
The Effect of High-Density Built Environments on Elderly Individuals’ Physical Health: A Cross-Sectional Study in Guangzhou, China


Abstract
:1. Introduction
2. Literature Review
3. Data Sources and Methods
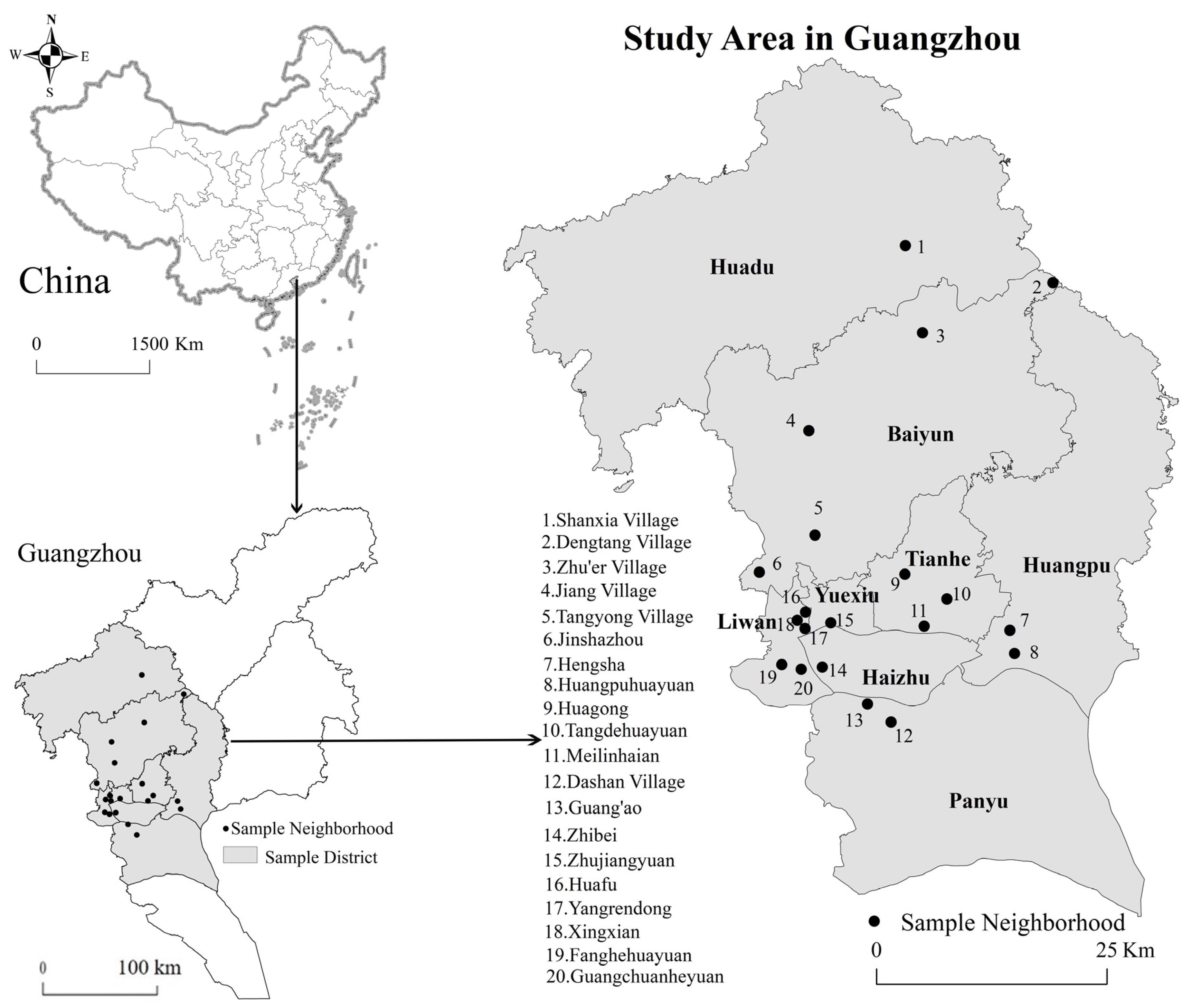
3.1. Data Sources
3.2. Variables and Measurement
3.2.1. Dependent Variables
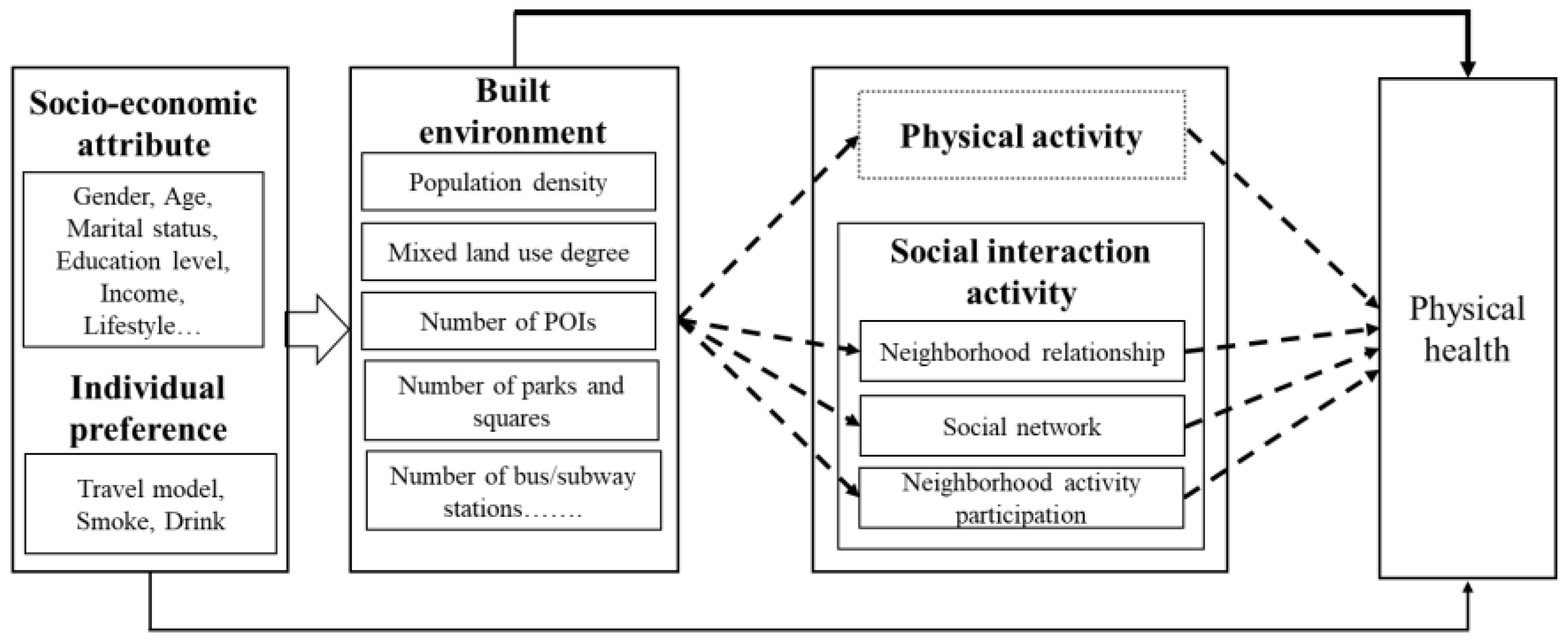
3.2.2. Independent Variables
- (i)
- Population density: Population density is defined by population divided by the sub-district area.
- (ii)
- Land use mix: The concept of information entropy is introduced to calculate the land use mix. This principle was originally applied as a method to measure energy conservation in physics [101,102]. According to the principle of thermodynamic conservation, more intense interaction between molecules means a higher entropy of the system. The model was designed as follows:where H(x) is the entropy of neighborhood x; Pi is the probability of the appearance of different types of POIs within the 1 km buffer based on a participant’s neighborhood committee location. Obviously, the higher the entropy, the higher the land use mix.
- (iii)
- Accessibility: We used the number of public facilities within the 1 km buffer as the proxy for accessibility, including the number of POIs, the number of parks and squares, and the number of bus and subway stations.
- (iv)
- Distance to the destination: We used the distance to the nearest public facilities within the 1 km buffer as the proxy for distance to the destination, including distance to the nearest bus or subway station and distance to the nearest park or square.
3.2.3. Control Variables
3.2.4. Mediating Variable
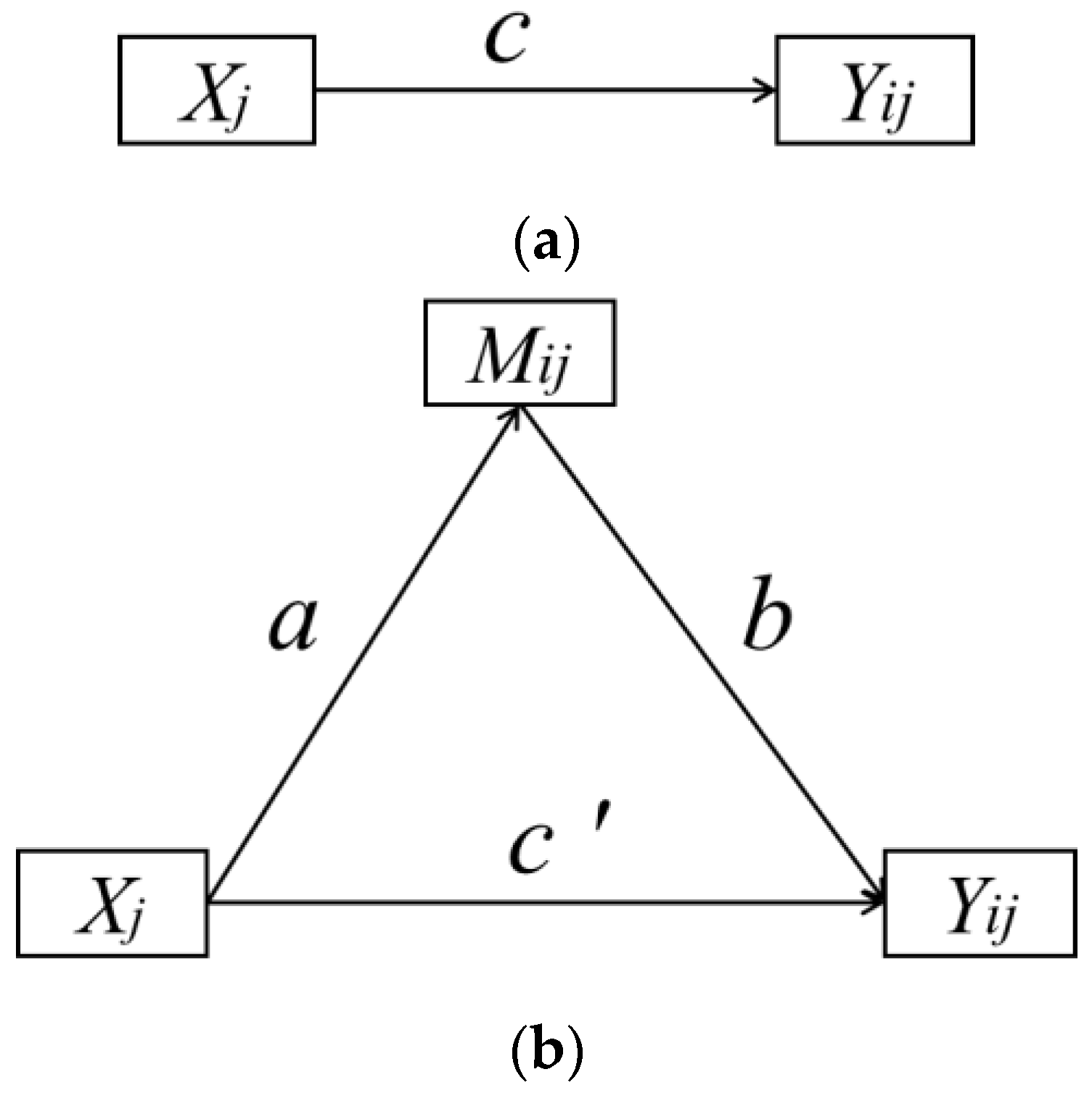
3.3. Method
4. Results
4.1. Descriptive Statistical Analysis of Samples
4.2. Relationship between Built Environment and Elderly Individuals’ Physical Health
4.3. Relationship between Built Environment and Possible Mediators
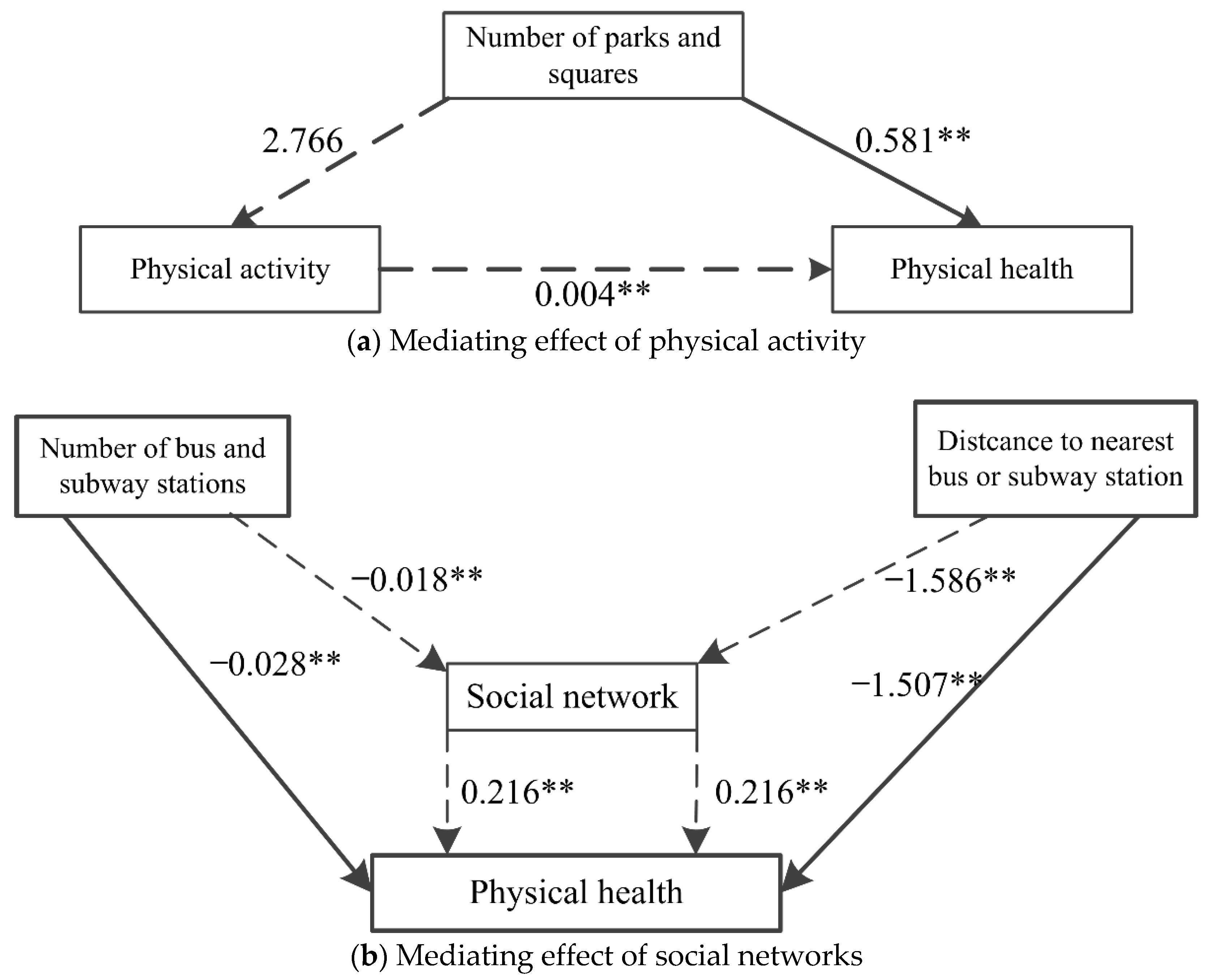
4.4. Relationship between Built Environment, Mediators, and Elderly Individuals’ Physical Health
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Measurement Scales
- (i)
- How do you feel about your health?
- (ii)
- Are there restrictions on activities with a large amount of exercise?
- (iii)
- Have you had physical pain in the past 4 weeks (such as headache, chest tightness, nausea, etc.)?
- (i)
- Do you think the relationships in the neighborhood are harmonious?
- (ii)
- Do you know many people in the neighborhood?
- (iii)
- Do you often participate in neighborhood or park activities?
References
- Huang, N.C.; Chu, C.; Kung, S.F.; Hu, S.C. Association of the built environments and health-related quality of life in community-dwelling older adults: A cross-sectional study. Qual. Life Res. 2019, 28, 2393–2407. [Google Scholar] [CrossRef]
- Zhou, Y.; Yuan, Y.; Chen, Y.; Lai, S. Association Pathways Between Neighborhood Greenspaces and the Physical and Mental Health of Older Adults-A Cross-Sectional Study in Guangzhou, China. Front. Public Health 2020, 8, 551453. [Google Scholar] [CrossRef]
- Li, C.; Zhou, Y. Residential environment and depressive symptoms among Chinese middle- and old-aged adults: A longitudinal population-based study. Health Place 2020, 66, 102463. [Google Scholar] [CrossRef]
- Wang, R.; Liu, Y.; Lu, Y.; Zhang, J.; Liu, P.; Yao, Y.; Grekousis, G. Perceptions of built environment and health outcomes for older Chinese in Beijing: A big data approach with street view images and deep learning technique. Comput. Environ. Urban Syst. 2019, 78, 101386. [Google Scholar] [CrossRef]
- National Bureau of Statistics of China. Statistical Communiqu’e of the People’s Republic of China on the 2019 National Economic and Social Development. 2014. Available online: http://www.stats.gov.cn/english/PressRelease/202002/t20200228_1728917.html (accessed on 15 September 2021).
- Fang, E.F.; Scheibye-Knudsen, M.; Jahn, H.J.; Li, J.; Ling, L.; Guo, H.; Zhu, X.; Preedy, V.; Lu, H.; Bohr, V.A.; et al. A research agenda for aging in China in the 21st century. Ageing Res. Rev. 2015, 24, 197–205. [Google Scholar] [CrossRef] [Green Version]
- US Census Bureau. State and County QuickFacts. Available online: http://www.census.gov/programs-surveys/sis/resources/data-tools/quickfacts.html (accessed on 15 September 2021).
- United Nations Publications Department of Economic and Social Affairs, Population Division. 2019 Revision of World Population Prospects; United Nations: New York, NY, USA, 2019. [Google Scholar]
- WHO. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar] [CrossRef]
- WHO. Social Development and Ageing: Crisis or Opportunity? World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- United Nations Publications. World Urbanization Prospects; United Nations: New York, NY, USA, 2014. [Google Scholar]
- Noreau, L.; Boschen, K. Intersection of Participation and Environmental Factors: A Complex Interactive Process. Arch. Phys. Med. Rehabil. 2010, 91, S44–S53. [Google Scholar] [CrossRef]
- Bonaccorsi, G.; Manzi, F.; Del Riccio, M.; Setola, N.; Naldi, E.; Milani, C.; Giorgetti, D.; Dellisanti, C.; Lorini, C. Impact of the Built Environment and the Neighborhood in Promoting the Physical Activity and the Healthy Aging in Older People: An Umbrella Review. Int. J. Environ. Res. Public Health 2020, 17, 6127. [Google Scholar] [CrossRef] [PubMed]
- Namgung, M.; Gonzalez, B.E.M.; Park, S. The Role of Built Environment on Health of Older Adults in Korea: Obesity and Gender Differences. Int. J. Environ. Res. Public Health 2019, 16, 3486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Putrik, P.; van Amelsvoort, L.; De Vries, N.K.; Mujakovic, S.; Kunst, A.E.; van Oers, H.; Jansen, M.; Kant, I. Neighborhood Environment is Associated with Overweight and Obesity, Particularly in Older Residents: Results from Cross-Sectional Study in Dutch Municipality. J. Urban Health 2015, 92, 1038–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, S.C.; Mason, C.A.; Lombard, J.L.; Martinez, F.; Plater-Zyberk, E.; Spokane, A.R.; Newman, F.L.; Pantin, H.; Szapocznik, J. The relationship of built environment to perceived social support and psychological distress in Hispanic elders: The role of “eyes on the street”. J. Gerontol. B Psychol. Sci. Soc. Sci. 2009, 64, 234–246. [Google Scholar] [CrossRef]
- Pan, H.; Liu, Y.; Chen, Y. The health effect of perceived built environment on depression of elderly people in rural China: Moderation by income. Health Soc. Care Community 2021, 29, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Clarke, P.; Nieuwenhuijsen, E.R. Environments for healthy ageing: A critical review. Maturitas 2009, 64, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Jeon, C.Y.; Lokken, R.P.; Hu, F.B.; van Dam, R.M. Physical activity of moderate intensity and risk of type 2 diabetes: A systematic review. Diabetes Care 2007, 30, 744–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, E.S.; Zhao, G.; Tsai, J.; Li, C. Low-Risk Lifestyle Behaviors and All-Cause Mortality: Findings from the National Health and Nutrition Examination Survey III Mortality Study. Am. J. Public Health 2011, 101, 1922–1929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rummo, P.E.; Meyer, K.A.; Green Howard, A.; Shikany, J.M.; Guilkey, D.K.; Gordon-Larsen, P. Fast food price, diet behavior, and cardiometabolic health: Differential associations by neighborhood SES and neighborhood fast food restaurant availability in the CARDIA study. Health Place 2015, 35, 128–135. [Google Scholar] [CrossRef] [Green Version]
- Helbich, M. Toward dynamic urban environmental exposure assessments in mental health research. Environ. Res. 2018, 161, 129–135. [Google Scholar] [CrossRef]
- Saelens, B.E.; Handy, S.L. Built environment correlates of walking: A review. Med. Sci. Sports Exerc. 2008, 40, S550–S566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nations, U. Revision of World Urbanization Prospects; United Nations: New York, NY, USA, 2018. [Google Scholar]
- White, M.P.; Alcock, I.; Grellier, J.; Wheeler, B.W.; Hartig, T.; Warber, S.L.; Bone, A.; Depledge, M.H.; Fleming, L.E. Spending at least 120 min a week in nature is associated with good health and wellbeing. Sci. Rep. 2019, 9, 7730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beemer, C.J.; Stearns-Yoder, K.A.; Schuldt, S.J.; Kinney, K.A.; Lowry, C.A.; Postolache, T.T.; Brenner, L.A.; Hoisington, A.J. A brief review on the mental health for select elements of the built environment. Indoor Built Environ. 2019, 30, 152–165. [Google Scholar] [CrossRef]
- Frank, L.D.; Iroz-Elardo, N.; MacLeod, K.E.; Hong, A. Pathways from built environment to health: A conceptual framework linking behavior and exposure-based impacts. J. Transp. Health 2019, 12, 319–335. [Google Scholar] [CrossRef]
- Li, X.; Zhang, W. The impacts of health insurance on health care utilization among the older people in China. Soc. Sci. Med. 2013, 85, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Wiles, J.L.; Leibing, A.; Guberman, N.; Reeve, J.; Allen, R.E.S. The Meaning of “Aging in Place” to Older People. Gerontologist 2012, 52, 357–366. [Google Scholar] [CrossRef]
- Garin, N.; Olaya, B.; Miret, M.; Ayuso-Mateos, J.L.; Power, M.; Bucciarelli, P.; Haro, J.M. Built environment and elderly population health: A comprehensive literature review. Clin. Pract. Epidemiol. Ment. Health 2014, 10, 103–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levinger, P.; Sales, M.; Polman, R.; Haines, T.; Dow, B.; Biddle, S.J.H.; Duque, G.; Hill, K.D. Outdoor physical activity for older people—The senior exercise park: Current research, challenges and future directions. Health Promot. J. Aust. 2018, 29, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Asiamah, N.; Kouveliotis, K.; Petersen, C.; Eduafo, R. The association between social capital factors and sedentary behaviour among older adults: Does the built environment matter? Adv. Gerontol. 2019, 32, 234–242. [Google Scholar] [PubMed]
- Chen, Y.; Yuan, Y. The neighborhood effect of exposure to blue space on elderly individuals’ mental health: A case study in Guangzhou, China. Health Place 2020, 63, 102348. [Google Scholar] [CrossRef]
- Roux, A.V.D. Investigating neighborhood and area effects on health. Am. J. Public Health 2001, 91, 1783–1789. [Google Scholar] [CrossRef]
- Rydin, Y.; Bleahu, A.; Davies, M.; Dávila, J.D.; Friel, S.; De Grandis, G.; Groce, N.; Hallal, P.C.; Hamilton, I.; Howden-Chapman, P.; et al. Shaping cities for health: Complexity and the planning of urban environments in the 21st century. Lancet 2012, 379, 2079–2108. [Google Scholar] [CrossRef] [Green Version]
- Andreucci, M.B.; Russo, A.; Olszewska-Guizzo, A. Designing Urban Green Blue Infrastructure for Mental Health and Elderly Wellbeing. Sustainability 2019, 11, 6425. [Google Scholar] [CrossRef] [Green Version]
- Forjuoh, S.N.; Ory, M.G.; Won, J.; Towne, S.D., Jr.; Wang, S.; Lee, C. Determinants of Walking among Middle-Aged and Older Overweight and Obese Adults: Sociodemographic, Health, and Built Environmental Factors. J. Obes. 2017, 2017, 9565430. [Google Scholar] [CrossRef] [Green Version]
- Kerr, J.; Rosenberg, D.; Frank, L. The Role of the Built Environment in Healthy Aging: Community Design, Physical Activity, and Health among Older Adults. J. Plan. Lit. 2012, 27, 43–60. [Google Scholar] [CrossRef]
- Melis, G.; Gelormino, E.; Marra, G.; Ferracin, E.; Costa, G. The Effects of the Urban Built Environment on Mental Health: A Cohort Study in a Large Northern Italian City. Int. J. Environ. Res. Public Health 2015, 12, 14898–14915. [Google Scholar] [CrossRef] [PubMed]
- Clarke, P.J.; Ailshire, J.A.; Nieuwenhuijsen, E.R.; de Kleijn-de Vrankrijker, M.W. Participation among adults with disability: The role of the urban environment. Soc. Sci. Med. 2011, 72, 1674–1684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Cauwenberg, J.; Van Holle, V.; De Bourdeaudhuij, I.; Van Dyck, D.; Deforche, B. Neighborhood walkability and health outcomes among older adults: The mediating role of physical activity. Health Place 2016, 37, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Frank, L.; Kerr, J.; Rosenberg, D.; King, A. Healthy Aging and Where You Live: Community Design Relationships with Physical Activity and Body Weight in Older Americans. J. Phys. Act. Health 2010, 7, S82–S90. [Google Scholar] [CrossRef]
- King, A.C.; Sallis, J.F.; Frank, L.D.; Saelens, B.E.; Cain, K.; Conway, T.L.; Chapman, J.E.; Ahn, D.K.; Kerr, J. Aging in neighborhoods differing in walkability and income: Associations with physical activity and obesity in older adults. Soc. Sci. Med. 2011, 73, 1525–1533. [Google Scholar] [CrossRef] [Green Version]
- Koohsari, M.J.; McCormack, G.R.; Nakaya, T.; Shibata, A.; Ishii, K.; Yasunaga, A.; Hanibuchi, T.; Oka, K. Urban design and Japanese older adults’ depressive symptoms. Cities 2019, 87, 166–173. [Google Scholar] [CrossRef]
- Sun, B.; Yin, C. Relationship between multi-scale urban built environments and body mass index: A study of China. Appl. Geogr. 2018, 94, 230–240. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, R.; Grekousis, G.; Liu, Y.; Yuan, Y.; Li, Z. Neighbourhood greenness and mental wellbeing in Guangzhou, China: What are the pathways? Landsc. Urban Plan. 2019, 190, 103602. [Google Scholar] [CrossRef]
- Sun, B.; Yan, H.; Zhang, T. Built environmental impacts on individual mode choice and BMI: Evidence from China. J. Transp. Geogr. 2017, 63, 11–21. [Google Scholar] [CrossRef]
- Kenworthy, J.; Hu, G. Transport and Urban Form in Chinese Cities: An International Comparative and Policy Perspective with Implications for Sustainable Urban Transport in China. Disp Plan. Rev. 2002, 38, 4–14. [Google Scholar] [CrossRef]
- Gao, Y.; Kenworthy, J. The Urban Transport Crisis in Emerging Economies; Springer: Cham, Switzerland, 2017; pp. 33–58. [Google Scholar] [CrossRef]
- Dong, H.; Qin, B. Exploring the link between neighborhood environment and mental wellbeing: A case study in Beijing, China. Landsc. Urban Plan. 2017, 164, 71–80. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. Toward an Experimental Ecology of Human Development. Am. Psychol. 1977, 32, 513–531. [Google Scholar] [CrossRef]
- Sallis, J.F.; Owen, N.; Fisher, E.B. Ecological models of health behavior. In Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 465–485. [Google Scholar]
- Cervero, R.; Kockelman, K. Travel demand and the 3Ds: Density, diversity, and design. Transp. Res. Part D Transp. Environ. 1997, 2, 199–219. [Google Scholar] [CrossRef]
- Ewing, R.; Cervero, R. Travel and the Built Environment. J. Am. Plan. Assoc. 2010, 76, 265–294. [Google Scholar] [CrossRef]
- Lopez, R.P. Neighborhood risk factors for obesity. Obesity 2007, 15, 2111–2119. [Google Scholar] [CrossRef]
- Rundle, A.; Roux, A.V.D.; Freeman, L.M.; Miller, D.; Neckerman, K.M.; Weiss, C.C. The Urban Built Environment and Obesity in New York City: A Multilevel Analysis. Am. J. Health Promot. 2007, 21, 326–334. [Google Scholar] [CrossRef]
- Frank, L.D.; Andresen, M.A.; Schmid, T.L. Obesity relationships with community design, physical activity, and time spent in cars. Am. J. Prev. Med. 2004, 27, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Mobley, L.R.; Root, E.D.; Finkelstein, E.A.; Khavjou, O.; Farris, R.P.; Will, J.C. Environment, obesity, and cardiovascular disease risk in low-income women. Am. J. Prev. Med. 2006, 30, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Pearson, A.L.; Bentham, G.; Day, P.; Kingham, S. Associations between neighbourhood environmental characteristics and obesity and related behaviours among adult New Zealanders. BMC Public Health 2014, 14, 553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, G.; Christian, H.; Foster, S.; Boruff, B.J.; Bull, F.; Knuiman, M.; Giles-Corti, B. The association between neighborhood greenness and weight status: An observational study in Perth Western Australia. Environ. Health 2013, 12, 49. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, J.M.; Stokes, R.J.; Cohen, D.A.; Kofner, A.; Ridgeway, G.K. The effect of light rail transit on body mass index and physical activity. Am. J. Prev. Med. 2010, 39, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Creatore, M.I.; Glazier, R.H.; Moineddin, R.; Fazli, G.S.; Johns, A.; Gozdyra, P.; Matheson, F.I.; Kaufman-Shriqui, V.; Rosella, L.C.; Manuel, D.G.; et al. Association of Neighborhood Walkability with Change in Overweight, Obesity, and Diabetes. JAMA 2016, 315, 2211–2220. [Google Scholar] [CrossRef] [Green Version]
- Wasfi, R.A.; Dasgupta, K.; Orpana, H.; Ross, N.A. Neighborhood Walkability and Body Mass Index Trajectories: Longitudinal Study of Canadians. Am. J. Public Health 2016, 106, 934–940. [Google Scholar] [CrossRef]
- Yen, I.H.; Michael, Y.L.; Perdue, L. Neighborhood environment in studies of health of older adults: A systematic review. Am. J. Prev. Med. 2009, 37, 455–463. [Google Scholar] [CrossRef] [Green Version]
- Michael, Y.L.; Nagel, C.L.; Gold, R.; Hillier, T.A. Does change in the neighborhood environment prevent obesity in older women? Soc. Sci. Med. 2014, 102, 129–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, S.; Yap, W.; Hou, Y.; Yuen, B. Neighbourhood built Environment, physical activity, and physical health among older adults in Singapore: A simultaneous equations approach. J. Transp. Health 2020, 18, 100881. [Google Scholar] [CrossRef]
- Ewing, R.; Meakins, G.; Hamidi, S.; Nelson, A.C. Relationship between urban sprawl and physical activity, obesity, and morbidity-update and refinement. Health Place 2014, 26, 118–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. Fact Sheet for health professionals on physical activity guidelines for adults. In Centers for Disease Control and Prevention, Division of Nutrition, Physical Activity, and Obesity; Centers for Disease Control and Prevention, Ed.; Available online: https://www.cdc.gov/physicalactivity/resources/factsheets.html (accessed on 5 July 2021).
- Saelens, B.E.; Sallis, J.F.; Black, J.B.; Chen, D. Neighborhood-Based Differences in Physical Activity: An Environment Scale Evaluation. Am. J. Public Health 2003, 93, 1552–1558. [Google Scholar] [CrossRef] [PubMed]
- Ngo, V.; Frank, L.; Bigazzi, A. Effects of new urban greenways on transportation energy use and greenhouse gas emissions: A longitudinal study from Vancouver, Canada. Transp. Res. Part D Transp. Environ. 2018, 62, 715–725. [Google Scholar] [CrossRef]
- Colchero, M.A.; Caballero, B.; Bishai, D. The effect of income and occupation on body mass index among women in the Cebu Longitudinal Health and Nutrition Surveys (1983–2002). Soc. Sci. Med. 2008, 66, 1967–1978. [Google Scholar] [CrossRef]
- Gascon, M.; Triguero-Mas, M.; Martinez, D.; Dadvand, P.; Rojas-Rueda, D.; Plasencia, A.; Nieuwenhuijsen, M.J. Residential green spaces and mortality: A systematic review. Environ. Int. 2016, 86, 60–67. [Google Scholar] [CrossRef] [Green Version]
- Diez Roux, A.V.; Evenson, K.R.; McGinn, A.P.; Brown, D.G.; Moore, L.; Brines, S.; Jacobs, D.R., Jr. Availability of recreational resources and physical activity in adults. Am. J. Public Health 2007, 97, 493–499. [Google Scholar] [CrossRef]
- Wendel-Vos, G.W.; Schuit, A.J.; Tijhuis, M.A.R.; Kromhout, D. Leisure time physical activity and health-related quality of life: Cross-sectional and longitudinal associations. Qual. Life Res. 2004, 13, 667–677. [Google Scholar] [CrossRef]
- Brown, B.B.; Werner, C.M.; Smith, K.R.; Tribby, C.P.; Miller, H.J. Physical activity mediates the relationship between perceived crime safety and obesity. Prev. Med. 2014, 66, 140–144. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Yang, D. Exploring the Impact of the Built Environment on Outdoor Recreational Activities of the Elderly in the Neighborhood A Comparative Study of Four Typical Neighborhoods in Dalian. J. Archit. 2016, 6, 25–29. [Google Scholar]
- Balfour, J.L.; Kaplan, G.A. Neighborhood environment and loss of physical function in older adults: Evidence from the alameda county study. Am. J. Epidemiol. 2002, 155, 507–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parra, D.C.; Gomez, L.F.; Fleischer, N.L.; David Pinzon, J. Built environment characteristics and perceived active park use among older adults: Results from a multilevel study in Bogota. Health Place 2010, 16, 1174–1181. [Google Scholar] [CrossRef] [PubMed]
- Berkman, L.F.; Kawachi, I. Social Epidemiology; Oxford University Press: New York, NY, USA, 2000. [Google Scholar]
- Pearce, S.; Kristjansson, E. Perceptions of the Physical and Social Neighbourhood Environment and Youth Volunteerism: Canadas Capital Region. Can. J. Nonprofit Soc. Econ. Res./Rev. Can. Rech. Sur Les OSBL l’économie Soc. 2009, 10, 41–60. [Google Scholar]
- Leyden, K.M. Social capital and the built environment: The importance of walkable neighborhoods. Am. J. Public Health 2003, 93, 1546–1551. [Google Scholar] [CrossRef] [PubMed]
- Coan, J.A.; Sbarra, D.A. Social Baseline Theory: The social regulation of risk and effort. Curr. Opin. Psychol. 2015, 1, 87–91. [Google Scholar] [CrossRef] [Green Version]
- Holt-Lunstad, J. Why Social Relationships Are Important for Physical Health: A Systems Approach to Understanding and Modifying Risk and Protection. Annu. Rev. Psychol. 2018, 69, 437–458. [Google Scholar] [CrossRef]
- Hirsch, J.A.; Diez Roux, A.V.; Rodriguez, D.A.; Brines, S.J.; Moore, K.A. Discrete land uses and transportation walking in two U.S. cities: The Multi-Ethnic Study of Atherosclerosis. Health Place 2013, 24, 196–202. [Google Scholar] [CrossRef] [Green Version]
- Diez Roux, A.V.; Mujahid, M.S.; Hirsch, J.A.; Moore, K.; Moore, L.V. The Impact of Neighborhoods on CV Risk. Glob. Heart 2016, 11, 353–363. [Google Scholar] [CrossRef] [Green Version]
- Cao, X. How does neighborhood design affect life satisfaction? Evidence from Twin Cities. Travel Behav. Soc. 2016, 5, 68–76. [Google Scholar] [CrossRef]
- Sallis, J.F.; Cerin, E.; Conway, T.L.; Adams, M.A.; Frank, L.D.; Pratt, M.; Salvo, D.; Schipperijn, J.; Smith, G.; Cain, K.L.; et al. Physical activity in relation to urban environments in 14 cities worldwide: A cross-sectional study. Lancet 2016, 387, 2207–2217. [Google Scholar] [CrossRef] [Green Version]
- Kim, H. Walking distance, route choice, and activities while walking: A record of following pedestrians from transit stations in the San Francisco Bay area. Urban Des. Int. 2015, 20, 144–157. [Google Scholar] [CrossRef]
- Ermagun, A.; Levinson, D.M. “Transit makes you short”: On health impact assessment of transportation and the built environment. J. Transp. Health 2017, 4, 373–387. [Google Scholar] [CrossRef]
- Cabrera, J.F.; Najarian, J.C. How the Built Environment Shapes Spatial Bridging Ties and Social Capital. Environ. Behav. 2013, 47, 239–267. [Google Scholar] [CrossRef]
- Beard, J.R.; Blaney, S.; Cerda, M.; Frye, V.; Lovasi, G.S.; Ompad, D.; Rundle, A.; Vlahov, D. Neighborhood characteristics and disability in older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2009, 64, 252–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemperman, A.; Timmermans, H. Green spaces in the direct living environment and social contacts of the aging population. Landsc. Urban Plan. 2014, 129, 44–54. [Google Scholar] [CrossRef]
- Kweon, B.-S.; Sullivan, W.C.; Wiley, A.R. Green Common Spaces and the Social Integration of Inner-City Older Adults. Environ. Behav. 1998, 30, 832–858. [Google Scholar] [CrossRef]
- He, X.; Yuan, X.; Zhang, D.; Zhang, R.; Li, M.; Zhou, C. Delineation of Urban Agglomeration Boundary Based on Multisource Big Data Fusion—A Case Study of Guangdong–Hong Kong–Macao Greater Bay Area (GBA). Remote Sens. 2021, 13, 1801. [Google Scholar]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zhou, S.; Kwan, M.P. A comparative analysis of the impacts of objective versus subjective neighborhood environment on physical, mental, and social health. Health Place 2019, 59, 102170. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, R.; Xiao, Y.; Huang, B.; Chen, H.; Li, Z. Exploring the linkage between greenness exposure and depression among Chinese people: Mediating roles of physical activity, stress and social cohesion and moderating role of urbanicity. Health Place 2019, 58, 102168. [Google Scholar] [CrossRef]
- Wu, Z.J.; Song, Y.; Wang, H.L.; Zhang, F.; Li, F.H.; Wang, Z.Y. Influence of the built environment of Nanjing’s Urban Community on the leisure physical activity of the elderly: An empirical study. BMC Public Health 2019, 19, 1459. [Google Scholar] [CrossRef]
- Ulmer, J.M.; Wolf, K.L.; Backman, D.R.; Tretheway, R.L.; Blain, C.J.; O’Neil-Dunne, J.P.; Frank, L.D. Multiple health benefits of urban tree canopy: The mounting evidence for a green prescription. Health Place 2016, 42, 54–62. [Google Scholar] [CrossRef]
- Zhao, P.; Ji, X. Validation of the Mandarin Version of the Vocabulary Size Test. RELC J. 2016, 49, 308–321. [Google Scholar] [CrossRef]
- Yeh, A.; Li, X. Measurement and monitoring of urban sprawl in a rapidly growing region using entropy. Photogramm. Eng. Remote Sens. 2001, 67, 83–90. [Google Scholar]
- Miaoyi, L. Application of spatial and temporal entropy based on multivariate data for measuring the degree of urban function mix. China City Plan. Rev. 2015, 2015, 40–48. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- van Tilburg, T. Losing and Gaining in Old Age: Changes in Personal Network Size and Social Support in a Four-Year Longitudinal Study. J. Gerontol. Ser. B 1998, 53, S313–S323. [Google Scholar] [CrossRef]
- Biswas, R.K.; Kabir, E. Influence of distance between residence and health facilities on non-communicable diseases: An assessment over hypertension and diabetes in Bangladesh. PLoS ONE 2017, 12, e0177027. [Google Scholar] [CrossRef] [PubMed]
- Jennings, N.; Boyle, M.; Mahawar, K.; Balupuri, S.; Small, P. The relationship of distance from the surgical centre on attendance and weight loss after laparoscopic gastric bypass surgery in the United Kingdom. Clin. Obes. 2013, 3, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Zulian, G.; Donisi, V.; Secco, G.; Pertile, R.; Tansella, M.; Amaddeo, F. How are caseload and service utilisation of psychiatric services influenced by distance? A geographical approach to the study of community-based mental health services. Soc. Psychiatry Psychiatr. Epidemiol. 2011, 46, 881–891. [Google Scholar] [CrossRef] [PubMed]
- Moniruzzaman, M.; Páez, A.; Nurul Habib, K.M.; Morency, C. Mode use and trip length of seniors in Montreal. J. Transp. Geogr. 2013, 30, 89–99. [Google Scholar] [CrossRef]
- Schmidt, T.; Kerr, J.; Schipperijn, J. Associations between Neighborhood Open Space Features and Walking and Social Interaction in Older Adults-A Mixed Methods Study. Geriatrics 2019, 4, 41. [Google Scholar] [CrossRef] [Green Version]
- Rantanen, T.; Portegijs, E.; Viljanen, A.; Eronen, J.; Saajanaho, M.; Tsai, L.-T.; Kauppinen, M.; Palonen, E.-M.; Sipilä, S.; Iwarsson, S.; et al. Individual and environmental factors underlying life space of older people–study protocol and design of a cohort study on life-space mobility in old age (LISPE). BMC Public Health 2012, 12, 1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.; Sun, B. Impact of Built Environment on Urban Residents’ Subjective Well-being:Evidence from the China Labor-force Dynamics Survey. Urban Dev. Stud. 2017, 24, 69–75. [Google Scholar]
- Feng, J.; Huang, X.; Tang, S. Comparing the Influences of Objective and Subjective Built Environments on Physical Activities Participation among the Elderly:A Case Study of Nanjing, China. Shanghai Urban Plan. Rev. 2017, 3, 17–23. [Google Scholar]
- Liu, Z.; Wang, M. Job accessibility and its impacts on commuting time of urban residents in Beijing: From a spatial mismatch perspective. Acta Geogr. Sin. 2011, 66, 457–467. [Google Scholar]
- Zhu, J.; Fan, Y. Commute happiness in Xi’an, China: Effects of commute mode, duration, and frequency. Travel Behav. Soc. 2018, 11, 43–51. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Types of Social Areas | District | Subdistrict | Neighborhood | House Type | Number of Questionnaires Completed |
|---|---|---|---|---|---|
| High concentration area of the elderly population in old urban areas | Liwan | Hualin | Xingxian | Historical | 23 |
| Longjin | Huafu | Historical | 10 | ||
| Lingnan | Yangrendong | Historical | 28 | ||
| Yuexiu | Zhuguang | Zhujiangyuan | Historical | 61 | |
| Gathering areas for elderly individuals who have retired from government enterprises and institutions | Liwan | Baihedong | Guangchuanheyuan | Danwei | 93 |
| Haizhu | Nanshitou | Zhibei | Danwei | 120 | |
| Huangpu | Huangpu | Huangpuhuayuan | Commercial housing | 28 | |
| Tianhe | Yuancun | Meilinhaian | Commercial housing | 35 | |
| Scattered distribution area of the elderly who retired from educational and scientific research institutions | Tianhe | Wushan | Huagong | Danwei | 87 |
| Mixed population distribution area | Liwan | Dongjiao | Fanghehuayuan | Affordable housing | 21 |
| Baiyun | Jinsha | Jinshazhou | Affordable housing | 88 | |
| Panyu | Luopu | Guang’ao | Commercial housing | 18 | |
| Huangpu | Dasha | Hengsha | Urban village | 30 | |
| Concentrated distribution area of the rural elderly population | Baiyun | Zhongluotan | Dengtang | Rural village | 52 |
| Baiyun | Zhuyuan | Zhuer | Rural village | 25 | |
| Baiyun | Jianggao | Jiangcun | Rural village | 20 | |
| Huadu | Huadong | Shanxia | Rural village | 47 | |
| New development zone with a young population | Baiyun | Xinshi | Tangyong | Urban village | 38 |
| Panyu | dashi | Dashan | Urban village | 51 | |
| Tianhe | Tangxia | Tanged | Affordable housing | 7 |
| Variables | Proportion/Mean | Std | Maximum | Minimum |
|---|---|---|---|---|
| Dependent variable | ||||
| Physical health | 10.454 | 2.543 | 15 | 3 |
| Independent variable | ||||
| Population density | 1.944 | 1.824 | 8.211 | 0.079 |
| Land use mix | 0.667 | 0.085 | 0.749 | 0.454 |
| Number of POIs | 4044.568 | 3546.420 | 13344 | 36 |
| Number of parks and squares | 4.734 | 4.519 | 16 | 0 |
| Number of bus and subway stations | 28.733 | 16.137 | 69 | 1 |
| Distance to nearest park or square (km) | 0.482 | 0.578 | 2.8 | 0.016 |
| Distance to nearest bus or subway station (km) | 0.267 | 0.225 | 0.958 | 0.040 |
| Mediating variable | ||||
| Physical activity duration (h) | 1.559 | 1.117 | 5 | 1 |
| Neighborhood relationship | 3.969 | 0.660 | 5 | 1 |
| Social network | 3.732 | 0.967 | 5 | 1 |
| Neighborhood activity participation | 1.720 | 0.739 | 5 | 1 |
| Control variable | ||||
| Gender | ||||
| Female | 56.364% | |||
| Male | 43.636% | |||
| Age | ||||
| 60–75 | 79.205% | |||
| Above 75 | 20.795% | |||
| Educational level | ||||
| Primary school and below | 40.795% | |||
| Junior middle school | 27.614% | |||
| High school or technical secondary school | 24.886% | |||
| Training school | 4.3182% | |||
| Bachelor’s degree or above | 2.386% | |||
| Income | 4739.13 | 4213.04 | 47500 | 600 |
| Lifestyle | ||||
| Live alone or with a spouse | 49.659% | |||
| Live with children | 50.341% | |||
| Marital status | ||||
| Unmarried | 1.25 | |||
| Widowed or divorced | 20.682% | |||
| Married | 78.068% | |||
| Individual preferences | ||||
| Travel model | ||||
| Walk or ride | 72.841% | |||
| Public transport | 3.75% | |||
| Drive or take taxis | 23.409% | |||
| Smoke | 17.841% | |||
| Drink | 9.205% |
| Model 1 DV: Physical Health | Model 2a DV: Physical Activity | Model 2b DV: Neighborhood Relationship | Model 2c DV: Social Network | Model 2d DV: Neighborhood Activity Participation | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Coef. | SE | Coef. | SE | Coef. | SE | Coef. | SE | Coef. | SE | |
| Dependent variable | ||||||||||
| Built environment | ||||||||||
| Population density | −0.024 | 0.104 | −4.158 | 3.134 | 0.044 | 0.027 | 0.026 | 0.061 | −0.069 ** | 0.031 |
| Land use mix | 2.668 | 1.829 | 138.633 | 58.014 | −0.582 | 0.479 | −0.787 | 1.239 | 0.772 | 0.536 |
| Number of POIs | 0.0002322 ** | 0.00009 | 0.002 | 0.003 | −0.00004 | 0.00002 | −0.00003 | 0.00006 | 0.000009 | 0.00003 |
| Number of parks and squares | 0.060 * | 0.032 | 2.766 * | 1.002 | −0.002 | 0.008 | 0.030 | 0.021 | 0.019 ** | 0.009 |
| Number of bus and subway stations | −0.032 ** | 0.014 | 0.407 | 0.255 | −0.005 | 0.004 | −0.018 ** | 0.009 | 0.003 | 0.004 |
| Distance to nearest park or square | 0.578 ** | 0.275 | −0.622 | 8.727 | 0.073 | 0.072 | 0.269 | 0.184 | 0.230 ** | 0.081 |
| Distance to nearest bus or subway station | −1.833 ** | 0.696 | 16.471 | 23.008 | −0.559 ** | 0.182 | −1.586 ** | 0.511 | −0.650 ** | 0.204 |
| Control variable | ||||||||||
| Socioeconomic attribute | ||||||||||
| Age (ref. 60–75) | −0.516 ** | 0.221 | −14.873 ** | 5.898 | −0.062 | 0.058 | −1.128 | 0.081 | −0.084 | 0.065 |
| Gender (ref. female) | 0.327 * | 0.196 | 3.000 | 5.237 | −0.078 | 0.051 | −0.149 ** | 0.072 | −0.091 | 0.058 |
| Marital status (ref. unmarried) | ||||||||||
| Widowed or divorced | 0.624 | 0.809 | −9.680 | 21.549 | −0.225 | 0.212 | −0.049 | 0.295 | 0.072 | 0.237 |
| Married | 0.616 | 0.435 | −3.446 | 21.016 | −0.289 | 0.206 | −0.184 | 0.288 | −0.046 | 0.231 |
| Education level (ref. primary school and below) | ||||||||||
| Junior middle school | 0.347 | 0.221 | 8.754 | 5.883 | −0.047 | 0.058 | −0.035 | 0.081 | 0.027 | 0.065 |
| High school or technical secondary school | 0.507 ** | 0.241 | 13.251 ** | 6.439 | 0.043 | 0.063 | −0.013 | 0.089 | 0.040 | 0.071 |
| Training school | 0.218 | 0.447 | 13.168 | 11.916 | 0.038 | 0.117 | −0.112 | 0.163 | 0.168 | 0.131 |
| Bachelor’s degree or above | 0.719 | 0.587 | 26.860 * | 15.649 | −0.274 * | 0.154 | −0.086 | 0.214 | 0.070 | 0.172 |
| Income | 0.322 ** | 0.093 | −4.930 * | 2.515 | 0.051 ** | 0.024 | 0.191 *** | 0.035 | 0.047 * | 0.027 |
| Lifestyle (ref. live alone) | ||||||||||
| Live with children | −0.077 | 0.175 | 0.126 | 4.680 | −0.033 | 0.046 | −0.033 | 0.064 | 0.013 | 0.051 |
| Individual preferences | ||||||||||
| Travel model (ref. walk or ride) | ||||||||||
| Public transport | 0.034 | 0.449 | 6.066 | 11.975 | 0.132 | 0.118 | 0.348 ** | 0.164 | 0.171 | 0.132 |
| Drive or take taxis | 0.083 | 0.204 | 0.811 | 5.450 | 0.040 | 0.053 | 0.112 | 0.075 | 0.123 ** | 0.060 |
| Smoke (ref. no) | −0.238 | 0.264 | −7.670 | 7.054 | 0.033 | 0.069 | −0.027 | 0.097 | −0.068 | 0.077 |
| Drink (ref. no) | −0.205 | 0.326 | 5.080 | 8.692 | −0.006 | 0.085 | 0.044 | 0.119 | 0.117 | 0.096 |
| Constant | 5.679 *** | 1.564 | 31.519 | 47.466 | 4.590 *** | 0.409 | 3.681 *** | 0.944 | 0.812 * | 0.458 |
| Log likelihood | −2033.375 | −4919.8415 | −854.6478 | −1153.4956 | −954.4083 | |||||
| Prob > chi2 | 0.0000 | 0.0136 | 0.0001 | 0.0000 | 0.0000 | |||||
| AIC | 4114.75 | 9887.683 | 1757.296 | 2354.991 | 1956.817 | |||||
| Model 3a Mediator: Physical Activity | Model 3b Mediator: Neighborhood Relationship | Model 3c Mediator: Social Network | Model 3d Mediator: Neighborhood Activity Participation | |||||
|---|---|---|---|---|---|---|---|---|
| Coef. | SE | Coef. | SE | Coef. | SE | Coef. | SE | |
| Dependent variable | ||||||||
| Built environment | ||||||||
| Population density | −0.008 | 0.104 | −0.037 | 0.104 | −0.031 | 0.104 | −0.007 | 0.104 |
| Land use mix | 2.114 | 1.827 | 2.841 | 1.826 | 2.847 | 1.825 | 2.487 | 1.827 |
| Number of POIs | 0.0002253 ** | 0.00009 | 0.0002429 ** | 0.00009 | 0.0002389 ** | 0.00009 | 0.00023 ** | 0.0000892 |
| Number of parks and squares | −0.056 * | 0.031 | −0.060 ** | 0.032 | −0.069 ** | 0.032 | −0.065 ** | 0.032 |
| Number of bus and subway stations | −0.034 ** | 0.014 | −0.031 ** | 0.014 | −0.028 * | 0.014 | −0.033 ** | 0.014 |
| Distance to nearest park or square | 0.581 ** | 0.274 | 0.557 ** | 0.275 | 0.528 * | 0.275 | 0.524 * | 0.276 |
| Distance to nearest bus or subway station | −1.909 ** | 0.692 | −1.668 ** | 0.697 | −1.507 ** | 0.707 | −1.682 ** | 0.698 |
| Mediating variable | ||||||||
| Physical activity | 0.004 ** | 0.001 | ||||||
| neighborhood relationship | 0.296 ** | 0.129 | ||||||
| Social network | 0.216 ** | 0.091 | ||||||
| Neighborhood activity participation | 0.233 ** | 0.115 | ||||||
| Control variable | ||||||||
| Socioeconomic attribute | ||||||||
| Age (ref. 60–75) | −0.456 ** | 0.221 | −0.497 ** | 0.221 | −0.494 ** | 0.221 | −0.496 ** | 0.221 |
| Gender (ref. female) | 0.317 | 0.195 | 0.350 * | 0.196 | 0.356 * | 0.196 | 0.348 | 0.196 |
| Marital status (ref. unmarried) | ||||||||
| Widowed or divorced | 0.665 | 0.805 | 0.690 | 0.807 | 0.641 | 0.807 | 0.607 | 0.808 |
| Married | 0.633 | 0.785 | 0.701 | 0.787 | 0.661 | 0.787 | 0.626 | 0.787 |
| Education level (ref. primary school and below) | ||||||||
| Junior middle school | 0.312 | 0.220 | 0.361 | 0.219 | 0.355 | 0.219 | 0.341 | 0.220 |
| High school or technical secondary school | 0.453 * | 0.241 | 0.494 ** | 0.240 | 0.508 ** | 0.240 | 0.497 ** | 0.241 |
| Training school | 0.160 | 0.445 | 0.207 | 0.446 | 0.257 | 0.446 | 0.179 | 0.446 |
| Bachelor’s degree or above | 0.608 | 0.585 | 0.800 | 0.586 | 0.751 | 0.586 | 0.703 | 0.586 |
| Income | 0.340 *** | 0.093 | 0.307 ** | 0.093 | 0.279 ** | 0.095 | 0.311 ** | 0.093 |
| Lifestyle (ref. live alone or with spouse) | ||||||||
| Live with children | −0.080 | 0.174 | −0.068 | 0.175 | −0.069 | 0.175 | −0.080 | 0.175 |
| Individual preferences | ||||||||
| Travel model (ref. walk or ride) | ||||||||
| Public transport | 0.011 | 0.447 | −0.006 | 0.448 | −0.040 | 0.449 | −0.006 | 0.449 |
| Drive or take taxis | 0.081 | 0.203 | 0.071 | 0.203 | 0.054 | 0.204 | 0.054 | 0.204 |
| Smoke (ref. no) | 0.269 | 0.263 | 0.228 | 0.263 | 0.245 | 0.264 | 0.254 | 0.264 |
| Drink (ref. no) | 0.183 | 0.325 | 0.207 | 0.325 | 0.198 | 0.325 | 0.177 | 0.326 |
| Constant | 5.565 *** | 1.556 | 4.876 ** | 1.596 | 5.489 | 1.563 | ||
| Log likelihood | −2028.33 | −2030.7321 | −2030.5733 | −2031.3131 | ||||
| Intra-class variance | 0.00000004 | 1.26 × 10−6 | 8.59 × 10−7 | 0.1475 | ||||
| Inter-class variance | 2.4318 | 2.4384 | 2.4379 | 2.443548 | ||||
| Prob > chi2 | 0.0000 | 0.0000 | 0.0000 | 0.0000 | ||||
| AIC | 4106.66 | 4111.464 | 4111.147 | 4112.626 | ||||
| 95% Confidence Interval | Physical Activity | Neighborhood Relationship | Social Network | Neighborhood Activity Participation |
|---|---|---|---|---|
| Number of POIs | (−0.00001, 1.32 × 10−6) | (−0.0000187, −2.29 × 10−8) | (−0.0000193, −1.91 × 10−6) | (−2.93 × 10−6, 5.94 × 10−6) |
| Number of parks and squares | (−0.058032, −0.0041877) | (0.0075623, 0.0013637) | (−0.0034038, 0.0041927) | (−0.0001714, 0.0094156) |
| Number of bus and subway stations | (−0.0013139, 0.000964) | (−0.0029858, 0.0001178) | (−0.003491, −0.0000702) | (−0.0002155, 0.0021805) |
| Distance to nearest park or square | (−0.0074899, 0.0012913) | (−0.0197871, 0.0237924) | (−0.0491438, 0.0083953) | (−0.0550303, 0.0085365) |
| Distance to nearest bus or subway station | (−0.1176748, 0.0603461) | (−0.1308616, 0.0274121) | (−0.2816985, −0.0106241) | (−0.2269755, 0.0058005) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, R.; Liu, S.; Li, M.; He, X.; Zhou, C. The Effect of High-Density Built Environments on Elderly Individuals’ Physical Health: A Cross-Sectional Study in Guangzhou, China. Int. J. Environ. Res. Public Health 2021, 18, 10250. https://doi.org/10.3390/ijerph181910250
Zhang R, Liu S, Li M, He X, Zhou C. The Effect of High-Density Built Environments on Elderly Individuals’ Physical Health: A Cross-Sectional Study in Guangzhou, China. International Journal of Environmental Research and Public Health. 2021; 18(19):10250. https://doi.org/10.3390/ijerph181910250
Chicago/Turabian StyleZhang, Rongrong, Song Liu, Ming Li, Xiong He, and Chunshan Zhou. 2021. "The Effect of High-Density Built Environments on Elderly Individuals’ Physical Health: A Cross-Sectional Study in Guangzhou, China" International Journal of Environmental Research and Public Health 18, no. 19: 10250. https://doi.org/10.3390/ijerph181910250
APA StyleZhang, R., Liu, S., Li, M., He, X., & Zhou, C. (2021). The Effect of High-Density Built Environments on Elderly Individuals’ Physical Health: A Cross-Sectional Study in Guangzhou, China. International Journal of Environmental Research and Public Health, 18(19), 10250. https://doi.org/10.3390/ijerph181910250