1. Introduction
As the life expectancy of the elderly increases due to the effects of medical technology and increased living standards, physical changes and health challenges due to aging become a primary concern. Advanced age is associated with decreased flexibility, coordination, and muscle strength, and increased physical response time due to neuronal degeneration. Therefore, the elderly are not capable of rapid response to sudden changes in the environment [
1]. These changes in the elderly reduce cognitive motor responses and postural control, thereby increasing the incidence of trauma and death due to falls [
2,
3]. It has been reported that 30% of the elderly aged at least 65 years residing in the community sustain a fall injury at least once a year. The risks and economic costs of falls increase along with age, and nearly 40% of those who sustain an initial fall injury experience recurrent falls [
4,
5].
Falls occur due to intrinsic factors related to physiological changes associated with aging or disease as well as extrinsic environmental factors, such as slippery grounds, poor lighting and obstacles [
6]. These factors can be independent or related to each other in complex and diverse ways. Decreased ability to maintain posture, increased postural sway, decreased walking speed and dynamic balance may be closely related to the occurrence of falls [
7]. The incidence of falls is reported to be the highest during walking, followed by descending stairs, standing up, and changing direction, and is higher among women than men [
8].
Recently, various interventions have been attempted to prevent falls in the elderly and improve their daily living activities and ability to balance. Motor imagery training and task-oriented training are being used as evidence-based interventions in diverse fields of rehabilitation [
9,
10].
Motor imagery training is a learning process in which movements are only internally imagined without being physically carried out [
11]. Imagery training engages the same areas of the brain that are activated during exercise, suggesting that the activity of imaginary muscles is increased and resulting in increased muscle strength and speed [
12]. For this reason, motor imagery has been used to improve performance in athletes and promote functional recovery in patients at reduced burden and cost, without the need for exercise equipment or therapists [
13,
14]. In addition, since it can be done at home, it serves as an appropriate intervention in the elderly and patients who cannot participate in daily exercise programs [
15]. Multiple forms of motor imagery training exist. However, it is important to include familiar and task-oriented exercise in motor imagery training because the motor neurons are activated further by meaningful exercise-related tasks based on clear-cut goals and motivation [
16]. Motor imagery training combined with other therapeutic interventions enhances the recovery of daily living activities in the elderly [
17]. Zapparoli et al. reported that the patient’s damaged motor function was recovered by combining motor imagery training and physical therapy [
18].
Task-oriented training is based on motor behavior system theory and motor learning. It is an effective intervention in the field of rehabilitation medicine because it provides patients with the motivation to solve problems more actively via exercise programs that are focused on functional tasks rather than repeated and simple training movements. To maximize the effectiveness of task-oriented training, the form of the training task should be similar to that of a task seen in real-world situations, and it should be a meaningful and important task for the subjects. To this end, various forms, such as task-oriented circuit training and progressive resistance task-oriented training, are used as effective interventions in the field of rehabilitation medicine [
19,
20].
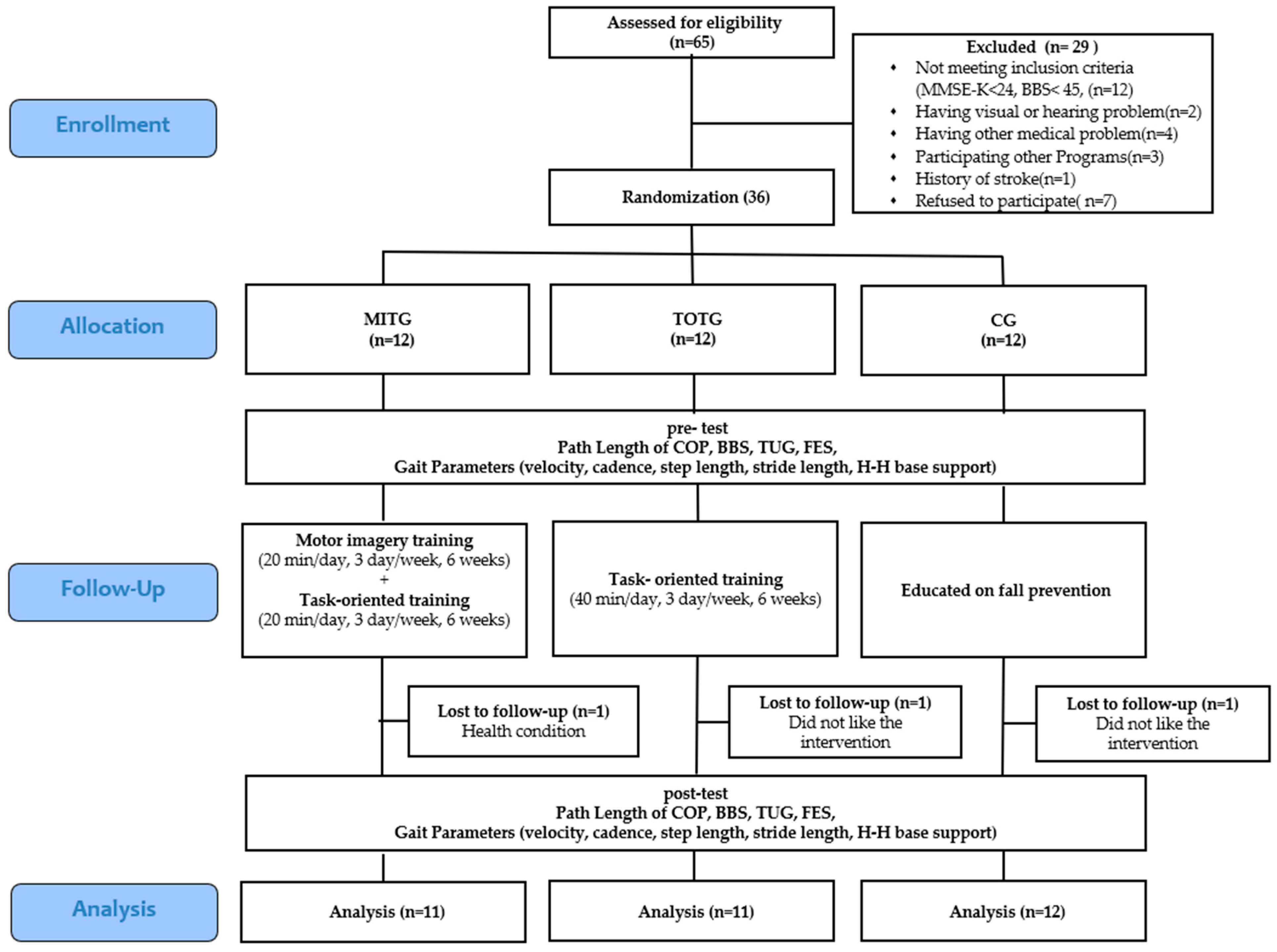
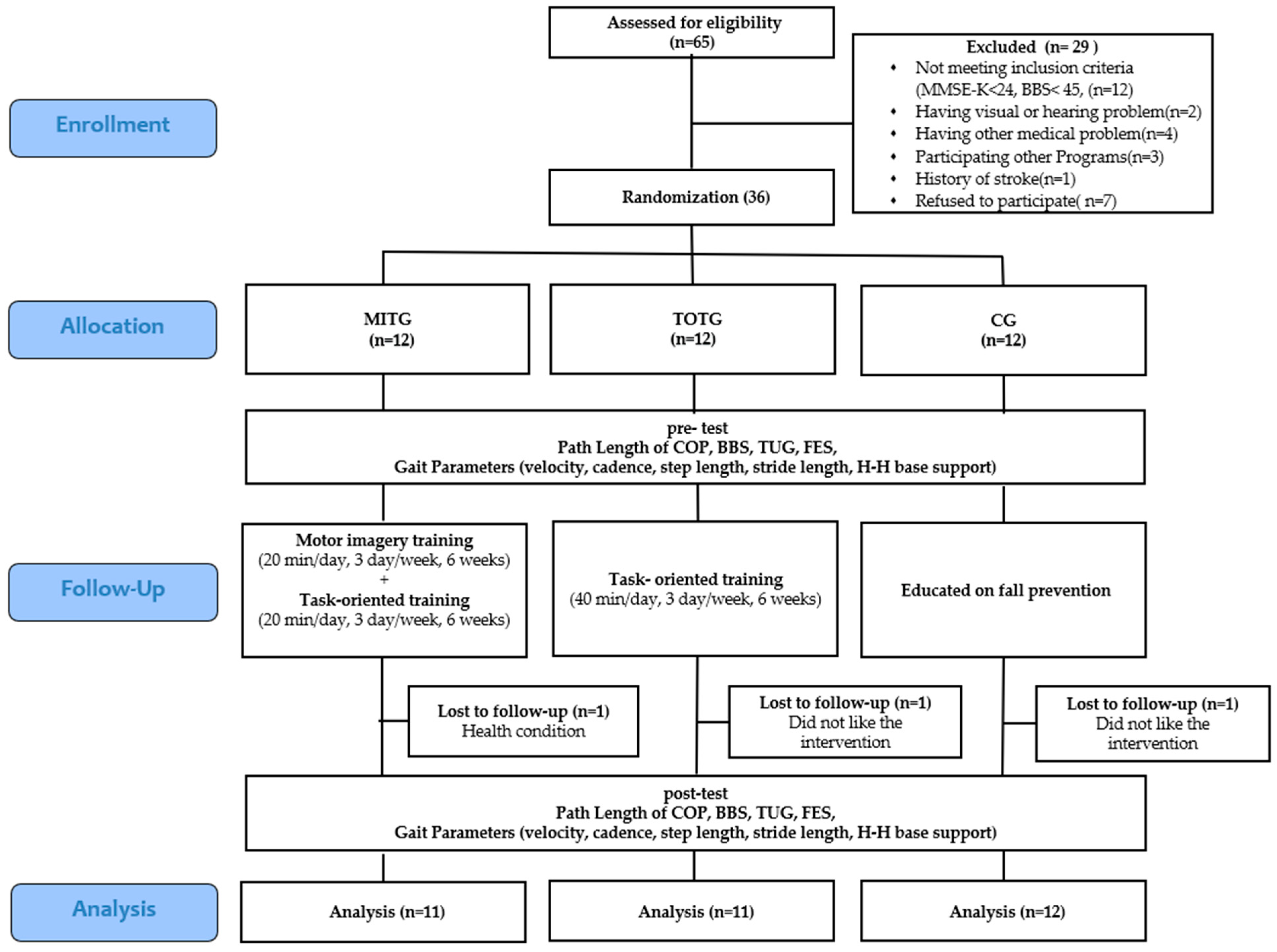
Thus, individual interventions via motor imagery training and task-oriented training are designed to improve balance and gait, respectively. However, most previous studies assessing these interventions involved athletes and patients rather than the elderly, and studies combining the two interventions to assess the risk of falls among the elderly have yet to be reported. Therefore, the purpose of this study was to evaluate the effect of these training on the balance and gait of the elderly after conducting motor imagery training combined with task-oriented training based on various real environments in which falls could occur to prevent falls.
4. Discussion
Motor imagery training is consistently reported to improve balance and gait in the elderly, and many studies have investigated falls in the elderly population. Thus, the current study conducted motor imagery training centered on activities of daily life that aimed to maintain balance and protect the body in the event of a fall in order to assess the effects of such training on balance and walking.
Malouin et al. stated that it is important to determine the extent to which subjects can concentrate on imagining movements because the quality of imagination during motor imagery training may differ across individuals [
29,
30]. This is an important factor that affects the outcome of motor imagery training. Several types of questionnaires that measure the ability to imagine have been developed for a variety of populations. Butler et al. tested whether the MIQ-RS, developed for healthy young adults, was valid for the elderly and stroke patients, and reported that it is useful for evaluating imagination among the elderly and stroke patients [
31]. Therefore, in this study, MIQ-RS was used to determine the extent to which subjects imagine or execute movements. The method includes a first-person perspective, in which the person imagines movement by changing the position of the joint angles to coincide with a given activity, and a third-person perspective, in which the person visualizes his/her movements from the viewpoint of others, similar to a movie [
32]. Dickstein and Deutsch stated that although the application of these viewpoints varies according to the task at hand, division of the two viewpoints may be academic and artificial [
33]. However, Fery argued that the third-person perspective may be effective in imitating forms for writing but applying the first-person viewpoint to the proprioceptive sense is more effective [
34]. A study in stroke patients conducted by Kim and Kim reported that the first-person point of view is more effective at enhancing balance than the third-person perspective [
35]. Therefore, in this study, since the nature of the task is appropriate for a first-person perspective, the subjects were requested to perform training accordingly.
On the Path Length of COP-based static balance test, the Path Length after intervention decreased more in MITG and TOTG than in the control group, indicating that the ability to balance was improved to a greater extent in the intervention groups. Similar results were obtained on the BBS test, which is designed to evaluate both static and dynamic balances. The TUG, which is another dynamic balance test used to assess rapidity, speed, and agility, also yielded similar results, which are consistent with Hosseini et al.’s findings in stroke patients [
36]. Haslinger et al. reported that application of task-oriented visual feedback training in the elderly improved the results of TUG [
37]. Liu et al. reported that, in an elderly population, muscle strength and daily activities were improved by a task-oriented exercise program, which coincides with the results of the present study; together, these findings suggest that task-oriented training not only improves balance in the elderly, but also interacts with motor imagery training to result in more positive effects [
38]. Whereas MITG and TOTG did not show different results on the static balance test, the group exposed to the combination of motor imagery training and task-oriented training showed more significant improvement than the group that performed only task-oriented training in the dynamic balance test. A study conducted by Shamsipour-Dehkordy et al. reported that combined motor imagery and physical training in the elderly produced more significant improvement in terms of static and dynamic balance than motor imagery training alone [
39]. Lee et al. reported that a group of stroke patients exposed to both functional training and motor imagery training showed significantly greater improvement in dynamic balance than a group who performed only functional training [
21]. These results are consistent with the results of the present study, indicating that motor imagery is more effective when used together with other interventions. However, according to Boraxbekk et al., neurological response tests in the elderly who learned a new task revealed that the group that combined functional movements with motor imagery showed no greater effect than the group exposed to a single intervention [
40]. This phenomenon was explained by activation of mainly the premotor cortex in the movement group and activation of the secondary visual cortex in the motor imagery training group, suggesting that the activities interfered with each other in the combined group, leading to decreased brain activation. Therefore, although motor imagery training has positive effects on balance and gait in the elderly, the results differ depending on the type of task and method used. It may be difficult to activate motor sensation in the elderly when the imaginary movements are identical to actual movements [
41], and the ability to learn and maintain new tasks may also decrease in an older population [
42]. However, activation of the cerebral visual cortex via imagery training generates muscle tension through voluntary or involuntary movements of the eyes and brain when an object moves or a sudden change in eye direction occurs [
43,
44]. Also, Mattay et al. stated that, during the elderly learning movement tasks based on visual information, the brain forms more neural networks bilaterally than are formed in younger learners [
44]. Therefore, motor imagery training has a positive effect on balance and gait. In addition, since the motor imagery training carried out in this study did not involve new tasks or tasks that included simple movements, but instead focused on tasks that were relatively familiar in daily life and were important in relation to falls, the participants’ motor imaging ability was strengthened to facilitate actual motor functions. In a study of motor imagery training combined with manual dexterity tasks, Ruffino et al. reported that motor ability was improved in the experimental compared to the control group [
45]. Based on a systematic review, Nicholson et al. showed that motor imagery training can be an alternative means of improving balance and gait in the elderly who do not have any neurological issues [
10].
The walking patterns of the elderly characteristically show reduced velocity, step length, and cadence, wide stride width, long stance phase, and short swing phase [
46]. In this study, the GAITRite system was used to evaluate the gait of the elderly participants based on temporospatial variables. The results revealed that both MITG and TOTG showed increased velocity and cadence, which are temporal variables, and step length and stride length, which are spatial variables, compared to the control group. The H-H base support was significantly decreased in MITG. Dunlap et al. reported that the elderly who experience falls show increased width between the two feet when walking in a new environment due to the fear of falling [
47]. The results of this study indicated that the H-H base support decreased the most in MITG, resulting in improved walking ability.
Scheffer et al. reported that elderly individuals who experience falls tend to decrease their physical activities due to their fear of falls, which reduces their motor functions, in turn leading to increased risk of falls [
48]. Therefore, in this study, Falls Efficacy Scale (FES) tests were conducted to examine changes in the fear of falls in the elderly. The results suggest that the fear of falls decreased the most in MITG, which is consistent with the results of a study conducted by Chung et al. [
49]. Kumar et al. reported that fall efficacy is closely related to balance and movement [
50]. Therefore, the improvements in balance and walking ability in this study positively affected fall efficacy, and the repetitive learning about falls via motor imagery training further reduced the fear of falls.
Thus, motor imagery and task-oriented training had a positive effect on static and dynamic balance, walking, and fall efficacy in the elderly. Motor imagery training combined with task-oriented training improved functional abilities more than the single intervention. However, there are several problems in interpreting the results of this study. First, because the number of subjects is small, it is difficult to generalize the results to the entire elderly population. Second, no previous studies reported task-oriented training combined with motor imagery training in the elderly. Third, this study failed to evaluate the duration of the learning effect of motor imagery training. Therefore, additional studies are needed to address these limitations.



{kind=link}