1. Introduction
Cement and concrete are essential elements of modern-day infrastructure. Cement is the most common ingredient used in the construction industry as a binding material which sets and cures over time due to chemical reaction with water. Concrete is a mixture of sand, coarse stones, and cement. Water is added to concrete to activate the cement, which binds the mixture together. By the addition of coarse stones or aggregates, concrete can serve as a building material. Construction activities involving sawing, cutting, and grinding of cast cementitious and cured concrete expose construction workers to a cloud of crystalline dust particles. Exposure to these particles can be a serious health hazard. The Bureau of Labor Statistics estimates that more than 196,000 workers are employed as cement masons and concrete finishers in the USA alone [
1]. Their occupation involves smoothening and finishing concrete surfaces with a variety of hand and power tools, which exposes them to the resultant dust. Several other trades including laborers may also perform concrete grinding activities, adding significantly to the total number of exposed workers [
2]. In several of these occupations, the crystalline silica exposure from respirable construction dust can exceed by several hundred times that of the NIOSH Recommended Exposure Limit (REL) of 0.05 mg/m
3 [
3]. With such a large portion of the working-age population at stake, there is a necessity to characterize and analyze the dust for its potential adverse health impacts.
In cement plants, cough, sputum, and breathing difficulty is prevalent in exposed workers [
4]. Several studies indicate that chronic exposure to cement dust can significantly lower pulmonary functions with duration of exposure [
5,
6,
7,
8]. Furthermore, cement dust is also known to cause cancer of the larynx and lung [
9,
10]. Animal studies have shown that the dust can cause emphysema and fibrosis in lung tissues [
11,
12].
Cement dust inhalation appears to have secondary impacts as well because of its ability to reach various organs. Pimentel et al. inferred that the inhaled cement particles can enter into the bloodstream and reach the liver because swelling, inflammation, and lesions were found around the liver in cement mill workers [
13]. Meo et al. found decreased performance of intercostal muscles and suggested that when cement dust enters the bloodstream, it can also reach and deposit into skeletal muscles, affecting their structure and performance [
14]. More recently, inhaled particles were seen to cause disorders in the nervous system [
15,
16]. Other unhealthy traits such as higher blood pressure and significant increase in weight were found to be statistically prominent in exposed workers [
17]. Studies have also revealed an association between cement dust exposure and lowering of hemoglobin and red blood cells in workers [
18,
19]. Some research groups have also speculated about the translocation of inhaled particles from the respiratory tract to the placenta and fetus, potentially affecting the offspring [
20]. Studies have shown that suspended cement particles not only affect cement workers but also residents living near a cement factory or other sources of cement dust from manufacturing operations [
21,
22,
23,
24].
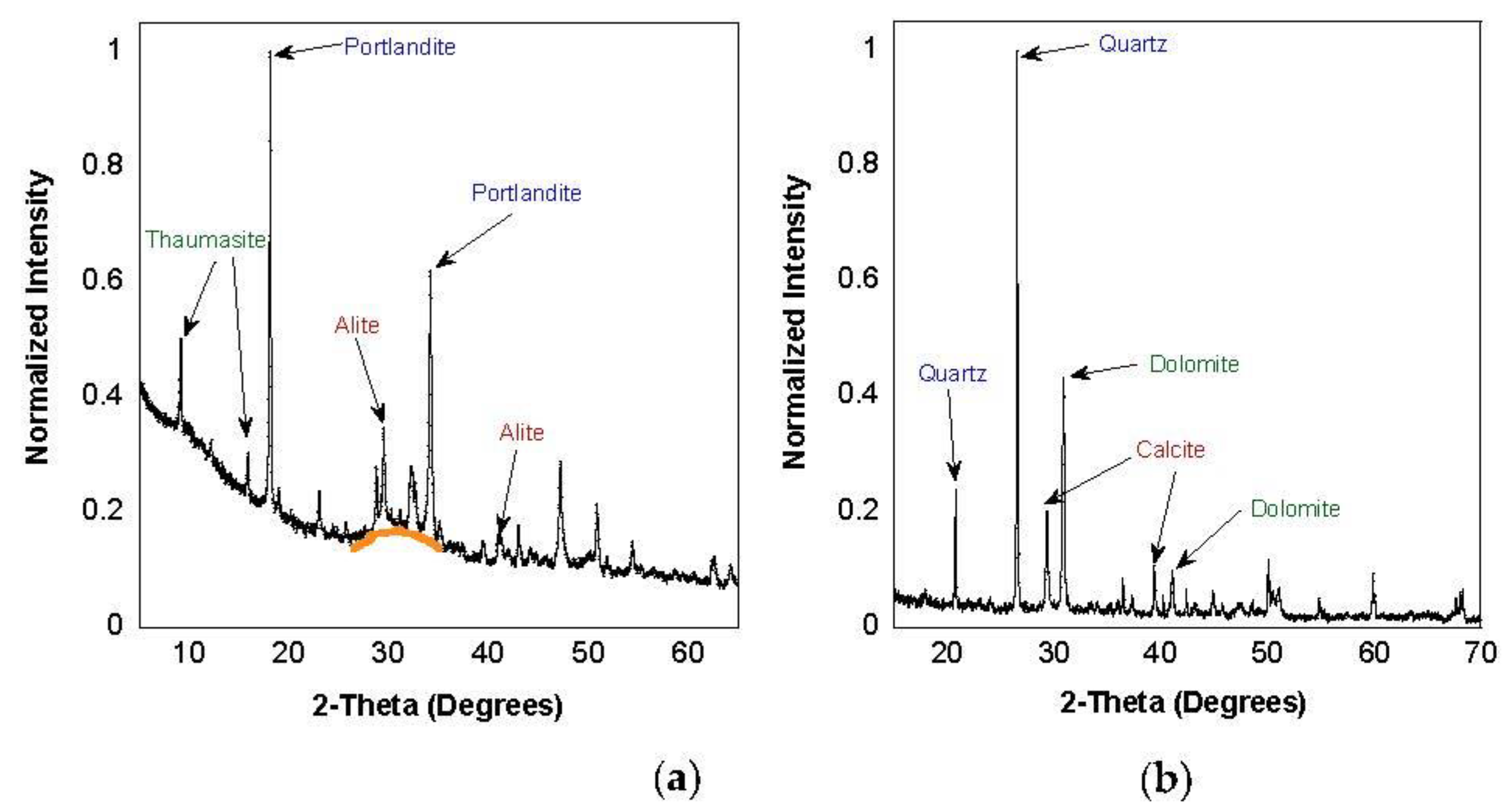
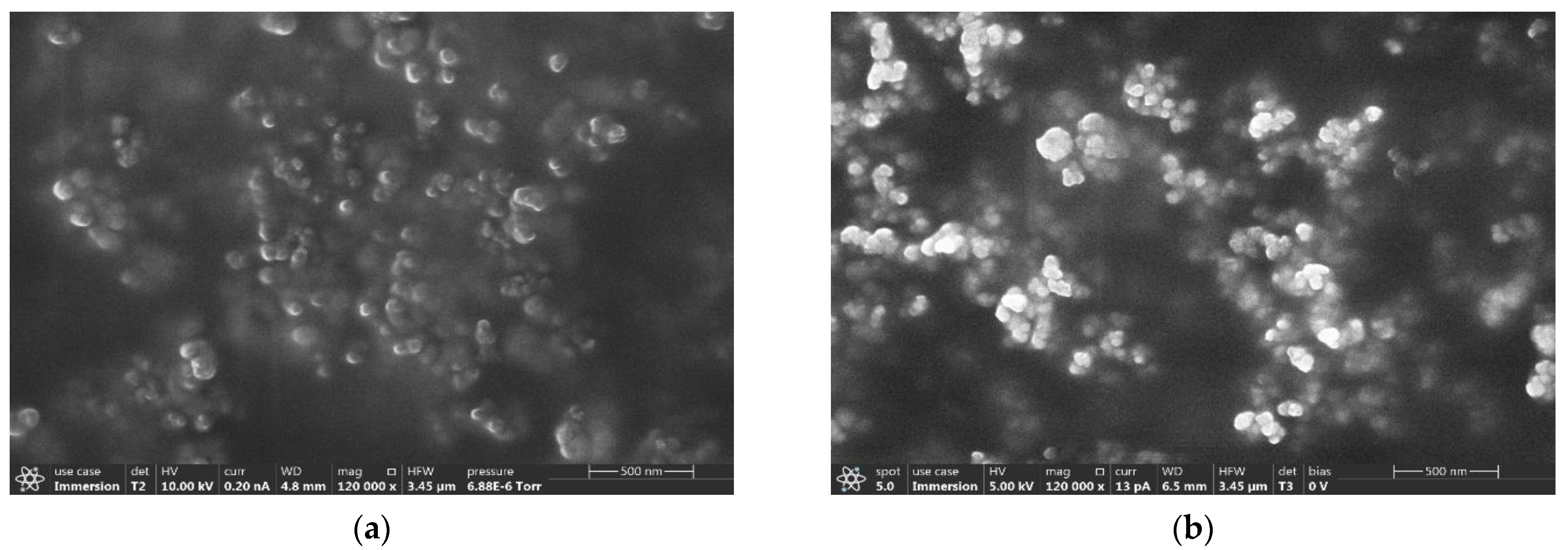
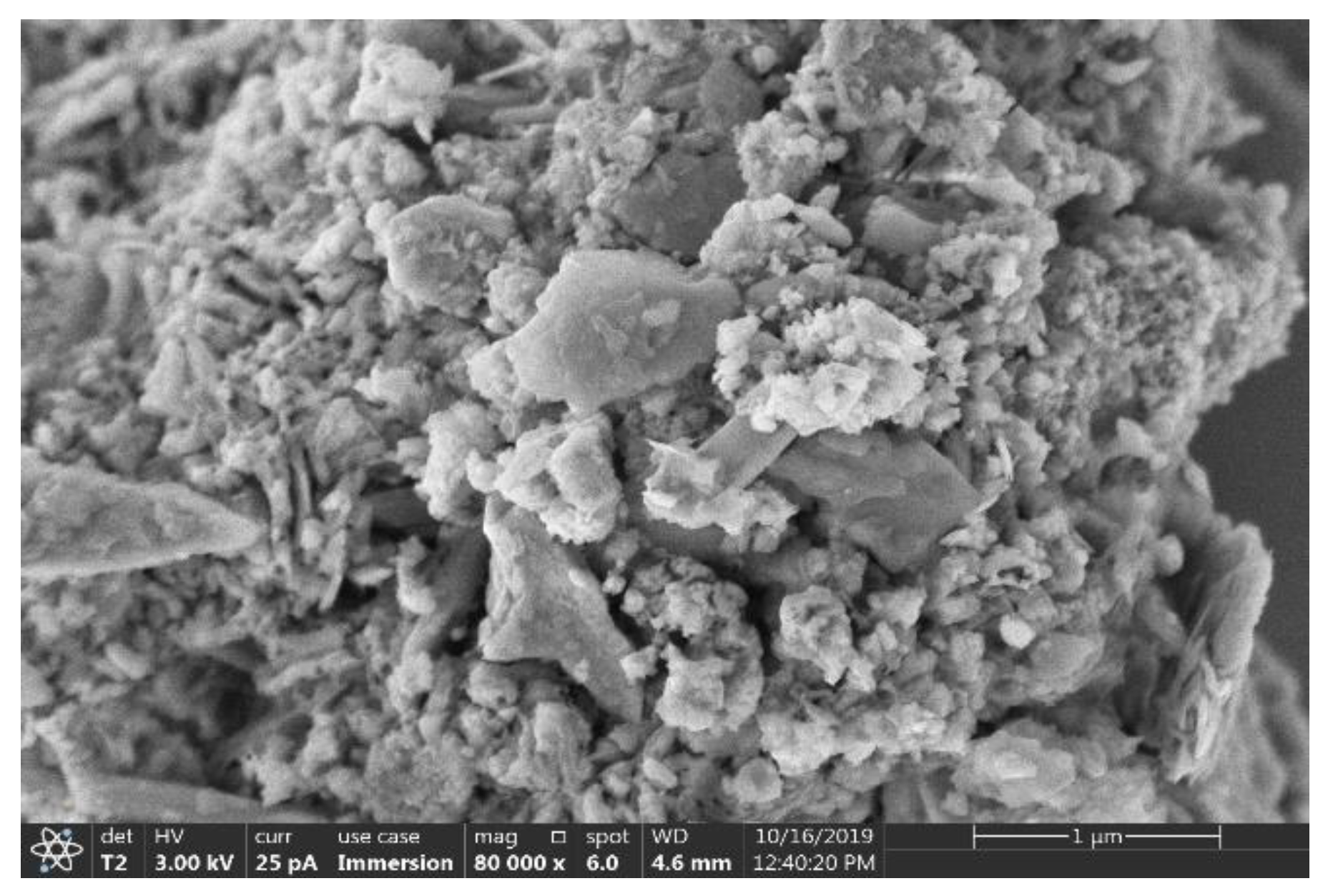
Differentiated from these workplace and exposure studies are construction activities involving the action of sawing, cutting, or grinding of cementitious materials and concrete. After casting or pouring and subsequent curing, the mineralogic composition of cement and concrete has changed. Well-known mineral forms include portlandite and quartz, each with its own crystalline structure and elemental composition. As often observed at building sites, and sidewalk and highway repair, clouds of dust are generated by the often-used circular saws. The duration of these particles being suspended in air and how far they travel from the source of emission is dependent of the particle size distribution of the dust. The finer particles can remain suspended longer and reach farther distances. In addition, particle translocation and associated secondary impacts seen in various other organs such as liver, heart, spleen, muscles, and so on, are also size dependent, as found in multiple studies [
14,
15,
16,
25,
26]. Particles finer than 2.5 μm are more hazardous, as they enter deeper into the pulmonary system and bloodstream [
27] and further reach other organs. Hence, a study of dust size distribution generated during cutting activities is critical.
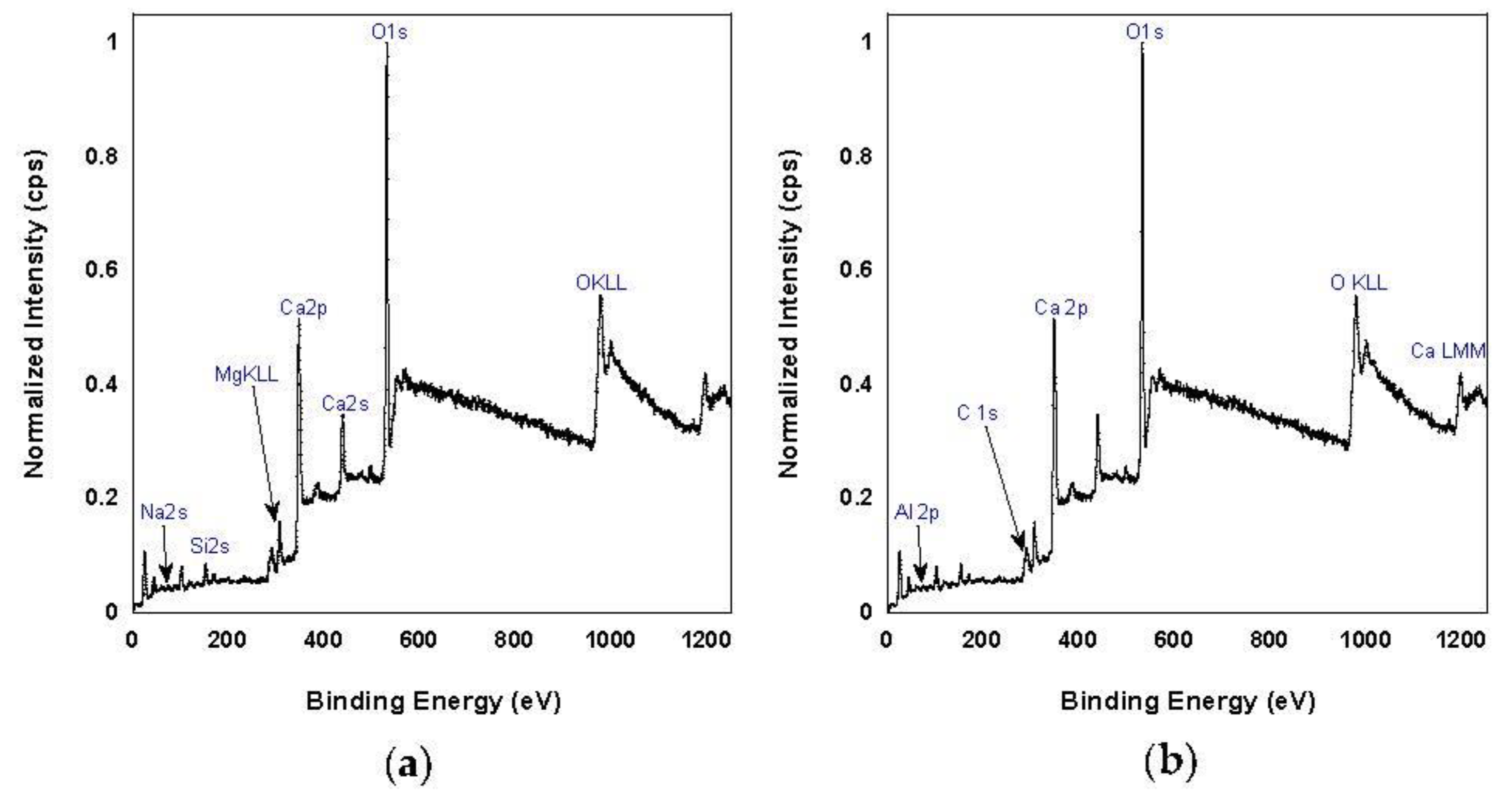
Apart from particle size, the chemical composition of the dust also has a direct impact on the hazards posed by the dust particles. With reference to the components of cement and concrete products, crystalline silica is a known abrasive to the lung tissues and the cause of silicosis [
28]. Calcium hydroxide causes irritation of the nose and throat with a risk of permanent lung damage [
29,
30]. Inhalation of dust containing metal content in the dust particles can also contribute to inflammation and lung damage [
31].
Although the chemical composition of cement and concrete can be easily read off the manufacturer’s data sheet, the chemical phases in the cement undergo substantial changes after hydration and setting. In addition, surface composition can be more important than overall composition, as the particle surface is what will be in direct contact with cell membranes. Surface composition can differ from the overall particle composition, contingent on the way cleavage occurs at the mineral phase boundaries in cement and concrete during the cutting activities. In addition, some of the chemical phases may separate out and preferentially form finer particles, depending on hardness and other physical properties of different phases and dynamics occurring during scission. Therefore, an in-depth study regarding the chemical nature of the dust is crucial for assessing the health concerns.
To understand the risks of cement and concrete dust toxicity, it is necessary to quantify the physical and chemical properties of these particles. Prolonged exposure to even small concentrations of toxins can be a serious health concern. To our knowledge, no study to date has collected and performed size and chemical characterization of actual dust produced by cutting and grinding cement-based construction materials. To date, studies and regulations have focused upon cement dust exposure from factories. However, as routinely observed at construction sites, pre-cast concrete panels require cutting (e.g., for making slots and holes). Similarly, the replacement and repair work observed routinely on highways exposes the road crews (and passers-by) to cement dust during cutting. Workers are commonly seen without respiratory protection; even a mask is not required for such work. Although cutting of cement and concrete is extensive, surprisingly, very little is known about the particulate emissions from such activities. The toxic effects of this inhalation hazard will fundamentally depend upon particulate properties such as size, surface area, chemical composition, and crystalline structure. This study aimed to characterize the physico-chemical properties of cementitious dust as a basis for gauging potential health hazards. Armed with this knowledge, appropriate precautions and protective actions can be implemented.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}