. Eur. J. Cardiovasc. Prev. Rehabil. 2009, 16, 457–463. [Google Scholar] [CrossRef]
- Garcia-Diaz, A.M.; Marchena, P.J.; Toril, J.; Arnedo, G.; Munoz-Torrero, J.F.S.; Yeste, M.; Aguilar, E.; Monreal, M. Alcohol consumption and outcome in stable outpatients with peripheral artery disease. J. Vasc. Surg. 2011, 54, 1081–1087. [Google Scholar] [CrossRef] [Green Version]
- Alvarez, L.R.; Balibrea, J.M.; Surinach, J.M.; Coll, R.; Pascual, M.T.; Toril, J.; Lopez-Jimenez, L.; Monreal, M. Smoking cessation and outcome in stable outpatients with coronary, cerebrovascular, or peripheral artery disease. Eur. J. Prev. Cardiol. 2013, 20, 486–495. [Google Scholar] [CrossRef]
- Sanchez Munoz-Torrero, J.F.; Rico-Martin, S.; Alvarez, L.R.; Aguilar, E.; Alcala, J.N.; Monreal, M. Lipoprotein (a) levels and outcomes in stable outpatients with symptomatic artery disease. Atherosclerosis 2018, 276, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Munoz-Torrero, J.F.S.; Zamorano, J.; Rico-Martin, S.; Rivas, M.D.; Bacaicoa, M.A.; Robles, R.; Sanchez-Bacaicoa, C.; Monreal, M. Proton pump inhibitors and risk for recurrent ischemic events or death in outpatients with symptomatic artery disease. Atherosclerosis 2020, 292, 84–89. [Google Scholar] [CrossRef] [Green Version]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redon, J.; Zanchetti, A.; Bohm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J. Hypertens. 2013, 31, 1281–1357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, X.; Atkins, E.; Lv, J.; Bennett, A.; Neal, B.; Ninomiya, T.; Woodward, M.; MacMahon, S.; Turnbull, F.; Hillis, G.S.; et al. Effects of intensive blood pressure lowering on cardiovascular and renal outcomes: Updated systematic review and meta-analysis. Lancet 2016, 387, 435–443. [Google Scholar] [CrossRef] [Green Version]
- Saiz, L.C.; Gorricho, J.; Garjon, J.; Celaya, M. feminine C.; Erviti, J.; Leache, L. Blood pressure targets for the treatment of people with hypertension and cardiovascular disease. Cochrane Database Syst. Rev. 2018, 7, CD010315. [Google Scholar] [PubMed]
- Vidal-Petiot, E.; Ford, I.; Greenlaw, N.; Ferrari, R.; Fox, K.M.; Tardif, J.-C.; Tendera, M.; Tavazzi, L.; Bhatt, D.L.; Steg, P.G. Cardiovascular event rates and mortality according to achieved systolic and diastolic blood pressure in patients with stable coronary artery disease: An international cohort study. Lancet 2016, 388, 2142–2152. [Google Scholar] [CrossRef] [Green Version]
- Messerli, F.H.; Mancia, G.; Conti, C.R.; Hewkin, A.C.; Kupfer, S.; Champion, A.; Kolloch, R.; Benetos, A.; Pepine, C.J. Dogma disputed: Can aggressively lowering blood pressure in hypertensive patients with coronary artery disease be dangerous? Ann. Intern. Med. 2006, 144, 884–893. [Google Scholar] [CrossRef]
- Cushman, W.C.; Evans, G.W.; Byington, R.P.; Goff, D.C.J.; Grimm, R.H.J.; Cutler, J.A.; Simons-Morton, D.G.; Basile, J.N.; Corson, M.A.; Probstfield, J.L.; et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N. Engl. J. Med. 2010, 362, 1575–1585. [Google Scholar] [PubMed] [Green Version]
- Wright, J.T.J.; Williamson, J.D.; Whelton, P.K.; Snyder, J.K.; Sink, K.M.; Rocco, M.V.; Reboussin, D.M.; Rahman, M.; Oparil, S.; Lewis, C.E.; et al. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N. Engl. J. Med. 2015, 373, 2103–2116. [Google Scholar] [PubMed]
- Bavry, A.A.; Anderson, R.D.; Gong, Y.; Denardo, S.J.; Cooper-Dehoff, R.M.; Handberg, E.M.; Pepine, C.J. Outcomes Among hypertensive patients with concomitant peripheral and coronary artery disease: Findings from the INternational VErapamil-SR/Trandolapril STudy. Hypertension 2010, 55, 48–53. [Google Scholar] [CrossRef] [Green Version]
- Hausenloy, D.J.; Candilio, L.; Evans, R.; Ariti, C.; Jenkins, D.P.; Kolvekar, S.; Knight, R.; Kunst, G.; Laing, C.; Nicholas, J.; et al. Remote Ischemic Preconditioning and Outcomes of Cardiac Surgery. N. Engl. J. Med. 2015, 373, 1408–1417. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Harmsen, P.; Lappas, G.; Rosengren, A.; Wilhelmsen, L. Long-term risk factors for stroke: Twenty-eight years of follow-up of 7457 middle-aged men in Goteborg, Sweden. Stroke 2006, 37, 1663–1667. [Google Scholar] [CrossRef] [Green Version]
- Joosten, M.M.; Pai, J.K.; Bertoia, M.L.; Rimm, E.B.; Spiegelman, D.; Mittleman, M.A.; Mukamal, K.J. Associations between conventional cardiovascular risk factors and risk of peripheral artery disease in men. JAMA 2012, 308, 1660–1667. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinical Characteristics | <130 mm Hg | 130–140 mm Hg | >140 mm Hg |
|---|---|---|---|
| Patients, n | 1664 | 1302 | 1823 |
| Clinical characteristics | |||
| Mean age (years) | 63 ± 13 | 67 ± 11 ‡ | 69 ± 10 ‡ |
| Gender (male) | 1306 (78%) | 965 (74%) † | 1291 (71%) ‡ |
| Body mass index (Kg/m2) | 27 ± 4.4 | 28 ± 4.2 ‡ | 29 ± 4.5 ‡ |
| Underlying diseases | |||
| Cancer | 79 (4.7%) | 71 (5.5%) | 122 (6.7%) * |
| Diabetes | 552 (33%) | 523 (40%) ‡ | 799 (44%) ‡ |
| Current smokers | 318 (19%) | 326 (25%) ‡ | 394 (22%) |
| Chronic lung disease | 254 (15%) | 181 (14%) | 251 (14%) |
| Chronic heart disease | 164 (9.9%) | 88 (6.8%) † | 134 (7.4%) † |
| Clinical presentation | |||
| Coronary artery disease | 900 (54%) | 442 (34%) ‡ | 380 (21%) ‡ |
| Cerebrovascular disease | 364 (22%) | 439 (34%) ‡ | 580 (32%) ‡ |
| Peripheral artery disease | 400 (24%) | 421 (32%) ‡ | 863 (47%) ‡ |
| Physical examination | |||
| Sinus rhythm | 1474 (89%) | 1203 (92%) ‡ | 1667 (91%) † |
| Mean SBP levels (mm Hg) | 119 ± 8.0 | 135 ± 3.1 ‡ | 153 ± 10.4 ‡ |
| Number of SBP measurements | 8487 | 6229 | 8792 |
| Mean (SD) of SBP measurements | 5.1 ± 3.3 | 4.8 ± 2.5 † | 4.8 ± 2.5 † |
| Median (IQR) of SBP measurements | 4 (3–5) | 4 (3–5) | 4 (3–6) |
| Laboratory levels | |||
| Creatinine Clearance (mL/min) | 80 ± 33 | 77 ± 29 † | 72 ± 29 ‡ |
| Total cholesterol (mg/100 mL) | 170 ± 35 | 177 ± 35 ‡ | 180 ± 37 ‡ |
| LDL-cholesterol (mg/100 mL) | 100 ± 30 | 104 ± 31 ‡ | 105 ± 32 ‡ |
| Drugs | |||
| Diuretics | 513 (31%) | 464 (36%) † | 931 (51%) ‡ |
| Beta-blockers | 907 (55%) | 497 (38%) ‡ | 556 (30%) ‡ |
| ACE-inhibitors | 762 (46%) | 536 (41%) * | 872 (48%) |
| Angiotensin-II antagonists | 299 (18%) | 405 (31%) ‡ | 734 (40%) ‡ |
| Calcium antagonists | 321 (19%) | 337 (26%) ‡ | 637 (35%) ‡ |
| Antiplatelets | 1478 (89%) | 1185 (91%) | 1630 (89%) |
| Anticoagulants | 281 (17%) | 176 (14%) * | 262 (14%) * |
| Statins | 1394 (84%) | 1064 (82%) | 1458 (80%) † |
| Insulin | 216 (13%) | 169 (13%) | 327 (18%) ‡ |
| Oral antidiabetics | 382 (23%) | 415 (32%) ‡ | 611 (34%) ‡ |
| Subsequent Events | <130 mm Hg | 130–140 mm Hg | >140 mm Hg | |||||
|---|---|---|---|---|---|---|---|---|
| n | 100 Patient-Years (95% CI) | n | 100 Patient-Years (95% CI) | Rate Ratio (95% CI) | n | 100 Patient-Years (95% CI) | Rate Ratio (95% CI) | |
| CAD patients, n | 900 | 442 | 380 | |||||
| Follow-up (years) | 1.406 | 0.574 | 0.486 | |||||
| Myocardial infarction | 32 | 2.27 (1.55–3.21) | 18 | 3.13 (1.85–4.95) | 1.37 (75–2.44) | 27 | 5.55 (3.66–8.08) | 2.44 (1.45–4.08) ‡ |
| Ischemic stroke | 2 | 0.14 (0.04–0.62) | 6 | 1.05 (0.38–2.27) | 7.34 (1.55–52.9) * | 9 | 1.86 (0.85–3.51) | 13.02 (3.10–88.41) ‡ |
| Limb amputation | 3 | 0.21 (0.05–0.58) | 0 | - | - | 2 | 0.41 (0.46–1.48) | 1.92 (0.22–1.29) |
| Death | 28 | 1.99 (1.32–2.87) | 23 | 4.01 (2.53–6.01) | 2.01 (1.14–3.50) * | 29 | 5.96 (3.99–8.57) | 2.99 (1.77–5.06) ‡ |
| CVD patients, n | 364 | 439 | 580 | |||||
| Follow-up (years) | 0.571 | 0.580 | 0.689 | |||||
| Myocardial infarction | 4 | 0.71 (0.23–1.71) | 3 | 0.52 (0.13–1.42) | 0.73 (0.13–3.57) | 3 | 0.44 (0.11–1.19) | 0.62 (0.11–3.01) |
| Ischemic stroke | 17 | 3.04 (1.83–4.76) | 10 | 1.75 (0.89–3.12) | 0.57 (0.25–1.26) | 35 | 5.20 (3.68–7.16) | 1.70 (0.96–3.11) |
| Limb amputation | 2 | 0.35 (0.06–1.16) | 0 | - | - | 2 | 0.29 (0.05–0.96) | 0.82 (0.08–7.96) |
| Death | 27 | 4.73 (3.18–6.79) | 13 | 2.24 (1.25–3.73) | 0.47 (0.23–0.91) * | 28 | 4.07 (2.75–5.80) | 0.85 (0.50–1.46) |
| PAD patients, n | 400 | 421 | 863 | |||||
| Follow-up (years) | 0.578 | 0.637 | 1.352 | |||||
| Myocardial infarction | 17 | 2.98 (1.80–4.68) | 10 | 1.58 (0.80–2.81) | 0.53 (0.23–1.16) | 22 | 1.65 (1.06–2.45) | 0.55 (0.29–1.05) |
| Ischemic stroke | 13 | 2.28 (1.27–3.79) | 11 | 1.74 (0.92–3.03) | 0.76 (0.33–1.73) | 22 | 1.65 (1.06–2.45) | 0.72 (0.36–1.47) |
| Limb amputation | 23 | 3.97 (2.52–5.97) | 16 | 2.56 (1.52–4.07) | 0.63 (0.32–1.19) | 26 | 1.92 (1.25–2.81) | 0.48 (0.27–0.85) * |
| Death | 47 | 8.13 (5.97–10.81) | 25 | 3.92 (2.53–5.79) | 0.48 (0.29–0.78) † | 40 | 2.95 (2.11–4.02) | 0.36 (0.23–0.55) ‡ |
| Predictors | CAD Patients | CVD Patients | PAD Patients |
|---|---|---|---|
| Age > 65 years | 2.16 (1.17–4.01) * | - | - |
| Chronic heart disease | - | 2.44 (1.13–5.28) * | - |
| SBP < 130 mm Hg | Ref. | Ref. | Ref. * |
| SBP 130–140 mm Hg | 1.06 (0.62–1.80) | 0.52 (0.25–1.10) | 0.71 (0.46–1.09) |
| SBP >140 mm Hg | 1.39 (0.86–2.26) | 1.46 (0.84–2.54) | 0.57 (0.39–0.83) † |
| CrCl levels < 60 mL/min | 2.19 (1.32–3.62) † | - | - |
| Diuretics | 1.83 (1.14–2.93) * | - | - |
| Beta-blockers | - | - | 1.46 (1.03–2.09) * |
| Insulin | 2.38 (1.53–3.70) ‡ | - | 2.83 (2.02–3.98) ‡ |
| Antiplatelets | - | 5.19 (1.94–13.9) † | - |
| Anticoagulants | - | 2.57 (1.45–4.56) † | - |
| Predictors | CAD Patients | CVD Patients | PAD Patients |
|---|---|---|---|
| Age > 65 years | 3.42 (1.49–7.87) † | 3.66 (1.53–8.76) † | 1.74 (1.05–2.87) * |
| Cancer | 2.33 (1.19–4.59) * | - | - |
| Chronic lung disease | 1.85 (1.10–3.11) * | - | - |
| Chronic heart disease | 1.86 (1.11–3.10) * | - | - |
| Sinus rhythm | - | 0.27 (0.17–0.45) ‡ | |
| SBP < 130 mm Hg | Ref. | Ref. † | Ref. ‡ |
| SBP 130–140 mm Hg | 1.28 (0.74–2.25) | 0.39 (0.20–0.77) † | 0.47 (0.29–0.78) † |
| SBP >140 mm Hg | 1.46 (0.85–2.51) | 0.46 (0.26–0.84) * | 0.32 (0.21–0.50) ‡ |
| CrCl levels < 60 mL/min | 1.88 (1.07–3.28) * | 1.90 (1.15–3.15) * | 2.09 (1.35–3.26) † |
| Beta-blockers | - | - | 0.58 (0.35–0.98) * |
| Diuretics | 1.98 (1.13–3.48) * | - | - |
| Statins | 0.45 (0.27–0.75) † | 0.36 (0.22–0.59) ‡ | 0.39 (0.26–0.58) ‡ |
| Insulin | - | 1.85 (1.01–3.37) * | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez Muñoz-Torrero, J.F.; Escudero-Sánchez, G.; Calderón-García, J.F.; Rico-Martín, S.; Robles, N.R.; Bacaicoa, M.A.; Alcalá-Pedrajas, J.N.; Gil-Fernández, G.; Monreal, M.; on behalf of the FRENA Investigators. Systolic Blood Pressure and Outcomes in Stable Outpatients with Recent Symptomatic Artery Disease: A Population-Based Longitudinal Study. Int. J. Environ. Res. Public Health 2021, 18, 9348. https://doi.org/10.3390/ijerph18179348
Sánchez Muñoz-Torrero JF, Escudero-Sánchez G, Calderón-García JF, Rico-Martín S, Robles NR, Bacaicoa MA, Alcalá-Pedrajas JN, Gil-Fernández G, Monreal M, on behalf of the FRENA Investigators. Systolic Blood Pressure and Outcomes in Stable Outpatients with Recent Symptomatic Artery Disease: A Population-Based Longitudinal Study. International Journal of Environmental Research and Public Health. 2021; 18(17):9348. https://doi.org/10.3390/ijerph18179348
Chicago/Turabian StyleSánchez Muñoz-Torrero, Juan F., Guillermo Escudero-Sánchez, Julián F. Calderón-García, Sergio Rico-Martín, Nicolás Roberto Robles, M. Asunción Bacaicoa, José N. Alcalá-Pedrajas, Guadalupe Gil-Fernández, Manuel Monreal, and on behalf of the FRENA Investigators. 2021. "Systolic Blood Pressure and Outcomes in Stable Outpatients with Recent Symptomatic Artery Disease: A Population-Based Longitudinal Study" International Journal of Environmental Research and Public Health 18, no. 17: 9348. https://doi.org/10.3390/ijerph18179348