
Neonatal Outcomes after Combined Opioid and Nicotine Exposure in Utero: A Scoping Review

 , , and
, , and
Abstract
:1. Introduction
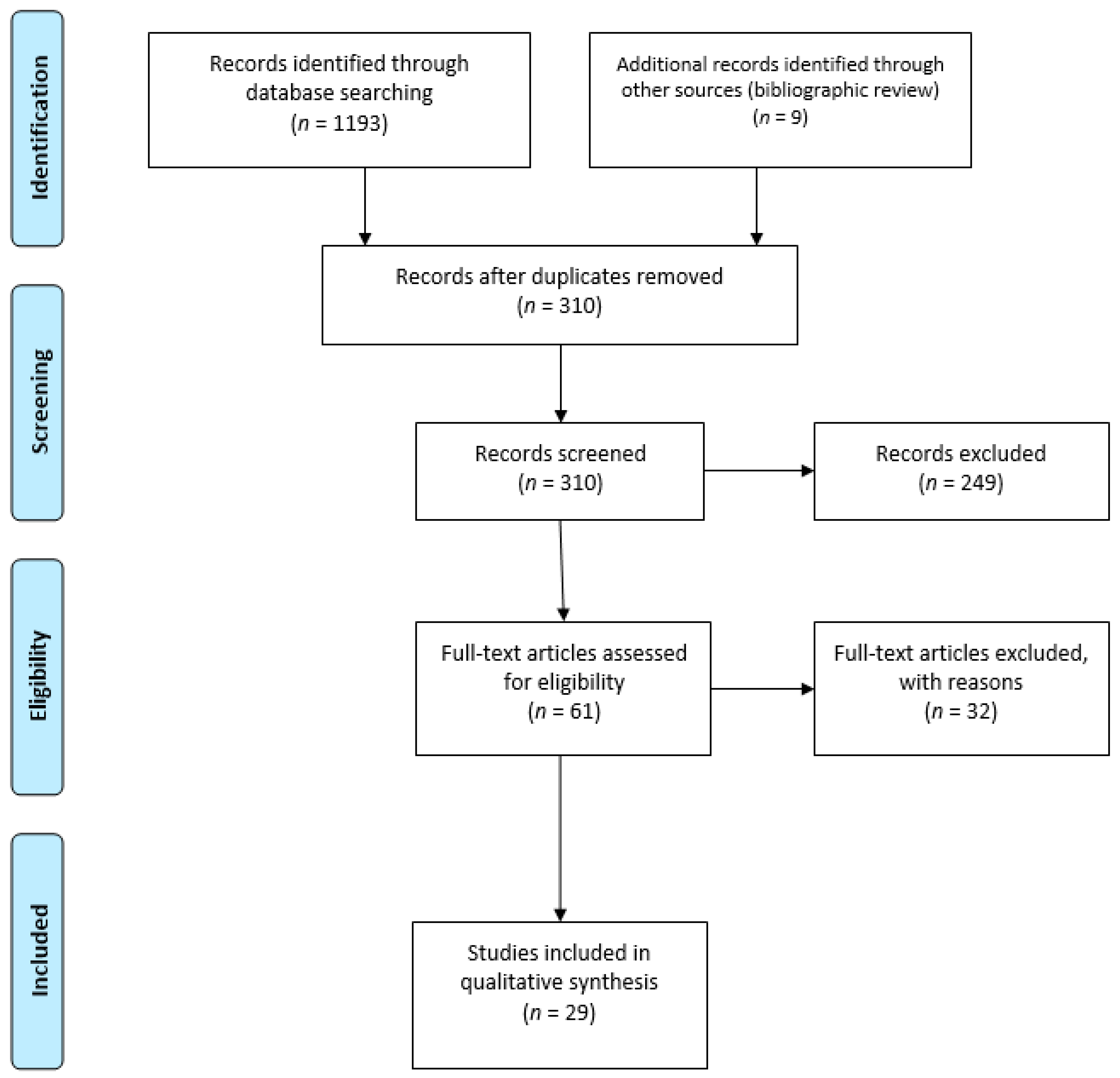
2. Methods
- Publication information (authors, publication date, journal in which the study was published);
- Known substances of in utero exposure (i.e., tobacco, antidepressants, selective serotonin reuptake inhibitors (SSRIs), antipsychotics, etc.) identified through self-report, urinalysis, or meconium testing;
- Outcomes that were measured (i.e., birth weight, birth length, length of stay, etc.);
- Study design (i.e., retrospective cohort study, clinical trial, etc.);
- Study population and group sample sizes;
- Reported outcome quantitative and qualitative data;
- Statistical measures utilized in the study;
3. Results
3.1. Methadone-Exposed Infants
3.2. Buprenorphine-Exposed Infants
3.3. Comparison of the Impact of Tobacco Consumption and Maternal Treatment with Either Methadone or Buprenorphine on Neonatal Outcomes
3.4. Polysubstance Exposure during Pregnancy
3.5. Prescription Opioid Use during Pregnancy
4. Discussion
4.1. Study Limitations
4.2. Recommendations for Tobacco Screening and Tobacco Cessation or Reduction for Women Who Are Pregnant with OUD
4.3. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Byatt, N.; Straus, J.; Stopa, A.; Biebel, K.; Mittal, L.; Moore Simas, T.A. Massachusetts Child Psychiatry Access Program for Moms. Obstet. Gynecol. 2018, 132, 345–353. [Google Scholar] [CrossRef]
- Center for Behavioral Health Statistics S. Results from the 2016 National Survey on Drug Use and Health: Detailed Tables Prevalence Estimates, Standard Errors, P Values, and Sample Sizes. 2017. Available online: https://www.samhsa.gov/data/sites/default/files/NSDUH-DetTabs-2016/NSDUH-DetTabs-2016.pdf (accessed on 15 August 2019).
- Kaltenbach, K.; Holbrook, A.M.; Coyle, M.G.; Heil, S.H.; Salisbury, A.L.; Stine, A.L.; Martin, P.R.; Jones, H.E. Predicting treatment for neonatal abstinence syndrome in infants born to women maintained on opioid agonist medication. Addiction 2012, 107, 45–52. [Google Scholar] [CrossRef] [Green Version]
- Jones, H.E.; Heil, S.H.; Tuten, M.; Chisolm, M.S.; Foster, J.M.; Grady, K.E.O.; Kaltenbach, K. Cigarette smoking in opioid-dependent pregnant women: Neonatal and maternal outcomes. Drug. Alcohol. Depend. 2013, 131, 271–277. [Google Scholar] [CrossRef] [Green Version]
- McLemore, G.L.; Lewis, T.; Jones, C.H.; Gauda, E.B. Novel pharmacotherapeutic strategies for treatment of opioid-induced neonatal abstinence syndrome. Semin. Fetal. Neonatal. Med. 2013, 18, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Gomez-Pomar, E.; Finnegan, L.P. The Epidemic of Neonatal Abstinence Syndrome, Historical References of Its’ Origins, Assessment, and Management. Front. Pediatr. 2018, 6, 33. [Google Scholar] [CrossRef] [Green Version]
- Aliyu, M.H.; Wilson, R.E.; Zoorob, R.; Brown, K.; Alio, A.P.; Clayton, H.; Salihu, H.M. Prenatal alcohol consumption and fetal growth restriction: Potentiation effect by concomitant smoking. Nicotine Tob. Res. 2009, 11, 36–43. [Google Scholar] [CrossRef]
- Mark, K.; Desai, A.; Terplan, M. Marijuana use and pregnancy: Prevalence, associated characteristics, and birth outcomes. Arch. Women’s Ment. Health 2016, 19, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Bailey, B.A.; McCook, J.G.; Hodge, A.; McGrady, L. Infant birth outcomes among substance using women: Why quitting smoking during pregnancy is just as important as quitting illicit drug use. Matern. Child Health J. 2012, 16, 414–422. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Alcohol Use in Pregnancy. Available online: https://www.cdc.gov/ncbddd/fasd/alcohol-use.html (accessed on 7 June 2018).
- Quesada, O.; Gotman, N.; Howell, H.B.; Funai, E.F.; Rounsaville, B.J.; Yonkers, K.A. Prenatal hazardous substance use and adverse birth outcomes. J. Matern. -Fetal Neonatal Med. 2012, 25, 1222–1227. [Google Scholar] [CrossRef] [PubMed]
- Warren, M.D.; Miller, A.M.; Traylor, J.; Bauer, A.; Patrick, S.W. Implementation of a statewide surveillance system for neonatal abstinence syndrome—Tennessee, 2013. Morb. Mortal. Wkly. Rep. 2015, 64, 125–128. [Google Scholar]
- Burstyn, I.; Kapur, N.; Cherry, N.M. Substance use of pregnant women and early neonatal morbidity: Where to focus intervention? Can. J. Public Health 2010, 101, 149–153. [Google Scholar] [CrossRef]
- Jones, H.E.; Heil, S.H.; O’Grady, K.E.; Martin, P.R.; Kaltenbach, K.; Coyle, M.G.; Stine, S.M.; Selby, P.; Arria, A.M.; Fischer, G. Smoking in pregnant women screened for an opioid agonist medication study compared to related pregnant and non-pregnant patient samples. Am. J. Drug Alcohol Abus. 2009, 35, 375–380. [Google Scholar] [CrossRef] [Green Version]
- Haug, N.A.; Stitzer, M.L.; Svikis, D.S. Smoking during pregnancy and intention to quit: A profile of methadone-maintained women. Nicotine Tob. Res. 2001, 3, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Polanska, K.; Jurewicz, J.; Hanke, W. Smoking and alcohol drinking during pregnancy as the risk factors for poor child neurodevelopment—A review of epidemiological studies. Int. J. Occup. Med. Environ. Health 2015, 28, 419–443. [Google Scholar] [CrossRef] [PubMed]
- Forray, A.; Foster, D. Substance use in the perinatal period. Curr. Psychiatry Rep. 2015, 17, 91. [Google Scholar] [CrossRef] [Green Version]
- Marynak, K.; VanFrank, B.; Tetlow, S.; Mahoney, M.; Phillips, E.; Jamal, A.; Schecter, A.; Tipperman, D.; Babb, S. Tobacco cessation interventions and smoke-free policies in mental health and substance abuse treatment facilities—United States, 2016. Morb. Mortal. Wkly. Rep. 2018, 67, 519–523. [Google Scholar] [CrossRef]
- Substance Abuse and Mental Health Services Administration. Buprenorphine. Available online: https://www.samhsa.gov/medication-assisted-treatment/medications-counseling-related-conditions/buprenorphine (accessed on 29 August 2021).
- Substance Abuse and Mental Health Services Administration. Methadone. Available online: https://www.samhsa.gov/medication-assisted-treatment/medications-counseling-related-conditions/methadone (accessed on 29 August 2021).
- Stroud, L.R.; Paster, R.L.; Papandonatos, G.D.; Niaura, R.; Salisbury, A.L.; Battle, C.; Lagasse, L.L.; Lester, B. Maternal smoking during pregnancy and newborn neurobehavior: Effects at 10 to 27 days. J. Pediatr. 2009, 154, 10–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Law, K.L.; Stroud, L.R.; LaGasse, L.L.; Niaura, R.; Liu, J.; Lester, B.M. Smoking during pregnancy and newborn neurobehavior. Pediatrics 2003, 111, 1318–1323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lester, B.M.; Tronick, E.Z. History and description of the Neonatal Intensive Care Unit Network Neurobehavioral Scale. Pediatrics 2004, 113, 634–640. [Google Scholar] [PubMed]
- Hurt, R.D.; Renner, C.C.; Patten, C.A.; Ebbert, J.O.; Offord, K.P.; Schroeder, D.R.; Enoch, C.C.; Gill, L.; Angstman, S.E.; Moyer, T.P. Iqmik—A form of smokeless tobacco used by pregnant Alaska natives: Nicotine exposure in their neonates. J. Matern. -Fetal Neonatal Med. 2005, 17, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Godding, V.; Bonnier, C.; Fiasse, L.; Michel, M.; Longueville, E.; Lebecque, P.; Robert, A.; Galanti, L. Does in utero exposure to heavy maternal smoking induce nicotine withdrawal symptoms in neonates? Pediatr. Res. 2004, 55, 645–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.J. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Baas, J.; Schotten, M.; Plume, A.; Côté, G.; Karimi, R. Scopus as a curated, high-quality bibliometric data source for academic research in quantitative science studies. Quant. Sci. Stud. 2020, 1, 1–10. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finnegan, L.; Kaltenbach, K. The assessment and management of Neonatal Abstinence Syndrome. In Primary Care, 3rd ed.; Friedman, S.B., Nelson, N., Seidel, H.M., Eds.; C.V. Mosby Company: St. Louis, MO, USA, 1992; pp. 1367–1378. [Google Scholar]
- Finnegan, L.P.; Connaughton, J.F.; Kron, R.E.; Emich, J.P. Neonatal abstinence syndrome: Assessment and management. Addict. Dis. 1975, 2, 141–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansson, L.M.; Velez, M.; Harrow, C. The opioid-exposed newborn: Assessment and pharmacologic management. J. Opioid. Manag. 2009, 5, 47–55. [Google Scholar] [CrossRef]
- Evidence-Based Recommendations–GRADE. Available online: www.cdc.gov (accessed on 15 August 2021).
- McMaster University. GRADE 2014; McMaster University: Hamilton, ON, Canada, 2013. [Google Scholar]
- Brożek, J.L.; Akl, E.A.; Alonso-Coello, P.; Lang, D.; Jaeschke, R.; Williams, J.W.; Phillips, B.; Lelgemann, M.; Lethaby, A.; Bousquet, J.; et al. Grading quality of evidence and strength of recommendations in clinical practice guidelines. Allergy 2009, 64, 669–677. [Google Scholar] [CrossRef]
- Burns, L.; Mattick, R.P. Using population data to examine the prevalence and correlates of neonatal abstinence syndrome. Drug Alcohol Rev. 2007, 26, 487–492. [Google Scholar] [CrossRef]
- Choo, R.E.; Huestis, M.A.; Schroeder, J.R.; Shin, A.S.; Jones, H.E. Neonatal abstinence syndrome in methadone-exposed infants is altered by level of prenatal tobacco exposure. Drug Alcohol Depend. 2004, 75, 253–260. [Google Scholar] [CrossRef]
- Seligman, N.S.; Almario, C.V.; Hayes, E.J.; Dysart, K.C.; Berghella, V.; Baxter, J.K. Relationship between maternal methadone dose at delivery and neonatal abstinence syndrome. J. Pediatr. 2010, 157, 428–433. [Google Scholar] [CrossRef] [Green Version]
- Ram, A.; Tuten, M.; Chisolm, M.S. Cigarette smoking reduction in pregnant women with opioid use disorder. J. Addict. Med. 2016, 10, 53–59. [Google Scholar] [CrossRef]
- Cleary, B.J.; Eogan, M.; O’Connell, M.P.; Fahey, T.; Gallagher, P.J.; Clarke, T.; White, M.J.; McDermott, C.; O’Sullivan, A.; Carmody, D.; et al. Methadone and perinatal outcomes: A prospective cohort study. Addiction 2012, 107, 1482–1492. [Google Scholar] [CrossRef]
- de Castro, A.; Jones, H.E.; Johnson, R.E.; Gray, T.R.; Shakleya, D.M.; Huestis, M.A. Methadone, cocaine, opiates, and metabolite disposition in umbilical cord and correlations to maternal methadone dose and neonatal outcomes. Ther. Drug Monit. 2011, 33, 443–452. [Google Scholar] [CrossRef]
- Jansson, L.M.; Dipietro, J.A.; Elko, A.; Velez, M. Maternal vagal tone change in response to methadone is associated with neonatal abstinence syndrome severity in exposed neonates. J. Matern. -Fetal Neonatal Med. 2007, 20, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Seligman, N.S.; Salva, N.; Hayes, E.J.; Dysart, K.C.; Pequignot, E.C.; Baxter, J.K. Predicting length of treatment for neonatal abstinence syndrome in methadone-exposed neonates. Am. J. Obstet. Gynecol. 2008, 199, 396–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velez, M.L.; Jansson, L.M.; Schroeder, J.; Williams, E.; Hopkins, J. Prenatal methadone exposure and neonatal neurobehavioral functioning. Pediatr. Res. 2009, 66, 704–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gray, T.R.; Choo, R.E.; Concheiro, M.; Williams, E.; Elko, A.; Jansson, L.M.; Jones, H.E.; Huestis, M.A. Prenatal methadone exposure, meconium biomarker concentrations and neonatal abstinence syndrome. Addiction 2010, 105, 2151–2159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansson, L.M.; DiPietro, J.A.; Elko, A.; Velez, M. Infant autonomic functioning and neonatal abstinence syndrome. Drug Alcohol Depend. 2010, 109, 198–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, A.; Alto, W.; Musgrave, K.; Gibbons, D.; Llanto, L.; Holden, S.; Karnes, J. Observational study of buprenorphine treatment of opioid-dependent pregnant women in a family medicine residency: Reports on maternal and infant outcomes. J. Am. Board Fam. Med. 2011, 24, 194–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, G.; Johnson, R.E.; Eder, H.; Jagsch, R.; Peternell, A.; Weninger, M.; Langer, M.; Aschauer, H.N. Treatment of opioid-dependent pregnant women with buprenorphine. Addiction 2000, 95, 239–244. [Google Scholar] [CrossRef]
- Kacinko, S.L.; Jones, H.E.; Johnson, R.E.; Choo, R.E.; Huestis, M.A. Correlations of maternal buprenorphine dose, buprenorphine, and metabolite concentrations in meconium with neonatal outcomes. Clin. Pharmacol. Ther. 2008, 84, 604–612. [Google Scholar] [CrossRef]
- Jansson, L.M.; Velez, M.L.; McConnell, K.; Spencer, N.; Tuten, M.; Jones, H.; Rios, R.; King, V.L.; Gandotra, N.; Millio, L.; et al. Maternal buprenorphine treatment and infant outcome. Drug Alcohol Depend. 2017, 180, 56–61. [Google Scholar] [CrossRef]
- Bakstad, B.; Sarfi, M.; Welle-Strand, G.K.; Ravndal, E. Opioid maintenance treatment during pregnancy: Occurrence and severity of neonatal abstinence syndrome. Eur. Addict. Res. 2009, 15, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Chisolm, M.S.; Acquavita, S.P.; Kaltenbach, K.; Winklbaur, B.; Heil, S.H.; Martin, P.R.; Stine, S.M.; Coyle, M.; Leoutsakos, J.S.; Tuten, M.; et al. Cigarette smoking and neonatal outcomes in depressed and non-depressed opioid-dependent agonist-maintained pregnant patients. Addict. Disord. Their Treat. 2011, 10, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Wachman, E.M.; Newby, P.K.; Vreeland, J.; Byun, J.; Bonzagni, A.; Bauchner, H.; Philipp, B.L. The relationship between maternal opioid agonists and psychiatric medications on length of hospitalization for neonatal abstinence syndrome. J. Addict. Med. 2011, 5, 293–299. [Google Scholar] [CrossRef]
- Gibson, K.S.; Stark, S.; Kumar, D.; Bailit, J.L. The relationship between gestational age and the severity of neonatal abstinence syndrome. Addiction 2017, 112, 711–716. [Google Scholar] [CrossRef] [PubMed]
- Fischer, G.; Ortner, R.; Rohrmeister, K.; Jagsch, R.; Baewert, A.; Langer, M.; Aschauer, H. Methadone versus buprenorphine in pregnant addicts: A double-blind, double-dummy comparison study. Addiction 2006, 101, 275–281. [Google Scholar] [CrossRef]
- Winklbaur, B.; Baewert, A.; Jagsch, R.; Rohrmeister, K.; Metz, V.; Jachmann, C.A.; Thau, K.; Fischer, G. Association between prenatal tobacco exposure and outcome of neonates born to opioid-maintained mothers. Implications for treatment. Eur. Addict. Res. 2009, 15, 150–156. [Google Scholar] [CrossRef]
- Tolia, V.N.; Murthy, K.; Bennett, M.M.; Miller, E.S.; Benjamin, D.K.; Smith, P.B.; Clark, R.H. Antenatal methadone vs buprenorphine exposure and length of hospital stay in infants admitted to the intensive care unit with neonatal abstinence syndrome. J. Perinatol. 2018, 38, 75–79. [Google Scholar] [CrossRef]
- O’Donnell, M.; Nassar, N.; Leonard, H.; Hagan, R.; Mathews, R.; Patterson, Y.; Stanley, F. Increasing prevalence of neonatal withdrawal syndrome: Population study of maternal factors and child protection involvement. Pediatrics 2009, 123, e614–e621. [Google Scholar] [CrossRef]
- Subedi, L.; Huang, H.; Pant, A.; Westgate, P.M.; Bada, H.S.; Bauer, J.A.; Giannone, P.J.; Sithisarn, T. Plasma brain-derived neurotrophic factor levels in newborn infants with neonatal abstinence syndrome. Front. Pediatr. 2017, 5, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patrick, S.W.; Dudley, J.; Martin, P.R.; Harrell, F.E.; Warren, M.E.; Hartmann, K.E.; Ely, E.W.; Grijalva, C.G.; Cooper, W.O. Prescription opioid epidemic and infant outcomes. Pediatrics 2015, 135, 842–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, R.J.; Huybrechts, K.F.; Hernandez-Diaz, S.; Mogun, H.; Patorno, E.; Kaltenbach, K.; Kerzner, L.S.; Bateman, B.T. Exposure to prescription opioid analgesics in utero and risk of neonatal abstinence syndrome: Population based cohort study. BMJ 2015, 350, h2102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shirel, T.; Hubler, C.P.; Shah, R.; Mager, A.B.; Koch, K.L.; Sheth, D.; Uhing, M.R.; Jones, C.W.; Field, J.J. Maternal opioid dose is associated with neonatal abstinence syndrome in children born to women with sickle cell disease. Am. J. Hematol. 2016, 91, 416–419. [Google Scholar] [CrossRef] [Green Version]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.-O. The Fagerstrom Test for Nicotine Dependence: A revision of the Fagerstrom Tolerance Questionnaire. Addiction 1991, 86, 1119–1127. [Google Scholar] [CrossRef]
- Substance Abuse and Mental Health Services Administration. Clinical Guidance for Treating Pregnant and Parenting Women with Opioid Use Disorder and Their Infants. Available online: https://store.samhsa.gov/product/Clinical-Guidance-for-Treating-Pregnant-and-Parenting-Women-With-Opioid-Use-Disorder-and-Their-Infants/SMA18- (accessed on 15 August 2020).
- World Health Organization. Management of Substance Abuse Team. Guidelines for the Identification and Management of Substance Use and Substance Use Disorders in Pregnancy. Available online: https://www.who.int/publications/i/item/97892415487312014 (accessed on 20 August 2020).
- ASAM National Practice Guideline for the Use of Medications in the Treatment of Addiction Involving Opioid Use. Available online: https://www.asam.org/docs/default-source/practice-support/guidelines-and-consensus-docs/asam-national-practice-guideline-supplement.pdf?sfvrsn=24 (accessed on 20 August 2018).
- Hostage, J.C.; Brock, J.; Craig, W.; Sepulveda, D. Integrating Screening, Brief Intervention and Referral to Treatment (SBIRT) for Substance Use into Prenatal Care. Matern. Child Health J. 2020, 24, 412–418. [Google Scholar] [CrossRef]
- Substance Abuse and Mental Health Services Administration. You Can Quit Tobacco Benefits and Tips for Quitting for Good If Your Last Smoke Was: 12 Hours Ago. Available online: https://www.who.int/news-room/q-a-detail/tobacco-health-benefits-of-smoking-cessation (accessed on 20 August 2020).
- Substance Abuse and Mental Health Services Administration HPNS-5069QT. Quitting Tobacco Help Your Clients to a Healthier Life Resources for Implementing Tobacco Cessation. Available online: https://store.samhsa.gov/product/Quitting-Tobacco/SMA18-5069QT (accessed on 20 August 2020).
- Substance Abuse and Mental Health Services—SAMHSA SMA18-5069QG. Implementing Tobacco Cessation Programs in Substance Use Disorder Treatment Settings. 2018. Available online: https://store.samhsa.gov/product/SMA18-5069QG (accessed on 20 August 2018).
- Akerman, S.C.; Brunette, M.F.; Green, A.I.; Goodman, D.J.; Blunt, H.B.; Heil, S.H. Treating tobacco use disorder in pregnant women in medication-assisted treatment for an opioid use disorder: A systematic review. J. Subst. Abuse Treat. 2015, 52, 40–47. [Google Scholar] [CrossRef] [Green Version]
- Haug, N.A.; Svikis, D.S.; DiClemente, C. Motivational enhancement therapy for nicotine dependence in methadone-maintained pregnant women. Psychol. Addict. Behav. 2004, 18, 289–292. [Google Scholar] [CrossRef] [PubMed]
- Holbrook, A.M.; Kaltenbach, K.A. Effectiveness of a smoking cessation intervention for methadone-maintained women: A comparison of pregnant and parenting women. Int. J. Pediatr. 2011, 2011, 1–6. [Google Scholar] [CrossRef]
- Tuten, M.; Svikis, D.S.; Keyser-Marcus, L.; O’Grady, K.E.; Jones, H.E. Lessons learned from a randomized trial of fixed and escalating contingency management schedules in opioid-dependent pregnant women. Am. J. Drug Alcohol Abuse. 2012, 38, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Fallin-Bennett, A.; Barnett, J.; Ducas, L.; Wiggins, A.T.; McCubbin, A.; Ashford, K. Pilot Tobacco Treatment Intervention for Women in Residential Treatment for Substance Use Disorder. J. Obstet. Gynecol. Neonatal Nurs. 2018, 47, 749–759. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.A.; Brown, A.L.; Baker, A.L.; Gould, G.S.; Dunlop, A.J. The Incentives to Quit tobacco in Pregnancy (IQuiP) protocol: Piloting a financial incentive-based smoking treatment for women attending substance use in pregnancy antenatal services. BMJ Open 2019, 9, e032330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faherty, L.J.; Matone, M.; Passarella, M.; Lorch, S. Mental Health of Mothers of Infants with Neonatal Abstinence Syndrome and Prenatal Opioid Exposure. Matern. Child Health J. 2018, 22, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Kranzler, H.R.; Washio, Y.; Zindel, L.R.; Lynch, K.G.; Hand, D.; Tyndale, R.F.; Oncken, C.; Schnoll, R. Pregnant smokers receiving opioid agonist therapy have an elevated nicotine metabolite ratio: A replication study. Nicotine Tob. Res. 2021, 22, 1923–1927. [Google Scholar] [CrossRef] [PubMed]
- Fallin-Bennett, A.; Ashford, K. Tailoring a NICU-Based Tobacco Treatment Program for Mothers Who Are Dependent on Opioids. J. Obstet. Gynecol. Neonatal Nurs. 2017, 46, 660–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Citation | Prenatal Opioid Exposure # | Study Design | Study Sample Size | Neonatal Outcomes Reported * | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| GAD | BL | BW | CPD | PFS | TX | LOS | LOT | ||||
| Buprenorphine Exposure | |||||||||||
| Fischer et al., 2000 | B | Clinical trial | 15 | x | x | x | x | x | x | ||
| Jansson et al., 2017 | B | Prospective cohort study | 41 | x | x | x | x | x | x | x | x |
| Kacinko et al., 2008 | B | Clinical trial | 10 | x | x | x | x | x | x | x | x |
| O’Connor et al., 2011 | B | Retrospective cohort study | 23 | x | x | ||||||
| Methadone Exposure | |||||||||||
| Burns and Mattick 2007 | M | Cross-sectional analysis | 2941 | x | x | ||||||
| Choo et al., 2004 | M | Clinical trial | 29 | x | x | x | x | x | |||
| Cleary et al., 2012 | M | Prospective cohort study | 114 | x | x | x | x | x | |||
| de Castro et al., 2011 | M | Secondary analysis of randomized clinical trial | 19 | x | x | ||||||
| Gray et al., 2010 | M | Prospective cohort study | 49 | x | x | x | x | x | x | x | |
| Jansson et al., 2007 | M | Prospective cohort study | 50 | x | x | x | x | x | x | x | |
| Jansson et al., 2010 | M | Prospective cohort study | 64 | x | x | x | |||||
| Ram, Tuten and Chisolm 2016 | M | Secondary analysis of randomized clinical trial | 118 | x | x | x | |||||
| Seligman et al., 2008 | M | Retrospective cohort study | 204 | x | x | ||||||
| Seligman et al., 2010 | M | Retrospective cohort study | 386 | x | x | ||||||
| Velez et al., 2009 | M | Prospective cohort study | 77 | x | x | x | x | x | x | ||
| Methadone OR Buprenorphine Exposure | |||||||||||
| Bakstad et al., 2009 | M/B | Prospective cohort study | 38 | x | x | x | x | x | x | x | |
| Chisolm et al., 2011 | M/B | Clinical trial (MOTHER) | 119 | x | x | x | x | ||||
| Fischer et al., 2006 | M/B | Clinical trial | 14 | x | x | x | x | x | |||
| Gibson et al., 2017 | M/B | Retrospective cohort study | 403 | x | x | x | |||||
| Jones et al., 2013 | M/B | Clinical trial (MOTHER) | 131 | x | x | x | x | x | |||
| Kaltenbach et al., 2012 | M/B | Clinical trial (MOTHER) | 131 | x | x | x | x | ||||
| Tolia et al., 2018 | M/B | Retrospective cohort study | 3364 | x | x | x | x | x | |||
| Wachman et al., 2011 | M/B | Retrospective cohort study | 273 | x | |||||||
| Winklbaur et al., 2009 | M/B | Clinical trial | 139 | x | x | x | x | x | x | ||
| Polypharmacy Exposure | |||||||||||
| O’Donnell et al., 2009 | Poly | Retrospective cohort study | 637,195 | x | x | x | |||||
| Subedi et al., 2017 | Poly | Prospective cohort study | 67 | x | x | x | x | x | |||
| Prescription Opioid Exposure | |||||||||||
| Desai et al., 2015 | RX | Retrospective cohort study | 1,379,450 | x | x | ||||||
| Patrick et al., 2015 | RX | Retrospective cohort study | 112,029 | x | x | x | |||||
| Shirel et al., 2016 | RX | Retrospective cohort study | 34 | x | x | x | x | ||||
| Basic Clinical Issues |
|---|
| Is there a differential influence of prenatal tobacco exposure on methadone- vs. buprenorphine-exposed neonatal outcomes? |
| What is the combined effect of prenatal nicotine and opioid exposure on the likelihood of sudden infant death syndrome? |
| If reduction is an attainable goal, what should be the maximum number of CPD? Would this number of CPD differ between women in treatment with methadone or buprenorphine? Note, whether the woman is encouraged to quit or reduce will largely depend on the CPD that the woman is smoking and the time in pregnancy when she comes to treatment. More CPD and later arrival to treatment will not permit a large decrease in CPD. |
| What would be quantitative differences in biochemical results of prenatal tobacco exposure by the status and type of opioid agonist therapy? |
| Is there an interaction between maternal depression, nicotine consumption, and NAS expression? Is there an interaction between medication for depression, nicotine consumption, and NAS expression? |
| What are the influences of combustible vs. smokeless tobacco, vapor or e-cigarettes, or nicotine replacement products on methadone- vs. buprenorphine-exposed neonatal outcomes? |
| Is there a difference in nicotine metabolite ratios between methadone- vs. buprenorphine-treated women who are pregnant and smokers? |
| Treatment Issues |
| What are the best treatment options (pharmacological and/or psychosocial) to treat prenatal smoking for women in treatment programs for OUD? What kind of interaction effect with methadone or buprenorphine treatment should be expected if pharmacotherapy was applied to treat prenatal nicotine use and birth outcomes? |
| Ideally, pre-conception would be an optimal time to start nicotine cessation to minimize fetal exposure. What is the optimal time to start a nicotine cessation program for a woman in treatment for OUD—at the induction onto methadone or buprenorphine? One or two months later? Pre-pregnancy? During pregnancy? Or early postpartum? |
| Implementation Issues |
| What are the critical components for an organization to adopt a prenatal nicotine cessation program? |
| What are the barriers and facilitators to implementing a nicotine cessation treatment program for women with OUD? |
| What is the cost-effectiveness in implementing and sustaining a nicotine cessation treatment program for women with OUD? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isaacs, K.R.; Atreyapurapu, S.; Alyusuf, A.H.; Ledgerwood, D.M.; Finnegan, L.P.; Chang, K.H.K.; Ma, T.X.; Washio, Y. Neonatal Outcomes after Combined Opioid and Nicotine Exposure in Utero: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 10215. https://doi.org/10.3390/ijerph181910215
Isaacs KR, Atreyapurapu S, Alyusuf AH, Ledgerwood DM, Finnegan LP, Chang KHK, Ma TX, Washio Y. Neonatal Outcomes after Combined Opioid and Nicotine Exposure in Utero: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(19):10215. https://doi.org/10.3390/ijerph181910215
Chicago/Turabian StyleIsaacs, Krystyna R., Sravanthi Atreyapurapu, Amal H. Alyusuf, David M. Ledgerwood, Loretta P. Finnegan, Katie H. K. Chang, Tony X. Ma, and Yukiko Washio. 2021. "Neonatal Outcomes after Combined Opioid and Nicotine Exposure in Utero: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 19: 10215. https://doi.org/10.3390/ijerph181910215