
Development of a Digital Case Management Tool for Community Based Inclusive Development Program

 , and
, and
Abstract
:1. Introduction
The CBID Demonstration Model in Laos PDR
2. Materials and Methods
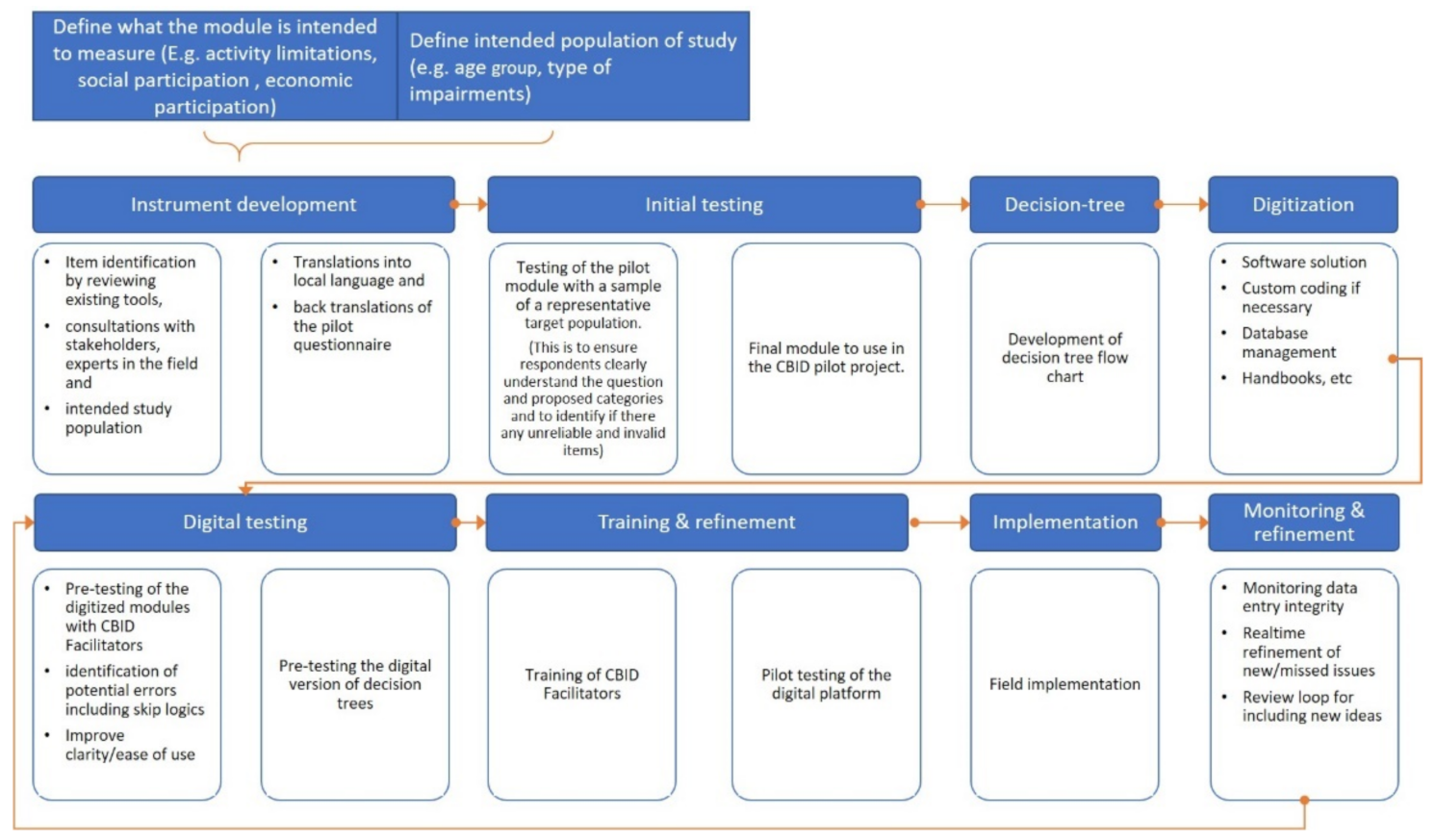
2.1. Phase 1. Establishing the Objectives of the Modular Tool
2.2. Phase 2. Content Development and Testing
2.3. Phase 3. Digitization and Testing
3. Results
3.1. Objectives of the Modular Tool and Its Rationale
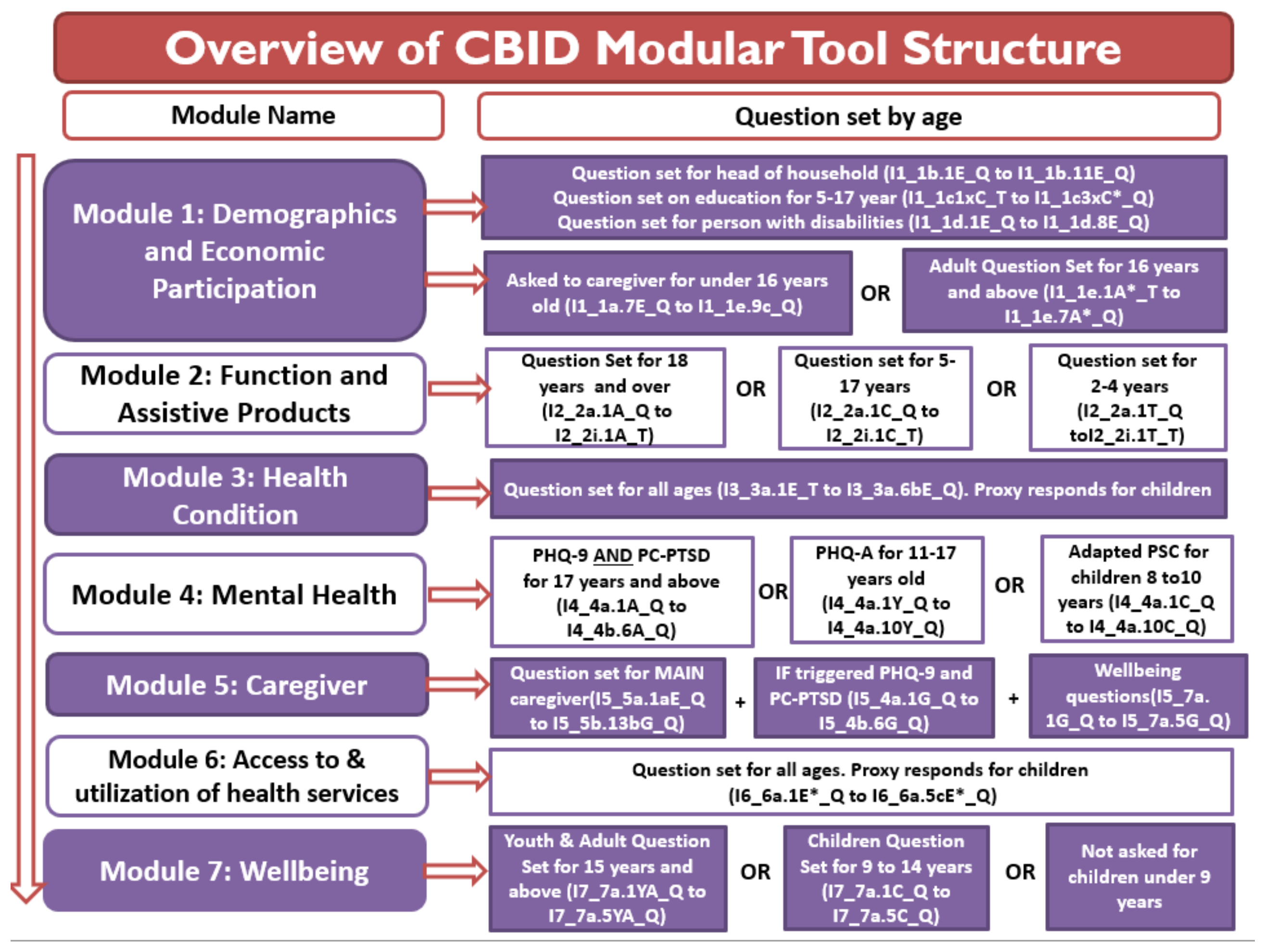
3.2. Content of the Modular Tool
3.3. Development of the Database for Automated Analysis
- I6_6a.3aE_T, I6_6a.4aE_T and/or I6_6a.5aE_T = 0, 1 or 89
- or I6_6a.2E*_T = 0,1,2,3, 6 or 7

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Questions | Response Categories | Code | Comments and Skips |
|---|---|---|---|---|
| I6_6a.1E*_Q | Thinking of the time you were ill last time, what was your first/immediate point of action? (Do not read options. Select one option) | No action | 0 | Go to I6_6a.2E*_T |
| Traditional method by self | 1 | |||
| Western medicine by self | 2 | |||
| Pharmacy/dispensary | 3 | |||
| Public health facilities | 4 | |||
| Private health clinic/ practitioner | 5 | |||
| Community health volunteer in the village | 6 | |||
| Traditional healer (use local term) | 7 | |||
| Other | 8 | |||
| Specify other | (Text) | |||
| I6_6a.2E*_T | Thinking about the illness you had, what did you do when the illness did not go away or worsened? (Do not read options. Select one option) | No action | 0 | Go to I6_6a.3aE_T |
| Traditional method by self | 1 | |||
| Western medicine by self | 2 | |||
| Pharmacy/dispensary | 3 | |||
| Public health facilities | 4 | |||
| Private health clinic/ practitioner | 5 | |||
| Community Health volunteer in the village | 6 | |||
| Traditional healer (use local term) | 7 | |||
| Other | 8 | |||
| Specify other | (Text) | |||
| I6_6a.3aE_T | In the last 3 months, to what extent have you been able to access health services? (Read all options and select one) | As much as needed | 3 | Go to I6_6a.4aE_T |
| Most times | 2 | Go to I6_6a.4aE_T | ||
| Sometimes | 1 | Go to I6_6a.3bE*_Q | ||
| Not at all | 0 | |||
| Have not needed | 4 | Go to I6_6a.4aE_T | ||
| Don’t know | 89 | Go to I6_6a.4aE_T | ||
| I6_6a.3bE*_Q | What are the reasons/difficulties for not being able to access health services as much as you needed? (Do not read options, select all applicable options) | Lack of information/do not know where to go | 1 | Go to I6_6a.3cE*_Q IF more than one response selected in I6_6a.3bE*_Q |
| No services/facilities | 2 | |||
| Too far | 3 | |||
| No transport available | 4 | |||
| Transport not accessible | 5 | |||
| Could not afford the cost of the visit | 6 | |||
| Could not afford the cost of transport | 7 | |||
| Nobody to accompany me | 8 | |||
| Do not like the attitudes of the staff at the facility | 9 | |||
| Was previously badly treated | 10 | |||
| Tried but denied health care | 11 | |||
| Did not think sick enough | 12 | |||
| Other | 13 | |||
| Specify other | (text) | |||
| I6_6a.3cE*_Q | Among the reasons you have listed which one has limited your access to health services the most? (Do not read options. Select one option) | Lack of information/do not know where to go | 1 | When asking the question only list options selected in I6_6a.3bE*_Q Go to I6_6a.4aE_T |
| No services/facilities | 2 | |||
| Too far | 3 | |||
| No transport available | 4 | |||
| Transport not accessible | 5 | |||
| Could not afford the cost of the visit | 6 | |||
| Could not afford the cost of transport | 7 | |||
| Nobody to accompany me | 8 | |||
| Do not like the attitudes of the staff at the facility | 9 | |||
| Was previously badly treated | 10 | |||
| Tried but denied health care | 11 | |||
| Did not think sick enough | 12 | |||
| Other | 13 | |||
| Specify other | (text) | |||
| I6_6a.4aE_T | In the last 3 months, to what extent have you been able to access rehabilitation services and assistive products? (Read all options and select one) | As much as needed | 3 | Go to I6_6a.5aE_T |
| Most times | 2 | Go to I6_6a.5aE_T | ||
| Sometimes | 1 | Go to I6_6a.4bE*_Q | ||
| Not at all | 0 | |||
| Have not needed | 4 | Go to I6_6a.5aE_T | ||
| Don’t know | 89 | Go to I6_6a.5aE_T | ||
| I6_6a.4bE*_Q | What are the reasons/difficulties for not being able to access rehabilitation services and assistive products as much as you needed? (Do not read options and select all applicable options) | Lack of information/do not know where to go | 1 | Go to I6_6a.4cE*_Q IF more than one response selected in I6_6a.4bE*_Q |
| No services/facilities | 2 | |||
| Too far | 3 | |||
| No transport available | 4 | |||
| Transport not accessible | 5 | |||
| Could not afford the cost of the visit | 6 | |||
| Could not afford the cost of transport | 7 | |||
| Nobody to accompany me | 8 | |||
| Do not like the attitudes of the staff at the facility | 9 | |||
| Was previously badly treated | 10 | |||
| Tried but denied health care | 11 | |||
| Did not think sick enough | 12 | |||
| Other | 13 | |||
| Specify other | (text) | |||
| I6_6a.4cE*_Q | Among the reasons you have listed which one has limited your access to rehabilitation services and assistive products the most? (Do not read options. Select one option) | Lack of information/do not know where to go | 1 | When asking the question only list options selected in I6_6a.4bE*_Q Go to I6_6a.5aE_T |
| No services/facilities | 2 | |||
| Too far | 3 | |||
| No transport available | 4 | |||
| Transport not accessible | 5 | |||
| Could not afford the cost of the visit | 6 | |||
| Could not afford the cost of transport | 7 | |||
| Nobody to accompany me | 8 | |||
| Do not like the attitudes of the staff at the facility | 9 | |||
| Was previously badly treated | 10 | |||
| Tried but denied health care | 11 | |||
| Did not think sick enough | 12 | |||
| Other | 13 | |||
| Specify other | (text) | |||
| I6_6a.5aE_T | In the last 3 months, to what extent have you been able to access services (MHPSS *) to help you with stress, anxiety, depression such as, a doctor with specialist skills in mental health or community health worker, peer to peer support or a social club (Read all options and select one) | As much as needed | 3 | Go to I7_1a.1E_Q |
| Most times | 2 | Go to I7_1a.1E_Q | ||
| Sometimes | 1 | Go to I6_6a.5bE*_Q | ||
| Not at all | 0 | |||
| Have not needed | 4 | Go to I7_1a.1E_Q | ||
| Don’t know | 89 | Go to I7_1a.1E_Q | ||
| I6_6a.5bE*_Q | What are the reasons/difficulties for not being able to access to services (MHPSS) to help you with stress, anxiety, depressions as much as you needed? (Do not read options. Select all applicable options) | Lack of information/do not know where to go | 1 | Go to I6_6a.5cE*_Q IF more than one response selected in I6_6a.5bE*_Q |
| No services/facilities | 2 | |||
| Too far | 3 | |||
| No transport available | 4 | |||
| Transport not accessible | 5 | |||
| Could not afford the cost of the visit | 6 | |||
| Could not afford the cost of transport | 7 | |||
| Nobody to accompany me | 8 | |||
| Do not like the attitudes of the staff at the facility | 9 | |||
| Was previously badly treated | 10 | |||
| Tried but denied health care | 11 | |||
| Did not think sick enough | 12 | |||
| Other | 13 | |||
| Specify other | (text) | |||
| I6_6a.5cE*_Q | Among the reasons you have listed which one has limited your access to services (MHPSS) when you have felt stressed, anxious, or depressed the most? (Do not read options. Select one option) | Lack of information/do not know where to go | 1 | When asking the question only list options selected in I6_6a.5bE*_Q Go to I7_1a.1E_Q |
| No services/facilities | 2 | |||
| Too far | 3 | |||
| No transport available | 4 | |||
| Transport not accessible | 5 | |||
| Could not afford the cost of the visit | 6 | |||
| Could not afford the cost of transport | 7 | |||
| Nobody to accompany me | 8 | |||
| Do not like the attitudes of the staff at the facility | 9 | |||
| Was previously badly treated | 10 | |||
| Tried but denied health care | 11 | |||
| Did not think sick enough | 12 | |||
| Other | 13 | |||
| Specify other | (text) |

3.4. Pilot Module
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization; World Bank. World Report on Disability; World Health Organization and The World Bank: Geneva, Switzerland, 2011. [Google Scholar]
- United Nations Economic and Social Commission for Asia and the Pacific. Biwako Millennium Framework: Towards an Inclusive, Barrier-Free and Rights-Based Society for Persons with Disabilities in Asia and the Pacific; Economic and Social Commission for Asia and the Pacific: Otsu City, Shiga, Japan, 2007. [Google Scholar]
- Mitra, S. A data revolution for disability-inclusive development. Lancet Glob. Health 2013, 1, e178–e179. [Google Scholar] [CrossRef] [Green Version]
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development; United Nations: New York, NY, USA, 2015. [Google Scholar]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Madans, J.H.; Loeb, M.E.; Altman, B.M. Measuring disability and monitoring the UN Convention on the Rights of Persons with Disabilities: The work of the Washington Group on Disability Statistics. BMC Public Health 2011, 11, S4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabariego, C.; Oberhauser, C.; Posarac, A.; Bickenbach, J.; Kostanjsek, N.; Chatterji, S.; Officer, A.; Coenen, M.; Chhan, L.; Cieza, A. Measuring Disability: Comparing the Impact of Two Data Collection Approaches on Disability Rates. Int. J. Environ. Res. Public Health 2015, 12, 10329–10351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marella, M.; Busija, L.; Islam, A.; Devine, A.; Fotis, K.; Baker, S.; Sprunt, B.; Edmonds, T.; Huq, N.L.; Cama, A.; et al. Field-testing of the rapid assessment of disability questionnaire. BMC Public Health 2014, 14, 900. [Google Scholar] [CrossRef] [Green Version]
- Marella, M.; Devine, A.; Armecin, G.F.; Zayas, J.; Marco, M.J.; Vaughan, C. Rapid assessment of disability in the Philippines: Understanding prevalence, well-being, and access to the community for people with disabilities to inform the W-DARE project. Popul. Health Metr. 2016, 14, 26. [Google Scholar] [CrossRef] [Green Version]
- Marella, M.; Daveta, M.; Sprunt, B.; Hoq, M.M. Rapid Assessment of Disability Baseline in the Access to Quality Education Program; Access to Quality Education Program: Suva, Fiji, 2015. [Google Scholar]
- Vaughan, C.; Zayas, J.; Devine, A.; Gill-Atkinson, L.; Marella, M.; Garcia, J.; Bisda, K.; Salgado, J.; Sobritchea, C.; Edmonds, T.; et al. W-DARE: A three-year program of participatory action research to improve the sexual and reproductive health of women with disabilities in the Philippines. BMC Public Health 2015, 15, 984. [Google Scholar] [CrossRef] [Green Version]
- Ramachandra, S.S.; Allagh, K.P.; Kumar, H.; Grills, N.; Marella, M.; Pant, H.; Mahesh, D.; Soji, F.; Mani, S.; Murthy, G. Prevalence of disability among adults using rapid assessment of disability tool in a rural district of South India. Disabil. Health J. 2016, 9, 624–631. [Google Scholar] [CrossRef]
- Pryor, W.; Nguyen, L.; Islam, Q.N.; Jalal, F.A.; Marella, M. Unmet Needs and Use of Assistive Products in Two Districts of Bangladesh: Findings from a Household Survey. Int. J. Environ. Res. Public Health 2018, 15, 2901. [Google Scholar] [CrossRef] [Green Version]
- Baker, S.; Reeve, M.; Marella, M.; Roubin, D.; Caleb, N.; Brown, T. Experiences of people with disabilities during and after Tropical Cyclone Pam and recommendations for humanitarian leaders. In Proceedings of the Asia Pacific Humanitarian Leadership Conference Proceedings, Melbourne, Australia, 17 February 2017; pp. 70–78. [Google Scholar]
- World Health Organization; United Nations Educational Scientific and Cultural Organization; International Labour Organization; International Disability Development Consortium. Community-Based Rehabilitation: CBR Guidelines; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Finkenflugel, H.; Wolffers, I.; Huijsman, R. The evidence base for community-based rehabilitation: A literature review. Int. J. Rehabil. Res. 2005, 28, 187–201. [Google Scholar] [CrossRef]
- Hartley, S.; Finkenflugel, H.; Kuipers, P.; Thomas, M. Community-based rehabilitation: Opportunity and challenge. Lancet 2009, 374, 1803–1804. [Google Scholar] [CrossRef]
- Lukersmith, S.; Hartley, S.; Kuipers, P.; Madden, R.; Llewellyn, G.; Dune, T. Community-based rehabilitation (CBR) monitoring and evaluation methods and tools: A literature review. Disabil. Rehabil. 2013, 35, 1941–1953. [Google Scholar] [CrossRef]
- Grandisson, M.; Thibeault, R.; Hébert, M.; Cameron, D. Expert consensus on best evaluative practices in community-based rehabilitation. Disabil. Rehabil. 2016, 38, 499–510. [Google Scholar] [CrossRef]
- Bahia, K.; Delapote, A. Connected Society. The State of Mobile Internet Connectivity 2020; GSMA: London, UK, 2020. [Google Scholar]
- Taylor, K.; Silver, L. Smartphone Ownership Is Growing Rapidly around the World, But Not Always Equally; Pew Research Center: Washigton, DC, USA, 2019. [Google Scholar]
- Hutchings, M.T.; Dev, A.; Palaniappan, M.; Srinivasan, V.; Ramanathan, N.; Taylor, J.; Ross, N.; Luu, P. mWASH: Mobile Phone Applications for the Water, Sanitation, and Hygiene Sector; Nexleaf Analytics & the Pacific Institute: Los Angeles, CA, USA, 2012; pp. 1–115. [Google Scholar]
- Gebreyesus, G.; Dessie, T.; Wamalwa, M.; Agaba, M.; Benor, S.; Mwai, O. Harnessing “ODK Collect” on Smartphones for On-Farm Data Collection in Africa: The ILRI-BecA Goat Project. In ILRI APM 2013; ILRI APM: Addis Ababa, Ethiopia, 2013. [Google Scholar]
- Bernabe-Ortiz, A.; Curioso, W.H.; Gonzales, M.A.; Evangelista, W.; Castagnetto, J.M.; Carcamo, C.P.; Hughes, J.P.; Garcia, P.J.; Garnett, G.P.; Holmes, K.K. Handheld computers for self-administered sensitive data collection: A comparative study in Peru. BMC Med. Inform. Decis. Mak. 2008, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, M.; Solomon, W.; Singh, Y.; Doherty, T.; Chopra, M.; Ijumba, P.; Tsai, A.C.; Jackson, D. The use of mobile phones as a data collection tool: A report from a household survey in South Africa. BMC Med. Inform. Decis. Mak. 2009, 9, 51. [Google Scholar] [CrossRef]
- Braun, R.; Catalani, C.; Wimbush, J.; Israelski, D. Community health workers and mobile technology: A systematic review of the literature. PLoS ONE 2013, 8, e65772. [Google Scholar] [CrossRef] [PubMed]
- World Education Inc. USAID Okard. Available online: https://laos.worlded.org/usaid-okard/ (accessed on 15 September 2021).
- United Nations. United Nations Convention on the Rights of Persons with Disabilities. Available online: https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities.html (accessed on 15 June 2012).
- Waddington, L.; Priestley, M. A human rights approach to disability assessment. J. Int. Comp. Soc. Policy 2021, 37, 1–15. [Google Scholar] [CrossRef]
- Nguyen, L.; Pryor, W.; Marella, M.; Robinson, A.; Smith, F. Community Based Inclusive Development (CBID) Demonstration Model Impact Assessment—Baseline Survey Report; World Education Inc.: Vientiane, Laos, 2020. [Google Scholar]
- Lao Statistics Bureau. Results of Population and Housing Census 2015; Ministry of Planning and Investment: Vientiane, Laos, 2016.
- Lao Statistics Bureau. Lao Social Indicator Survey II 2017, Survey Findings Report; Lao Statistics Bureau and UNICEF: Vientiane, Laos, 2018.
- World Health Organization. Capturing the Difference We Make: Community-Based Rehabilitation Indicators Manual; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Washington Group on Disability Statistics. Understanding and Interpreting Disability as Measured Using the Washington Group Short Set of Questions. Available online: http://www.cdc.gov/nchs/data/washington_group/meeting8/interpreting_disability.pdf (accessed on 8 May 2011).
- Cappa, C.; Mont, D.; Loeb, M.; Misunas, C.; Madans, J.; Comic, T.; de Castro, F. The development and testing of a module on child functioning for identifying children with disabilities on surveys. III: Field testing. Disabil. Health J. 2018, 11, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Üstün, T.B.; Kostanjsek, N.; Chatterji, S.; Rehm, J. Measuring Health and Disability: Manual for WHO Disability Assessment Schedule WHODAS 2.0; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- World Health Organization. Advancing Data Collection on Assistive Technology. Available online: https://www.who.int/tools/ata-toolkit (accessed on 15 September 2021).
- Piyasil, V.; Ketuman, P.; Plubrukarn, R.; Jotipanut, V.; Tanprasert, S.; Aowjinda, S.; Thaeeromanophap, S. Post traumatic stress disorder in children after tsunami disaster in Thailand: 2 years follow-up. Med. J. Medi. Assoc. Thail. 2007, 90, 2370. [Google Scholar]
- Pagano, M.E.; Cassidy, L.J.; Little, M.; Murphy, J.M.; Jellinek, S.M. Identifying psychosocial dysfunction in School-Age children: The pediatric symptom checklist as a Self-Report measure. Psychol. Sch. 2000, 37, 91–106. [Google Scholar] [CrossRef]
- Richardson, L.P.; McCauley, E.; Grossman, D.C.; McCarty, C.A.; Richards, J.; Russo, J.E.; Rockhill, C.; Katon, W. Evaluation of the Patient Health Questionnaire-9 Item for detecting major depression among adolescents. Pediatrics 2010, 126, 1117–1123. [Google Scholar] [CrossRef] [Green Version]
- Lotrakul, M.; Sumrithe, S.; Saipanish, R. Reliability and validity of the Thai version of the PHQ-9. BMC Psychiatry 2008, 8, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cameron, R.P.; Gusman, D. The primary care PTSD screen (PC-PTSD): Development and operating characteristics. Prim. Care Psychiatry 2003, 9, 9–14. [Google Scholar]
- Joseph, S.; Becker, S.; Elwick, H.; Silburn, R. Adult carers quality of life questionnaire (AC-QoL): Development of an evidence-based tool. Ment. Health Rev. J. 2012, 17, 57–69. [Google Scholar] [CrossRef]
- Gadermann, A.M.; Schonert-Reichl, K.A.; Zumbo, B.D. Investigating validity evidence of the satisfaction with life scale adapted for children. Soc. Indic. Res. 2010, 96, 229–247. [Google Scholar] [CrossRef]




| Number | Questions | Response Categories | Code | Comments and Skips |
|---|---|---|---|---|
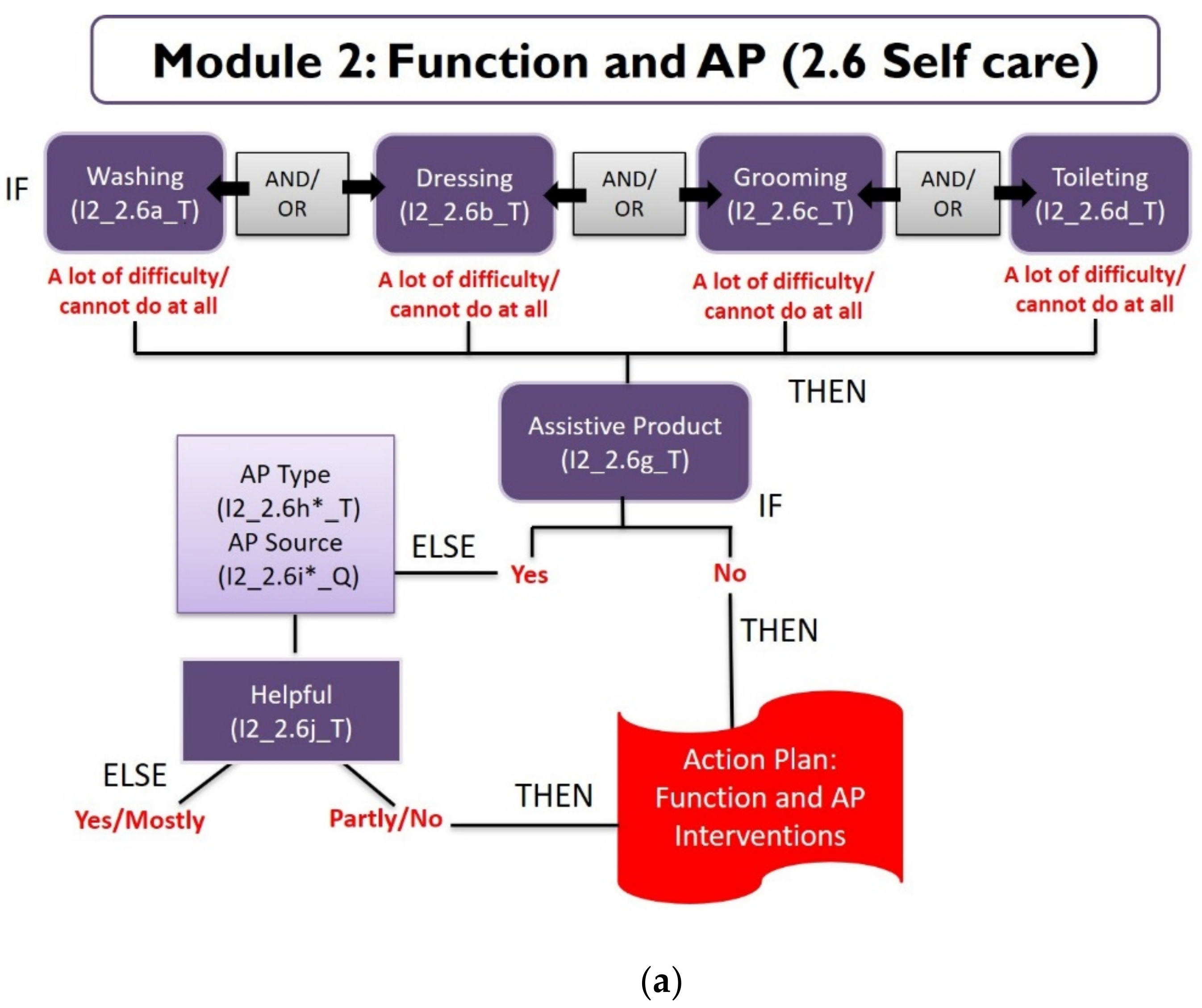
| 2.6a | Do you have difficulty washing your whole body? (read all options and select one) | No difficulty | 0 | Go to 2.6b |
| Some difficulty | 1 | |||
| A lot of difficulty | 2 | |||
| Cannot do at all | 3 | |||
| Not applicable | 99 | |||
| 2.6b | Do you have difficulty getting dressed? (read all options and select one) | No difficulty | 0 | Go to 2.6c |
| Some difficulty | 1 | |||
| A lot of difficulty | 2 | |||
| Cannot do at all | 3 | |||
| Not applicable | 99 | |||
| 2.6c | Do you have difficulty grooming (e.g., brushing hair, shaving, cutting finger/toe nails and cleaning teeth)? (read all options and select one) | No difficulty | 0 | Go to 2.6d |
| Some difficulty | 1 | |||
| A lot of difficulty | 2 | |||
| Cannot do at all | 3 | |||
| Not applicable | 99 | |||
| 2.6d | Do you have difficulty using the toilet? (read all options and select one) | No difficulty | 0 | Go to 2.6e |
| Some difficulty | 1 | |||
| A lot of difficulty | 2 | |||
| Cannot do at all | 3 | |||
| Not applicable | 99 | |||
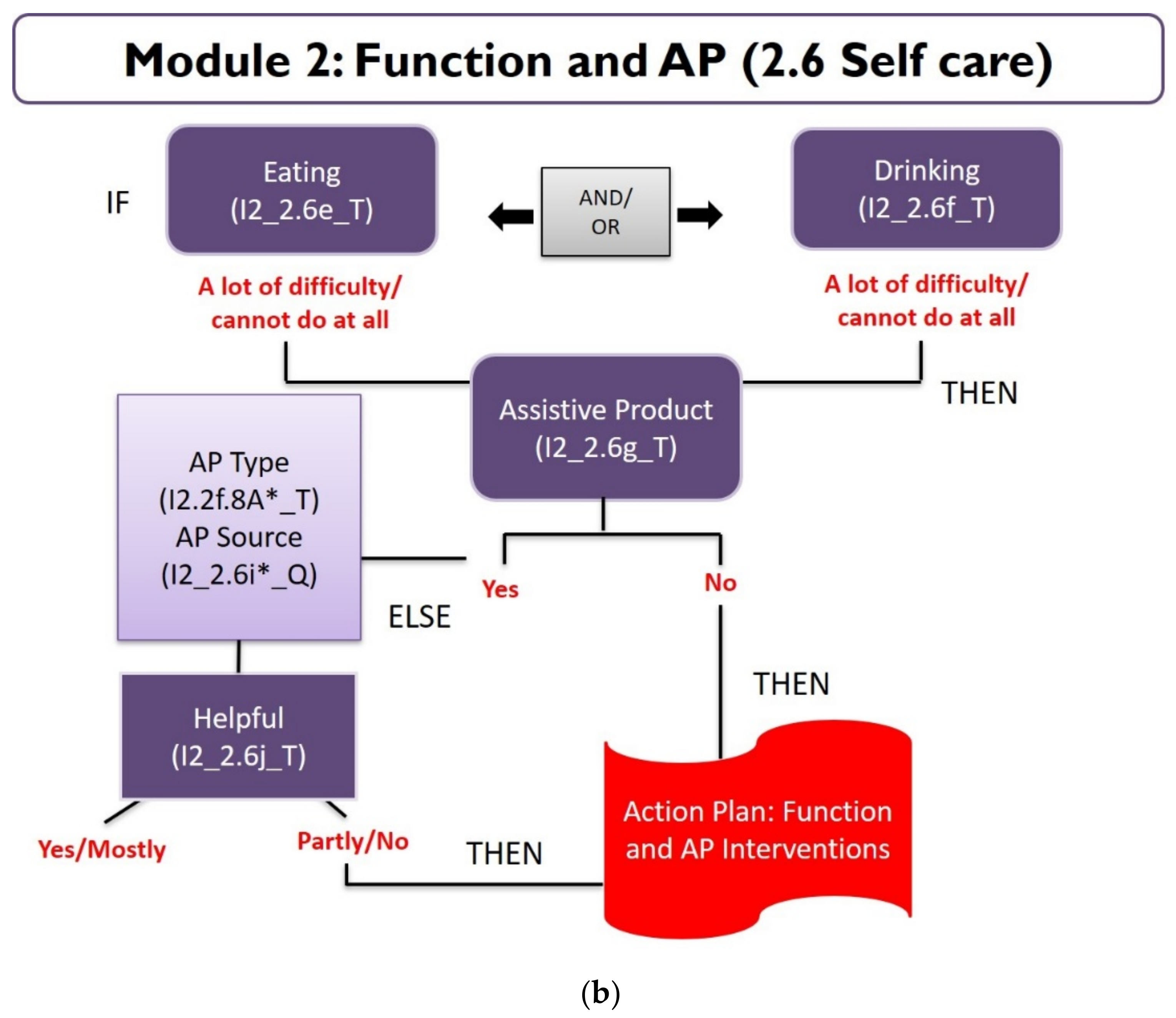
| 2.6e | Do you have difficulty eating/feeding yourself? (read all options and select one) | No difficulty | 0 | Go to 2.6e |
| Some difficulty | 1 | |||
| A lot of difficulty | 2 | |||
| Cannot do at all | 3 | |||
| Not applicable | 99 | |||
| 2.6f | Do you have difficulty drinking by yourself? (read all options and select one) | No difficulty | 0 | Go to 2.6e |
| Some difficulty | 1 | |||
| A lot of difficulty | 2 | |||
| Cannot do at all | 3 | |||
| Not applicable | 99 | |||
| 2.6g | Do you use any assistive products to help you eat; for toileting or washing; to dress by yourself or to manage other daily activities? | Yes | 1 | Go to 2.6h |
| No | 0 | Go to 2.7a | ||
| 2.6h | Which assistive products do you use? (select all applicable options) | Orthoses, upper limb | 1 | Q2.6i |
| Prostheses, upper limb | 2 | |||
| Hand rails/grab bars | 3 | |||
| Incontinence products, absorbent | 4 | |||
| Chairs for shower/bath/toilet | 5 | |||
| Adapted cutlery | 6 | |||
| Adapted cooking tools | 7 | |||
| Transfer board | 8 | |||
| Other—device not listed here | 9 | |||
| Please specify other | (text) | |||
| 2.6i | Where did you get your product [insert name of the selected product in Q2.6h]? read all options and select one) | Rehabilitation center | 1 | Go to Q2.6j Repeat Q2.6i and 2.6j IF Q2.6h is more than one assistive product |
| Public health facility | 2 | |||
| Private health facility | 3 | |||
| Local/private market | 4 | |||
| Pharmacist | 5 | |||
| Made by local handyman | 6 | |||
| NGO/Charity | 7 | |||
| Purchased outside Laos | 8 | |||
| Made by self | 9 | |||
| Made by family member/friend | 10 | |||
| Other | 11 | |||
| Please specify other | (text) | |||
| 2.6j | Does the assistive product you use help you eat; for toileting or washing; to dress by yourself or to manage other daily activities? (read all options and select one) | Yes | 1 | Go to Q2.7a |
| Mostly | 2 | |||
| Partly/To an extent | 3 | |||
| No | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marella, M.; Koolmees, D.; Vongvilay, C.; Frank, B.; Pryor, W.; Smith, F. Development of a Digital Case Management Tool for Community Based Inclusive Development Program. Int. J. Environ. Res. Public Health 2021, 18, 11000. https://doi.org/10.3390/ijerph182011000
Marella M, Koolmees D, Vongvilay C, Frank B, Pryor W, Smith F. Development of a Digital Case Management Tool for Community Based Inclusive Development Program. International Journal of Environmental Research and Public Health. 2021; 18(20):11000. https://doi.org/10.3390/ijerph182011000
Chicago/Turabian StyleMarella, Manjula, Donna Koolmees, Chandalin Vongvilay, Bernard Frank, Wesley Pryor, and Fleur Smith. 2021. "Development of a Digital Case Management Tool for Community Based Inclusive Development Program" International Journal of Environmental Research and Public Health 18, no. 20: 11000. https://doi.org/10.3390/ijerph182011000