
Cardiovascular Disease Recognition Based on Heartbeat Segmentation and Selection Process


Abstract
:1. Introduction
Contributions
2. Related Work
2.1. PCG Signal Preprocessing, Denoising, and Enhancing
2.2. PCG Signal Segmentation
2.3. PCG Signal Feature Extraction and Classification
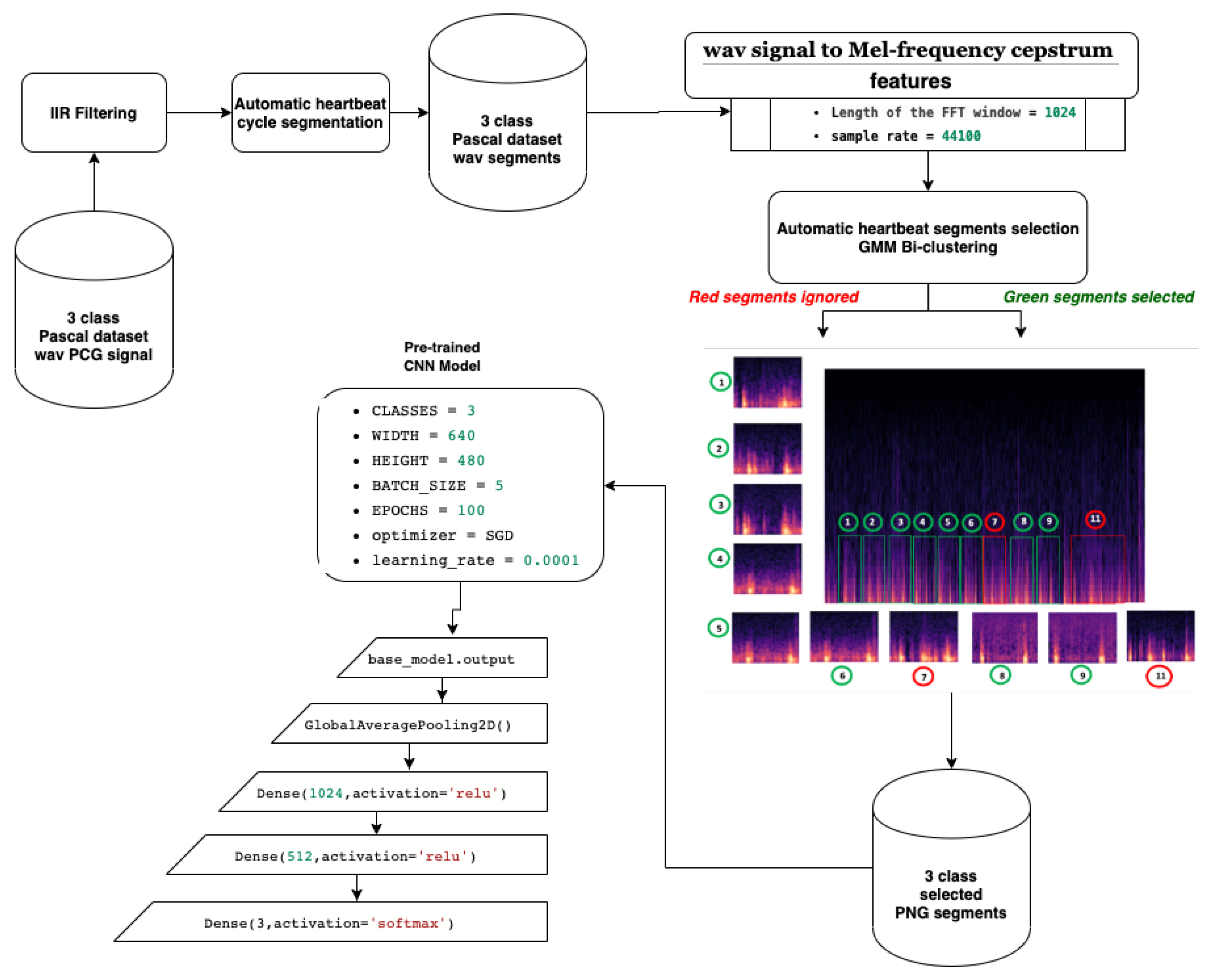
3. The Proposed Model
3.1. Preprocessing
3.1.1. Noise Filtering
3.1.2. Automatic Heart Cycle Segmentation
3.1.3. Mel-Frequency Spectrum Images
- By performing a Hamming windowing at fixed interval of 1024 (in our case), the PCG signal is divided into acoustic chunks. The outcome of this step is a vector representing the cepstal features related to each chunks.
- Applying discrete Fourier transform (DFT) to each window chunk.
- For each DFT chunk, it retains only the amplitude spectrum logarithm to conserve the signal loudness property, which was found to be approximately logarithmic.
- To obtain essential frequency features, MFCC technique is based on spectrum smoothing process.
- By applying discrete cosine transform to the fourth step output, we obtain the MFCC features of our PCG signal.
3.1.4. Segment Selection by Clustering
- -
- Step 1: Parameter initialization
- -
- Step 2: Repeat until convergence
- •
- Estimation step: calculation of conditional probabilities that the sample i comes from the Gaussian k. with : the set of Gaussians.
- •
- Maximization step: update settings and , ,
3.2. CNN Classification
4. Performance Evaluation
4.1. Experimental Setup
4.2. Dataset
5. Results and Discussion
6. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. World Health Ranking; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Wilkins, E.; Wilson, L.; Wickramasinghe, K.; Bhatnagar, P.; Leal, J.; Luengo-Fernandez, R.; Burns, R.; Rayner, M.; Townsend, N. European Cardiovascular Disease Statistics 2017; European Heart Network: Brussel, Belgium, 2017. [Google Scholar]
- Lloyd-Jones, D.; Adams, R.; Brown, T.; Carnethon, M.; Dai, S.; De Simone, G.; Ferguson, T.; Ford, E.; Furie, K.; Gillespie, C.; et al. Heart disease and stroke statistics—2010 update: A report from the American Heart Association. Circulation 2010, 121, e46. [Google Scholar]
- Latif, S.; Khan, M.Y.; Qayyum, A.; Qadir, J.; Usman, M.; Ali, S.M.; Abbasi, Q.H.; Imran, M. Mobile technologies for managing non-communicable-diseases in developing countries. In Mobile Applications and Solutions for Social Inclusion; Paiva, S., Ed.; IGI Global: Hershey, PA, USA, 2018; pp. 261–287. [Google Scholar] [CrossRef] [Green Version]
- Kwak, C.; Kwon, O. Cardiac disorder classification by heart sound signals using murmur likelihood and hidden markov model state likelihood. IET Signal Process. 2012, 6, 326–334. [Google Scholar] [CrossRef]
- Yang, Z.J.; Liu, J.; Ge, J.P.; Chen, L.; Zhao, Z.G.; Yang, W.Y. Prevalence of Cardiovascular Disease Risk Factor in the Chinese Population:the 2007–2008 China National Diabetes and Metabolic Disorders Study. Eur. Heart J. 2011, 33, 213–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, H.; Zhang, J.; Sun, J.; Qiu, T.; Park, Y. Phonocardiogram signal compression using sound repetition and vector quantization. Comput. Biol. Med. 2016, 71, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Silverman, M.; Fleming, P.; Hollman, A.; Julian, D.; Krikler, D. British Cardiology in the 20th Century; Springer: London, UK, 2000. [Google Scholar] [CrossRef]
- Care, A.A.H. How Much Does an EKG Cost? 2020. Available online: https://health.costhelper.com/ecg.html (accessed on 15 February 2020).
- Mondal, A.; Kumar, K.; Bhattacharya, P.; Saha, G. Boundary Estimation of Cardiac Events S1 and S2 Based on Hilbert Transform and Adaptive Thresholding Approach. In Proceedings of the 2013 Indian Conference on Medical Informatics and Telemedicine (ICMIT), Kharagpur, India, 28–30 March 2013. [Google Scholar]
- Mangione, S.; Nieman, L.Z. Cardiac Auscultatory Skills of Internal Medicine and Family Practice Trainees: A Comparison of Diagnostic Proficiency. JAMA 1997, 278, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Lam, M.; Lee, T.; Boey, P.; Ng, W.; Hey, H.; Ho, K.; Cheong, P. Factors influencing cardiac auscultation proficiency in physician trainees. Singap. Med. J. 2005, 46, 11–14. [Google Scholar]
- Roelandt, J. The decline of our physical examination skills: Is echocardiography to blame? Eur. Heart J. Cardiovasc. Imaging 2013, 15, 249–252. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Lim, C.; Chauhan, S.; Foo, J.Y.A.; Venkataraman, A. Phonocardiographic Signal Analysis Method Using a Modified Hidden Markov Model. Ann. Biomed. Eng. 2007, 35, 367–374. [Google Scholar] [CrossRef]
- Zheng, Y.; Guo, X.; Ding, X. A novel hybrid energy fraction and entropy-based approach for systolic heart murmurs identification. Expert Syst. Appl. 2015, 42, 2710–2721. [Google Scholar] [CrossRef]
- Uguz, H. A Biomedical System Based on Artificial Neural Network and Principal Component Analysis for Diagnosis of the Heart Valve Diseases. J. Med. Syst. 2010, 36, 61–72. [Google Scholar] [CrossRef]
- Mishra, M.; Singh, A.; Dutta, M.K.; Burget, R.; Masek, J. Classification of normal and abnormal heart sounds for automatic diagnosis. In Proceedings of the 2017 40th International Conference on Telecommunications and Signal Processing (TSP), Barcelona, Spain, 5–7 July 2017; pp. 753–757. [Google Scholar]
- Meziani, F.; Debbal, S.; Atbi, A. Analysis of phonocardiogram signals using wavelet transform. J. Med. Eng. Technol. 2012, 36, 283–302. [Google Scholar] [CrossRef]
- Chakrabarti, T.; Saha, S.; Roy, S.S.; Chel, I. Phonocardiogram signal analysis - practices, trends and challenges: A critical review. In Proceedings of the 2015 International Conference and Workshop on Computing and Communication (IEMCON), Vancouver, BC, Canada, 15–17 October 2015; pp. 1–4. [Google Scholar]
- Nabih, M.; El-Dahshan, E.S.; Yahia, A.S. A review of intelligent systems for heart sound signal analysis. J. Med. Eng. Technol. 2017, 41, 1–11. [Google Scholar] [CrossRef]
- Patel, S.B.; Callahan, T.F.; Callahan, M.G.; Jones, J.T.; Graber, G.P.; Foster, K.S.; Glifort, K.; Wodicka, G.R. An adaptive noise reduction stethoscope for auscultation in high noise environments. J. Acoust. Soc. Am. 1998, 103, 2483–2491. [Google Scholar] [CrossRef]
- Dewangan, N. Noise Cancellation Using Adaptive Filter for PCG Signal. Blood 2014, 3, 38–43. [Google Scholar]
- Papadaniil, C.; Hadjileontiadis, L. Efficient Heart Sound Segmentation and Extraction Using Ensemble Empirical Mode Decomposition and Kurtosis Features. IEEE J. Biomed. Health Inform. 2014, 18, 1138–1152. [Google Scholar] [CrossRef]
- Ali, M.N.; El-Dahshan, E.S.A.; Yahia, A.H. Denoising of Heart Sound Signals Using Discrete Wavelet Transform. Circuits Syst. Signal Process. 2017, 36, 4482–4497. [Google Scholar] [CrossRef]
- Kang, S.; Doroshow, R.; McConnaughey, J.; Khandoker, A.; Shekhar, R. Heart Sound Segmentation toward Automated Heart Murmur Classification in Pediatric Patents. In Proceedings of the 2015 8th International Conference on Signal Processing, Image Processing and Pattern Recognition (SIP), Jeju, Korea, 25–28 November 2015; pp. 9–12. [Google Scholar] [CrossRef]
- Ahmad, M.; Khan, A.; Khattak, J.; Khattak, S. A Signal Processing Technique for Heart Murmur Extraction and Classification Using Fuzzy Logic Controller. Res. J. Appl. Sci. Eng. Technol. 2014, 8, 1–8. [Google Scholar] [CrossRef]
- Naseri, H.; Homaeinezhad, M.R. Detection and Boundary Identification of Phonocardiogram Sounds Using an Expert Frequency-Energy Based Metric. Ann. Biomed. Eng. 2012, 41, 279–292. [Google Scholar] [CrossRef] [PubMed]
- Salman, A.; Ahmadi, N.; Mengko, R.; Langi, A.Z.R.; Mengko, T. Empirical Mode Decomposition (EMD) Based Denoising Method for Heart Sound Signal and Its Performance Analysis. Int. J. Electr. Comput. Eng. (IJECE) 2016, 6, 2197. [Google Scholar] [CrossRef]
- Zheng, Y.; Guo, X.; Jiang, H.; Zhou, B. An innovative multi-level singular value decomposition and compressed sensing based framework for noise removal from heart sounds. Biomed. Signal Process. Control 2017, 38, 34–43. [Google Scholar] [CrossRef]
- Pham, D.H.; Meignen, S.; Dia, N.; Fontecave-Jallon, J.; Rivet, B. Phonocardiogram Signal Denoising Based on Non-negative Matrix Factorization and Adaptive Contour Representation Computation. IEEE Signal Process. Lett. 2018. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.; Jiang, Z. Comparison of Envelope Extraction Algorithms for Cardiac Sound Signal Segmentation. Expert Syst. Appl. 2008, 34, 1056–1069. [Google Scholar] [CrossRef]
- Zhang, W.; Han, J.; Deng, S. Heart sound classification based on scaled spectrogram and partial least squares regression. Biomed. Signal Process. Control 2017, 32, 20–28. [Google Scholar] [CrossRef]
- Varghees, N.; Ramachandran, K.I. Heart murmur detection and classification using wavelet transform and Hilbert phase envelope. In Proceedings of the 2015 Twenty First National Conference on Communications (NCC), Mumbai, India, 27 February–1 March 2015. [Google Scholar] [CrossRef]
- Hamidah, A.; Saputra, R.; Mengko, T.; Mengko, R.; Anggoro, B. Effective heart sounds detection method based on signal’s characteristics. In Proceedings of the 2016 International Symposium on Intelligent Signal Processing and Communication Systems (ISPACS), Phuket, Thailand, 24–27 October 2016; pp. 1–4. [Google Scholar] [CrossRef]
- Moukadem, A.; Dieterlen, A.; Hueber, N.; Brandt, C. A robust heart sounds segmentation module based on S-transform. Biomed. Signal Process. Control 2013, 8, 273–281. [Google Scholar] [CrossRef] [Green Version]
- Gupta, C.N.; Palaniappan, R.; Swaminathan, S.; Krishnan, S.M. Neural Network Classification of Homomorphic Segmented Heart Sounds. Appl. Soft Comput. 2007, 7, 286–297. [Google Scholar] [CrossRef]
- Jimenez, J.A.; Becerra, M.A.; Delgado-Trejos, E. Heart murmur detection using Ensemble Empirical Mode Decomposition and derivations of the Mel-Frequency Cepstral Coefficients on 4-area phonocardiographic signals. In Proceedings of the Computing in Cardiology 2014, Cambridge, MA, USA, 7–10 September 2014; pp. 493–496. [Google Scholar]
- Dominguez-Morales, J.P.; Jimenez-Fernandez, A.F.; Dominguez-Morales, M.J.; Jimenez-Moreno, G. Deep Neural Networks for the Recognition and Classification of Heart Murmurs Using Neuromorphic Auditory Sensors. IEEE Trans. Biomed. Circuits Syst. 2018, 12, 24–34. [Google Scholar] [CrossRef]
- Sun, S.; Wang, H.; Jiang, Z.; Fang, Y.; Ting, T. Segmentation-based heart sound feature extraction combined with classifier models for a VSD diagnosis system. Expert Syst. Appl. Int. J. 2014, 41, 1769–1780. [Google Scholar] [CrossRef]
- He, J.; Jiang, Y.; Du, M. Analysis and classification of heart sounds with mechanical prosthetic heart valves based on Hilbert-Huang transform. Int. J. Cardiol. 2011, 151, 126–127. [Google Scholar] [CrossRef]
- Pedrosa, J.; Castro, A.; Vinhoza, T.T. Automatic heart sound segmentation and murmur detection in pediatric phonocardiograms. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 2294–2297. [Google Scholar]
- Kao, W.C.; Wei, C.C. Automatic Phonocardiograph Signal Analysis for Detecting Heart Valve Disorders. Expert Syst. Appl. 2011, 38, 6458–6468. [Google Scholar] [CrossRef]
- Schmidt, S.; Egon, T.; Holst-Hansen, C.; Graff, C.; Struijk, J. Segmentation of Heart Sound Recordings from an Electronic Stethoscope by a Duration Dependent Hidden Markov Model. In Proceedings of the 2008 Computers in Cardiology, Bologna, Italy, 14–17 September 2008; Volume 35, pp. 345–348. [Google Scholar] [CrossRef] [Green Version]
- Gamero, L.G.; Watrous, R. Detection of the First and Second Heart Sound Using Probabilistic Models. In Proceedings of the 25th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (IEEE Cat. No.03CH37439), Cancun, Mexico, 17–21 September 2003; Volume 25, pp. 2877–2880. [Google Scholar] [CrossRef]
- Springer, D.; Tarassenko, L.; Clifford, G. Logistic Regression-HSMM-based Heart Sound Segmentation. IEEE Trans. Biomed. Eng. 2015, 63. [Google Scholar] [CrossRef] [PubMed]
- Eslamizadeh, G.; Barati, R. Heart murmur detection based on Wavelet Transformation and a synergy between Artificial Neural Network and modified Neighbor Annealing methods. Artif. Intell. Med. 2017, 78. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Doroshow, R.; McConnaughey, J.; Shekhar, R. Automated Identification of Innocent Still’s Murmur in Children. IEEE Trans. Biomed. Eng. 2017, 64, 1326–1334. [Google Scholar] [CrossRef]
- Deng, S.W.; Han, J. Towards heart sound classification without segmentation via autocorrelation feature and diffusion maps. Future Gener. Comput. Syst. 2016, 60. [Google Scholar] [CrossRef]
- Zhang, W.; Han, J.; Deng, S.W. Heart sound classification based on scaled spectrogram and tensor decomposition. Expert Syst. Appl. 2017, 84. [Google Scholar] [CrossRef]
- Redlarski, G.; Gradolewski, D.; Palkowski, A. A System for Heart Sounds Classification. PLoS ONE 2014, 9, e112673. [Google Scholar] [CrossRef]
- Güraksin, G.E.; Uguz, H. Classification of heart sounds based on the least squares support vector machine. Int. J. Innov. Comput. Inf. Control IJICIC 2011, 7, 7131–7144. [Google Scholar]
- Patidar, S.; Pachori, R. Classification of cardiac sound signals using constrained tunable-Q wavelet transform. Expert Syst. Appl. 2014, 41, 7161–7170. [Google Scholar] [CrossRef]
- Oliveira, J.; Oliveira, C.; Cardoso, B.; Sultan, M.S.; Coimbra, M.T. A multi-spot exploration of the topological structures of the reconstructed phase-space for the detection of cardiac murmurs. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015. [Google Scholar] [CrossRef]
- Hamidi, M.; Ghassemian, H.; Imani, M. Classification of Heart Sound Signal Using Curve Fitting and Fractal Dimension. Biomed. Signal Process. Control 2018, 39, 351–359. [Google Scholar] [CrossRef]
- Potes, C.; Parvaneh, S.; Rahman, A.; Conroy, B. Ensemble of Feature-based and Deep learning-based Classifiers for Detection of Abnormal Heart Sounds. In Proceedings of the 2016 Computing in Cardiology Conference (CinC), Vancouver, BC, Canada, 11–14 September 2016. [Google Scholar] [CrossRef]
- Bozkurt, B.; Germanakis, I.; Stylianou, Y. A study of time-frequency features for CNN-based automatic heart sound classification for pathology detection. Comput. Biol. Med. 2018, 100. [Google Scholar] [CrossRef]
- Messner, E.; Zöhrer, M.; Pernkopf, F. Heart Sound Segmentation-An Event Detection Approach Using Deep Recurrent Neural Networks. IEEE Trans. Biomed. Eng. 2018, 65, 1964–1974. [Google Scholar] [CrossRef] [PubMed]
- Yaseen; Son, G.Y.; Kwon, S. Classification of Heart Sound Signal Using Multiple Features. Appl. Sci. 2018, 8, 2344. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Wang, S.; Shen, C.H.; Choy, F. Matrix decomposition based feature extraction for murmur classification. Med. Eng. Phys. 2011, 34, 756–761. [Google Scholar] [CrossRef] [PubMed]
- Safara, F.; Doraisamy, S.; Azman, A.; Jantan, A.; Ranga, A. Multi-level basis selection of wavelet packet decomposition tree for heart sound classification. Comput. Biol. Med. 2013, 43, 1407–1414. [Google Scholar] [CrossRef] [PubMed]
- Guillermo, J.; Ricalde, L.J.; Sanchez, E.; Alanis, A. Detection of Heart Murmurs Based on Radial wavelet Neural Network with Kalman Learning. Neurocomputing 2015, 164. [Google Scholar] [CrossRef]
- Safara, F.; Doraisamy, S.; Azman, A.; Jantan, A.; Ranga, A. Wavelet Packet Entropy for Heart Murmurs Classification. Adv. Bioinform. 2012, 2012, 327269. [Google Scholar] [CrossRef]
- Thiyagaraja, S.; Dantu, R.; Shrestha, P.; Chitnis, A.; Thompson, M.; Anumandla, P.T.; Sarma, T.; Dantu, S. A novel heart-mobile interface for detection and classification of heart sounds. Biomed. Signal Process. Control 2018, 45, 313–324. [Google Scholar] [CrossRef]
- Choi, S.; Jung, G.; Park, H.K. A novel cardiac spectral segmentation based on a multi-Gaussian fitting method for regurgitation murmur identification. Signal Process. 2014, 104, 339–345. [Google Scholar] [CrossRef]
- Varghees, V.N.; Ramachandran, K.I. Effective Heart Sound Segmentation and Murmur Classification Using Empirical Wavelet Transform and Instantaneous Phase for Electronic Stethoscope. IEEE Sens. J. 2017. [Google Scholar] [CrossRef]
- Choi, S.; Shin, Y.; Park, H.K. Selection of wavelet packet measures for insufficiency murmur identification. Expert Syst. Appl. 2011, 38, 4264–4271. [Google Scholar] [CrossRef]
- Xiefeng, C.; Ma, Y.; Liu, C.; Zhang, X.; Guo, Y. Research on heart sound identification technology. Sci. China Inf. Sci. 2012, 55, 281–292. [Google Scholar] [CrossRef]
- Abo-Zahhad, M.; Ahmed, S.; Seha, S.N. Biometrics from heart sounds: Evaluation of a new approach based on wavelet packet cepstral features using HSCT-11 database. Comput. Electr. Eng. 2016, 53. [Google Scholar] [CrossRef]
- Chandrakar, B.; Yadav, O.; Chandra, V. A survey of noise removal techniques for ecg signals. Int. J. Adv. Res. Comput. Commun. Eng. 2013, 2, 1354–1357. [Google Scholar]
- Liu, Q.; Wu, X.; Ma, X. An automatic segmentation method for heart sounds. BioMed Eng. Online 2018, 17. [Google Scholar] [CrossRef] [Green Version]
- Tang, H.; Li, T.; Qiu, T. Segmentation of heart sounds based on dynamic clustering. Biomed. Signal Process. Control 2012, 7. [Google Scholar] [CrossRef]
- Dave, N. Feature extraction methods LPC, PLP and MFCC in speech recognition. Int. J. Adv. Res. Eng. Technol. 2013, 1, 1–4. [Google Scholar]
- Han, W.; Chan, C.F.; Choy, C.S.; Pun, K.P. An efficient MFCC extraction method in speech recognition. In Proceedings of the 2006 IEEE International Symposium on Circuits and Systems, Kos, Greece, 21–24 May 2006. [Google Scholar]
- Al Marzuqi, H.M.O.; Hussain, S.M.; Frank, A. Device Activation based on Voice Recognition using Mel Frequency Cepstral Coefficients (MFCC’s) Algorithm. Int. Res. J. Eng. Technol. 2019, 6, 4297–4301. [Google Scholar]
- McLachlan, G.; Peel, D. Finite Mixture Models; John Wiley & Sons: Hoboken, NJ, USA, 2004. [Google Scholar]
- McLachlan, G.; Krishnan, T. The EM Algorithm and Extensions; John Wiley & Sons: Hoboken, NJ, USA, 2007; Volume 382. [Google Scholar]
- Bishop, C.M. Pattern Recognition and Machine Learning; Springer: Berlin/Heidelberg, Germany, 2006. [Google Scholar]
- Hastie, T.; Tibshirani, R.; Friedman, J.; Franklin, J. The elements of statistical learning: Data mining, inference and prediction. Math. Intell. 2005, 27, 83–85. [Google Scholar]
- Gandarias, J.M.; Garcia-Cerezo, A.J.; Gomez-de Gabriel, J.M. CNN-based methods for object recognition with high-resolution tactile sensors. IEEE Sens. J. 2019, 19, 6872–6882. [Google Scholar] [CrossRef]
- Zhao, J.; Mao, X.; Chen, L. Speech emotion recognition using deep 1D & 2D CNN LSTM networks. Biomed. Signal Process. Control 2019, 47, 312–323. [Google Scholar]
- Cheng, W.; Sun, Y.; Li, G.; Jiang, G.; Liu, H. Jointly network: A network based on CNN and RBM for gesture recognition. Neural Comput. Appl. 2019, 31, 309–323. [Google Scholar] [CrossRef] [Green Version]
- Saitoh, T.; Zhou, Z.; Zhao, G.; Pietikäinen, M. Concatenated frame image based cnn for visual speech recognition. In Asian Conference on Computer Vision; Springer: Berlin/Heidelberg, Germany, 2016; pp. 277–289. [Google Scholar]
- Alexandre, L.A. 3D object recognition using convolutional neural networks with transfer learning between input channels. In Intelligent Autonomous Systems 13; Springer: Berlin/Heidelberg, Germany, 2016; pp. 889–898. [Google Scholar]
- Gao, Y.; Mosalam, K.M. Deep transfer learning for image-based structural damage recognition. Comput.-Aided Civ. Infrastruct. Eng. 2018, 33, 748–768. [Google Scholar] [CrossRef]
- Pandey, G.; Baranwal, A.; Semenov, A. Identifying Images with Ladders Using Deep CNN Transfer Learning. In Intelligent Decision Technologies 2019; Springer: Berlin/Heidelberg, Germany, 2020; pp. 143–153. [Google Scholar]
- Yang, Z.; Yu, W.; Liang, P.; Guo, H.; Xia, L.; Zhang, F.; Ma, Y.; Ma, J. Deep transfer learning for military object recognition under small training set condition. Neural Comput. Appl. 2019, 31, 6469–6478. [Google Scholar] [CrossRef]
- Tan, C.; Sun, F.; Kong, T.; Zhang, W.; Yang, C.; Liu, C. A survey on deep transfer learning. In International Conference on Artificial Neural Networks; Springer: Berlin/Heidelberg, Germany, 2018; pp. 270–279. [Google Scholar]
- Bentley, P.; Nordehn, G.; Coimbra, M.; Mannor, S. The PASCAL Classifying Heart Sounds Challenge 2011 (CHSC2011) Results. 2011. Available online: http://www.peterjbentley.com/heartchallenge/index.html (accessed on 15 January 2020).
- Clifford, G.D.; Liu, C.; Moody, B.; Springer, D.; Silva, I.; Li, Q.; Mark, R.G. Classification of normal/abnormal heart sound recordings: The PhysioNet/Computing in Cardiology Challenge 2016. In Proceedings of the 2016 Computing in Cardiology Conference (CinC), Vancouver, BC, Canada, 11–14 September 2016; pp. 609–612. [Google Scholar]
- Chollet, F. Xception: Deep learning with depthwise separable convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1251–1258. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Zoph, B.; Vasudevan, V.; Shlens, J.; Le, Q.V. Learning transferable architectures for scalable image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–22 June 2018; pp. 8697–8710. [Google Scholar]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L.C. Mobilenetv2: Inverted residuals and linear bottlenecks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–22 June 2018; pp. 4510–4520. [Google Scholar]
- Howard, A.G.; Zhu, M.; Chen, B.; Kalenichenko, D.; Wang, W.; Weyand, T.; Andreetto, M.; Adam, H. Mobilenets: Efficient convolutional neural networks for mobile vision applications. arXiv 2017, arXiv:1704.04861. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Szegedy, C.; Ioffe, S.; Vanhoucke, V.; Alemi, A.A. Inception-v4, inception-resnet and the impact of residual connections on learning. In Proceedings of the Thirty-First AAAI Conference on Artificial Intelligence, San Francisco, CA, USA, 4–9 February 2017. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Malik, S.I.; Akram, M.U.; Siddiqi, I. Localization and classification of heartbeats using robust adaptive algorithm. Biomed. Signal Process. Control 2019, 49, 57–77. [Google Scholar] [CrossRef]
- Chakir, F.; Jilbab, A.; Nacir, C.; Hammouch, A. Phonocardiogram signals processing approach for PASCAL classifying heart sounds challenge. Signal Image Video Process. 2018, 12, 1149–1155. [Google Scholar] [CrossRef]
- Chakir, F.; Jilbab, A.; Nacir, C.; Hammouch, A. Phonocardiogram signals classification into normal heart sounds and heart murmur sounds. In Proceedings of the 11th International Conference on Intelligent Systems: Theories and Applications (SITA), Mohammedia, Morocco, 19–20 October 2016; pp. 1–4. [Google Scholar]
- Sidra, G.; Ammara, N.; Taimur, H.; Bilal, H.; Ramsha, A. Fully Automated Identification of Heart Sounds for the Analysis of Cardiovascular Pathology. In Applications of Intelligent Technologies in Healthcare; Springer: Berlin/Heidelberg, Germany, 2019; pp. 117–129. [Google Scholar]
- Balili, C.C.; Sobrepena, M.C.C.; Naval, P.C. Classification of heart sounds using discrete and continuous wavelet transform and random forests. In Proceedings of the 2015 3rd IAPR Asian Conference on Pattern Recognition (ACPR), Kuala Lumpur, Malaysia, 3–6 November 2015; pp. 655–659. [Google Scholar]
- Nogueira, D.M.; Ferreira, C.A.; Jorge, A.M. Classifying heart sounds using images of MFCC and temporal features. In EPIA Conference on Artificial Intelligence; Springer: Berlin/Heidelberg, Germany, 2017; pp. 186–203. [Google Scholar]
- Ortiz, J.J.G.; Phoo, C.P.; Wiens, J. Heart sound classification based on temporal alignment techniques. In Proceedings of the 2016 Computing in Cardiology Conference (CinC), Vancouver, BC, Canada, 11–14 September 2016; pp. 589–592. [Google Scholar]
- Tang, H.; Chen, H.; Li, T.; Zhong, M. Classification of normal/abnormal heart sound recordings based on multi-domain features and back propagation neural network. In Proceedings of the 2016 Computing in Cardiology Conference (CinC), Vancouver, BC, Canada, 11–14 September 2016; pp. 593–596. [Google Scholar]
- Rubin, J.; Abreu, R.; Ganguli, A.; Nelaturi, S.; Matei, I.; Sricharan, K. Recognizing abnormal heart sounds using deep learning. arXiv 2017, arXiv:1707.04642. [Google Scholar]
- Kay, E.; Agarwal, A. DropConnected neural networks trained on time-frequency and inter-beat features for classifying heart sounds. Physiol. Meas. 2017, 38, 1645. [Google Scholar] [CrossRef]
- Abdollahpur, M.; Ghiasi, S.; Mollakazemi, M.J.; Ghaffari, A. Cycle selection and neuro-voting system for classifying heart sound recordings. In Proceedings of the 2016 Computing in Cardiology Conference (CinC), Vancouver, BC, Canada, 11–14 September 2016; pp. 1–4. [Google Scholar]
- Singh, S.A.; Majumder, S. Short unsegmented PCG classification based on ensemble classifier. Turk. J. Electr. Eng. Comput. Sci. 2020, 28, 875–889. [Google Scholar] [CrossRef]
- Han, W.; Yang, Z.; Lu, J.; Xie, S. Supervised threshold-based heart sound classification algorithm. Physiol. Meas. 2018, 39, 115011. [Google Scholar] [CrossRef]
- Whitaker, B.M.; Suresha, P.B.; Liu, C.; Clifford, G.D.; Anderson, D.V. Combining sparse coding and time-domain features for heart sound classification. Physiol. Meas. 2017, 38, 1701. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Dai, Z.; Jiang, Y.; Li, T.; Liu, C. PCG classification using multidomain features and SVM classifier. BioMed Res. Int. 2018, 2018, 4205027. [Google Scholar] [CrossRef] [Green Version]
- Plesinger, F.; Viscor, I.; Halamek, J.; Jurco, J.; Jurak, P. Heart sounds analysis using probability assessment. Physiol. Meas. 2017, 38, 1685. [Google Scholar] [CrossRef] [PubMed]
- Abdollahpur, M.; Ghaffari, A.; Ghiasi, S.; Mollakazemi, M.J. Detection of pathological heart sounds. Physiol. Meas. 2017, 38, 1616. [Google Scholar] [CrossRef] [PubMed]
- Homsi, M.N.; Warrick, P. Ensemble methods with outliers for phonocardiogram classification. Physiol. Meas. 2017, 38, 1631. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.A.; Majumder, S. Classification of unsegmented heart sound recording using KNN classifier. J. Mech. Med. Biol. 2019, 19, 1950025. [Google Scholar] [CrossRef]
- Langley, P.; Murray, A. Heart sound classification from unsegmented phonocardiograms. Physiol. Meas. 2017, 38, 1658. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model | Citation | Layers | Size | Parameters |
|---|---|---|---|---|
| Xception | Chollet [90] | 71 | 85 MB | 44.6 millions |
| VGG19 | Simonyan and Zisserman [91] | 26 | 549 MB | 143.6 millions |
| VGG16 | Simonyan and Zisserman [91] | 23 | 528 MB | 138.3 millions |
| ResNet152V2 | He et al. [92] | - | 98 MB | 25.6 millions |
| ResNet152 | He et al. [92] | - | 232 MB | 60.4 millions |
| ResNet101V2 | He et al. [92] | - | 171 MB | 44.6 millions |
| ResNet101 | He et al. [92] | 101 | 167 MB | 44.6 millions |
| ResNet50V2 | He et al. [92] | 98 MB | 25.6 millions | |
| ResNet50 | He et al. [92] | - | 98 MB | 25.6 millions |
| NASNetMobile | Zoph et al. [93] | - | 20 MB | 5.3 millions |
| MobileNetV2 | Sandler et al. [94] | 53 | 13 MB | 3.5 millions |
| MobileNet | Howard et al. [95] | 88 | 16 MB | 4.25 millions |
| InceptionV3 | Szegedy et al. [96] | 48 | 89 MB | 23.9 millions |
| InceptionResNetV2 | Szegedy et al. [97] | 164 | 209 MB | 55.9 millions |
| DenseNet201 | Huang et al. [98] | 201 | 77 MB | 20 millions |
| DenseNet169 | Huang et al. [98] | 169 | 57 MB | 14.3 millions |
| DenseNet121 | Huang et al. [98] | 121 | 33 MB | 8.06 millions |
| Training Set | Class | ||
|---|---|---|---|
| Normal | Murmur | Extrasystole | |
| A | 31 | 34 | 19 |
| B | 200 | 95 | 46 |
| Total | 231 | 129 | 65 |
| Training Set | Class Segments | ||
|---|---|---|---|
| Normal | Murmur | Extrasystole | |
| Selected | 323 | 317 | 62 |
| Ignored | 33 | 14 | 44 |
| Total segments | 356 | 331 | 106 |
| Model | Accuracy | |||
|---|---|---|---|---|
| Fold1 | Fold2 | Fold3 | AVG | |
| VGG16 | 0.77 | 0.82 | 0.80 | 0.81 |
| VGG19 | 0.78 | 0.81 | 0.83 | 0.81 |
| Xception | 0.56 | 0.58 | 0.58 | 0.57 |
| ResNet152V2 | 0.66 | 0.69 | 0.68 | 0.68 |
| ResNet152 | 0.73 | 0.73 | 0.71 | 0.72 |
| ResNet101V2 | 0.66 | 0.67 | 0.69 | 0.67 |
| ResNet101 | 0.69 | 0.72 | 0.74 | 0.72 |
| ResNet50v2 | 0.68 | 0.69 | 0.64 | 0.67 |
| ResNet50 | 0.72 | 0.73 | 0.72 | 0.72 |
| NasNetMobile | 0.63 | 0.62 | 0.60 | 0.62 |
| MobileNetV2 | 0.68 | 0.67 | 0.63 | 0.66 |
| MobileNet | 0.66 | 0.67 | 0.67 | 0.67 |
| Inceptionv3 | 0.68 | 0.68 | 0.68 | 0.68 |
| InceptionResNetV2 | 0.59 | 0.66 | 0.61 | 0.62 |
| DenseNet201 | 0.71 | 0.74 | 0.69 | 0.71 |
| DenseNet169 | 0.68 | 0.70 | 0.70 | 0.69 |
| DenseNet121 | 0.69 | 0.73 | 0.70 | 0.71 |
| Model | TPR | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fold1 | Fold2 | Fold3 | Avg | ||||||||||
| E | M | N | Avg | E | M | N | Avg | E | M | N | Avg | ||
| VGG16 | 0.36 | 0.77 | 0.90 | 0.68 | 0.62 | 0.80 | 0.89 | 0.77 | 0.31 | 0.83 | 0.93 | 0.69 | 0.72 |
| VGG19 | 0.44 | 0.80 | 0.88 | 0.70 | 0.54 | 0.81 | 0.89 | 0.75 | 0.4 | 0.88 | 0.91 | 0.73 | 0.73 |
| Xception | 0.0 | 0.52 | 0.77 | 0.43 | 0.0 | 0.41 | 0.91 | 0.44 | 0.0 | 0.46 | 0.88 | 0.44 | 0.44 |
| ResNet152V2 | 0.25 | 0.81 | 0.65 | 0.57 | 0.11 | 0.69 | 0.86 | 0.55 | 0.28 | 0.7 | 0.78 | 0.59 | 0.57 |
| ResNet152 | 0.27 | 0.70 | 0.89 | 0.62 | 0.25 | 0.69 | 0.91 | 0.62 | 0.14 | 0.77 | 0.83 | 0.58 | 0.61 |
| ResNet101V2 | 0.02 | 0.63 | 0.88 | 0.51 | 0.14 | 0.64 | 0.86 | 0.55 | 0.25 | 0.73 | 0.79 | 0.59 | 0.55 |
| ResNet101 | 0.16 | 0.81 | 0.74 | 0.57 | 0.25 | 0.79 | 0.80 | 0.61 | 0.0 | 0.79 | 0.91 | 0.56 | 0.58 |
| ResNet50v2 | 0.33 | 0.77 | 0.71 | 0.60 | 0.17 | 0.75 | 0.79 | 0.57 | 0.05 | 0.56 | 0.89 | 0.50 | 0.56 |
| ResNet50 | 0.19 | 0.74 | 0.85 | 0.59 | 0.2 | 0.73 | 0.89 | 0.60 | 0.17 | 0.7 | 0.90 | 0.59 | 0.59 |
| NasNetMobile | 0.22 | 0.58 | 0.81 | 0.54 | 0.0 | 0.6 | 0.82 | 0.47 | 0.0 | 0.56 | 0.83 | 0.46 | 0.49 |
| MobileNetV2 | 0.16 | 0.66 | 0.84 | 0.56 | 0.11 | 0.67 | 0.83 | 0.53 | 0.14 | 0.7 | 0.72 | 0.52 | 0.54 |
| MobileNet | 0.22 | 0.65 | 0.80 | 0.56 | 0.22 | 0.59 | 0.87 | 0.56 | 0.08 | 0.74 | 0.78 | 0.53 | 0.55 |
| Inceptionv3 | 0.0 | 0.65 | 0.91 | 0.52 | 0.0 | 0.63 | 0.94 | 0.52 | 0.02 | 0.6 | 0.95 | 0.52 | 0.52 |
| InceptionResNetV2 | 0.0 | 0.44 | 0.91 | 0.45 | 0.0 | 0.69 | 0.84 | 0.51 | 0.0 | 0.6 | 0.81 | 0.47 | 0.48 |
| DenseNet201 | 0.25 | 0.69 | 0.88 | 0.60 | 0.34 | 0.73 | 0.86 | 0.64 | 0.17 | 0.73 | 0.81 | 0.57 | 0.60 |
| DenseNet169 | 0.25 | 0.67 | 0.82 | 0.58 | 0.11 | 0.82 | 0.77 | 0.57 | 0.08 | 0.70 | 0.88 | 0.55 | 0.57 |
| DenseNet121 | 0.19 | 0.72 | 0.83 | 0.58 | 0.4 | 0.72 | 0.84 | 0.65 | 0.17 | 0.79 | 0.78 | 0.58 | 0.60 |
| Accuracy | Folds | |||
|---|---|---|---|---|
| Fold1 | Fold2 | Fold3 | AVG | |
| VGG16 | 0.85957 | 0.8383 | 0.84483 | 0.85 |
| VGG19 | 0.84255 | 0.89711 | 0.86207 | 0.87 |
| Xception | 0.65106 | 0.61277 | 0.67241 | 0.64 |
| ResNet152V2 | 0.72766 | 0.68287 | 0.69397 | 0.70 |
| ResNet152 | 0.75745 | 0.74468 | 0.83621 | 0.78 |
| ResNet101V2 | 0.75745 | 0.69787 | 0.73276 | 0.73 |
| ResNet101 | 0.77447 | 0.74894 | 0.77155 | 0.76 |
| ResNet50v2 | 0.72766 | 0.69362 | 0.73707 | 0.72 |
| ResNet50 | 0.75745 | 0.73191 | 0.78017 | 0.76 |
| NasNetMobile | 0.69362 | 0.69787 | 0.68966 | 0.69 |
| MobileNetV2 | 0.69787 | 0.65957 | 0.69397 | 0.68 |
| MobileNet | 0.74043 | 0.69787 | 0.71552 | 0.72 |
| Inceptionv3 | 0.70638 | 0.68511 | 0.66379 | 0.68 |
| InceptionResNetV2 | 0.69787 | 0.70213 | 0.67241 | 0.69 |
| DenseNet201 | 0.77447 | 0.7234 | 0.76293 | 0.75 |
| DenseNet169 | 0.74894 | 0.68085 | 0.75431 | 0.73 |
| DenseNet121 | 0.7234 | 0.70213 | 0.72414 | 0.71 |
| Model | TPR | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fold1 | Fold2 | Fold3 | Avg | ||||||||||
| E | M | N | Avg | E | M | N | Avg | E | M | N | Avg | ||
| VGG16 | 0.71 | 0.87 | 0.87 | 0.82 | 0.57 | 0.84 | 0.87 | 0.76 | 0.6 | 0.83 | 0.89 | 0.77 | 0.79 |
| VGG19 | 0.80 | 0.83 | 0.86 | 0.83 | 0.57 | 0.89 | 0.93 | 0.80 | 0.9 | 0.87 | 0.84 | 0.87 | 0.83 |
| Xception | 0.0 | 0.59 | 0.83 | 0.47 | 0.0 | 0.39 | 0.94 | 0.44 | 0.0 | 0.61 | 0.85 | 0.48 | 0.47 |
| ResNet152V2 | 0.61 | 0.72 | 0.75 | 0.69 | 0.62 | 0.71 | 0.72 | 0.68 | 0.75 | 0.68 | 0.69 | 0.70 | 0.70 |
| ResNet152 | 0.80 | 0.66 | 0.83 | 0.77 | 0.42 | 0.73 | 0.81 | 0.65 | 0.6 | 0.83 | 0.87 | 0.77 | 0.73 |
| ResNet101V2 | 0.66 | 0.69 | 0.83 | 0.73 | 0.09 | 0.63 | 0.87 | 0.53 | 0.7 | 0.73 | 0.73 | 0.72 | 0.66 |
| ResNet101 | 0.61 | 0.73 | 0.84 | 0.73 | 0.47 | 0.76 | 0.78 | 0.67 | 0.7 | 0.80 | 0.74 | 0.75 | 0.72 |
| ResNet50v2 | 0.47 | 0.66 | 0.84 | 0.65 | 0.19 | 0.61 | 0.87 | 0.55 | 0.4 | 0.72 | 0.81 | 0.64 | 0.62 |
| ResNet50 | 0.66 | 0.78 | 0.75 | 0.73 | 0.28 | 0.77 | 0.77 | 0.61 | 0.45 | 0.75 | 0.86 | 0.69 | 0.68 |
| NasNetMobile | 0.23 | 0.57 | 0.89 | 0.57 | 0.0 | 0.78 | 0.75 | 0.51 | 0.3 | 0.66 | 0.78 | 0.58 | 0.55 |
| MobileNetV2 | 0.28 | 0.61 | 0.86 | 0.58 | 0.09 | 0.55 | 0.87 | 0.50 | 0.3 | 0.54 | 0.91 | 0.58 | 0.56 |
| MobileNet | 0.76 | 0.61 | 0.86 | 0.74 | 0.38 | 0.95 | 0.50 | 0.61 | 0.6 | 0.8 | 0.65 | 0.68 | 0.68 |
| Inceptionv3 | 0.0 | 0.63 | 0.91 | 0.51 | 0.0 | 0.68 | 0.81 | 0.50 | 0.15 | 0.69 | 0.72 | 0.52 | 0.51 |
| InceptionResNetV2 | 0.0 | 0.65 | 0.87 | 0.51 | 0.0 | 0.75 | 0.78 | 0.51 | 0.0 | 0.63 | 0.83 | 0.48 | 0.50 |
| DenseNet201 | 0.71 | 0.68 | 0.87 | 0.75 | 0.19 | 0.78 | 0.76 | 0.58 | 0.8 | 0.70 | 0.81 | 0.77 | 0.70 |
| DenseNet169 | 0.76 | 0.78 | 0.71 | 0.75 | 0.33 | 0.82 | 0.61 | 0.58 | 0.45 | 0.69 | 0.86 | 0.67 | 0.67 |
| DenseNet121 | 0.42 | 0.78 | 0.72 | 0.64 | 0.47 | 0.82 | 0.62 | 0.64 | 0.7 | 0.63 | 0.81 | 0.71 | 0.67 |
| Works | PASCAL 2011 Signal Statistics | Classes | Overall Accuracy | Overall PPV | Overall TPR |
|---|---|---|---|---|---|
| Our method | Full labeled dataset | Normal, murmur, and extrasystole | 0.87 | 0.81 | 0.83 |
| Malik et al. [99] | 31 signals | Normal, murmur, and other sounds | 0.89 | 0.91 | 0.98 |
| Chakir et al. [100] | 52 signals | Normal and abnormal sounds | - | 0.63 | - |
| Zhang et al. [32] | Full dataset | Normal, murmur, and other sounds | - | 0.67 | - |
| Chakir et al. [101] | 14 from A and 127 from B | Normal and murmurs | - | 0.78 | - |
| Balili et al. [103] | Full dataset | Normal, murmur, and other sounds | 0.48 | - | - |
| Pedrosa et al. [41] | 111 signals | Normal heart sounds and murmurs | - | 0.986 | 0.892 |
| Sidra et al. [102] | 24 normal and 31 abnormal | normal and abnormal | 87.7 | - | 96.7 |
| Folds | Accuracy | TPR (Sensitivity) | Precision (PPV) | TNR (Specificity) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Extra | Murmur | Normal | Extra | Murmur | Normal | Extra | Murmur | Normal | Extra | Murmur | Normal | |
| Fold1 | 0.95 | 0.89 | 0.84 | 0.81 | 0.83 | 0.86 | 0.71 | 0.92 | 0.81 | 0.97 | 0.94 | 0.83 |
| Fold2 | 0.96 | 0.92 | 0.89 | 0.57 | 0.90 | 0.93 | 0.92 | 0.92 | 0.85 | 0.99 | 0.94 | 0.86 |
| Fold3 | 0.95 | 0.91 | 0.87 | 0.9 | 0.88 | 0.84 | 0.64 | 0.92 | 0.86 | 0.95 | 0.94 | 0.88 |
| Folds avg | 0.95 | 0.91 | 0.87 | 0.76 | 0.87 | 0.88 | 0.76 | 0.92 | 0.84 | 0.97 | 0.94 | 0.86 |
| Classes avg | 0.91 | 0.84 | 0.84 | 0.92 | ||||||||
| Average | Accuracy | TPR (Sensitivity) | Precision (PPV) | TNR (Specificity) |
|---|---|---|---|---|
| VGG16 | 0.966 | 0.930 | 0.946 | 0.930 |
| VGG19 | 0.970 | 0.946 | 0.944 | 0.946 |
| Xception | 0.828 | 0.877 | 0.732 | 0.877 |
| ResNet152V2 | 0.824 | 0.873 | 0.730 | 0.873 |
| ResNet152 | 0.490 | 0.667 | 0.640 | 0.667 |
| ResNet101V2 | 0.438 | 0.665 | 0.422 | 0.665 |
| ResNet101 | 0.690 | 0.592 | 0.812 | 0.592 |
| ResNet50v2 | 0.698 | 0.736 | 0.728 | 0.736 |
| ResNet50 | 0.620 | 0.763 | 0.685 | 0.763 |
| NasNetMobile | 0.203 | 0.489 | 0.350 | 0.489 |
| MobileNetV2 | 0.228 | 0.497 | 0.526 | 0.497 |
| MobileNet | 0.671 | 0.679 | 0.673 | 0.679 |
| Inceptionv3 | 0.659 | 0.791 | 0.686 | 0.791 |
| InceptionResNetV2 | 0.863 | 0.908 | 0.765 | 0.908 |
| DenseNet201 | 0.571 | 0.725 | 0.719 | 0.725 |
| DenseNet169 | 0.493 | 0.675 | 0.606 | 0.675 |
| DenseNet121 | 0.601 | 0.734 | 0.714 | 0.734 |
| Average | Accuracy | TPR (Sensitivity) | Precision (PPV) | TNR (Specificity) |
|---|---|---|---|---|
| our approach | 0.970 | 0.946 | 0.944 | 0.946 |
| [104] | 0.8697 | 0.964 | - | 0.726 |
| [55] | - | 0.942 | - | 0.778 |
| [105] | 0.824 | - | - | - |
| [106] | - | 0.8095 | - | 0.839 |
| [107] | - | 0.84 | - | 0.957 |
| [108] | 0.852 | - | - | - |
| [109] | - | 0.885 | - | 0.921 |
| [110] | 0.879 | 0.885 | - | 0.878 |
| [38] | 0.97 | 0.932 | - | 0.951 |
| [111] | 0.915 | 0.983 | 0.846 | |
| [112] | 0.892 | 0.90 | - | 0.884 |
| [113] | 0.88 | 0.88 | - | 0.87 |
| [114] | 0.85 | 0.89 | - | 0.816 |
| [115] | 0.826 | 0.769 | - | 0.883 |
| [116] | 0.801 | 0.796 | - | 0.806 |
| [117] | 0.9 | 0.93 | - | 0.9 |
| [118] | 0.79 | 0.77 | - | 0.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boulares, M.; Alotaibi, R.; AlMansour, A.; Barnawi, A. Cardiovascular Disease Recognition Based on Heartbeat Segmentation and Selection Process. Int. J. Environ. Res. Public Health 2021, 18, 10952. https://doi.org/10.3390/ijerph182010952
Boulares M, Alotaibi R, AlMansour A, Barnawi A. Cardiovascular Disease Recognition Based on Heartbeat Segmentation and Selection Process. International Journal of Environmental Research and Public Health. 2021; 18(20):10952. https://doi.org/10.3390/ijerph182010952
Chicago/Turabian StyleBoulares, Mehrez, Reem Alotaibi, Amal AlMansour, and Ahmed Barnawi. 2021. "Cardiovascular Disease Recognition Based on Heartbeat Segmentation and Selection Process" International Journal of Environmental Research and Public Health 18, no. 20: 10952. https://doi.org/10.3390/ijerph182010952