
Effect of Flexibility Training Associated with Multicomponent Training on Posture and Quality of Movement in Physically Inactive Older Women: A Randomized Study

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
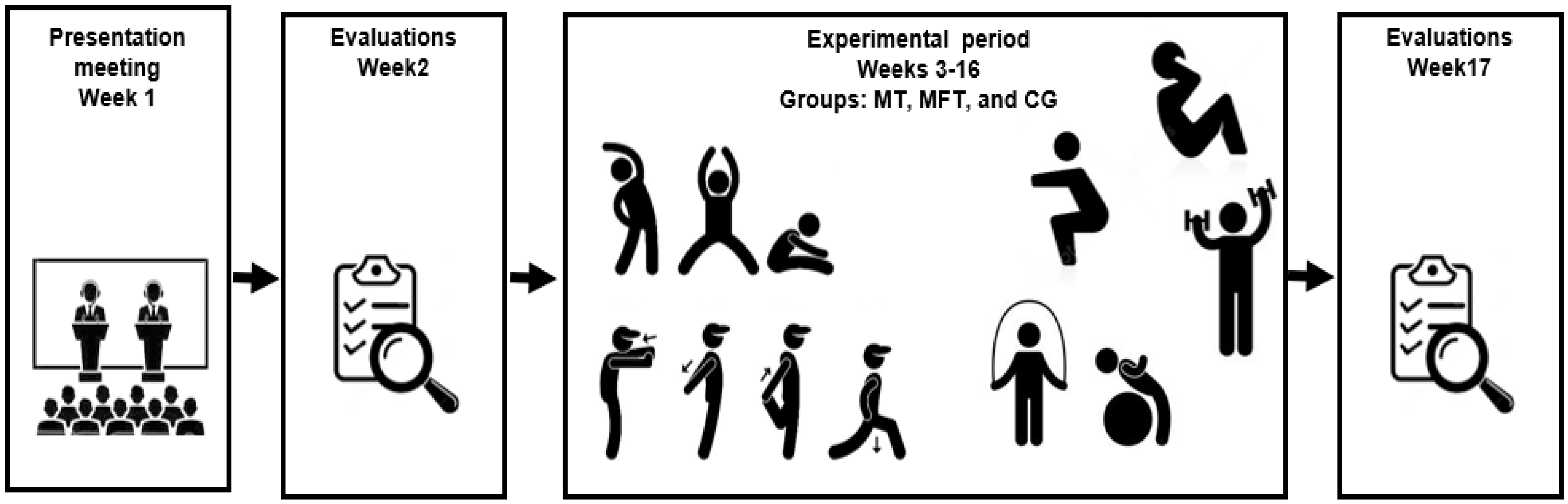
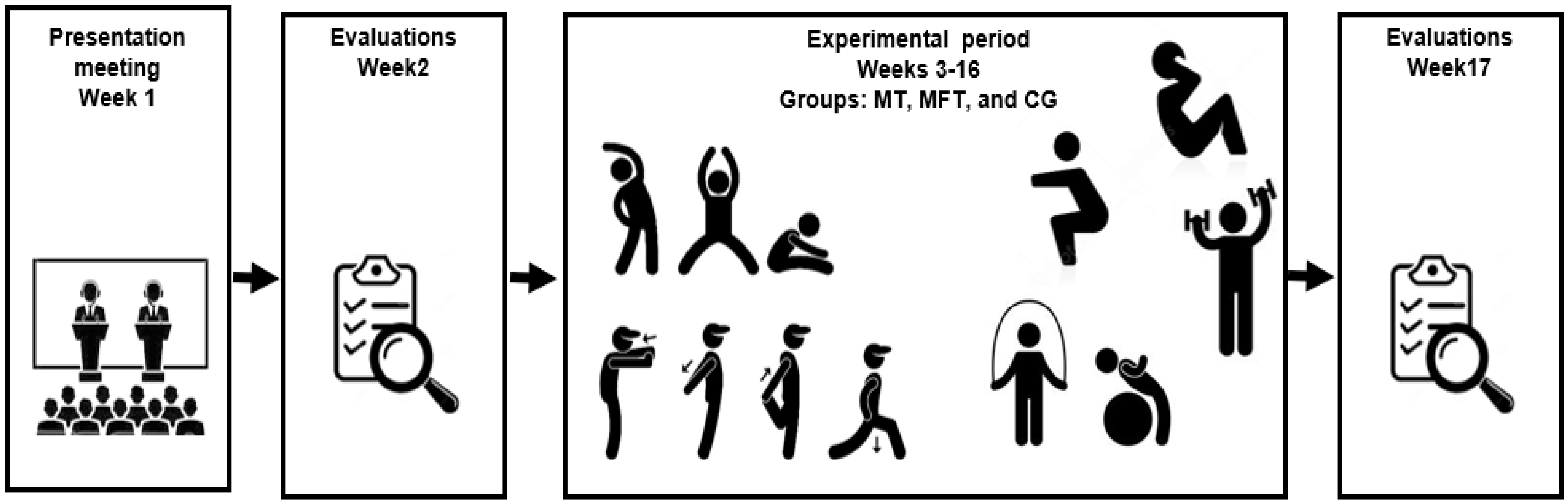
2.1. Study Design
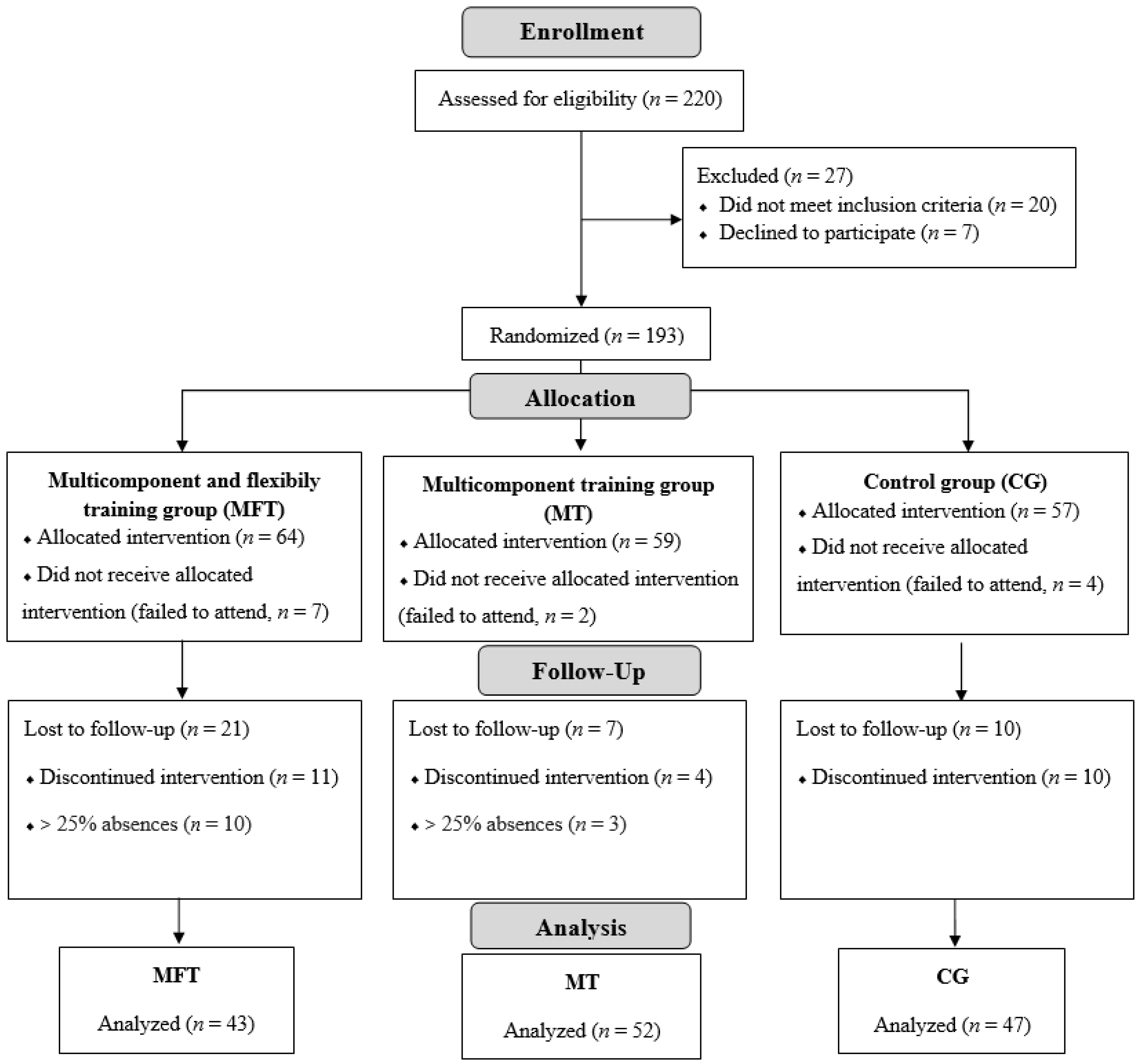
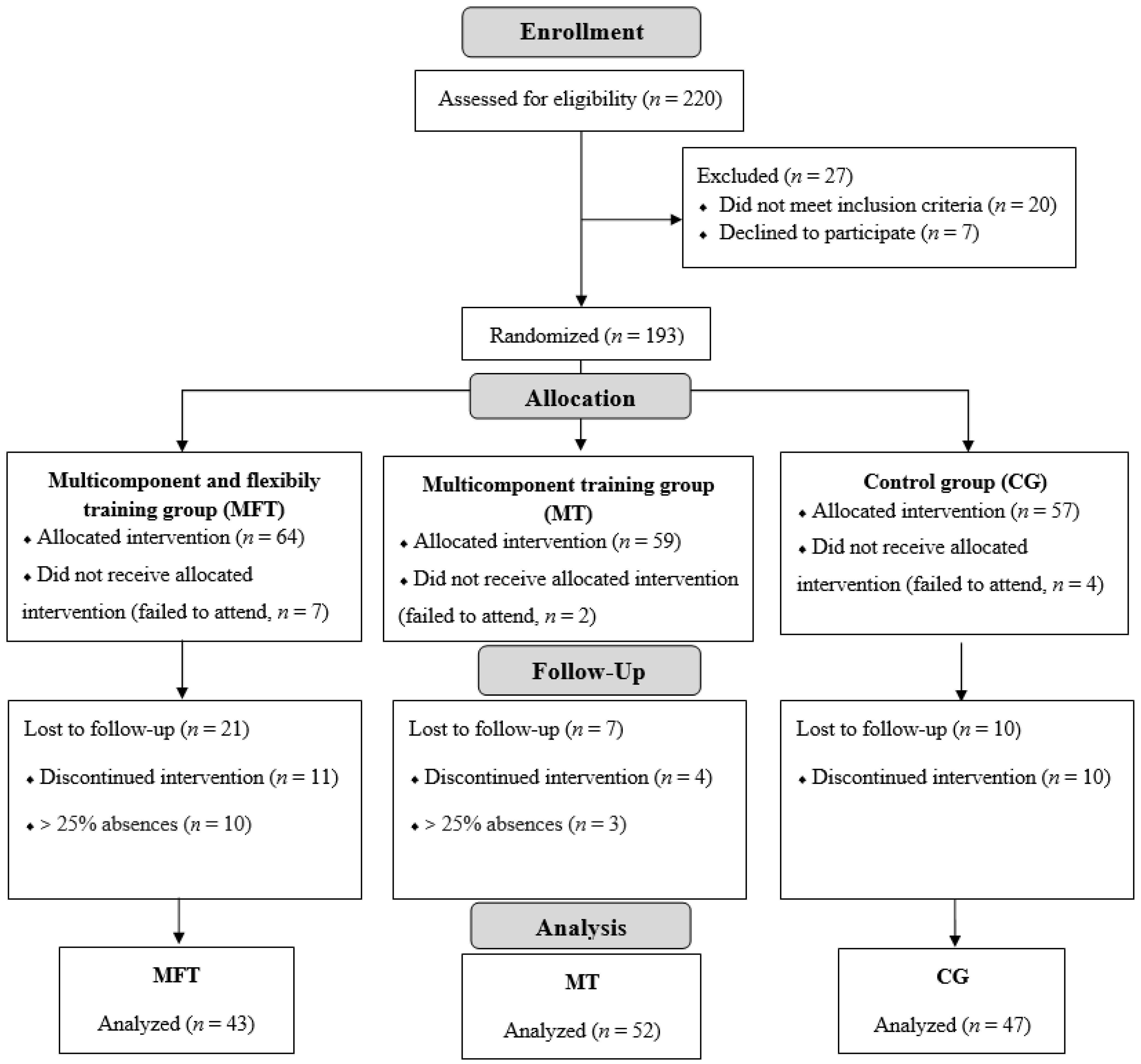
2.2. Participants
2.3. Interventions
2.3.1. Multicomponent Training
2.3.2. Individualized Flexibility Training
2.4. Evaluations
Motor Evaluations and Evaluative Instruments
2.5. Statistical Analysis
3. Results
4. Discussion
Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tavares, D.; Schlemer, G.B.V.; Turchiello, M.P.; dos Santos, J.C.; Pivetta, H.M.F.; Braz, M.M. Perfil da postural corporal estática em idosos: Revisão integrativa. An. Salão Inter. Ensino Pesq. Ext. 2018, 10, 1–4. [Google Scholar]
- Katzman, W.B.; Parimi, N.; Gladin, A.; Poltavskiy, E.A.; Schafer, A.L.; Long, R.K.; Fan, B.; Wong, S.S.; Lane, N.E. Sex differences in response to targeted kyphosis specific exercise and posture training in community-dwelling older adults: A randomized controlled trial. BMC Musculoskelet. Disord. 2017, 18, 509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geremia, J.M.; Iskiewicz, M.M.; Marschner, R.A.; Lehnen, T.E.; Lehnen, A.M. Effect of a physical training program using the Pilates method on flexibility in older adult’s participants. Age 2015, 37, 119–131. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, V.L.S.; Ribeiro, D.M.; Fernandes, L.C.; Menezes, R.L.D. Postural changes versus balance control and falls in community-living older adults: A systematic review. Fisioter. Mov. 2018, 31, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Daly, R.M.; Gianoudis, J.; Kersh, M.E.; Bailey, C.A.; Ebeling, P.R.; Krug, R.; Nowson, C.A.; Hill, K.; Sanders, K.M. Effects of a 12-month supervised, community-based, multimodal exercise program followed by a 6-month research-to-practice transition on bone mineral density, trabecular microarchitecture, and physical function in older adults: A randomized controlled trial. J. Bone Miner. Res. 2020, 35, 419–429. [Google Scholar] [CrossRef]
- Behm, D.G.; Cavanaugh, T.; Quigley, P.; Reid, J.C.; Nardi, P.S.; Marchetti, P.H. Acute bouts of upper and lower body static and dynamic stretching increase non-local joint range of motion. Eur. J. Appl. Physiol. 2016, 116, 241–249. [Google Scholar] [CrossRef]
- Queiroz, D.B.; Araújo, C.M.; Oliveira, L.C.; Novais, M.M.; Andrade, L.A.; Reis, L.A. Functionality, motor fitness, and health conditions in older adult’s people living in the home. Arq. Ciênc. Saúde 2016, 23, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Ueno, D.T.; Sebastião, E.; Corazza, D.I.; Gobbi, S. Methods for assessing physical activity: A systematic review focused on older adults. Rev. Bras. Cineantropom. Desempenho Hum. 2013, 15, 256–265. [Google Scholar]
- Cook, G.; Burton, L.; Kiesel, K. Movement: Functional Movement Systems: Screening, Assessment, and Corrective Strategies; On Target Publications: Santa Cruz, CA, USA, 2010; Volume 407, ISBN 978-1-931046-72-5. [Google Scholar]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Singh, M.A.F.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Rolland, Y.; Cesari, M.; Fielding, R.A.; Reginster, J.Y.; Vellas, B.; Cruz-Jentoft, A.J. Osteoporosis in Frail Older Adults: Recommendations for Research from the ICFSR Task Force 2020. J. Frailty Aging. 2021, 10, 168–175. [Google Scholar] [PubMed]
- Shariat, A.; Cleland, J.A.; Danaee, M.; Kargarfard, M.; Sangelaji, B.; Tamrin, S.B.M. Effects of stretching exercise training and ergonomic modifications on musculoskeletal discomforts of office workers: A randomized controlled trial. Braz. J. Phys. Ther. 2018, 22, 144–153. [Google Scholar] [CrossRef]
- D’Aurea, C.V.; Poyares, D.; Passos, G.S.; Santana, M.; Youngstedt, S.D.; Souza, A.A.; Bicudo, J.; Tufik, S.; de Mello, M.T. Effects of resistance exercise training and stretching on chronic insomnia. Braz J. Psychiatry 2019, 41, 51–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghasemi, E.; Khademi-Kalantari, K.; Khalkhali-Zavieh, M.; Rezasoltani, A.; Ghasemi, M.; Baghban, A.A.; Ghasemi, M. The effect of functional stretching exercises on neural and mechanical properties of the spastic medial gastrocnemius muscle in patients with chronic stroke: A randomized controlled trial. J. Stroke Cerebrovasc. Dis. 2018, 27, 1733–1742. [Google Scholar] [CrossRef] [PubMed]
- Trapé, A.A.; Lizzi, E.; Gonçalves, T.C.P.; Rodrigues, J.; Tavares, S.S.; Lacchini, R.; Pinheiro, L.C.; Ferreira, G.C.; Tanus-Santos, J.E.; Ovídio, P.P.; et al. Effect of multicomponent training on blood pressure, nitric oxide, redox status, and physical fitness in older adult women: Influence of endothelial nitric oxide synthase (NOS3) haplotypes. Oxid. Med. Cell Longev. 2017, 2017, 2578950. [Google Scholar] [CrossRef] [Green Version]
- Casas-Herrero, A.; Anton-Rodrigo, I.; Zambom-Ferraresi, F.; de Asteasu, M.L.S.; Martinez-Velilla, N.; Elexpuru-Estomba, J.; Ibañez, B. Effect of a multicomponent exercise programme (VIVIFRAIL) on functional capacity in frail community elders with cognitive decline: Study protocol for a randomized multicentre control trial. Trials 2019, 20, 362–374. [Google Scholar] [CrossRef]
- Suzuki, F.S.; Evangelist, A.L.; Teixeira, C.V.L.S.; Paunksnis, M.R.R.; Rica, R.L.; de Toledo Evangelista, R.A.G.; João, G.A.; Doro, M.R.; Sita, D.M.; Serra, A.J.; et al. Effects of a multicomponent exercise program on the functional fitness in older adult’s women. Rev. Bras. Med. Esporte. 2018, 24, 36–39. [Google Scholar] [CrossRef] [Green Version]
- Morton, S.K.; Whitehead, J.R.; Brinkert, R.H.; Caine, D.J. Resistance training vs. Static stretching: Effects on flexibility and strength. J. Strength. Cond. Res. 2011, 25, 3391–3398. [Google Scholar] [CrossRef] [Green Version]
- Souza, D.; Barbalho, M.; Vieira, C.A.; Martins, W.R.; Cadore, E.L.; Gentil, P. Minimal dose resistance training with elastic tubes promotes functional and cardiovascular benefits to older women. Exp. Gerontol. 2019, 115, 132–138. [Google Scholar] [CrossRef]
- Cadore, E.L.; Sáez de Asteasu, M.L.; Izquierdo, M. Multicomponent exercise and the hallmarks of frailty: Considerations on cognitive impairment and acute hospitalization. Exp. Gerontol. 2019, 122, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.A.V.; Noble, B.J. Perceived exertion. Exer. Sport Sci. Rev. 1974, 2, 131–153. [Google Scholar] [CrossRef]
- American College of Sports Medicine. Manual do ACSM Para Avaliação da Aptidão Física Relacionada à Saúde; Grupo Gen-Guanabara Koogan: Sao Paulo, Brazil, 2019. [Google Scholar]
- Mazo, G.Z.; Mota, J.; Benedetti, T.R.B.; Barros, M.V.G. Concurrent validity and reproducibility test-retest of the Modified Baecke Questionnaire for the older adults. Braz. J. Phys. Act. Health 2001, 6, 5–11. [Google Scholar]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibração do acelerômetro Computer Science and Applications. Med. Ciênci. Esp. Exerc. 1998, 30, 777–781. [Google Scholar]
- Rikli, R.E.; Jones, J.C. Teste de Aptidão Física Para Idosos; Manole: Barueri, Brazil, 2008. [Google Scholar]
- Barbosa, S.M. Estudo do equilíbrio em idosos através da fotogrametria computadorizada. Fisioter. Bras. 2016, 2, 189–196. [Google Scholar] [CrossRef]
- Porto, A.B.; Okazaki, V.H.A. Procedures of assessment on the quantification of thoracic kyphosis and lumbar lordosis by radiography and photogrammetry, A literature review. J. Bodyw. Mov. Ther. 2017, 21, 986–994. [Google Scholar] [CrossRef]
- McKay, M.J.; Baldwin, J.N.; Ferreira, P.; Simic, M.; Vanicek, N.; Burns, J. Normative reference values for strength and flexibility of 1000 children and adults. Neurology 2017, 88, 36–43. [Google Scholar] [CrossRef] [Green Version]
- Norkin, C.C.; White, D.J. Medida da Amplitude de Movimento Articular, um Guia Para Goniometria; FA Davis Co: Philadelphia, PA, USA, 1995. [Google Scholar]
- Leppink, J.; O’Sullivan, P.; Winston, K. Effect size—Large, medium, and small. Perspect. Med. Educ. 2016, 5, 347–349. [Google Scholar] [CrossRef] [Green Version]
- Wicke, J.; Gainey, K.; Figueroa, M. A comparison of self-administered proprioceptive neuromuscular facilitation to static stretching on range of motion and flexibility. J. Strength Cond. Res. 2014, 28, 168–172. [Google Scholar] [CrossRef] [Green Version]
- Medeiros, D.M.; Martini, T.F. Chronic effect of different types of stretching on ankle dorsiflexion range of motion: Systematic review and meta-analysis. Foot 2018, 34, 28–35. [Google Scholar] [CrossRef]
- Aslan, H.; Buddhadev, H.H.; Suprak, D.N.; San Juan, J.G. Acute effects of two hip flexor-stretching techniques on knee joint position sense and balance. Int. J. Sports Phys. Ther. 2018, 13, 846–859. [Google Scholar] [CrossRef]
- Kamonseki, D.H.; Gonçalves, G.A.; Yi, L.C.; Júnior, I.L. Effect of stretching with and without muscle strengthening exercises for the foot and hip in patients with plantar fasciitis: A randomized controlled single-blind. Clin. Trials J. 2016, 23, 76–82. [Google Scholar] [CrossRef]
- Hill, K.J.; Robinson, K.P.; Cuchna, J.W.; Hoch, M.C. Immediate effects of proprioceptive neuromuscular facilitation stretching programs compared with passive stretching programs for hamstring flexibility: A critically appraised topic. J. Sport Rehabil. 2017, 26, 567–572. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, U.H.; Johnson, A.W.; Vehrs, P.R.; Feland, J.B.; Hilton, S.C. Performance on the functional movement screen in older active adults. J. Sport Health Sci. 2016, 5, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Perry, F.T.; Koehle, M.S. Normative data for the functional movement screen in middle-aged adults. J. Strength Cond. Res. 2013, 27, 458–462. [Google Scholar] [CrossRef] [Green Version]
- Bandeira, F.M.; Delfino, F.C.; Carvalho, G.A.; Valduga, R. Comparison of thoracic kyphosis between sedentary and physically active older adults by the flexicurve method. Braz. J. Kinathrop. Hum. Perform. 2010, 12, 381–386. [Google Scholar] [CrossRef] [Green Version]
- Costa, G.C.; Corrêa, J.C.F.; Silva, S.M.; Corso, S.D.; Da Cruz, S.F.; Cunha, M.D.S.; Souza, P.H.L.; Saldanha, M.L.; Corrêa, F.I. Effect of transcranial direct current stimulation and multicomponent training on functional capacity in older adults: Protocol for a randomized, controlled, double-blind clinical trial. Trials 2020, 21, 203. [Google Scholar] [CrossRef]
- Ishikawa, Y.; Miyakoshi, N.; Hongo, M.; Kasukawa, Y.; Kudo, D.; Shimada, Y. Relationships among spinal mobility and sagittal alignment of spine and lower extremity to quality of life and risk of falls. Gait. Posture 2017, 53, 98–103. [Google Scholar] [CrossRef]
- Ishikawa, Y.; Miyakoshi, N.; Kasukawa, Y.; Hongo, M.; Shimada, Y. Spinal curvature and postural balance in patients with osteoporosis. Osteoporos Int. 2009, 20, 2049–2053. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, K.; Kawano, H.; Gando, Y.; Iemitsu, M.; Murakami, H.; Sanada, K.; Tanimoto, M.; Ohmori, Y.; Higuchi, M.; Tabata, I.; et al. Poor trunk flexibility is associated with arterial stiffening. Am. J. Physiol. Heart Circ. Physiol. 2009, 297, H1314–H1318. [Google Scholar] [CrossRef] [Green Version]
- Nishiwaki, M.; Kurobe, K.; Kiuchi, A.; Nakamura, T.; Matsumoto, N. Sex differences in flexibility-arterial stiffness relationship and its application for diagnosis of arterial stiffening: A cross-sectional observational study. PLoS ONE 2014, 9, e113646. [Google Scholar] [CrossRef]
- Nishiwaki, M.; Yonemura, H.; Kurobe, K.; Matsumoto, N. Four weeks of regular static stretching reduces arterial stiffness in middle-aged men. Springerplus 2015, 4, 555. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Level 1 | Level 2 | Level 3 | Level 4 | |
|---|---|---|---|---|
| Week of intervention | 1–2 | 3–6 | 7–10 | 11–14 |
| Duration of session | 20′ | 30′ | 40′ | 50′ |
| Time under tension | 10″ | 15″ | 20″ | 25″ |
| Interval between series | 10″ | 15″ | 20″ | 25″ |
| Series per exercise | 2 | 3 | 4 | 5 |
| Pain level * | 1 a 3 | 2 a 4 | 4 a 6 | 6 a 8 |
| Exercises per body region $ | 2 | 3 | 3 | 4 |
| Weekly dose # | 2400″ | 3600″ | 4800″ | 6000″ |
| MT (n = 52) | MFT (n = 43) | CG (n = 47) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Effect Size | Pre | Post | Effect Size | Pre | Post | Effect Size | |
| Age (years) | 63.1 ± 5.5 | 63.4 ± 5.6 | 64.0±4.9 | ||||||
| Last menstrual cycle (years) | 47.5 ± 6.3 | 48.1 ± 5.8 | 48.0 ± 6.2 | ||||||
| Height (m) | 1.56 ± 7.0 | 1.59 ± 6.9 | 1.58 ± 7.80 | ||||||
| Body mass (kg) ‡ | 75.1 ± 14.4 | 73.8 ± 12.8 | −0.096 | 74.7 ± 16.0 | 72.1 ± 15.8 | −0.164 | 76.1 ± 18.8 | 79.3 ± 10.0 | 0.222 |
| BMI (kg/m2) † | 29.4 ± 5.0 | 29.2 ± 4.7 | −0.041 | 28.4 ± 4.7 | 27.9 ± 5.3 | −0.100 | 25.3 ± 2.7 | 28.4 ± 4.1 $,#,* | 0.912 |
| SBP (mmHg) † | 131.9 ± 21.3 | 129.0 ± 10.2 | −0.184 | 129.2 ± 18.8 | 123.5 ± 15.4 * | −0.333 | 135.6 ± 17.9 | 136.5 ± 12.4 # | 0.059 |
| DBP (mmHg) † | 76.8 ± 10.6 | 76.8 ± 8.3 | 0.000 | 76.6 ± 10.6 | 71.9 ± 10.0 | −0.456 | 73.8 ± 10.1 | 79.1 ± 6.3 #,* | 0.646 |
| WC (cm) † | 100.5 ± 11.3 | 100.1 ± 9.2 | −0.039 | 96.8 ± 12.0 | 94.3 ± 12.1 $ | −0.207 | 97.4 ± 12.9 | 98.2 ± 9.9 $ | 0.070 |
| HC (cm) | 107.5 ± 12.3 | 106.1 ± 9.2 | −0.130 | 106.1 ± 9.7 | 105.1 ± 10.5 | −0.099 | 107.0 ± 10.7 | 104.6 ± 9.2 | −0.241 |
| BF (%) † | 41.2 ± 8.1 | 40.1 ± 6.8 | −0.148 | 46.2 ± 6.9 | 35.8 ± 7.9 *,$ | −1.405 | 43.1 ± 6.9 | 46.3 ± 6.7 $,#,* | 0.471 |
| MBQE (scores) ‡ | 6.9 ± 5.3 | 11.7 ± 7.5 | 0.750 | 6.3 ± 5.4 | 12.6 ± 5.0 | 1.212 | 6.4 ± 5.0 | 8.6 ± 7.6 | 0.349 |
| PA (accelerometer, counts) † | 382 ± 1361 | 877 ± 401 * | 0.562 | 386 ± 176 | 961 ± 401 *,$ | 1.993 | 348 ± 171 | 592 ± 365 # | 0.911 |
| MT (n = 52) | MFT (n = 43) | CG (n = 47) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Effect Size | Pre | Post | Effect Size | Pre | Post | Effect Size | |
| Hands behind the back (cm) | −9.5 ± 9.7 | −7.6 ± 9.6 | 0.197 | −5.0 ± 11.8 | −4.1 ± 9.2 | 0.086 | −7.6 ± 10.9 | −7.8 ± 11.9 | −0.018 |
| Sit and reach (cm) ‡ | −3.1 ± 8.8 | 2.0 ± 7.6 | 0.626 | 1.1 ± 9.9 | 3.3 ± 10.0 | 0.213 | −1.9 ± 7.9 | −2.5 ± 4.9 | −0.094 |
| Goniometry (°) | |||||||||
| Cervical extension † | 14.2 ± 5.4(38) | 15.7 ± 6.8 * | 0.246 | 15.7 ± 7.6(46) | 18.3 ± 7.5 * | 0.344 | 12.6 ± 6.4(47) | 12.6 ± 7.7 # | 0.000 |
| Cervical flexion † | 34.9 ± 14.4(38) | 36.6 ± 14.8 | 0.116 | 33.8 ± 12.1(46) | 37.3 ± 13.2 * | 0.277 | 31.4 ± 12.0(47) | 30.6 ± 11.8 *,#,$ | −0.067 |
| Shoulder extension ‡ | 30.3 ± 8.3 | 30.6 ± 8.6 | 0.036 | 30.4 ± 9.2 | 31.6 ±10.2 | 0.124 | 27.1 ± 9.7 | 30.2 ± 8.7 | 0.337 |
| Shoulder flexion † | 156.8 ± 19.4 | 156.9 ± 21.6 | 0.005 | 146.7 ± 18.2 | 148.4 ± 21.0 * | 0.087 | 137.6 ± 29.9 | 141.3 ± 30.0 *,# | −0.124 |
| Lumbar extension † | 15.5 ± 7.3 | 16.8 ± 8.3 | 0.167 | 16.7 ± 9.6 | 19.4 ± 10.6 *,$ | 0.267 | 16.6 ± 7.7 | 19.6 ± 8.6 *,$ | 0.368 |
| Lumbar flexion † | 73.2 ± 10.1 | 73.3 ± 9.9 | 0.010 | 75.7 ± 9.6 | 77.7 ± 11.4 *,$ | 0.190 | 74.3 ± 11.3 | 78.6 ± 11.2 *,$ | 0.382 |
| Hip extension † | 4.7 ± 1.7(38) | 5.8 ± 3.9 * | 0.393 | 4.5 ± 1.8(40) | 6.9 ± 1.8 * | 1.333 | 12.6 ± 6.4(47) | 12.6 ± 7.7 $,# | 0.000 |
| Hip flexion † | 58.0 ± 17.2(38) | 69.2 ± 17.4 * | 0.647 | 62.4 ± 10.3(40) | 71.1 ± 10.0 * | 0.857 | 31.4 ± 12.0(47) | 30.6 ± 11.8 $,# | −0.067 |
| Knee extension ‡ | 87.7 ± 20.8 | 86.9 ± 20.4 | −0.039 | 93. 8 ± 20.4 | 96.5 ± 19.1 | 0.137 | 94.8 ± 16.3 | 96.1 ± 19.2 | 0.073 |
| Knee flexion ‡ | 87.7 ± 20.8 | 86.9 ± 20.4 | −0.039 | 93.8 ± 20.4 | 96.5 ± 19.1 | 0.137 | 94.8 ± 16.3 | 96.1 ± 19.2 | 0.073 |
| Ankle extension † | 8.7 ± 3.2(38) | 9.7 ± 4.8 * | 0.250 | 9.6 ± 2.9(47) | 12.8 ± 3.1 *,$ | 1.067 | 8.7 ± 2.9(47) | 7.2 ± 3.7 $, | −0.455 |
| Ankle flexion † | 18.8 ± 7.6(38) | 21.5 ± 7.7 * | 0.353 | 17.5 ± 7.9(47) | 21.9 ± 8.0 * | 0.553 | 19.4 ± 7.7(47) | 19.9 ± 8.3 | 0.063 |
| Functional movement screen (scores) † | 16.6 ± 3.4 | 19.9 ± 3.9 * | 0.904 | 15.9 ± 3.7 | 18.8 ± 5.3 * | 0.644 | 16.2 ± 3.7 | 16.8 ± 4.3 $, | 0.150 |
| Postural Evaluation | MT | MFT | CG |
|---|---|---|---|
| Anterior view | |||
| Head | ⊗ | ⊗ | ⊗ |
| Torso | ⊗⊗⊗ | ⊗⊗⊝ | ⊗⊗⊗ |
| Lower limbs | ⊗⊗⊗⊗⊗⊗ | ⊗⊗⊗⊝⊝⊝ | ⊗⊗⊗⊗⊗⊗ |
| Posterior view | |||
| Torso | ⊗ | ⊗ | ⊗ |
| Lower limbs | ⊗⊗ | ⊗⊝ | ⊗⊝ |
| Right lateral view | |||
| Head | ⊗⊗ | ⊗⊝ | ⊗⊝ |
| Torso | ⊗⊗⊗⊗ | ⊗⊗⊝⊝ | ⊗⊗⊗⊝ |
| Lower limbs | ⊗⊗ | ⊗⊝ | ⊗⊗ |
| Left lateral view | |||
| Head | ⊗⊝ | ⊗⊝ | ⊗⊗ |
| Torso | ⊗⊗⊗⊗ | ⊗⊗⊝⊝ | ⊗⊗⊝⊝ |
| Lower limbs | ⊗⊝ | ⊝⊝ | ⊗⊗ |
| Asymmetries | |||
| Frontal and sagittal planes | ⊗⊝ | ⊝⊝ | ⊗⊗ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sobrinho, A.C.d.S.; Almeida, M.L.d.; Rodrigues, G.d.S.; Finzeto, L.C.; Silva, V.R.R.; Bernatti, R.F.; Bueno Junior, C.R. Effect of Flexibility Training Associated with Multicomponent Training on Posture and Quality of Movement in Physically Inactive Older Women: A Randomized Study. Int. J. Environ. Res. Public Health 2021, 18, 10709. https://doi.org/10.3390/ijerph182010709
Sobrinho ACdS, Almeida MLd, Rodrigues GdS, Finzeto LC, Silva VRR, Bernatti RF, Bueno Junior CR. Effect of Flexibility Training Associated with Multicomponent Training on Posture and Quality of Movement in Physically Inactive Older Women: A Randomized Study. International Journal of Environmental Research and Public Health. 2021; 18(20):10709. https://doi.org/10.3390/ijerph182010709
Chicago/Turabian StyleSobrinho, Andressa Crystine da Silva, Mariana Luciano de Almeida, Guilherme da Silva Rodrigues, Larissa Chacon Finzeto, Vagner Ramon Rodrigues Silva, Rodrigo Fenner Bernatti, and Carlos Roberto Bueno Junior. 2021. "Effect of Flexibility Training Associated with Multicomponent Training on Posture and Quality of Movement in Physically Inactive Older Women: A Randomized Study" International Journal of Environmental Research and Public Health 18, no. 20: 10709. https://doi.org/10.3390/ijerph182010709
APA StyleSobrinho, A. C. d. S., Almeida, M. L. d., Rodrigues, G. d. S., Finzeto, L. C., Silva, V. R. R., Bernatti, R. F., & Bueno Junior, C. R. (2021). Effect of Flexibility Training Associated with Multicomponent Training on Posture and Quality of Movement in Physically Inactive Older Women: A Randomized Study. International Journal of Environmental Research and Public Health, 18(20), 10709. https://doi.org/10.3390/ijerph182010709