
Using Total Worker Health® Implementation Guidelines to Design an Organizational Intervention for Low-Wage Food Service Workers: The Workplace Organizational Health Study

 , , and
, , and
Abstract
:1. Introduction
1.1. The Implementation Guidelines
1.2. Low-Wage Food Service Workers and the Workplace Organizational Health Study
2. Materials and Methods
2.1. Study Setting and Population
2.2. Design Team
2.3. Using the Implementation Guidelines to Develop the Intervention
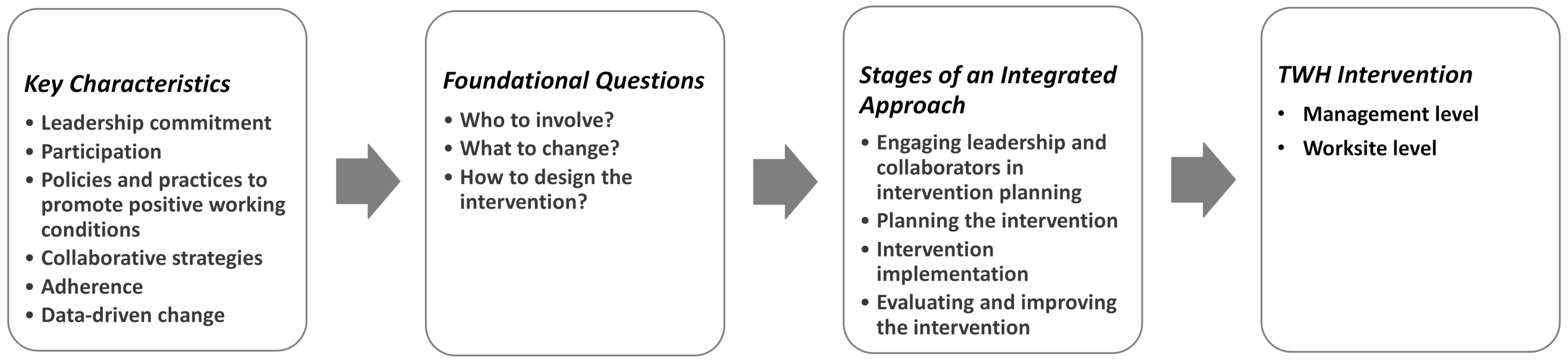
2.3.1. Key Characteristics
2.3.2. Stages
3. Results
3.1. Applying the Key Characteristics
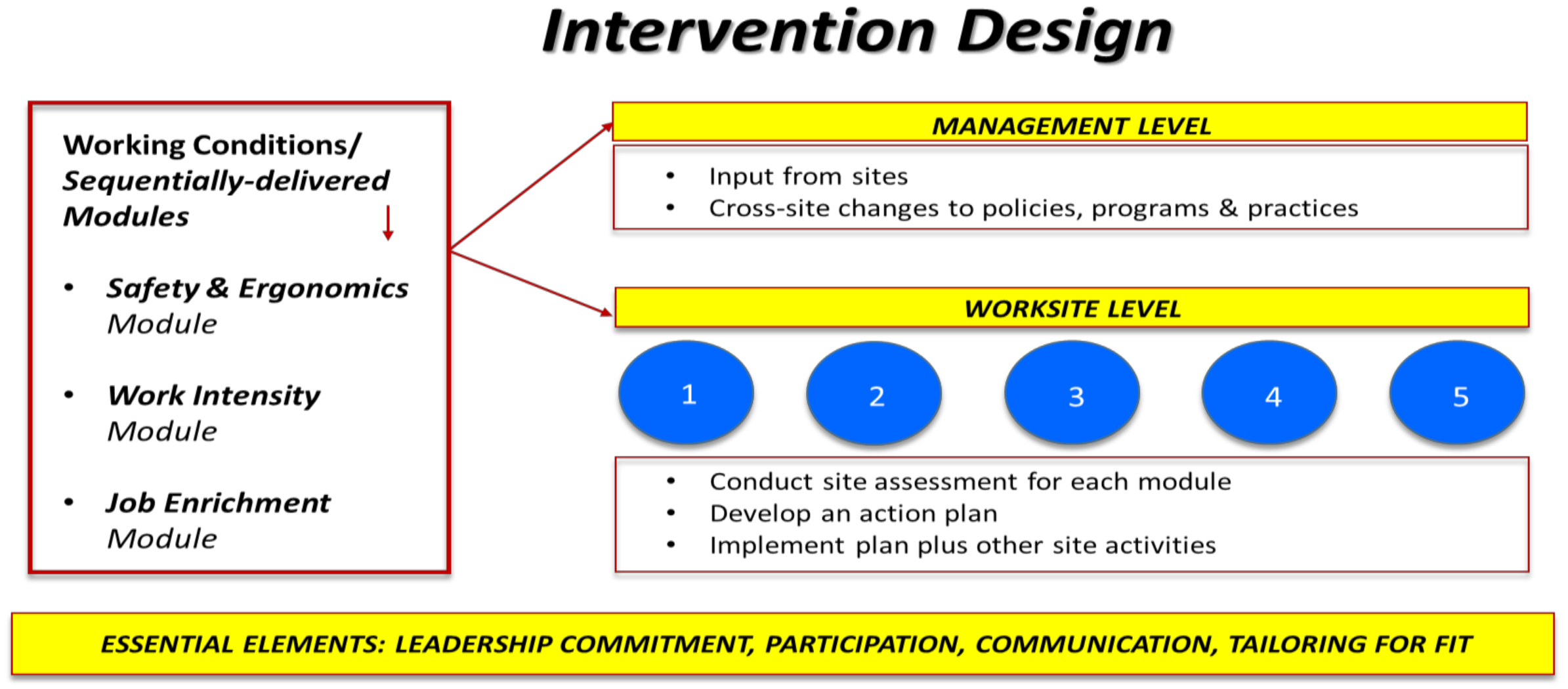
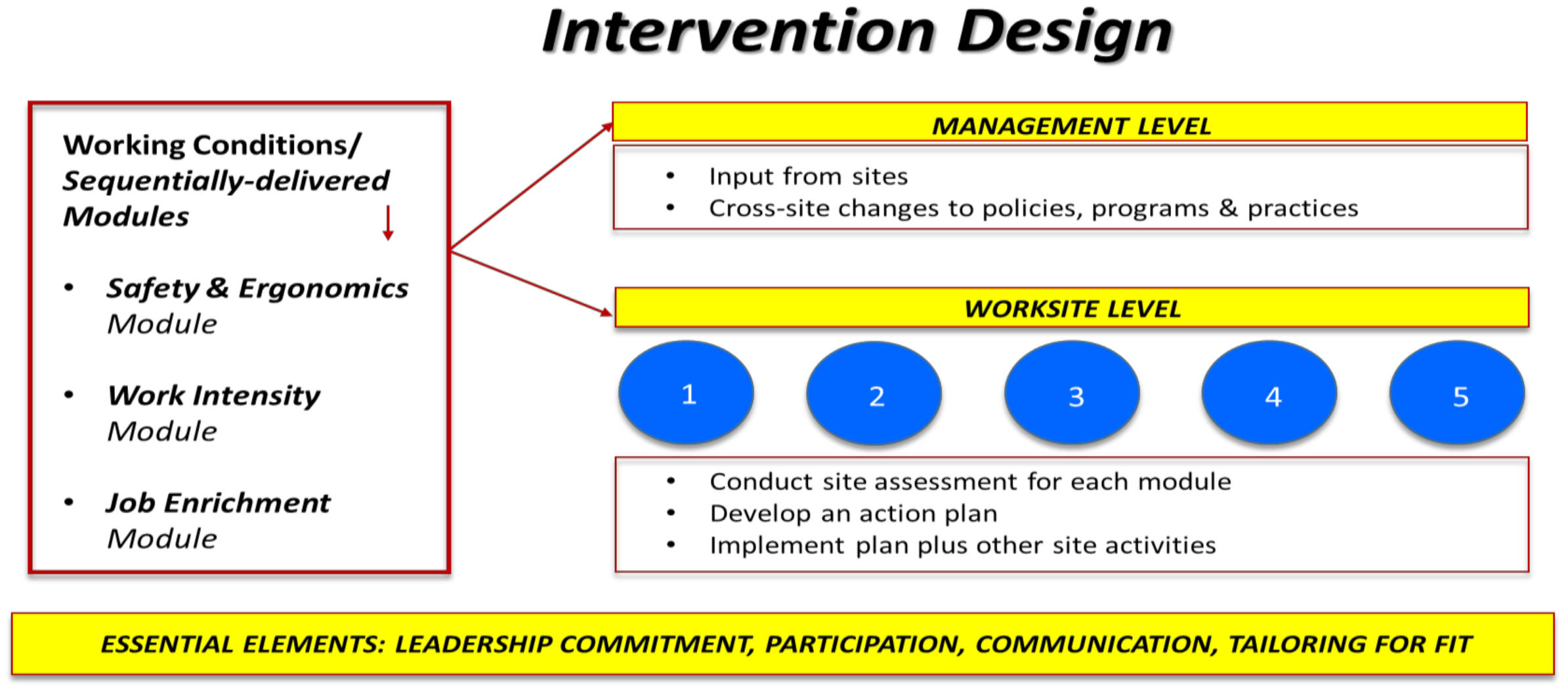
3.2. Applying the Stages
3.2.1. Stage 1: Engaging Leadership and Collaborators in Intervention Planning
- What the Implementation Guidelines Recommend.
- b.
- How we applied the Implementation Guidelines to engaging leadership and promoting collaboration.
- c.
- Considerations for intervention developers.
3.2.2. Stage 2: Planning the Intervention
- What the Implementation Guidelines recommend.
- b.
- How we applied the Implementation Guidelines to intervention planning.
- c.
- Considerations for intervention developers.
3.2.3. Stage 3: Planning for Implementation of the Intervention
- What the Implementation Guidelines recommend.
- b.
- How we applied the Implementation Guidelines to planning intervention implementation.
- c.
- Considerations for intervention developers.
3.2.4. Stage 4: Planning for Evaluating and Improving the Intervention
- What the Implementation Guidelines recommend.
- b.
- How we applied the Implementation Guidelines to plan for intervention improvement.
- c.
- Considerations for intervention developers.
4. Discussion
4.1. Strengths and Limitations
4.2. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sorensen, G.; McLellan, D.L.; Sabbath, E.L.; Dennerlein, J.T.; Nagler, E.M.; Hurtado, D.A.; Pronk, N.P.; Wagner, G.R. Integrating worksite health protection and health promotion: A conceptual model for intervention and research. Prev. Med. 2016, 91, 188–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute of Occupational Safety and Health. Total Worker Health. Available online: https://www.cdc.gov/niosh/twh/totalhealth.html (accessed on 16 May 2021).
- Chari, R.; Chang, C.C.; Sauter, S.L.; Petrun Sayers, E.L.; Cerully, J.L.; Schulte, P.; Schill, A.L.; Uscher-Pines, L. Expanding the Paradigm of Occupational Safety and Health: A New Framework for Worker Well-Being. J. Occup. Environ. Med. 2018, 60, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, G.; Dennerlein, J.T.; Peters, S.E.; Sabbath, E.L.; Kelly, E.L.; Wagner, G.R. The future of research on work, safety, health and wellbeing: A guiding conceptual framework. Soc. Sci. Med. (1982) 2021, 269, 113593. [Google Scholar] [CrossRef]
- EU-OSHA (European Agency for Safety and Health at Work). Third European survey of enterprises on new and emerging risks (ESENER-3). First findings. Publ. Off. Eur. Union 2019. [Google Scholar] [CrossRef]
- Nytrø, K.; Saksvik, P.Ø.; Mikkelsen, A.; Bohle, P.; Quinlan, M. An appraisal of key factors in the implementation of occupational stress interventions. Work Stress 2000, 14, 213–225. [Google Scholar] [CrossRef]
- Schuller, K. Interventions as the centrepiece of psychosocial risk assessment–why so difficult? Int. J. Workplace Health Manag. 2020, 13, 61–80. [Google Scholar] [CrossRef] [Green Version]
- Langenhan, M.K.; Leka, S.; Jain, A. Psychosocial risks: Is risk management strategic enough in business and policy making? Saf. Health Work 2013, 4, 87–94. [Google Scholar] [CrossRef] [Green Version]
- McLellan, D.; Moore, W.; Nagler, E.; Sorensen, G. Implementing an Integrated Approach Weaving Worker Health, Safety, and Well-being into the Fabric of Your Organization; Harvard, T.H., Ed.; Chan School of Public Health Center for Work, Health and Wellbeing: Boston, MA, USA, 2017. [Google Scholar]
- U.S. Department of Labor; Bureau of Labor Statistics. Incidence Rates of Nonfatal Occupational Injuries and Illnesses by Industry and Case Types. Available online: https://www.bls.gov/iif/oshwc/osh/os/summ1_00_2019.htm (accessed on 8 August 2021).
- Croot, L.; O’Cathain, A.; Sworn, K.; Yardley, L.; Turner, K.; Duncan, E.; Hoddinott, P. Developing interventions to improve health: A systematic mapping review of international practice between 2015 and 2016. Pilot Feasibility Stud. 2019, 5, 127. [Google Scholar] [CrossRef]
- Hoddinott, P. A new era for intervention development studies. Pilot Feasibility Stud. 2015, 1, 36. [Google Scholar] [CrossRef] [Green Version]
- McElroy, K.; Bibeau, D.; Steckler, A.; Glanz, K. An ecological perspective on health promotion programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef]
- Stokols, D. Translating social ecological theory into guidelines for community health promotion. Am. J. Health Promot. 1996, 10, 282–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorensen, G.; Emmons, K.; Hunt, M.K.; Barbeau, E.; Goldman, R.; Peterson, K.; Kuntz, K.; Stoddard, A.; Berkman, L. Model for incorporating social context in health behavior interventions: Applications for cancer prevention for working-class, multiethnic populations. Prev. Med. 2003, 37, 188–197. [Google Scholar] [CrossRef]
- Sorensen, G.; Barbeau, E.; Hunt, M.K.; Emmons, K. Reducing social disparities in tobacco use: A social contextual model for reducing tobacco use among blue-collar workers. Am. J. Public Health 2004, 94, 230–239. [Google Scholar] [CrossRef]
- Levy, B.S.; Wegman, D.H.; Baron, S.L.; Sokas, R.K. Occupational and Environmental Health: Recognizing and Preventing Disease and Injury, 5th ed.; Levy, B.S., Wegman, D.H., Baron, S.L., Sokas, R.K., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006. [Google Scholar]
- Office of Technology Assessment. Preventing Illness and Injury in the Workplace; Office of Technology Assessment, Congressional Board of the 99th Congress; US Government Printing Office: Washington, DC, USA, 1985.
- Roelofs, C.; Barbeau, E.; Moure-Eraso, R.; Ellenbecker, M.J. Prevention strategies in industrial hygiene: A critical literature review. Am. Ind. Hyg. Assoc. J. 2003, 64, 62–67. [Google Scholar] [CrossRef]
- Abildgaard, J.S.; Hasson, H.; von Thiele Schwarz, U.; Løvseth, L.T.; Ala-Laurinaho, A.; Nielsen, K. Forms of participation: The development and application of a conceptual model of participation in work environment interventions. Econ. Ind. Democr. 2018, 41, 746–769. [Google Scholar] [CrossRef] [Green Version]
- Sorensen, G.; Peters, S.; Nielsen, K.; Nagler, E.; Karapanos, M.; Wallace, L.; Burke, L.; Dennerlein, J.T.; Wagner, G.R. Improving Working Conditions to Promote Worker Safety, Health, and Wellbeing for Low-Wage Workers: The Workplace Organizational Health Study. Int. J. Environ. Res. Public Health 2019, 16, 1449. [Google Scholar] [CrossRef] [Green Version]
- Montano, D.; Hoven, H.; Siegrist, J. Effects of organisational-level interventions at work on employees’ health: A systematic review. BMC Public Health 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, S.A.; Madera, J.M. Sexual harassment is pervasive in the restaurant industry. Here’s what needs to change. Harv. Bus. Rev. 2018, 20, 2019. [Google Scholar]
- Korczynski, M.; Evans, C. Customer abuse to service workers: An analysis of its social cretion within the service economy. Work. Employ. Soc. 2013, 27, 768–784. [Google Scholar] [CrossRef] [Green Version]
- Williams, C.; Drago, R.; Miller, K. 44 Million, U.S. Workers Lacked Paid Sick Days in 2010: 77 Percent of Food Service Workers Lacked Access (IWPR #B293); Institute for Women’s Policy Research: Washington, DC, USA, 2011. [Google Scholar]
- Sorensen, G.; Peters, S.E.; Nielsen, K.; Stelson, E.; Wallace, L.M.; Burke, L.; Nagler, E.M.; Roodbari, H.; Karapanos, M.; Wagner, G.R. Implementation of an organizational intervention to improve low-wage woerkers’ safety, health and wellbeing: Findings from the Workplace Organizational Health Study. Under Rev. 2021. [Google Scholar] [CrossRef]
- Alamgir, H.; Swinkels, H.; Yu, S.; Yassi, A. Occupational injury among cooks and food service workers in the healthcare sector. Am. J. Ind. Med. 2007, 50, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Cann, A.P.; Baker, A.M.; Hansen, A.; Massie, D.; Vandervoort, A.A. A five year retrospective analysis of occupational injuries and incidence reported at a research intensive Canadian university. Work (Read. Mass) 2008, 30, 171–184. [Google Scholar]
- U.S. Department of Labor; Bureau of Labor Statistics. Injury and Illness Rates Higher in Special Food Services Than In Broader Food Services Industry. Available online: https://www.bls.gov/opub/ted/2019/injury-and-illness-rates-higher-in-special-food-services-than-in-broader-food-services-industry.htm (accessed on 28 October 2020).
- Cocci, S.J.; Namasivayam, K.; Bordi, P. An investigation of ergonomic design and productivity improvements in foodservice production tables. Foodserv. Res. Int. 2005, 16, 53–59. [Google Scholar] [CrossRef]
- Filiaggi, A.J.; Courtney, T.K. Restaurant hazards: Practice-based approaches to disabling occupational injuries. Prof. Saf. 2003, 48, 18–23. [Google Scholar]
- Stephenson, J. Determining optimal work surface height for Surrey Memorial Hospital food service workers. J. Can. Diet. Assoc. 1994, 55, 39–41. [Google Scholar] [PubMed]
- Andersen, J.H.; Kaergaard, A.; Mikkelsen, S.; Jensen, U.F.; Frost, P.; Bonde, J.P.; Fallentin, N.; Thomsen, J.F. Risk factors in the onset of neck/shoulder pain in a prospective study of workers in industrial and service companies. Occup. Environ. Med. 2003, 60, 649–654. [Google Scholar] [CrossRef] [Green Version]
- Verma, S.K.; Chang, W.R.; Courtney, T.K.; Lombardi, D.A.; Huang, Y.H.; Brennan, M.J.; Mittleman, M.A.; Perry, M.J. Workers’ experience of slipping in U.S. limited-service restaurants. J. Occup. Environ. Hyg. 2010, 7, 491–500. [Google Scholar] [CrossRef]
- U.S. Department of Labor; Bureau of Labor Statistics. Annual Total Separations Rates by Industry and Region, Not Seasonally Adjusted, 2016–2020. Available online: https://www.bls.gov/news.release/jolts.t16.htm (accessed on 10 August 2021).
- Busch, C.; Koch, T.; Clasen, J.; Winkler, E.; Vowinkel, J. Evaluation of an organizational health intervention for low-skilled workers and immigrants. Hum. Relat. 2017, 70, 994–1016. [Google Scholar] [CrossRef]
- Haukka, E.; Leino-Arjas, P.; Viikari-Juntura, E.; Takala, E.P.; Malmivaara, A.; Hopsu, L.; Mutanen, P.; Ketola, R.; Virtanen, T.; Pehkonen, I.; et al. A randomized controlled trial on whether a participatory ergonomics intervention could prevent musculoskeletal disorders. Occup. Environ. Med. 2008, 65, 849–856. [Google Scholar] [CrossRef]
- Haukka, E.; Pehkonen, I.; Leino-Arjas, P.; Viikari-Juntura, E.; Takala, E.P.; Malmivaara, A.; Hopsu, L.; Mutanen, P.; Ketola, R.; Virtanen, T.; et al. Effect of a participatory ergonomics intervention on psychosocial factors at work in a randomized controlled trial. Occup. Environ. Med. 2010, 67, 170–177. [Google Scholar] [CrossRef]
- Siukola, A.; Virtanen, P.; Huhtala, H.; Nygård, C.-H. Absenteeism following a workplace intervention for older food industry workers. Occup. Med. 2011, 61, 583–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, K.; Fredslund, H.; Christensen, K.B.; Albertsen, K. Success or failure? Interpreting and understanding the impact of interventions in four similar worksites. Work Stress 2006, 20, 272–287. [Google Scholar] [CrossRef]
- Peters, S.E.; Nielsen, K.M.; Nagler, E.M.; Revette, A.C.; Madden, J.; Sorensen, G. Ensuring Organization-Intervention Fit for a Participatory Organizational Intervention to Improve Food Service Workers’ Health and Wellbeing: Workplace Organizational Health Study. J. Occup. Environ. Med. 2020, 62, e33–e45. [Google Scholar] [CrossRef]
- Nagler, E.M.; Pednekar, M.S.; Viswanath, K.; Sinha, D.N.; Aghi, M.B.; Pischke, C.R.; Ebbeling, C.B.; Lando, H.A.; Gupta, P.C.; Sorensen, G.C. Designing in the social context: Using the social contextual model of health behavior change to develop a tobacco control intervention for teachers in India. Health Educ. Res. 2013, 28, 113–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, S.E.; Trieu, H.D.; Manjourides, J.; Katz, J.N.; Dennerlein, J.T. Designing a Participatory Total Worker Health(®) Organizational Intervention for Commercial Construction Subcontractors to Improve Worker Safety, Health, and Well-Being: The "ARM for Subs" Trial. Int. J. Environ. Res. Public Health 2020, 17, 5093. [Google Scholar] [CrossRef] [PubMed]
- Vella, J. Learning to Listen Learning to Teach: The Power of Dialogue in Educating Adults; Josey-Bass: San Francisco, CA, USA, 2002. [Google Scholar]
- Nielsen, K.; Noblet, A. Organizational interventions: Where are we, where do we go from here? In Organizational Interventions for Health and Well-Being: A Handbook for Evidence-Based Practice; Nielsen, K., Noblet, A., Eds.; Routledge: Oxford, UK, 2018; pp. 1–23. [Google Scholar]
- McLellan, D.L.; Cabán-Martinez, A.J.; Nelson, C.C.; Pronk, N.P.; Katz, J.N.; Allen, J.D.; Davis, K.L.; Wagner, G.R.; Sorensen, G. Organizational Characteristics Influence Implementation of Worksite Health Protection and Promotion Pro-grams: Evidence From Smaller Businesses. J. Occup. Environ. Med. 2015, 57, 1009–1016. [Google Scholar] [CrossRef] [Green Version]
- Cherniack, M.; Morse, T.; Henning, R.; Seidner, A.; Punnett, L. Health promotion site selection blues: Barriers to participation and implementation. J. Occup. Environ. Med. 2010, 52, 626–634. [Google Scholar] [CrossRef]
- Hunt, M.K.; Lederman, R.; Stoddard, A.M.; LaMontagne, A.D.; McLellan, D.; Combe, C.; Barbeau, E.; Sorensen, G. Process evaluation of an integrated health promotion/occupational health model in WellWorks-2. Health Educ. Behav. 2005, 32, 10–26. [Google Scholar] [CrossRef]
- Pronk, N.P.; Katz, A.S.; Lowry, M.; Payfer, J.R. Reducing occupational sitting time and improving worker health: The Take-a-Stand Project, 2011. Prev. Chronic Dis. 2012, 9, E154. [Google Scholar] [CrossRef] [Green Version]
- von Thiele Schwarz, U.; Augustsson, H.; Hasson, H.; Stenfors-Hayes, T. Promoting employee health by integrating health protection, health promotion, and continuous improvement: A longitudinal quasi-experimental intervention study. J. Occup. Environ. Med. 2015, 57, 217–225. [Google Scholar] [CrossRef]
- Amabile, T.; Kramer, S.J. The Power of Small Wins. Harv. Bus. Rev. 2011, 89, 70–80. [Google Scholar]
- Lewis, C.; Darnell, D.; Kerns, S.; Monroe-DeVita, M.; Landes, S.J.; Lyon, A.R.; Stanick, C.; Dorsey, S.; Locke, J.; Marriott, B.; et al. Advancing efficient methodologies through community partnerships and team science. In Implementation Science, Proceedings of the 3rd Biennial Conference of the Society for Implementation Research Collaboration (SIRC) 2015, Seattle, WA, USA, 24–26 September 2015; BioMed Central Ltd: London, UK, 2016; Volume 11, (Suppl. 1), p. 85. [Google Scholar] [CrossRef] [Green Version]
- Nadeem, E.; Gleacher, A.; Beidas, R.S. Consultation as an implementation strategy for evidence-based practices across multiple contexts: Unpacking the black box. Adm. Policy Ment. Health 2013, 40, 439–450. [Google Scholar] [CrossRef] [Green Version]
- Quelch, J.; Boudreau, E.C. Building a Culture of Health: A New Imperative for Business; Springer International Publishing: Cham, Switzerland, 2016. [Google Scholar]
- Institute of Medicine. Integrating Employee Health: A Model Program for NASA; National Academy Press: Washington, DC, USA, 2005. [Google Scholar]
- Hunnicutt, D. Evaluation: Why, what, how, and when you should evaluate your wellness program. Absol. Advant. 2007, 6, 12–19. [Google Scholar]
- Escoffery, C.; Lebow-Skelley, E.; Haardoerfer, R.; Boing, E.; Udelson, H.; Wood, R.; Hartman, M.; Fernandez, M.E.; Mullen, P.D. A systematic review of adaptations of evidence-based public health interventions globally. Implement. Sci. 2018, 13, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Tamers, S.L.; Chosewood, L.C.; Childress, A.; Hudson, H.; Nigam, J.; Chang, C.C. Total Worker Health® 2014–2018: The Novel Approach to Worker Safety, Health, and Well-Being Evolves. Int. J. Environ. Res. Public Health 2019, 16, 321. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Occupational Safety and Health. Fundamentals of Total Worker Health Approaches: Essential Elements for Advancing Worker Safety, Health, and Well-Being; US Department of Health and Human Services; Centers for Disease Control and Prevention; National Institute for Occupational Safety and Health: Cincinnati, OH, USA, 2016.
- Hudson, H.L.; Nigam, J.A.S.; Sauter, S.L.; Chosewood, L.C.; Schill, A.L.; Howard, J. Total Worker Health; American Psychological Association: Washington, DC, USA, 2019. [Google Scholar]
- Tamers, S.L.; Streit, J.; Pana-Cryan, R.; Ray, T.; Syron, L.; Flynn, M.A.; Castillo, D.; Roth, G.; Geraci, C.; Guerin, R.; et al. Envisioning the future of work to safeguard the safety, health, and well-being of the workforce: A perspective from the CDC’s National Institute for Occupational Safety and Health. Am. J. Ind. Med. 2020, 63, 1065–1084. [Google Scholar] [CrossRef] [PubMed]
- Dennerlein, J.T.; Burke, L.; Sabbath, E.L.; Williams, J.A.R.; Peters, S.E.; Wallace, L.; Karapanos, M.; Sorensen, G. An Integrative Total Worker Health Framework for Keeping Workers Safe and Healthy During the COVID-19 Pandemic. Hum. Factors 2020, 62, 689–696. [Google Scholar] [CrossRef] [PubMed]
- Pronk, N.P.; McLellan, D.L.; Dennerlein, J.T.; Anderson, P.; Karapanos, M.; Nagler, E.; Schmidt, D.; Spoonheim, J.; Wallace, L.M.; Sorensen, G. Building Capacity for Integrated Occupational Safety, Health, and Well-Being Initiatives Using Guidelines for Total Worker Health® Approaches. J. Occup. Environ. Med. 2021, 63, 411–421. [Google Scholar] [CrossRef]
- Sorensen, G.; Pednekar, M.; Cordeira, L.S.; Pawar, P.; Nagler, E.M.; Stoddard, A.M.; Kim, H.Y.; Gupta, P.C. Effects of a worksite tobacco control intervention in India: The Mumbai worksite tobacco control study, a cluster-randomised trial. Tob. Control 2017, 26, 210–216. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Key Characteristic | Definition from the Implementation Guidelines |
|---|---|
| 1. Leadership commitment | Leadership makes worker safety, health, and well-being a clear priority for the entire organization. They drive accountability and provide the necessary resources and environment to create positive working conditions. |
| 2. Participation | Stakeholders at every level of an organization, including organized labor when applicable, help plan and carry out efforts to protect and promote worker safety, health, and well-being. |
| 3. Policies, programs, and practices focused on positive working conditions | The organization enhances worker safety, health, and well-being with policies, programs and practices that improve working conditions. |
| 4. Comprehensive and collaborative strategies | Employees from across the organization work together to develop comprehensive safety, health, and well-being initiatives. |
| 5. Adherence | The organization adheres to federal and state regulations, as well as ethical norms, that advance worker safety, health, and well-being. |
| 6. Data-driven change | Regular evaluation guides an organization’s priority setting, decision making, and continuous improvement of worker safety, health, and well-being initiatives. |
| Stage | Description from the Implementation Guidelines |
|---|---|
| 1. Engaging Leadership and Collaborators | Buy-in and collaboration from across the organization are important. Seek top leadership support early on, encourage collaboration, work closely with middle managers, and give workers clear opportunities to participate. |
| 2. Planning | Successful initiatives start with a clear plan. Define the goal and choose SMART (Specific-Measurable-Achievable-Relevant-Time Bound) objectives. Define working conditions; gather and analyze worksite information; select tactics; create an action plan; identify required resources. |
| 3. Implementation | Changes to policies, practices, and programs play out in the workplace. To facilitate implementation, start small, communicate about progress, and conduct training. |
| 4. Evaluation and Improvement | Monitor and analyze data to measure success and improve an initiative. Use a variety of data collection methods, evaluate as needed, and communicate findings frequently. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagler, E.M.; Stelson, E.A.; Karapanos, M.; Burke, L.; Wallace, L.M.; Peters, S.E.; Nielsen, K.; Sorensen, G. Using Total Worker Health® Implementation Guidelines to Design an Organizational Intervention for Low-Wage Food Service Workers: The Workplace Organizational Health Study. Int. J. Environ. Res. Public Health 2021, 18, 9383. https://doi.org/10.3390/ijerph18179383
Nagler EM, Stelson EA, Karapanos M, Burke L, Wallace LM, Peters SE, Nielsen K, Sorensen G. Using Total Worker Health® Implementation Guidelines to Design an Organizational Intervention for Low-Wage Food Service Workers: The Workplace Organizational Health Study. International Journal of Environmental Research and Public Health. 2021; 18(17):9383. https://doi.org/10.3390/ijerph18179383
Chicago/Turabian StyleNagler, Eve M., Elisabeth A. Stelson, Melissa Karapanos, Lisa Burke, Lorraine M. Wallace, Susan E. Peters, Karina Nielsen, and Glorian Sorensen. 2021. "Using Total Worker Health® Implementation Guidelines to Design an Organizational Intervention for Low-Wage Food Service Workers: The Workplace Organizational Health Study" International Journal of Environmental Research and Public Health 18, no. 17: 9383. https://doi.org/10.3390/ijerph18179383
APA StyleNagler, E. M., Stelson, E. A., Karapanos, M., Burke, L., Wallace, L. M., Peters, S. E., Nielsen, K., & Sorensen, G. (2021). Using Total Worker Health® Implementation Guidelines to Design an Organizational Intervention for Low-Wage Food Service Workers: The Workplace Organizational Health Study. International Journal of Environmental Research and Public Health, 18(17), 9383. https://doi.org/10.3390/ijerph18179383