
Translation, Adaptation, and Validation of the L’Échelle d’Interactions Infirmière-Patient-23 for the Portuguese Culture: The Multidimensional Nature of Nursing Care


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection and Procedure
Participants
2.3. Data Collection Instrument
2.4. Ethical Considerations
3. Results
3.1. Exploratory Factor Analysis
3.2. Reliability Analysis
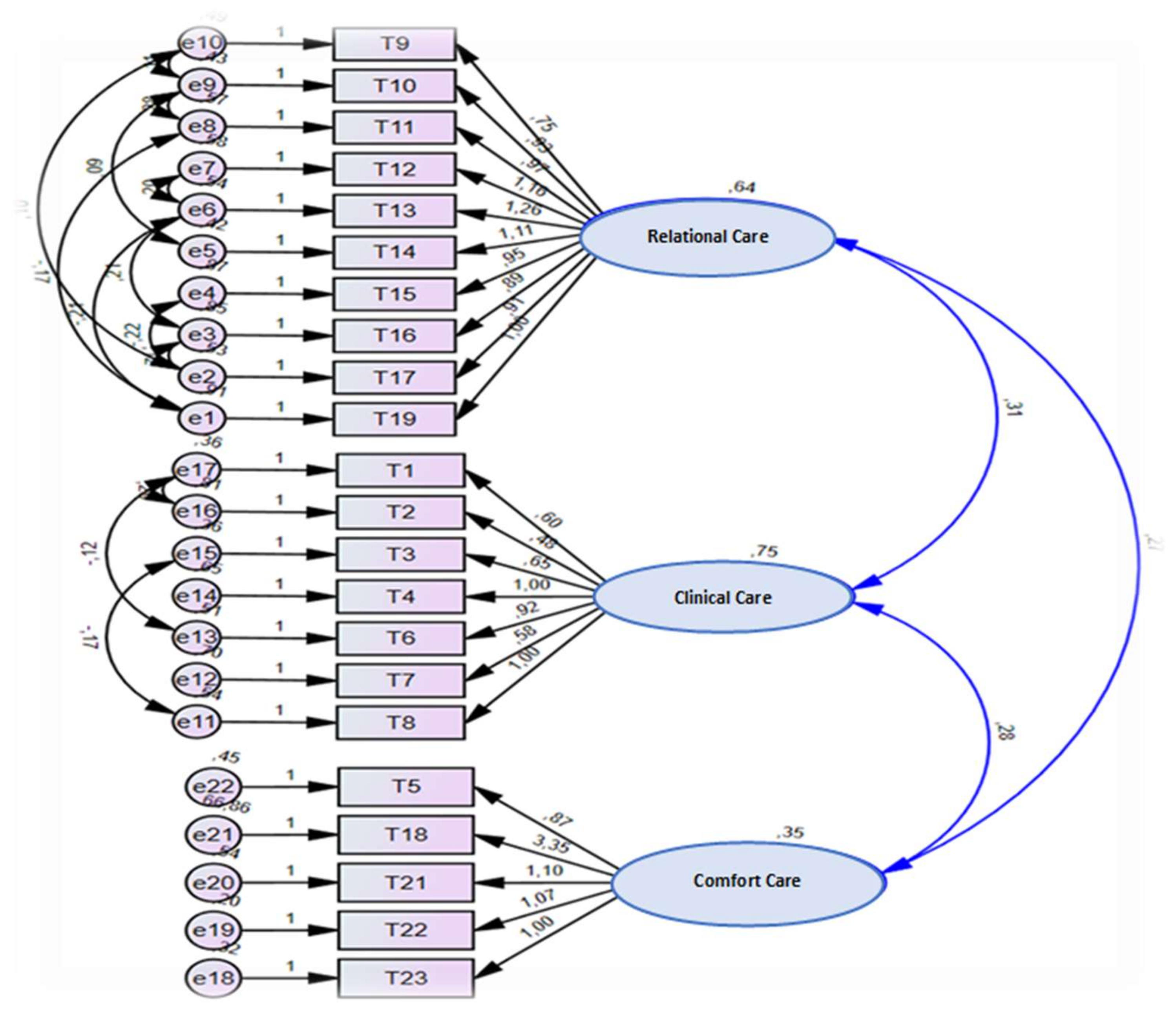
3.3. Confirmatory Factor Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cossette, S.; Pepin, J.; Fontaine, G. Caring Nurse-Patient Interactions Scale. In Assessing and Measuring Caring in Nursing and Health Sciences, 3rd ed.; Sitzman, K.L., Watson, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2019; pp. 251–270. [Google Scholar] [CrossRef]
- Hovenga, E.J.S.; Lowe, C. Measuring Capacity to Care Using Nursing Data; Elsevier: St. Louis, MO, USA, 2020. [Google Scholar]
- Kol, E.; Arıkan, F.; İlaslan, E.; Akıncı, M.A.; Koçak, M.C. A quality indicator for the evaluation of nursing care: Determination of patient satisfaction and related 200 factors at a university hospital in the Mediterranean Region in Turkey. Collegian 2018, 25, 51–56. [Google Scholar] [CrossRef]
- Karaca, A.; Durna, Z. Patient satisfaction with the quality of nursing care. Nurs. Open 2019, 6, 535–545. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, F.; Kuznier, T.P.; Sousa, C.C.; Chianca, T.C.M. Aspectos Teóricos e Metodológicos para Adaptação Cutural e Validação de Instrumentos na Enfermagem. Texto Contexto Enferm. 2018, 27, e4900016. [Google Scholar] [CrossRef] [Green Version]
- Silva, L.F.; Costa, G.R. Estratégias utilizadas para a avaliação da qualidade da assistência de enfermagem: Revisão Integrativa. Res. Soc. Dev. 2021, 10, e45310212679. [Google Scholar] [CrossRef]
- Cossette, S.; Cote, J.K.; Pepin, J.; Ricard, N.; D’Aoust, L.X. A dimensional structure of nurse-patient interactions from a caring perspective: Refinement of the Caring Nurse-Patient Interaction Scale (CNPI-Short Scale). J. Adv. Nur. 2006, 55, 198–214. [Google Scholar] [CrossRef] [PubMed]
- Genet, G.; Lheureux, F.; Truchot, D. La relation soignant–soigné dans la littérature académique: Tendances générales, limites et perspectives futures. Ann. Med. Psychol. Rev. Psych. 2018, 176, 135–144. [Google Scholar] [CrossRef]
- Cossette, S. Guide D’utilisation Échelle D’interactions Infirmière Patient (EIIP-70) (EIIP-23); Faculté des Sciences Infirmières, Université de Montréal: Montreal, QC, Canada, 2015; p. 40. [Google Scholar]
- Lecocq, D.; Delmas, P.; Antonini, M.; Lefebvre, H.; Laloux, M.; Beghuin, A.; Cutsem, V.A.; Pirson, M. Comparing feeling of competence regarding humanistic caring in Belgian nurses and nursing students: A comparative cross-sectional study conducted in a French Belgian teaching hospital. Nurs. Open 2021, 8, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Coates, C.J. Caring Efficacy Scale. In Assessing and Measuring Caring in Nursing and Health Sciences, 3rd ed.; Springer: Berlin/Heidelberg, Germany, 2019; pp. 165–171. [Google Scholar] [CrossRef]
- Brousseau, S.; Cara, C.M.; Blais, R. A humanistic caring quality of work life model in nursing administration based on Watson’s Philosophy. Int. J. Hum. Caring 2017, 21, 2–8. [Google Scholar] [CrossRef]
- Cossette, S.; Pépin, J.; Côté, J.K.; Courval, F.P. The multidimensionality of caring: A confirmatory factor analysis of the Caring Nurse-Patient Interaction Short Scale. J. Adv. Nurs. 2008, 61, 699–710. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.L.; Ruan, H.; Xiang, X.J.; Jia, Q. Investigation and analysis of the caring attitude and behaviour of nurses in Shanghai, China. Int. J. Nurs. Pract. 2015, 21, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Im, S.B.; Cho, M.K.; Heo, M. Validity and reliability of the Korean version of the Watson Caritas Patient Score. J. Nurs. Res. 2019, 28, e80. [Google Scholar] [CrossRef] [PubMed]
- Calong, A.K.; Soriano, P.G. Construct Validity and Reliability of Caring Nurse Patient Interaction Scale Nurse among Filipino Nurses. Int. J. Caring Sci. 2019, 12, 1017. [Google Scholar]
- Sharour, A. Translation and Validation of the Arabic Version of the Caring Nurse-Patient Interaction Scale–Patient Version (CNPI-23P). Cancar Nurs. 2021, 44, E62–E67. [Google Scholar] [CrossRef]
- Beaton, D.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Recommendations for the cross-cultural adaptation of the DASH & QuickDASH outcome measures. Inst. Work Health 2007, 1, 1–45. [Google Scholar]
- Gray, J.R.; Grove, S.K. The Practice of Nursing research: Appraisal, Synthesis and Generation of Evidence, 9th ed.; Elsevier: St. Louis, MO, USA, 2021. [Google Scholar]
- Almeida, S. Estatística Aplicada em Investigação em Ciências da Saúde—um Guia com SPSS; Loures: Lusodidacta, Portugal, 2017. [Google Scholar]
- Marôco, J. Análise Estatística com o SPSS Statistics, 7th ed.; Pêro Pinheiro: Sintra, Portugal, 2018. [Google Scholar]
- Atar, Y.A.; Asti, A.T. Validity and Reliability of Turkish Version of the Caring Nurse-Patient Interaction Scale. Florence Nightingale Hemşir Dergisi. 2012, 20, 129–139. [Google Scholar]

{kind=link}
| Items | Components | ||
|---|---|---|---|
| 1 Relational Care | 2 Clinical Care | 3 Comfort Care | |
| Item 9 | 0.699 | - | - |
| Item 10 | 0.851 | - | - |
| Item 11 | 0.799 | - | - |
| Item 12 | 0.802 | - | - |
| Item 13 | 0.831 | - | - |
| Item 14 | 0.840 | - | - |
| Item 15 | 0.662 | - | - |
| Item 16 | 0.530 | - | - |
| Item 17 | 0.608 | - | - |
| Item 19 | 0.470 | - | - |
| Item 1 | - | 0.651 | - |
| Item 2 | - | 0.475 | - |
| Item 3 | - | 0.729 | - |
| Item 4 | - | 0.768 | - |
| Item 6 | - | 0.825 | - |
| Item 7 | - | 0.494 | - |
| Item 8 | - | 0.698 | - |
| Item 5 | - | - | 0.595 |
| Item 18 | 0.590 | ||
| Item 21 | - | - | 0.733 |
| Item 22 | - | - | 0.688 |
| Item 23 | - | - | 0.543 |
| Explained Variance | 70.183 | 24.433 | 90.219 |
| Cronbach’s Alpha | 0.910 | 0.827 | 0.745 |
| Components | Alpha | AVE |
|---|---|---|
| 1. Relational Care | 0.910 | 0.52 |
| 2. Clinical Care | 0.827 | 0.46 |
| 3. Comfort Care | 0.745 | 0.41 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agostinho, P.; Gaspar, F.; Potra, T. Translation, Adaptation, and Validation of the L’Échelle d’Interactions Infirmière-Patient-23 for the Portuguese Culture: The Multidimensional Nature of Nursing Care. Int. J. Environ. Res. Public Health 2021, 18, 10791. https://doi.org/10.3390/ijerph182010791
Agostinho P, Gaspar F, Potra T. Translation, Adaptation, and Validation of the L’Échelle d’Interactions Infirmière-Patient-23 for the Portuguese Culture: The Multidimensional Nature of Nursing Care. International Journal of Environmental Research and Public Health. 2021; 18(20):10791. https://doi.org/10.3390/ijerph182010791
Chicago/Turabian StyleAgostinho, Paula, Filomena Gaspar, and Teresa Potra. 2021. "Translation, Adaptation, and Validation of the L’Échelle d’Interactions Infirmière-Patient-23 for the Portuguese Culture: The Multidimensional Nature of Nursing Care" International Journal of Environmental Research and Public Health 18, no. 20: 10791. https://doi.org/10.3390/ijerph182010791