
Characterization and Hazard Identification of Respirable Cement and Concrete Dust from Construction Activities


Abstract
:1. Introduction
2. Methodology
2.1. Laser Diffraction
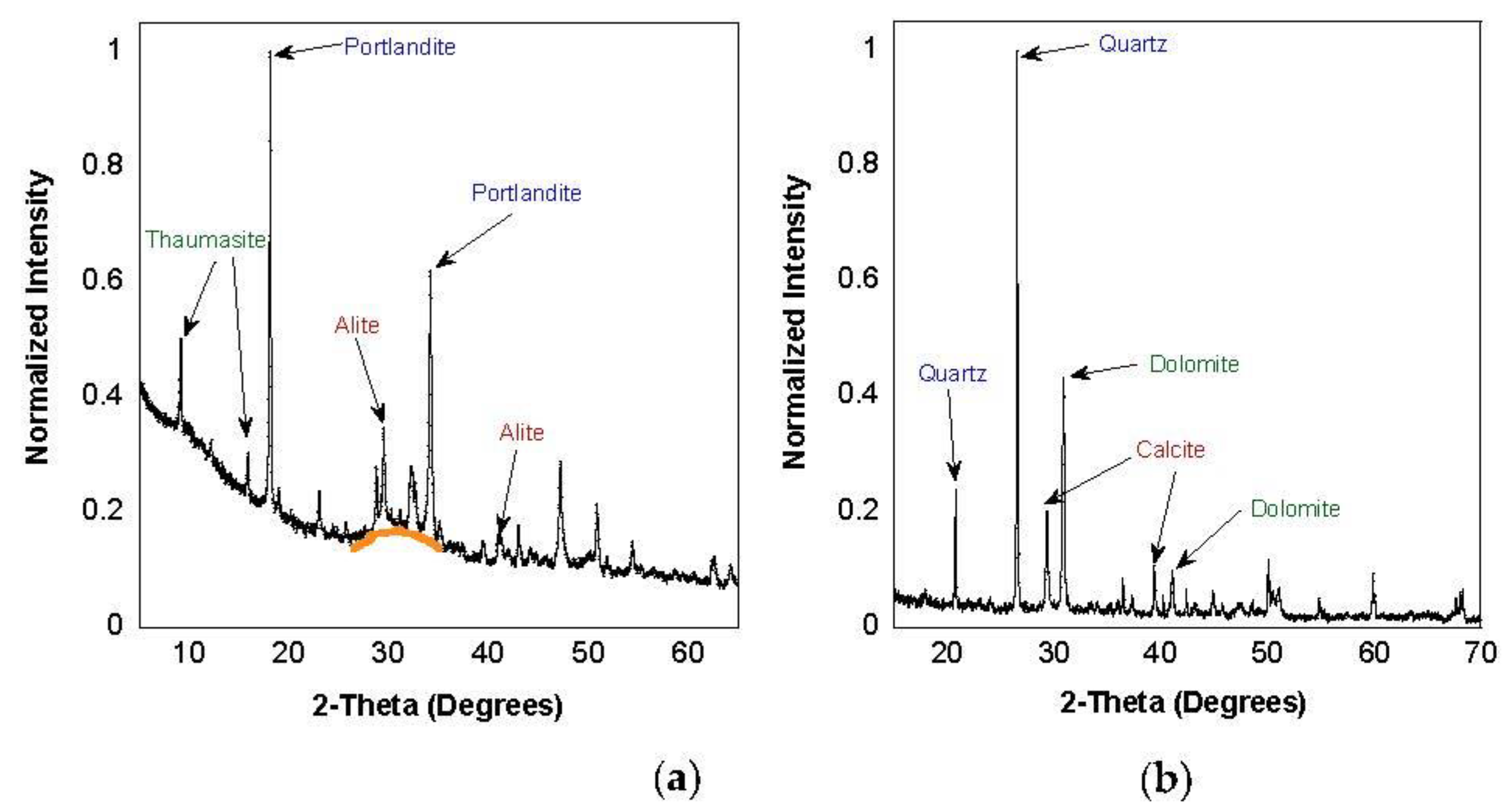
2.2. XRD
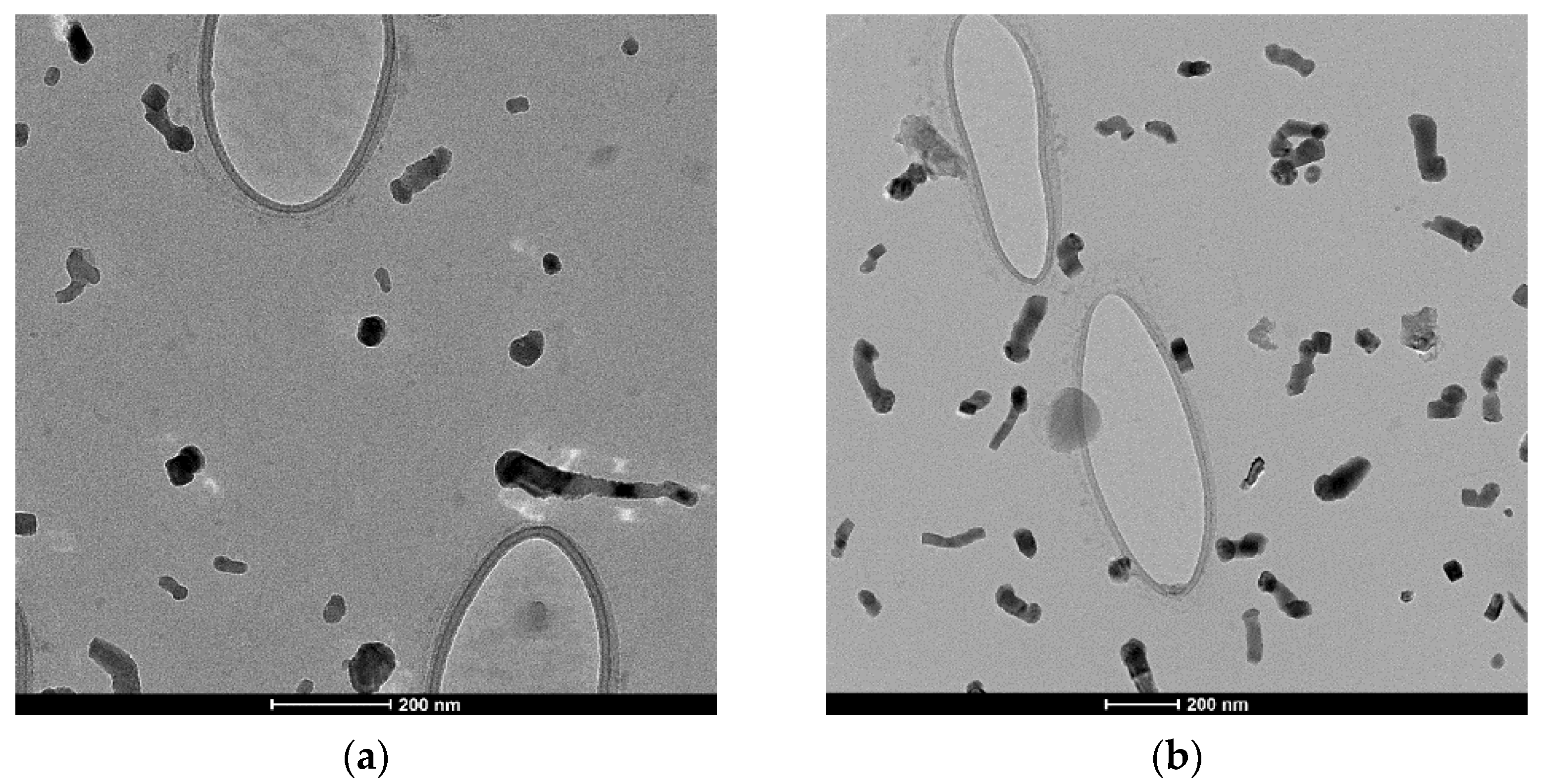
2.3. TEM
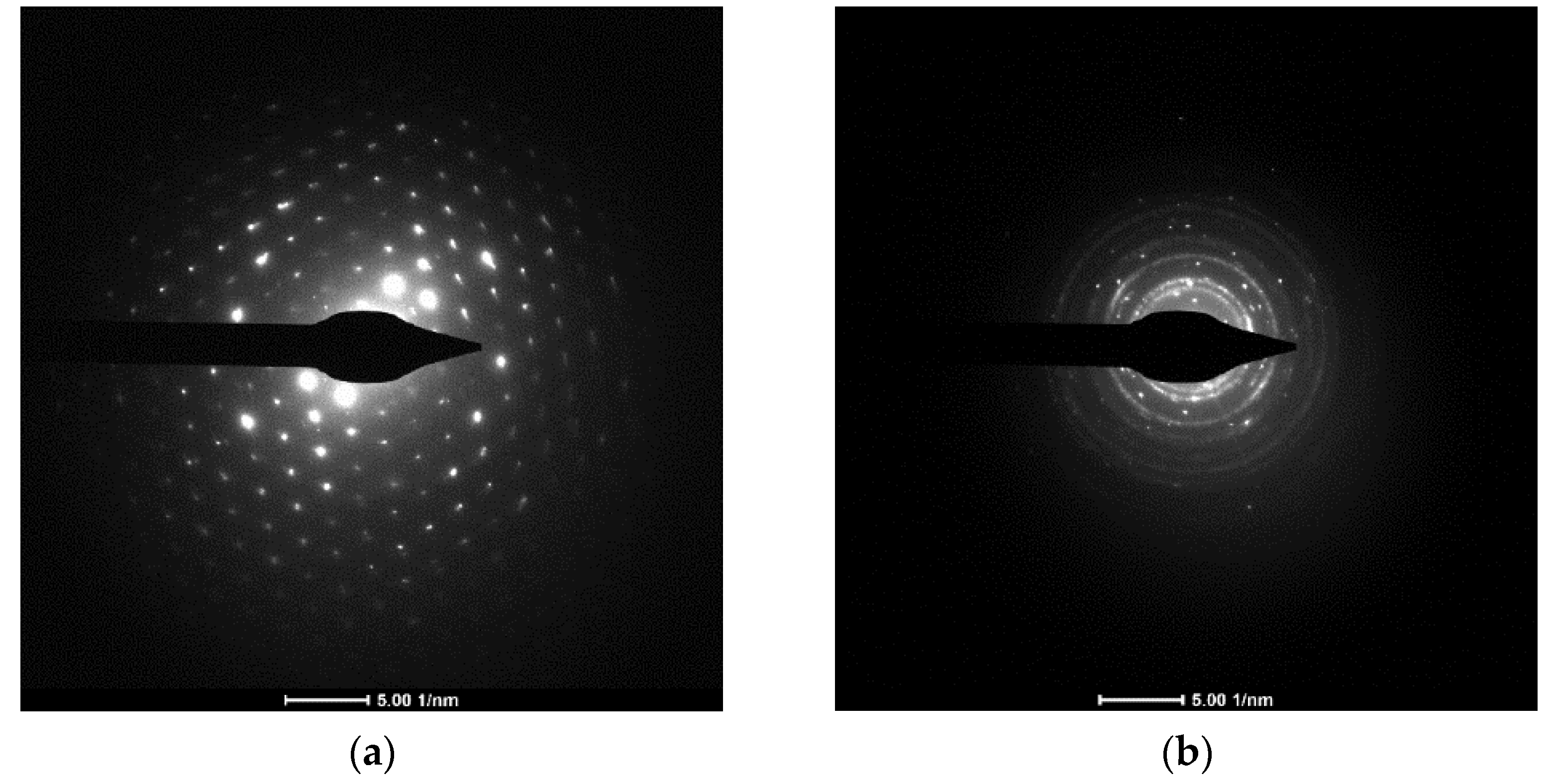
2.4. Electron Diffraction
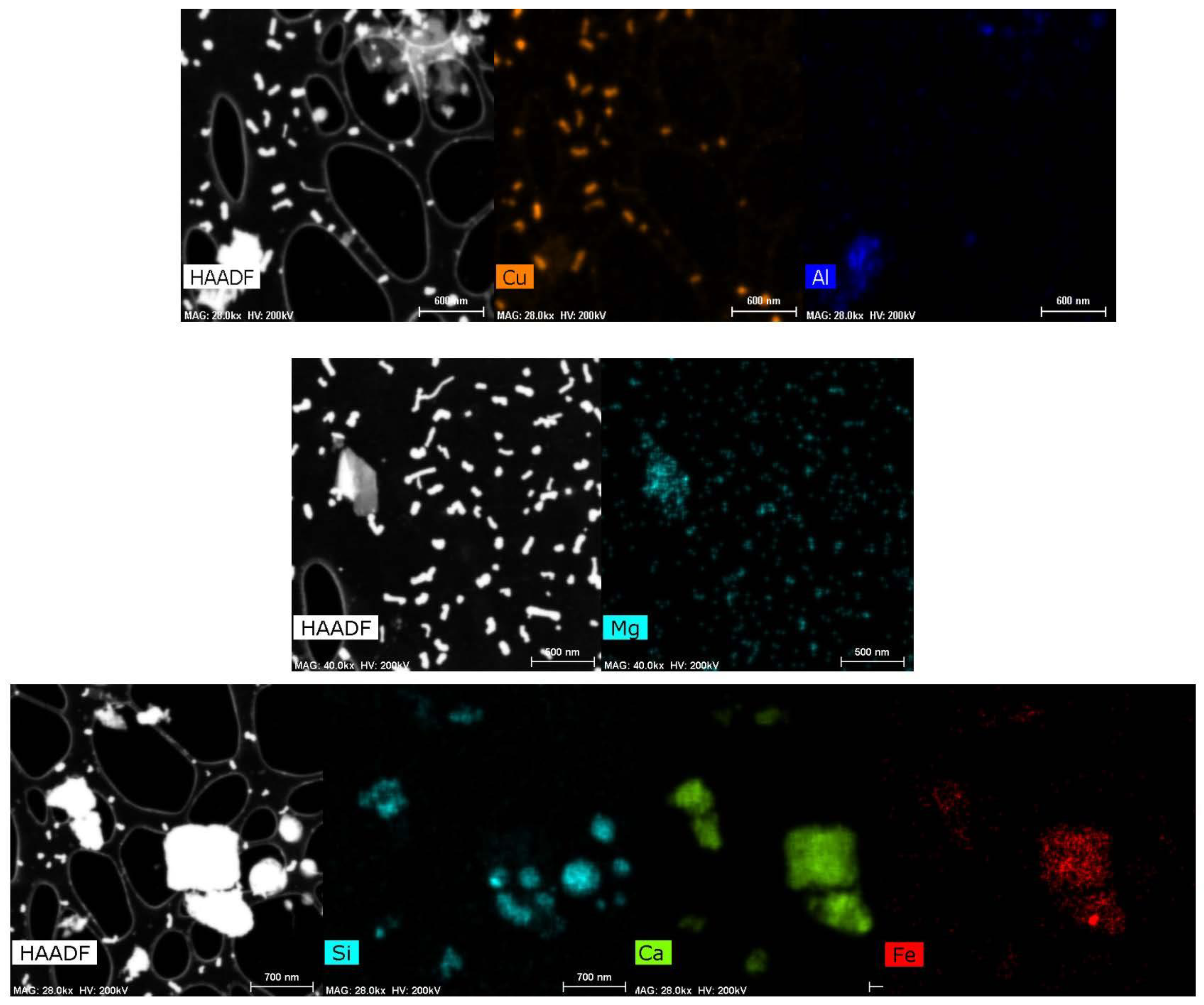
2.5. EDS
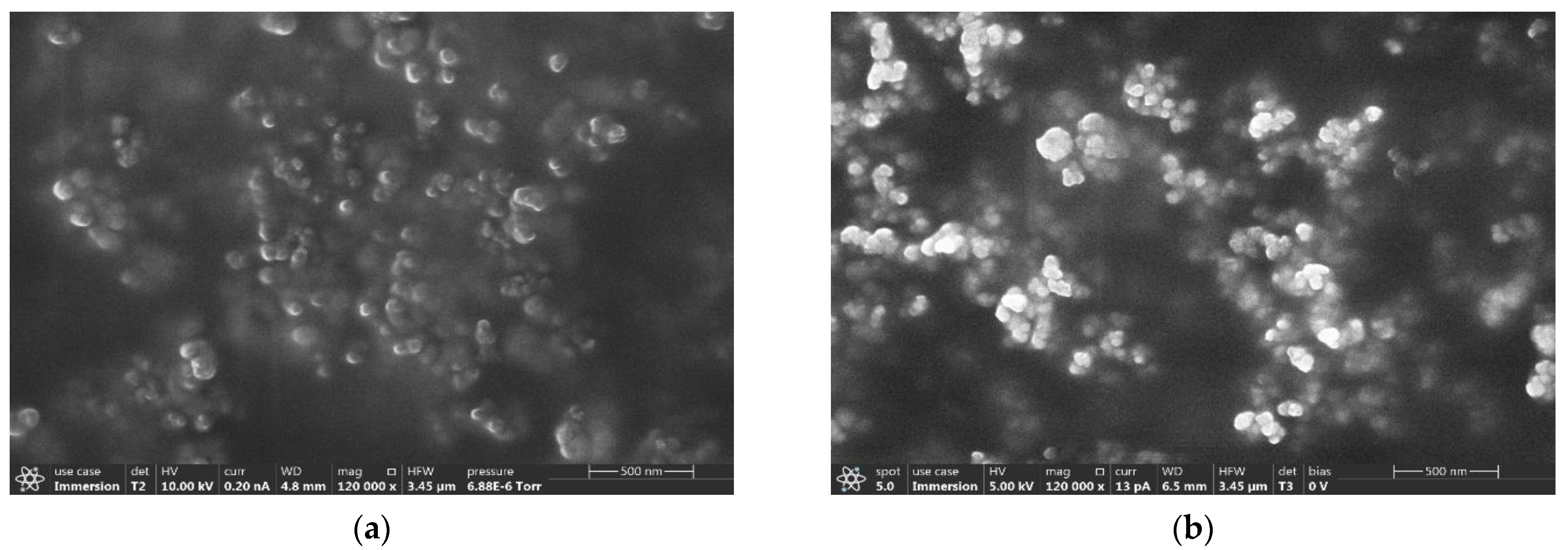
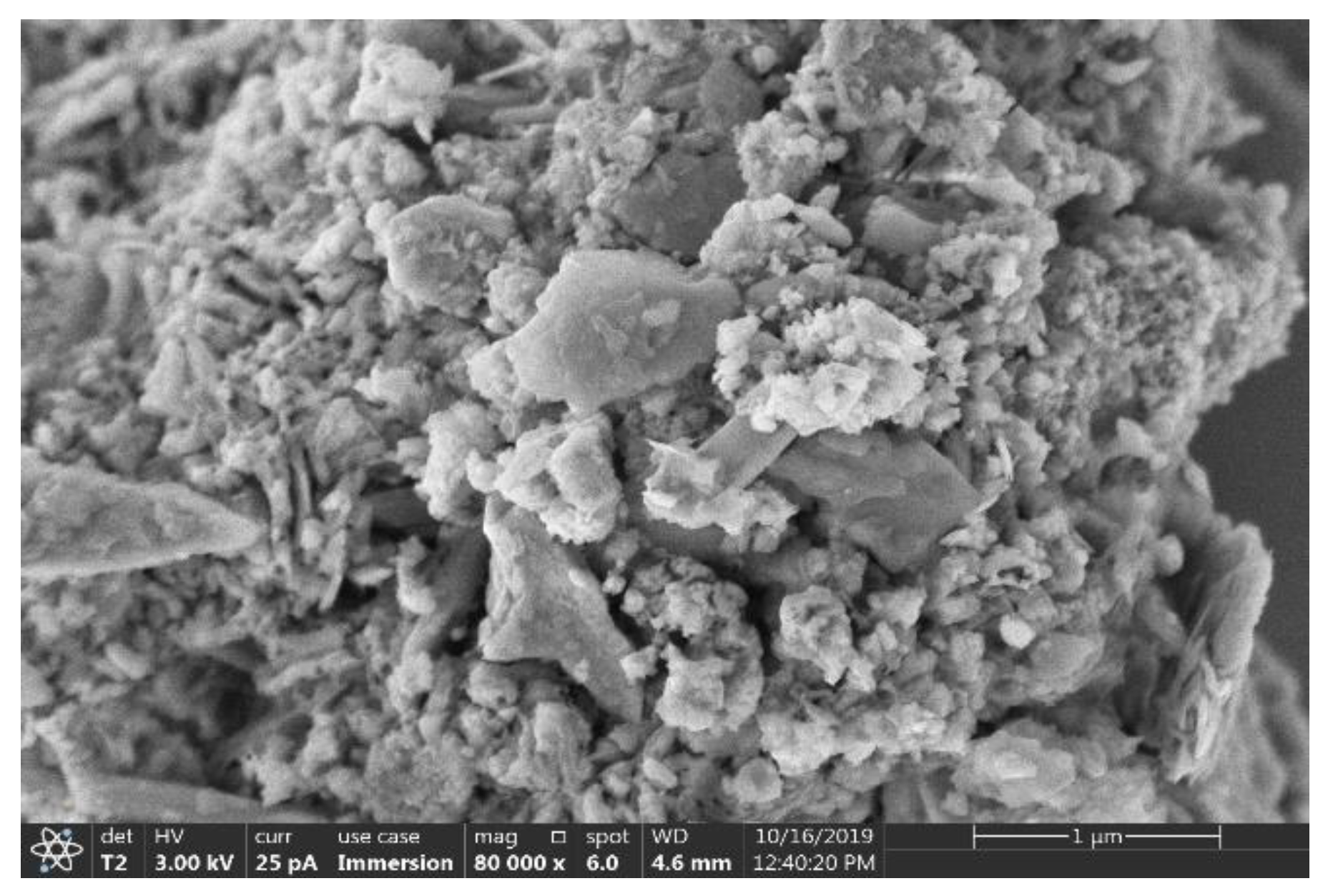
2.6. SEM
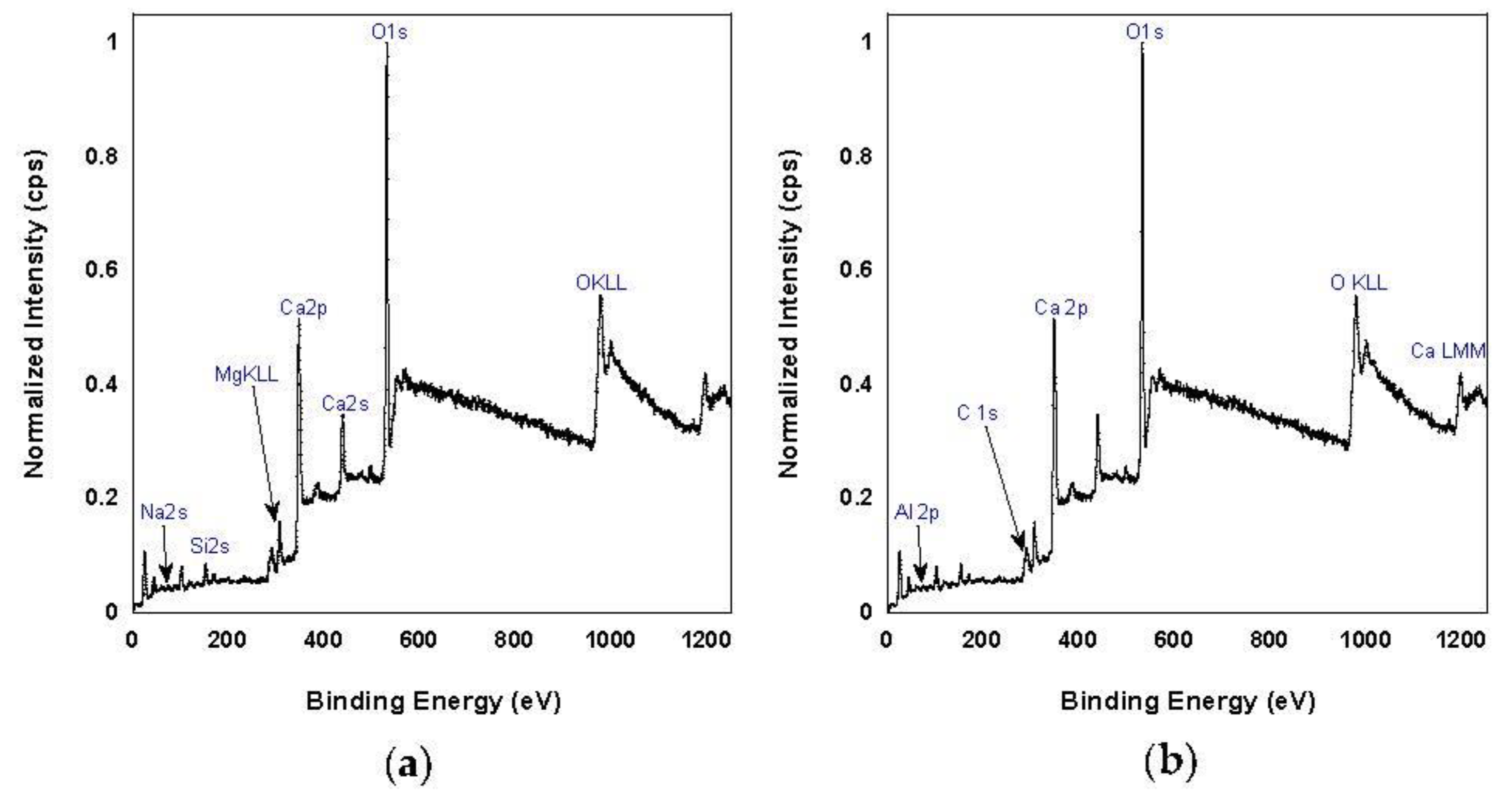
2.7. XPS
3. Discussion
3.1. Particle Size
3.2. Composition
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cement Masons and Concrete Finishers. May 2019. Available online: https://www.bls.gov/oes/current/oes472051.htm#TB_inline?height=200&width=325&inlineId=oes_program_links (accessed on 25 December 2019).
- Akbar-Khanzadeh, F.; Milz, S.; Ames, A.; Susi, P.P.; Bisesi, M.; Khuder, S.A.; Akbar-Khanzadeh, M. Crystalline silica dust and respirable particulate matter during indoor concrete grinding—wet grinding and ventilated grinding compared with uncontrolled conventional grinding. J. Occup. Environ. Hyg. 2007, 4, 770–779. [Google Scholar] [CrossRef] [PubMed]
- Linch, K.D. Respirable concrete dust—silicosis hazard in the construction industry. Appl. Occup. Environ. Hyg. 2002, 17, 209–221. [Google Scholar] [CrossRef] [PubMed]
- Kakooei, H.; Gholami, A.; Ghasemkhani, M.; Hosseini, M.; Panahi, D.; Pouryaghoub, G. Dust exposure and respiratory health effects in cement production. Acta Med. Iran. 2012, 50, 122–126. [Google Scholar] [PubMed]
- Alakija, W.; Iyawe, V.I.; Jarikre, L.N.; Chiwuzie, J.C. Ventilatory function of workers at Okpella cement factory in Nigeria. West. Afr. J. Med. 1990, 9, 187. [Google Scholar] [PubMed]
- Siracusa, A.; Forcina, A.; Volpi, R.; Mollichella, E.; Cicioni, C.; Fiordi, T. An 11-year longitudinal study of the occupational dust exposure and lung function of polyvinyl chloride, cement and asbestos cement factory workers. Scand. J. Work Environ. Health 1988, 14, 181–188. [Google Scholar] [CrossRef]
- Gomzi, M.; Stilinovic, L.; Godnic-Cvar, J. Alpha 1-antitrypsin and lung function in cement workers. Med. Lav. 1989, 80, 301. [Google Scholar]
- Al-Neaimi, Y.I.; Gomes, J.; Lloyd, O.L. Respiratory illnesses and ventilatory function among workers at a cement factory in a rapidly developing country. Occup. Med. 2001, 51, 367–373. [Google Scholar] [CrossRef] [Green Version]
- Noor, H. Effect of exposure to dust on lung function of cement factory workers. Med. J. Malays. 2000, 55, 51–57. [Google Scholar]
- Maier, H.; Gewelke, U.; Dietz, A.; Thamm, H.; Heller, W.D.; Weidauer, H. Laryngeal cancer and occupation—Results of the Heidelberg laryngeal cancer study. HNO 1992, 40, 44. [Google Scholar]
- Merenu, I.A.; Mojiminiyi, F.; Njoku, C.N.; Ibrahim, M. The effect of chronic cement dust exposure on lung function of cement factory workers in Sokoto, Nigeria. Afr. J. Biomed. Res. 2007, 10. [Google Scholar] [CrossRef] [Green Version]
- Bazas, T. Effects of occupational exposure to dust on the respiratory system of cement workers. Occup. Med. 1980, 30, 31–36. [Google Scholar] [CrossRef]
- Pimentel, J.C.; Menezes, A.P. Pulmonary and hepatic granulomatous disorders due to the inhalation of cement and mica dusts. Thorax 1978, 33, 219–227. [Google Scholar] [CrossRef] [Green Version]
- Meo, S.A.; Azeem, M.A.; Ghori, M.G.; Subhan, M.M. Lung function and surface electromyography of intercostal muscles in cement mill workers. Int. J. Occup. Med. Environ. Health 2002, 15, 279–287. [Google Scholar]
- Lucchini, R.G.; Dorman, D.C.; Elder, A.; Veronesi, B. Neurological impacts from inhalation of pollutants and the nose–brain connection. Neurotoxicology 2012, 33, 838–841. [Google Scholar] [CrossRef] [Green Version]
- Heusinkveld, H.J.; Wahle, T.; Campbell, A.; Westerink, R.H.; Tran, L.; Johnston, H.; Schins, R.P. Neurodegenerative and neurological disorders by small inhaled particles. Neurotoxicology 2016, 56, 94–106. [Google Scholar] [CrossRef]
- Manjula, R.; Praveena, R.; Clevin, R.R.; Ghattargi, C.H.; Dorle, A.S.; Lalitha, D.H. Effects of occupational dust exposure on the health status of portland cement factory workers. Int. J. Med. Public Health 2013, 3, 192–196. [Google Scholar] [CrossRef] [Green Version]
- Emmanuel, T.F.; Ibiam, U.A.; Okaka, A.N.; Alabi, O.J. Effects of cement dust on the hematological parameters in Obajana cement factory workers. Eur. Sci. J. 2015, 11, 256–266. [Google Scholar]
- Jude, A.C.; Sasikala, K.; Kumar, R.A.; Sudha, S.; Raichel, J. Haematological and cytogenetic studies in workers occupationally exposed to cement dust. Int. J. Hum. Genet. 2002, 2, 95–99. [Google Scholar] [CrossRef]
- Hougaard, K.S.; Campagnolo, L.; Chavatte-Palmer, P.; Tarrade, A.; Rousseau-Ralliard, D.; Valentino, S.; Ross, B.L. A perspective on the developmental toxicity of inhaled nanoparticles. Reprod. Toxicol. 2015, 56, 118–140. [Google Scholar] [CrossRef]
- Mehraj, S.S.; Bhat, G.A.; Balkhi, H.M. Cement factories and human health. Int. J. Cur. Res. Rev. 2013, 5, 47–54. [Google Scholar]
- Bertoldi, M.; Borgini, A.; Tittarelli, A.; Fattore, E.; Cau, A.; Fanelli, R.; Crosignani, P. Health effects for the population living near a cement plant: An epidemiological assessment. Environ. Int. 2012, 41, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Nkhama, E.; Ndhlovu, M.; Dvonch, J.T.; Lynam, M.; Mentz, G.; Siziya, S.; Voyi, K. Effects of airborne particulate matter on respiratory health in a community near a cement factory in Chilanga, Zambia results from a panel study. Int. J. Environ. Res. Public Health 2017, 14, 1351. [Google Scholar] [CrossRef] [Green Version]
- Richard, E.E.; Augusta Chinyere, N.A.; Jeremaiah, O.S.; Opara UC, A.; Henrieta, E.M.; Ifunanya, E.D. Cement dust exposure and perturbations in some elements and lung and liver functions of cement factory workers. J. Toxicol. 2016, 2016. [Google Scholar] [CrossRef] [Green Version]
- Meo, S.A. Health hazards of cement dust. Saudi. Med. J. 2004, 25, 1153–1159. [Google Scholar]
- Riediker, M.; Zink, D.; Kreyling, W.; Oberdörster, G.; Elder, A.; Graham, U.; Kobayashi, T. Particle toxicology and health-where are we? Part. Fibre Toxicol. 2019, 16, 19. [Google Scholar] [CrossRef]
- Adeyanju, E.; Okeke, C.A. Exposure effect to cement dust pollution a mini review. SN Appl. Sci. 2019, 1, 1572. [Google Scholar] [CrossRef] [Green Version]
- Work Safely with Concrete and Cement. 2019. Available online: https://safeatworkca.com/working-safely-with-concrete-and-cement/ (accessed on 27 December 2020).
- Hazardous Substance Fact Sheet-Calcium Hydroxide. Available online: https://nj.gov/health/eoh/rtkweb/documents/fs/0322.pdf (accessed on 5 February 2021).
- Calcium Hydroxide Poisoning. 9 September 2019. Available online: http://pennstatehershey.adam.com/content.aspx?productid=117&pid=1&gid=002910#~text=Scars%20may%20form%20in%20these,eye%2C%20permanent%20blindness%20can%20result (accessed on 5 February 2021).
- Charrier, J.G.; Anastasio, C. Rates of hydroxyl radical production from transition metals and quinones in a surrogate lung fluid. Environ. Sci. Technol. 2015, 49, 9317–9325. [Google Scholar] [CrossRef] [Green Version]
- Hackley, V.A.; Hackley, V.A.; Gintautas, V.; Ferraris, C.F. Particle Size Analysis by Laser Diffraction Spectrometry Application to Cementitious Powders; US Department of Commerce, National Institute of Standards and Technology: Gaithersburg, MD, USA, 2004. [Google Scholar]
- Particulate Matter Basics. 14 November 2018. Available online: https://www.epa.gov/pm-pollution/particulate-matter-pm-basics (accessed on 26 September 2021).
- Roach, S.A. Sampling air for particulates. The Industrial Environment—Its Evaluation and Control; Cincinnati, US Dept of Health, Education, and Welfare, Public Health Service, Center for Disease Control, National Institute for Occupational Safety and Health: Washington, DC, USA, 1973; pp. 139–153. [Google Scholar]
- Hall, S.A. Airborne Contaminants. In Occupational Health Practice; Butterworth-Heinemann: London, UK, 1973; pp. 288–308. [Google Scholar]
- Winder, C.; Carmody, M. The dermal toxicity of cement. Toxicol. Ind. Health 2002, 18, 321–331. [Google Scholar] [CrossRef]
- Castranova, V.; Dalal, N.S.; Vallyathan, V. Role of surface free radicals in the pathogenicity of silica. In Silica and Silica-Induced Diseases; CRC: Boca Raton, FL, USA, 1996; pp. 91–105. [Google Scholar]
- Occupational Safety and Health Administration. Occupational Exposure to Respirable Crystalline Silica—Review of Health Effects Literature and Preliminary Quantitative Risk Assessment; OSHA: Washington, DC, USA, 2010.
- Wikipedia Contributors. Silicosis. Wikipedia, The Free Encyclopedia. Available online: https://en.wikipedia.org/w/index.php?title=Silicosis&oldid=953534302 (accessed on 27 April 2020).
- Donaldson, K.; Tran, C.L. Inflammation caused by particles and fibers. Inhal. Toxicol. 2002, 14, 5–27. [Google Scholar] [CrossRef] [PubMed]
- Nordby, K.C.; Notø, H.; Eduard, W.; Skogstad, M.; Fell, A.K.; Thomassen, Y.; Kongerud, J. Thoracic dust exposure is associated with lung function decline in cement production workers. Eur. Respir. J. 2016, 48, 331–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fell, A.K.M.; Sikkeland, L.I.B.; Svendsen, M.V.; Kongerud, J. Airway inflammation in cement production workers. Occup. Environ. Med. 2010, 67, 395–400. [Google Scholar] [CrossRef] [Green Version]
- van Berlo, D.; Haberzettl, P.; Gerloff, K.; Li, H.; Scherbart, A.M.; Albrecht, C.; Schins, R.P. Investigation of the cytotoxic and proinflammatory effects of cement dusts in rat alveolar macrophages. Chem. Res. Toxicol. 2009, 22, 1548–1558. [Google Scholar] [CrossRef] [PubMed]
- Dixon, S.J.; Stockwell, B.R. The role of iron and reactive oxygen species in cell death. Nat. Chem. Biol. 2014, 10, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Chemical Properties of Magnesium—Health Effects of Magnesium—Environmental Effects of Magnesium. Available online: https://www.lenntech.com/periodic/elements/mg.htm#ixzz6R9lomJ00 (accessed on 19 January 2020).
- Aluminum Properties—Health Effects of Aluminum—Environmental Effects of Aluminum. Available online: https://www.lenntech.com/periodic/elements/al.htm (accessed on 8 August 2020).
- Peters, S.; Reid, A.; Fritschi, L.; De Klerk, N.; Musk, A.B. Long-term effects of aluminium dust inhalation. Occup. Environ. Med. 2013, 70, 864–868. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phases | wt.% |
|---|---|
| Portlandite | 38.5 |
| Thaumasite | 31.6 |
| Lamite | 7.8 |
| Alite monoclinic | 7.3 |
| Calcite | 6.9 |
| Gypsum | 4.8 |
| Periclase | 3.0 |
| Phases | wt.% |
|---|---|
| Dolomite | 45.1 |
| Quartz | 32.2 |
| Calcite | 18.3 |
| Portlandite | 2.2 |
| Pseudo-wollastonite | 2.3 |
| Element | wt.% |
|---|---|
| Silicon | 10.10 |
| Calcium | 38.32 |
| Oxygen | 36.14 |
| Aluminum | 1.68 |
| Magnesium | 0.30 |
| Iron | 1.09 |
| Sulfur | 1.73 |
| Carbon | 10.64 |
| Chromium | 0.008 |
| Element | wt.% |
|---|---|
| Silicon | 32.56 |
| Calcium | 2.79 |
| Oxygen | 38.85 |
| Aluminum | 9.52 |
| Magnesium | 0.31 |
| Iron | 0.17 |
| Sulfur | 0.08 |
| Carbon | 3.20 |
| Potassium | 12.40 |
| Sodium | 0.132 |
| Element | wt.% |
|---|---|
| Aluminum | 1.1 |
| Calcium | 17.8 |
| Iron | - |
| Potassium | 0.8 |
| Magnesium | 1.2 |
| Sodium | - |
| Oxygen | 59.1 |
| Silicon | 4.4 |
| Carbon | 15.5 |
| Element | wt.% |
|---|---|
| Aluminum | 3.7 |
| Calcium | 12.4 |
| Iron | 0.2 |
| Potassium | 0.6 |
| Magnesium | 4.4 |
| Sodium | 2.8 |
| Oxygen | 52.7 |
| Silicon | 8.8 |
| Carbon | 14.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gharpure, A.; Heim, J.W., II; Vander Wal, R.L. Characterization and Hazard Identification of Respirable Cement and Concrete Dust from Construction Activities. Int. J. Environ. Res. Public Health 2021, 18, 10126. https://doi.org/10.3390/ijerph181910126
Gharpure A, Heim JW II, Vander Wal RL. Characterization and Hazard Identification of Respirable Cement and Concrete Dust from Construction Activities. International Journal of Environmental Research and Public Health. 2021; 18(19):10126. https://doi.org/10.3390/ijerph181910126
Chicago/Turabian StyleGharpure, Akshay, James William Heim, II, and Randy L. Vander Wal. 2021. "Characterization and Hazard Identification of Respirable Cement and Concrete Dust from Construction Activities" International Journal of Environmental Research and Public Health 18, no. 19: 10126. https://doi.org/10.3390/ijerph181910126
APA StyleGharpure, A., Heim, J. W., II, & Vander Wal, R. L. (2021). Characterization and Hazard Identification of Respirable Cement and Concrete Dust from Construction Activities. International Journal of Environmental Research and Public Health, 18(19), 10126. https://doi.org/10.3390/ijerph181910126