From Environmental to Possible Occupational Exposure to Risk Factors: What Role Do They Play in the Etiology of Endometriosis?


Abstract
:1. Introduction
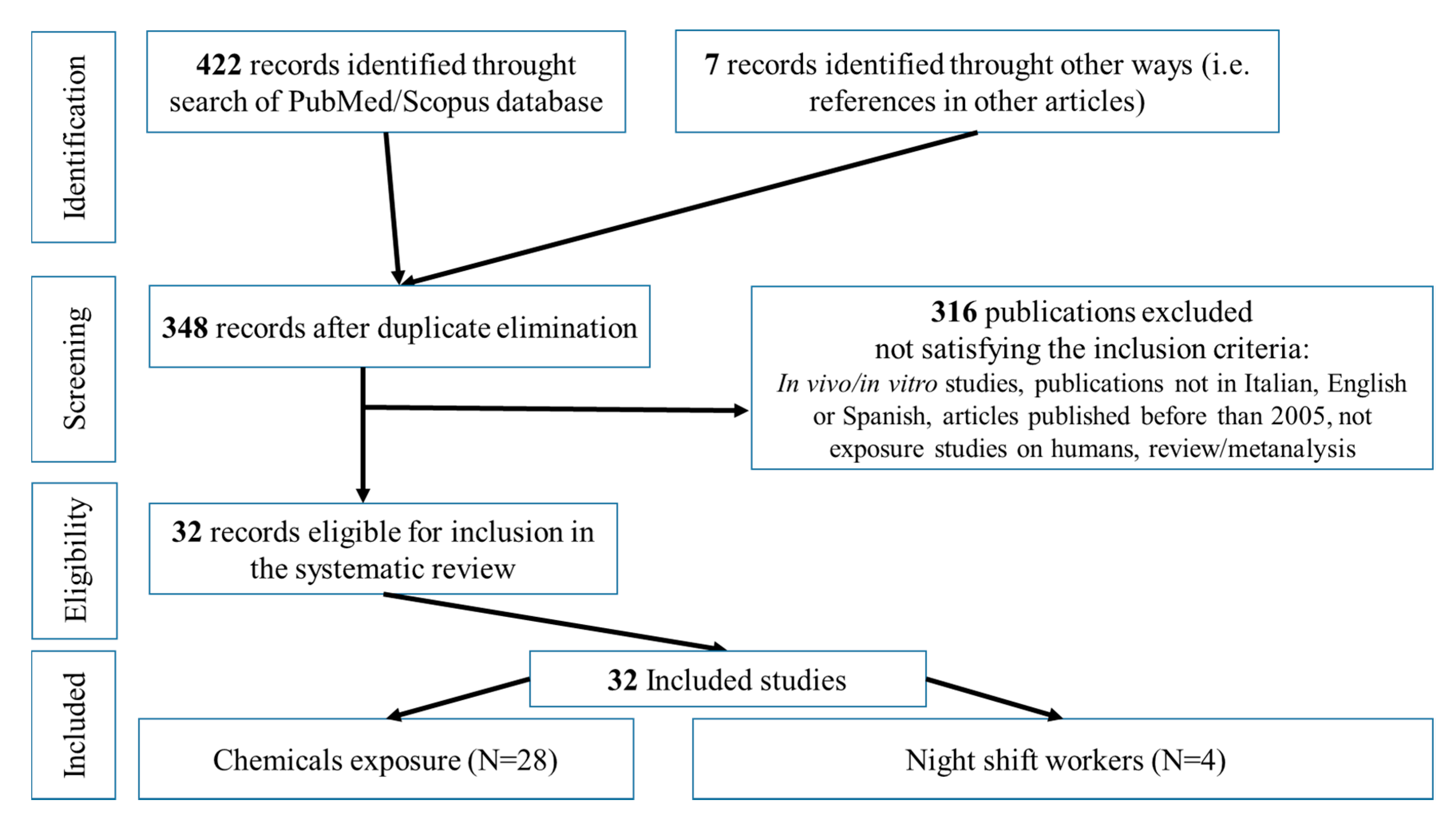
2. Materials and Methods
2.1. Literature Search Methodology
2.2. Eligibility Criteria and Study Selection
2.3. Bias Assessment
3. Results
3.1. Exposure to Plasticizers/Plasticizing Agents
3.2. Exposure to Metals
3.3. Exposure to Organohalogen Compounds and Pesticides
3.4. Night Workers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Zondervan, K.T.; Becker, C.M.; Koga, K.; Missmer, S.A.; Taylor, R.N.; Viganò, P. Endometriosis. Nat. Rev. Dis. Primers 2018, 4, 9. [Google Scholar] [CrossRef] [PubMed]
- Bulun, S.E. Endometriosis. N. Engl. J. Med. 2009, 360, 268–279. [Google Scholar] [CrossRef] [PubMed]
- Cartabellotta, A.; Laganà, A.S.; Ghezzi, F. Linee guida per la diagnosi e il trattamento dell’endometriosi. Evidence 2017, 9, e1000172. [Google Scholar] [CrossRef]
- Peñarrubia, P.G.; Ruiz-Alcaraz, A.J.; Martinez-Esparza, M.; Marin, P.; Machado-Linde, F. Hypothetical roadmap towards endometriosis: Prenatal endocrine-disrupting chemical pollutant exposure, anogenital distance, gut-genital microbiota and subclinical infections. Hum. Reprod. Update 2020, 26, 1–33. [Google Scholar] [CrossRef]
- Parazzini, F.; Esposito, G.; Tozzi, L.; Noli, S.; Bianchi, S. Epidemiology of endometriosis and its comorbidities. Eur J. Obstet. Gynecol. Reprod. Biol. 2017, 209, 3–7. [Google Scholar] [CrossRef]
- Kvaskoff, M.; Mu, F.; Terry, K.L.; Harris, H.R.; Poole, E.M.; Farland, L.; Missmer, S.A. Endometriosis: A high-risk population for major chronic diseases? Hum. Reprod. Update 2015, 21, 500–516. [Google Scholar] [CrossRef] [Green Version]
- Rashtian, J.; Chavkin, D.E.; Merhi, Z. Water and soil pollution as determinant of water and food quality/contamination and its impact on female fertility. Reprod. Biol. Endocrinol. 2019, 17, 5. [Google Scholar] [CrossRef] [Green Version]
- Vabre, P.; Gatimel, N.; Moreau, J.; Gayrard, V.; Picard-Hagen, N.; Parinaud, J.; Leandri, R.D. Environmental pollutants, a possible etiology for premature ovarian insufficiency: A narrative review of animal and human data. Environ. Health 2017, 16, 37. [Google Scholar] [CrossRef] [Green Version]
- Piazza, M.J.; Urbanetz, A.A. Environmental toxins and the impact of the other endocrine disrupting chemicals in women’s reproductive health. JBRA Assist. Reprod. 2019, 23, 154–164. [Google Scholar] [CrossRef]
- Marino, J.L.; Holt, V.L.; Chen, C.; Davis, S. Lifetime occupational history and risk of endometriosis. Scand. J. Work Environ. Health 2009, 35, 233–240. [Google Scholar] [CrossRef] [Green Version]
- Buck Louis, G.M.; Peterson, C.M.; Chen, Z.; Croughan, M.; Sundaram, R.; Stanford, J.; Varner, M.W.; Kennedy, A.; Giudice, L.; Fujimoto, V.Y.; et al. Bisphenol A and phthalates and endometriosis: The Endometriosis: Natural History, Diagnosis and Outcomes Study. Fertil. Steril. 2013, 100, 162–169.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gamble, K.L.; Resuehr, D.; Johnson, C.H. Shift work and circadian dysregulation of reproduction. Front. Endocrinol. 2013, 4, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Linee guida per il reporting di revisioni sistematiche e meta analisi: Il PRISMA statement. Evidence 2015, 7, e1000114. [Google Scholar]
- Wen, X.; Xiong, Y.; Qu, X.; Jin, L.; Zhou, C.; Zhang, M.; Zhang, Y. The risk of endometriosis after exposure to endocrine disrupting chemicals: A meta analysis of 30 epidemiology studies. Gynecol. Endocrinol. 2019, 35, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Sifakis, S.; Androutsopoulos, V.P.; Tsatsakis, A.M.; Spandidos, D.A. Human exposure to endocrine disrupting chemicals: Effects on the male and female reproductive systems. Environ. Toxicol. Pharmacol. 2017, 51, 56–70. [Google Scholar] [CrossRef]
- Cano Sancho, G.; Ploteau, S.; Matta, K.; Adoamnei, E.; Buck Louis, G.; Mendiola, J.; Darai, E.; Squifflet, J.; Le Bizec, B.; Antignac, J.P. Human epidemiological evidence about the associations between exposure to organochlorine chemicals and endometriosis: Systematic review and meta-analysis. Environ. Int. 2019, 123, 209–223. [Google Scholar] [CrossRef]
- Porpora, M.G.; Resta, S.; Fuggetta, E.; Brunelli, R.; Perrone, G.; D’Itri, F.; Storelli, P.; Manganaro, L.; De Filip, E. Esposizione a inquinanti organoclorurati ed endometriosi: Minireview. G. Ital. Ostet. Ginecol. 2012, 34, 527–530. [Google Scholar]
- Yao, M.; Hu, T.; Wang, Y.; Du, Y.; Hu, C.; Wu, R. Polychlorinated biphenyls and its potential role in endometriosis. Environ. Pollut. 2017, 229, 837–845. [Google Scholar] [CrossRef]
- Niskar, A.S.; Needham, L.L.; Rubin, C.; Turner, W.E.; Martin, C.A.; Patterson, D.G.J.; Hasty, L.; Wong, L.Y.; Marcus, M. Serum dioxins, polychlorinated biphenyls, and endometriosis: A case-control study in Atlanta. Chemosphere 2009, 74, 944–949. [Google Scholar] [CrossRef]
- Trabert, B.; De Roos, A.J.; Schwarts, S.M.; Peters, U.; Scholes, D.; Barr, D.B.; Holt, V.L. Non-dioxin-like polychlorinated biphenyls and risk of endometriosis. Environ. Health Res. 2010, 118, 1280–1285. [Google Scholar] [CrossRef] [Green Version]
- Heilier, J.F.; Donnez, J.; Lison, D. Organochlorines and endometriosis: A mini review. Chemosphere 2008, 71, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomized trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peinado, F.M.; Lendinez, I.; Sotelo, R.; Iribarne-Duran, L.M.; Fernandez-Parra, J.; Vela-Soria, F.; Olea, N.; Fernandez, M.F.; Freire, C.; Leon, J.; et al. Association of urinary levels of bisphenol A, F and S with endometriosis risk: Preliminary results of the EndEA study. Int. J. Environ. Res. Public Health 2020, 17, 1194. [Google Scholar] [CrossRef] [Green Version]
- Itoh, H.; Iwasaki, M.; Hanaoka, T.; Sasaki, H.; Tanaka, T.; Tsugane, S. Urinary bisphenol A concentration in infertile Japanese women and its association with endometriosis: A cross sectional study. Environ. Health Prev. Med. 2007, 12, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Cobellis, L.; Colacurci, N.; Trabucco, E.; Carpentiero, C.; Grumetto, L. Measurement of bisphenol A and bisphenol B levels in human blood sera from healthy and endometriotic women. Biomed. Chromatogr. 2009, 23, 1186–1190. [Google Scholar] [CrossRef]
- Moreira Fernandez, M.A.; Cardeal, Z.L.; Carneiro, M.M.; Andrè, L.C. Study of possible association between endometriosis and phthalate and bisphenol A by biomarkers analysis. J. Pharm. Biomed. Anal. 2019, 172, 238–242. [Google Scholar] [CrossRef]
- Kim, S.H.; Cho, S.; Ihm, H.J.; Oh, Y.S.; Heo, S.H.; Chun, S.; Im, H.; Chae, H.D.; Kim, C.H.; Kang, B.M. Possible role of phthalate in the pathogenesis of endometriosis: In Vitro, animal and human data. J. Clin. Endocrinol. Metab. 2015, 100, E1502–E1511. [Google Scholar] [CrossRef]
- Reddy, B.S.; Rozati, R.; Reddy, B.V.R.; Raman, N.V.V.S.S. Association of phthalate esters with endometriosis in Indian women. BJOG 2006, 113, 515–520. [Google Scholar] [CrossRef]
- Upson, K.; Sathyanarayana, S.; De Ross, A.J.; Thompson, M.L.; Scholes, D.; Dills, R.; Holt, V.L. Phthalates and risk of endometriosis. Environ. Res. 2013, 126, 91–97. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.H.; Chun, S.; Jang, J.Y.; Chae, H.D.; Kim, C.H.; Kang, B.M. Increased plasma levels of phthalate esters in women with advanced-stage endometriosis: A prospective case control study. Fertil. Steril. 2011, 95, 357–359. [Google Scholar] [CrossRef]
- Weuve, J.; Hauser, R.; Calafat, A.M.; Missmer, S.A.; Wise, L.A. Association of exposure to phthalate with endometriosis and uterine leiomyomata: Findings from NHANES, 1999–2004. Environ. Health Perspect. 2010, 118, 825–832. [Google Scholar] [CrossRef] [PubMed]
- Itoh, H.; Iwasaki, M.; Hanaoka, T.; Sasaki, H.; Tanaka, T.; Tsugane, S. Urinary phthalate monoesters and endometriosis in infertile Japanese women. Sci. Total Environ. 2009, 408, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Reddy, B.S.; Rozati, R.; Reddy, S.; Kodampur, S.; Reddy, P.; Reddy, R. High plasma concentration of polychlorinated bisphenyls and phthalate esters in women with endometriosis: A prospective case control study. Fertil. Steril. 2006, 85, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.C.; Tsai, E.M.; Li, W.F.; Liao, P.C.; Chung, M.C.; Wang, Y.H.; Wang, S.L. Association between phthalate exposure and glutathione S-transferase MI polymorphism in adenomyosis, leiomyoma and endometriosis. Hum. Reprod. 2010, 25, 986–994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Upson, K.; Sathyanarayana, S.; De Roos, A.J.; Koch, H.M.; Scholes, D.; Holt, V.L. A population based case-control study of urinary bisphenol A concentrations and risk of endometriosis. Hum. Reprod. 2014, 2, 2457–2464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simonelli, A.; Guadagni, R.; De Franciscis, P.; Colacurci, N.; Pieri, M.; Basilicata, P.; Pedata, P.; Lambereti, M.; Sannolo, N.; Miraglia, N. Environmental and occupational exposure to bisphenol A and endometriosis: Urinary and peritoneal fluid concentration levels. Int. Arch. Occup. Environ. Health 2017, 90, 49–61. [Google Scholar] [CrossRef]
- Jackson, L.W.; Zullo, M.D.; Goldberg, J.M. The association between heavy metals, endometriosis and uterine myomas among premenopausal women: National Health and Nutrition Examination Survey 1999–2002. Hum. Reprod. 2008, 23, 679–687. [Google Scholar] [CrossRef] [Green Version]
- Itoh, H.; Iwasaki, M.; Nakajima, Y.; Endo, Y.; Hanaoka, T.; Sasaki, H.; Tanaka, T.; Yang, B.; Tsugane, S. A case-control study of the association between urinary cadmium concentration and endometriosis in infertile Japanese women. Sci. Total Environ. 2008, 402, 171–175. [Google Scholar] [CrossRef]
- Heilier, J.F.; Donnez, J.; Verougstraete, V.; Donnez, O.; Grandjean, F.; Haufroid, V.; Nackers, F.; Lison, D. Cadmium, lead and endometriosis. Int. Arch. Occup. Environ. Health 2006, 80, 149–153. [Google Scholar] [CrossRef]
- Silva, N.; Senanayake, H.; Waduge, V. Elevated levels of whole blood nickel in a group of Sri Lanka women with endometriosis: A case control study. BMC Res. Notes 2013, 6, 13. [Google Scholar] [CrossRef] [Green Version]
- Pollack, A.Z.; Buck Louis, G.M.; Chen, Z.; Peterson, C.M.; Sundaram, R.; Croughan, M.S.; Sun, L.; Hediger, M.L.; Stanford, J.B.; Varner, M.W.; et al. Trace elements and endometriosis: The ENDO Study. Reprod. Toxicol. 2013, 42, 41–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, G.L.; Yeh, C.C.; Yeh, C.Y.; Chen, R.Y.; Fu, C.L.; Chen, C.H.; Tzeng, C.R. Decreased zinc and increased lead blood levels are associated with endometriosis in Asian women. Reprod. Toxicol. 2017, 74, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Cooney, M.A.; Buck Louis, G.M.; Hediger, M.L.; Vexler, A.; Kostyniak, P.J. Organochloride pesticides and endometriosis. Reprod. Toxicol. 2010, 30, 365–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Upson, K.; De Roos, A.J.; Thompson, M.L.; Sathyanarayana, S.; Scholes, D.; Barr Boyd, D.; Holt, V.L. Organochloride pesticides and risk of endometriosis: Findings from a population-based case-control study. Environ. Health Perspect. 2013, 121, 1319–1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buck Louis, G.M.; Chen, Z.; Peterson, C.M.; Hediger, M.L.; Croughan, M.S.; Sundaram, R.; Stanford, J.B.; Varner, M.W.; Fujimoto, V.Y.; Giudice, L.C.; et al. Persistent lipophilic environmental chemicals and endometriosis: The ENDO study. Environ. Health Perspect. 2012, 120, 811–816. [Google Scholar] [CrossRef] [Green Version]
- Campbell, S.; Raza, M.; Pollack, A.Z. Perfluoroalkyl substances and endometriosis in US women in NHANES 2003–2006. Reprod. Toxicol. 2016, 65, 230–235. [Google Scholar] [CrossRef]
- Li, A.J.; Chen, Z.; Lin, T.C.; Buck Louis, M. Association of urinary metabolites of organophosphate and pyrethroid insecticides and phenoxy herbicides with endometriosis. Environ. Int. 2020, 136, 105456. [Google Scholar] [CrossRef]
- Ploteau, S.; Cano-Sancho, G.; Volteau, C.; Legrand, A.; Venisseaux, A.; Vacher, V.; Marchand, P.; Le Bizec, B.; Antignac, J.P. Associations between internal exposure levels of persistent organic pollutants in adipose tissue and deep infiltrating endometriosis with or without concurrent ovarian endometrioma. Environ. Int. 2017, 108, 195–203. [Google Scholar] [CrossRef]
- Johnson, C.Y.; Grajewski, B.; Lawson, C.C.; Whelan, E.A.; Bertke, S.J.; Tseng, C.Y. Occupational risk factors for endometriosis in a cohort of flight attendants. Scand. J. Work Environ. Health 2016, 42, 52–60. [Google Scholar] [CrossRef] [Green Version]
- Marino, J.L.; Holt, V.L.; Chen, C.; Davis, S. Shift work, hCLOCK T3111C Polymorphism, and Endometriosis risk. Epidemiology 2008, 19, 477–484. [Google Scholar] [CrossRef] [Green Version]
- Schernhammer, E.S.; Vitonis, A.F.; Rich-Edwards, J.; Missmer, S.A. Rotating nightshift work and the risk of endometriosis in premenopausal women. Am. J. Obstet. Gynecol. 2011, 205, e1–e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, L.Y.; Kim, M.R.; Kim, J.H.; Cho, H.H. Aldo-keto reductase activity after diethylhexyl phthalate exposure in eutopic and ectopic endometrial cells. Eur. J. Obst. Gynecol. 2017, 215, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Pollack, A.Z.; Ranasinghe, S.; Sjaarda, L.A.; Mumford, S.L. Cadmium and reproductive health in women: A systematic review of the epidemiologic evidence. Curr. Environ. Health Rep. 2014, 1, 172–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rzymski, P.; Tomczyk, K.; Rzymski, P.; Pniedzialek, B.; Opala, T.; Wilczak, M. Impact of heavy metals on the female reproductive system. Ann. Agricol. Environ. Med. 2015, 22, 259–264. [Google Scholar] [CrossRef]
- Silva, N.; Peiris-John, R.; Wickremasinghe, S.H.; Sathiakumar, N. Cadmium a metalloestrogen: Are we convinced? J. Appl. Toxicol. 2011, 32, 318–332. [Google Scholar] [CrossRef]
- Atsdr- Agency fot Toxic Substances and Disease Registry. Toxicological Profile for Cadmium; US department of Health and Human Services, Public Health Services: Atlanta, GA, USA, 1999.
- Meharg, A.A.; Norton, G.; Deacon, C.; Williams, P.; Adomako, E.E.; Price, A.; Zhu, Y.; Li, G.; Zhao, F.J.; McGrath, S.; et al. Variation in rice cadmium related to human exposure. Environ. Sci. Technol. 2013, 47, 5613–5618. [Google Scholar] [CrossRef]
- Thornton, I. Sources and pathways of cadmium in the environment. IARC Sci. Publ. 1992, 118, 149–162. [Google Scholar]
- Scherer, G.; Barkemeyer, H. Cadmium concentrations in tobacco and tobacco smoke. Ecotoxicol. Environ. Saf. 1983, 7, 71–78. [Google Scholar] [CrossRef]
- Driscoll, T.R.; Carey, R.N.; Peters, S.; Glass, D.C.; Benke, G.; Reid, A.; Fritschi, L. The Australian work exposures study: Occupational exposure to lead and lead compounds. Ann. Occup. Hyg. 2016, 60, 113–123. [Google Scholar] [CrossRef]
- Koh, D.H.; Locke, S.J.; Chen, Y.C.; Purdue, M.P.; Friesen, M.C. Lead exposure in US worksites: A literature review and development of an occupational lead exposure database from published literature. Am. J. Ind. Med. 2015, 58, 605–616. [Google Scholar] [CrossRef] [Green Version]
- Järup, L. Hazards of heavy metals contamination. Br. Med. Bull. 2003, 68, 167–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjørklund, G.; Hilt, B.; Dadar, M.; Lindh, U.; Aaseth, J. Neurotoxic effects of mercury exposure in dental personnel. Basic Clin. Pharmacol. Toxicol. 2019, 124, 568–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anglen, J.; Gruninger, S.E.; Chou, H.N.; Weuve, J.; Turyk, M.E.; Freels, S.; Stayner, L.T. Occupational Mercury Exposure in Association With Prevalence of Multiple Sclerosis and Tremor Among US Dentists. J. Am. Dent. Assoc. 2015, 146, 659–668. [Google Scholar] [CrossRef] [PubMed]
- Shirkhanloo, H.; Fallah Mehrjerdi, M.A.; Hassani, H. Identifying Occupational and Nonoccupational Exposure to Mercury in Dental Personnel. Arch. Environ. Occup. Health 2017, 72, 63–69. [Google Scholar] [CrossRef]
- Besson, J.C.; Augarde, E.; Nasterlack, M. Worker protection during electrolysis plant decommissioning. Arhiv za Higijenu Rada i Toksikologiju 2012, 63, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Wilson, E.; Lafferty, J.S.; Thiboldeaux, R.; Tomasallo, C.; Grajewski, B.; Wozniak, R.; Meiman, J. Occupational Mercury Exposure at a Fluorescent Lamp Recycling Facility—Wisconsin, 2017. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 763–766. [Google Scholar] [CrossRef] [Green Version]
- Al-Batanony, M.A.; Abdel-Rasul, G.M.; Abu-Salem, M.A.; Al-Dalatony, M.M.; Allam, H.K. Occupational exposure to mercury among workers in a fluorescent lamp factory, Quisna Industrial Zone, Egypt. Int. J. Occup. Environ. Med. 2013, 4, 149–156. [Google Scholar]
- Bose-O’Reilly, S.; Bernaudat, L.; Siebert, U.; Roider, G.; Nowak, D.; Drasch, G. Signs and Symptoms of Mercury-Exposed Gold Miners. Int. J. Occup. Med. Environ. Health 2017, 30, 249–269. [Google Scholar] [CrossRef]
- Boivin, D.B.; James, F.O. Circadian adaptation to night-shift work by judicious light and darkness exposure. J. Biol. Rhythms 2002, 17, 556–567. [Google Scholar] [CrossRef]
- Luboshitzky, R.; Herer, P.; Shen Orr, Z. Cyproterone acetate-ethinyl estradiol treatment alters urinary 6-sulfatoxymelatonin excretion in hyperandrogenic women. Neuro Endocrinol. Lett. 2002, 23, 309–313. [Google Scholar]
- Kennaway, D.J.; Boden, M.J.; Varcoe, T.J. Circadian rhythms and fertility. Mol. Cell Endocrinol. 2012, 349, 56–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boden, M.J.; Kennaway, D.J. Circadian rhythms and reproduction. Reproduction 2006, 132, 379–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahoney, M.M. Shift work, jet lag and female reproduction. Int. J. Endocrinol. 2010, 2010, 813764. [Google Scholar] [CrossRef] [PubMed]
- Lawson, C.C.; Whelan, E.A.; Lividoti Hibert, E.N.; Spiegelman, D.; Schernhammer, E.S.; Rich-Edwards, J.W. Rotating shift work and menstrual cycle characteristics. Epidemiology 2011, 22, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Cone, J.E.; Vaughan, L.M.; Huete, A.; Samuels, S.J. Reproductive health outcomes among female flight attendants: An exploratory study. J. Occup. Environ. Med. 1998, 40, 210–216. [Google Scholar] [CrossRef]
- Rocheleau, C.M.; Lawson, C.C.; Whelan, E.A.; Rich-Edwards, J.W. Shift work and adverse pregnancy outcomes: Comments on a recent meta analysis. BJOG 2012, 119, 378. [Google Scholar] [CrossRef]
- Giudice, L.C.; Kao, L.C. Endometriosis. Lancet 2004, 364, 1789–1799. [Google Scholar] [CrossRef]
- Swaen, G.M.H.; Otter, R. Letter to the Editor: Phthalates and endometriosis. J. Clin. Endocrinol. Metab. 2016, 101, L108–L109. [Google Scholar] [CrossRef]
- Kay, V.R.; Chabers, C.; Forster, W.G. Reproductive and developmental effects of phthalate diesters in females. Crit. Rev. Toxicol. 2013, 43, 200–219. [Google Scholar] [CrossRef] [Green Version]
- Koch, H.M.; Bolt, H.M.; Preuss, R.; Angerer, J. New metabolites of di(2-ethylhexyl)phthalate (DEHP) in human urine and serum after single oral doses of deuterium-labelled DEHP. Arch. Toxicol. 2005, 79, 367–376. [Google Scholar] [CrossRef]
- Cai, W.; Yang, J.; Liu, Y.; Bi, Y.; Wang, H. Association between phthalate metabolite and risk of endometriosis. Int. J. Environ. Res. Public Health 2019, 16, 3678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caserta, D.; Di Segni, N.; Mallozzi, M.; Giovanale, V.; Mantovani, A.; Marci, R.; Moscarini, M. Bisphenol A and the female reproductive tract: An overview of recent laboratory evidence and epidemiological studies. Reprod. Biol. Endocrinol. 2014, 12, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngueta, G.; Longnecker, M.P.; Yoon, M.; Ruark, C.D.; Clewell, H.J.; Andersen, M.E.; Verner, M.A. Quantitative bias analysis of a reported association between perfluoroalkyl substances (PFAS) and endometriosis: The influence of oral contraceptive use. Environ. Int. 2017, 104, 118–121. [Google Scholar] [CrossRef] [PubMed]
- Vandenberg, L.N. Low doses effects of hormones and endocrine disruptors. Vitam. Horm. 2014, 94, 129–165. [Google Scholar] [CrossRef]
- Garavaglia, E.; Ricci, E.; Cioffi, R.; Trojano, G.; Bilfoni, A.; Parazzini, F.; Viganò, P. Smoking habits and endometriosis risk among infertile women: Results from a case control study. Ital. J. Gynecol. Obst. 2017, 29, 15–18. [Google Scholar] [CrossRef]
- Bravi, F.; Parazzini, F.; Cipriani, S.; Chiaffarino, F.; Ricci, E.; Chiantena, V.; Viganò, P.; La Vecchia, C. Tobacco smoking and risk of endometriosis: A systematic review and meta-analysis. BMJ Open 2014, 4, e006325. [Google Scholar] [CrossRef]
- Hunt, P.A.; Sathyanarayana, S.; Fowler, P.A.; Trasande, L. Female reproductive disorders, diseases, and costs of exposure to endocrine disrupting chemicals in the European Union. J. Clin. Endocrinol. Metab. 2016, 101, 1562–1570. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Ref. | Substance | Type of Study | Sample | Biomarkers and Concentrations | Results | Considerations |
|---|---|---|---|---|---|---|
| [24] | BPA a | cross-sectional | 166 women with endometriosis | Urinary BPA (μg/g creat. b) 0.80 (median) | No correlation was found between urinary BPA levels and disease severity. | Mean BPA values did not differ significantly between women with stage 0–I (0.74μg/g creat.) of endometriosis severity compared to stage II–IV (0.93 μg/g creat.). |
| [25] | BPA and BPB c | case-control | 58 women with endometriosis, 11 women controls | Serum BPA and BPB (μg/L) BPA 2.91 vs. 0.00 BPB 5.15 vs. 0.00 (arithmetic mean) | None of the control biological samples showed the presence of BPA or BPB, whereas there was presence in 63.8% of cases. | The sample size and the absence of an evaluation of statistical significance make the data indicative but not usable for the purpose of an evaluation of correlation with onset of the disease. |
| [26] | BPA and phthalates | case-control | 30 women cases, with laparoscopic diagnosis of endometriosis and 22 women controls | Urinary BPA and phthalate metabolites. (μg/g creat.) BPA: 9.78 vs. 8.80 MMP d 62.8 vs. 105.0 MiBP e 185.0 vs. 183.0 MnBP f 83.3 vs. 76.3 MCHP g 12.6 vs. 6.87 MEHP h 30.4 vs. 30.2 MiNP i 73.2 vs. 18.9 MOP j 670.0 vs. <LOQ MBzP k 23.8 vs. <LOQ (arithmetic mean) | Absence of statistically significant differences between the two groups. For monoisobutyl phthalate, an OR l = 1.93, 95% CI m 0.51–7.33) was obtained but not significant (χ2). | The sample size can greatly affect the consistency of the study outcome. |
| [23] | BPA, BPF n and BPS o | case-control | 35 women with laparoscopic diagnosis of endometriosis, and 89 women controls | Urinary BPA, BPF, BPS (μg/g creat.) BPA 3.6 vs. 3.0 BPS 0.1 vs. 0,2 BPF 0.1 vs. 0.1 (geometric mean) | There is an increased risk between: BPA exposure and endometriosis- OR 1.5, 95% CI 1.0–2.3; exposure to the sum of three alkylphenols (BPA, BPF, BPS) and endometriosis -OR = 1.5, 95% CI 0.9–2.3. | Exposure to BPA is suggestive of a greater risk of endometriosis, but the study sample is numerically limited. |
| [27] | phthalates | case-control | 55 women with endometriosis, 33 women controls | Urinary phthalate metabolites (μg/g creat.) MEHHP p 18.2 vs. 12.9 MEOHP q 13.4 vs. 10.3 MnBP 41.7 vs. 32.4 MBzP 5.8 vs. 7.3 MECPP r 23.8 vs. 19.0 (arithmetic mean) | The association between MEHHP and MEOHP levels (both metabolites of DEHP s) and endometriosis was significant. | The data were suggestive of a possible association between exposure and endometriosis, but the sample size can considerably affect the robustness of the study, in addition to the reduced number of controls compared to cases. |
| [28] | phthalates | case-control | 85 women with laparoscopic diagnosis of endometriosis and 135 women controls | Blood phthalates. (μg/mL) DnBP t 0.44 vs. 0.15 BBzP u 0.66 vs. 0.11 DnOP v 3.32 vs. 0.00 DEHP 2.44 vs. 0.45 (arithmetic mean) | Statistically significant differences emerged between the controls and the group of women with stage I and IV of endometriosis severity; in particular for DnBP, BBzP, DEHP and DnOP (p <0.05 ANOVA w). | The results were indicative of a correlation between exposure to some phthalates and the onset of endometriosis. |
| [29] | phthalates | case-control | 92 women with endometriosis and 195 women controls | Urinary phthalate metabolites (μg/g creat.) MEHP 2.2 vs. 3.4 MEHHP 14.8 vs. 18.8 MEOHP 8.1 vs. 10.8 MBzP 4.5 vs. 5.0 MEP x 61.9 vs. 43.9 MECPP 14.4 vs. 18.0 MiBP 1.3 vs. 1.5 MnBP 9.8 vs. 10.0 (median) | Inverse association between urinary levels of the DEHP metabolites and endometriosis was found, while a direct correlation for MBzP and MEP was identified, both without statistical significance. | Controversial data in terms of risk for incidence of endometriosis emerged, different by type of phthalate. |
| [30] | phthalates | case-control | 97 women with endometriosis and 169 women controls | Blood phthalates (μg/L) MEHP 17.4 vs. 12.4 DEHP 179.7 vs. 92.5 (arithmetic mean) | There was a statistically significant difference between cases and controls in DEHP blood levels (179.7 ± 32.5 ng/mL vs. 92.5 ± 31.1 ng/mL) with a weak but significant association with MEHP (OR = 1.020, 95% CI 1.003–1.038 p = 0.020). | In the stratification of the sample with respect to the stages of severity of endometriosis, the data suggest a correlation between exposure and disease. The blood determination of phthalates carries a greater risk of contamination by laboratory plastic material than the urinary determination of metabolites. |
| [31] | phthalates | cross-sectional | 1227 women with self-reported diseases—of which 87 with endometriosis | Urinary phthalate metabolites (μg/L) MEHP 2.5 vs. 3.4 MBP 28.9 vs. 25.5 MEP 207.0 vs. 219.9 MBzP 14.4 vs. 14.1 MEHHP 16.5 vs. 19.7 MEOHP 11.5 vs. 13.5 (geometric mean) | An association between endometriosis and exposure to MnBP, OR 1.36 (95% CI 0.77–2.41) and an inverse association with MEHP OR = 0.44 (95% CI 0.19–1.02) were identified. | Need for confirmation of data in prospective and case-control studies. |
| [32] | phthalates | case-control | 57 women with laparoscopic diagnosis of endometriosis and 80 women controls (stage 0–I endometriosis severity) | Urinary phthalates metabolites (μg/L) MnBP 26.5 vs. 20.0 MMP 12.0 vs. 8.3 MEHP 8.9 vs. 5.4 MEHHP 17.6 vs. 9.1 MEOHP 8.0 vs. 3.7 (arithmetic mean) | The comparison between the urinary levels of MEHP, MnBP, MBzP, MEHHP did not reveal a significant correlation between exposure to phthalates and endometriosis. | The results do not support the hypothesis of a greater risk of endometriosis in the case of greater exposure to phthalates. |
| [33] | phthalates | case-control | 49 infertile women with endometriosis; 38 infertile women controls but without endometriosis; 21 fertile women without endometriosis | Blood phthalates (μg/L) Stage IV ofendometriosis severity vs. controls: DnBP 1.05 vs. 0.11 BBzP 1.27 vs. 0.14 DEHP 4.39 vs. 0.48 DnOP 5.35 vs. 0.03 (arithmetic mean) | The cases showed significantly higher values of DnBP, BBzP, DnOP and serum DEHP compared to the two control groups. Furthermore, the correlation between phthalates and the severity of endometriosis seemed statistically significant. | The study supports the hypothesis of correlation between exposure to phthalates and the onset of endometriosis, although the sample size is particularly low. The blood determination of phthalates carries a greater risk of contamination by laboratory plastic material than the urinary determination of metabolites. |
| [34] | phthalates | case-control | 28 women with laparoscopic diagnosis of endometriosis, 29 women controls | Urinary phthalate metabolites (μg/g creat.) MnBP 94.1 vs. 58.0 MMP 52.4 vs. 32.1 MEP 58.0 vs. 71.4 MBzP 12.2 vs. 8.9 MEHP 4.2 vs. 3.4 5-oxo-MEHP y 19.0 vs. 7.8 5-OH-MEHP z 16.7 vs. 9.9 (arithmetic mean) | The cases showed higher urinary levels of MnBP (94.1 vs. 58.0 μg/g creat.) than controls. | The same authors suggested producing further studies of greater statistical strength to confirm the data relating to the possible association between exposure to phthalates and endometriosis. |
| [35] | BPA | case-control | 143 women with laparoscopic diagnosis of endometriosis. 287 women controls | Urinary BPA (μg/g creat.) 1.32 vs. 1.24 (median) | Total BPA urinary levels did not show differences between cases and controls and no correlation with the different stages of severity of the disease was found. | Limitations of the study: the sampling time of the biological material (single urine spot sample); the absence of disease in the controls was self-declared, which could make the control sample not entirely suitable. |
| [36] | BPA | case-control | 68 women with endometriosis and 60 women controls | Urinary BPA (μg/L) 5.31 vs. 1.64 (arithmetic mean) | A significant difference between cases and controls in BPA urinary levels was found. Conflicting data emerged with respect to the identification of work activities potentially at greater risk of endometriosis and/or exposure to BPA. | The data relating to work activity were collected with self-administration of a questionnaire. This generated mixed data. The authors underlined the need to structure exposure studies directly in specific work environments. |
| [11] | phthalates | case-control (matched cohort design) | 495 women of “operative cohort” (190 with endometriosis) and 131 women of the “population cohort” (14 with endometriosis) | Urinary BPA and phthalate metabolites (μg/L) (operative/population cohort) BPA 1.5 vs. 1.6/4.2 vs. 1.7 MMP 2.1 vs. 2.4/3.7 vs. 2.7 MEP 107.2 vs. 109.6/ 152.0 vs. 138.2 MCPP A 2.7 vs. 3.4/ 5.8 vs. 4.1 MnBP 12.1 vs. 11.0/ 19.1 vs. 11.2 MECCP 24.7 vs. 22.0/54.2 vs. 20.3 MCMHP B 29.3 vs. 29.2/ 53.5 vs. 22.5 MEHHP 16.3 vs. 14.4/ 32.4 vs. 11.9 MEOHP 11.0 vs. 10.1/ 23.0 vs. 8.3 MCHP 0.03 vs. 0.04/ 0.04 vs. 0.03 MBzP 7.0 vs. 7.8/ 9.9 vs. 6.5 MEHP 4.8vs. 4.1/ 8.3 vs. 3.1 MOP 0.06vs0.06/ 0.06 vs. 0.05 MiNP 0.16vs0.16/ 0.22 vs. 0.16 (geometric mean) | Urinary levels of the metabolites of 6 phthalates were associated with an increase in the diagnosis of endometriosis and in particular for MnOP (OR 1.38, 95% CI 1.10–1.72) and MEHP (OR 1.35, 95% CI 1.03–1.78). | The greatest significance was observed in sub-populations including laparoscopic and cytological diagnoses. |
| Ref. | Metal | Type of Study | Sample | Result | Considerations |
|---|---|---|---|---|---|
| [37] | cadmium, lead and mercury | cross-sectional | 1425 women with self-reported endometriosis | A correspondence between blood levels of cadmium and endometriosis was highlighted; 2nd tertile vs. 1st OR a = 1.94, 95% CI b 0.73–5.18; 3rd tertile vs. 1st OR = 3.39, 95% CI 1.37–8.40. | It is a cross-sectional study; the data should be confirmed with prospective and case-control studies. |
| [38] | cadmium | case-control | 54 infertile women with endometriosis and 74 women controls | No statistically significant differences emerged between urinary cadmium levels in cases and controls. | The hypothesis of interaction between cadmium and endometriosis was not confirmed; the sample was small. |
| [39] | cadmium and lead | case-control | 119 women with endometriosis and 25 women controls | The mean urinary and blood values of cadmium did not differ in the two groups. The values of lead in the cases were lower than in the controls. | The data did not support the hypothesis of exposure to metals as a risk factor; the number of controls was particularly small. |
| [40] | lead, cadmium, nickel | case-control | 50 women with laparoscopic diagnosis of endometriosis and 50 women controls | Blood data for cadmium and lead showed no differences between the two groups. On average nickel values were significantly higher in cases (2.6 vs. 0.8 μg/L). | The association between exposure to nickel and the onset of endometriosis is controversial for the same authors, especially due to the small study sample. |
| [41] | lead cadmium, mercury and other metallic elements | case-control | 473 women with surgical diagnosis of endometriosis, 131 women controls without endometriosis highlighted with magnetic resonance imaging | Blood cadmium was inversely associated with the diagnosis of endometriosis (OR = 0.55, 95% CI 0.31–0.98), while urinary chromium and copper showed a direct correlation (OR 1.97, 95% CI 1.21–3.19 and OR 2.66, 95% CI 1.26–5.64, respectively). | The data did not support the hypothesis of a correlation between exposure to lead, mercury or cadmium and the onset of endometriosis. The number of controls compared to the cases was far too low to give robustness to the statistical processing. |
| [42] | lead, cadmium, mercury and other metallic elements | cross-sectional | 190 infertile women, with and without endometriosis | The only significant data was for lead: OR = 2.59, 95% CI 1.11–6.06. | Infertile women with endometriosis had higher blood lead values than the others. The results require confirmation with prospective studies. |
| Ref. | Substance | Type of Study | Sample | Results | Considerations |
|---|---|---|---|---|---|
| [43] | organo-chlorinated | case-control | 29 women with endometriosis and 51 women controls | The highest tertile of aromatic fungicide exposure was associated with a higher risk of endometriosis (OR a = 5.3, 95% CI b 1.2–23.6). | Increased risk due to aromatic fungicides exposure emerged; the sample number was very small. |
| [44] | organo-chlorinated | case-control | 248 women with endometriosis and 538 women controls | Increased risk due to β-chlorocyclohexane exposure (fourth vs. first tertile OR 1.3, 95% CI 0.8–2.4) emerged. The association was greater between serum levels of β-chlorocyclohexane and ovarian endometriosis (OR 2.5, 95% CI 1.1–5.3). | The data were suggestive of an increased risk of endometriosis due to pesticide exposure, particularly for β-chlorocyclohexane. |
| [45] | organo-chlorinated | cross-sectional matched cohort | 473 women (190 with endometriosis), 127 in the general population (14 with endometriosis) | In the operative cohort, γ-hexachlorocyclohexane showed positive association with endometriosis (OR = 1.27, 95% CI 1.01–1.59) and β-hexachlorocyclohexane in the population cohort (OR 1.72, 95% CI: 1.09–2.72). | Positive association between organochlorine compound exposure and the onset of endometriosis emerged, particularly for β- and γ-hexachlorocyclohexane. |
| [46] | Perfluoro-alkyls | cross-sectional | 753 women, (54 with self-reported endometriosis) | Serum levels of perfluoroalkyls are significantly higher in women with endometriosis. | The data were suggestive of a possible association between exposure and endometriosis. |
| [47] | organo-phosphorics, pyrethroids, phenoxy herbicides | cross-sectional matched cohort | 471 women (188 with endometriosis) and 123 in the general population (14 with endometriosis) | High exposure levels to diazinon, chlorpyrifos and chlorpyrifos methyl seemed to be associated with a higher incidence of endometriosis. | The risk incidence data, adjusted due to possible confounding factors reduce/eliminate statistical significance. |
| [48] | organo-chlorinated | case-control | 44 women with endometriosis and 49 women controls | A correlation was found, in particular, for: β-hexachlorocyclohexane (logOR = 0.46, 95% CI −0.09/1.00), hexachlorobenzene (log OR = 0.72, 95% CI 0.13/1.31); the trans-nonachlor (log OR = 0.79, 95% CI 0.17/1.41); dieldrin (log OR = 1.95% CI 0.41/1.59); oxychlordane (log OR = 1.17, 95% CI 0.38/1.95); the cis-heptachlor epoxide (log OR = 1.68, 95% CI 0.78/2.58). | The data were suggestive of an involvement of organochlorine compounds in the etiology of endometriosis. However, the sample size was small. |
| Reference | Type of Study | Sample | Results | Considerations |
|---|---|---|---|---|
| [49] | cross-sectional | 1945 female flight attendants and 236 female teachers | There was no difference between the two cohorts, OR a 1.0 (95% CI b 0.5–2.2). Higher incidence of endometriosis in flight attendants with long haul flights than in the lowest quartiles OR 2.2 (95% CI 1.1–4.2) emerged. | In addition to shift work, the greatest exposure to cosmic rays for flight attendants was evaluated. |
| [50] | case-control | 235 women with surgical diagnosis of endometriosis and 545 women controls | Night work was associated with an increase in the incidence of endometriosis OR 1.48 (95% CI 0.96–2.29), in the case of jobs involving more than half of their work time during the night hours OR 1.98 (95% CI 1.01–3.85). High risk of endometriosis emerged mostly for those who worked for 5 consecutive years for more than 50% of the time in night work shifts (OR = 5.32 95% CI 1.21–23.0). | The influence of night work, especially if prolonged, on the incidence of disease was suggested. |
| [51] | prospective (follow up 16 years) | 89,400 women; 2062 women with laparoscopic diagnosis of endometriosis over 16 years of follow-up | There was no correlation between night work and the incidence of endometriosis. In the sub-sample of infertile women, a significance was highlighted for those who had been working at night for more than 5 years, OR 1.71 (95% CI 1.18–2.49). | Women with seniority (nurses) > 5 years, with night shifts, had a greater risk in the case of concomitant situation of infertility. |
| [10] | case-control | 341 women with laparoscopic diagnosis of endometriosis and 742 women controls | Higher incidence of endometriosis reported in flight attendants (OR 9.80, 95% CI 1.08–89.02) serving at service stations (OR 5.77, 95% CI 1.03–32.43), health workers (OR 1.49, 95% CI 1.03– 2.15). | The sample size of the subgroups, divided by work activity, was very small. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caporossi, L.; Capanna, S.; Viganò, P.; Alteri, A.; Papaleo, B. From Environmental to Possible Occupational Exposure to Risk Factors: What Role Do They Play in the Etiology of Endometriosis? Int. J. Environ. Res. Public Health 2021, 18, 532. https://doi.org/10.3390/ijerph18020532
Caporossi L, Capanna S, Viganò P, Alteri A, Papaleo B. From Environmental to Possible Occupational Exposure to Risk Factors: What Role Do They Play in the Etiology of Endometriosis? International Journal of Environmental Research and Public Health. 2021; 18(2):532. https://doi.org/10.3390/ijerph18020532
Chicago/Turabian StyleCaporossi, Lidia, Silvia Capanna, Paola Viganò, Alessandra Alteri, and Bruno Papaleo. 2021. "From Environmental to Possible Occupational Exposure to Risk Factors: What Role Do They Play in the Etiology of Endometriosis?" International Journal of Environmental Research and Public Health 18, no. 2: 532. https://doi.org/10.3390/ijerph18020532