
Winning Conditions for the Adoption and Maintenance of Long-Term Healthy Lifestyles According to Physical Activity Students


Abstract
:1. Introduction
1.1. Improving Health by Promoting Healthy Lifestyles
1.2. Current State of Research on Healthy Lifestyles and Theoretical Models in Health Promotion
1.3. Limitations of Studies and Their Methodologies to Study Long-Term HLHs
1.4. Relevance of the Study
1.4.1. Documenting the Positive Experiences
1.4.2. Use of a Long-Term Methodology through a Qualitative Design
1.4.3. Use of a Methodology That Works with Reverse Engineering (Chaubet et al., 2016)
1.5. Research Question and Objectives
- To describe the pathways that led physical and health education (PE) and Master of Science students in Physical Activity (M) to adopt and maintain HLHs and to characterize the forms of change in or maintenance of these HLHs;
- To identify the winning conditions in the adoption and maintenance of HLHs among these students and characterize them;
- To integrate the winning conditions into a conceptual model of HLH adoption and maintenance.
2. Methods
2.1. Research Design
2.2. Participants and Recruitment
2.3. Instrumentation and Data Collection
2.4. Analyses
3. Results
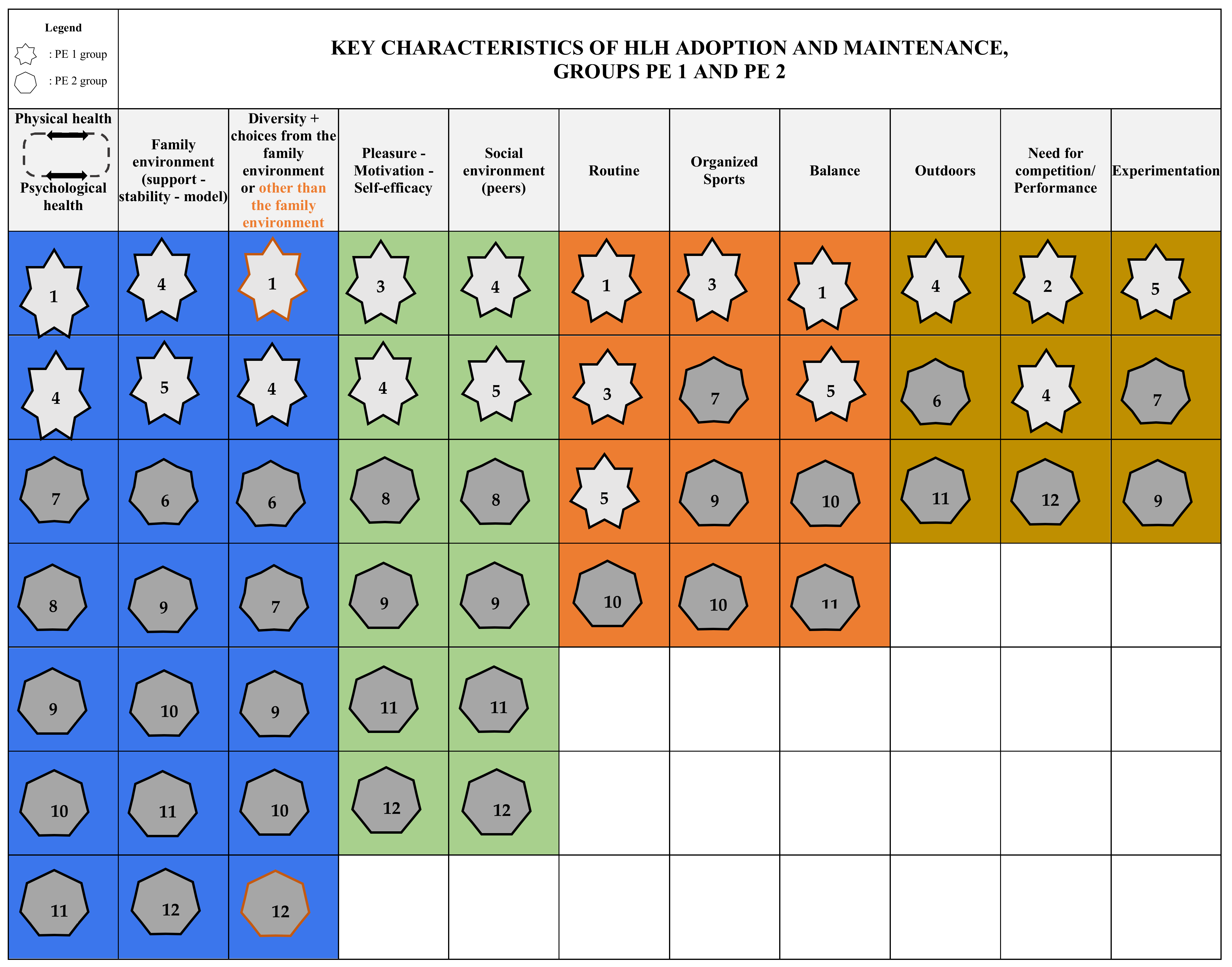
3.1. Summary of the Winning Conditions for the Adoption and Maintenance of Healthy Lifestyle Habits
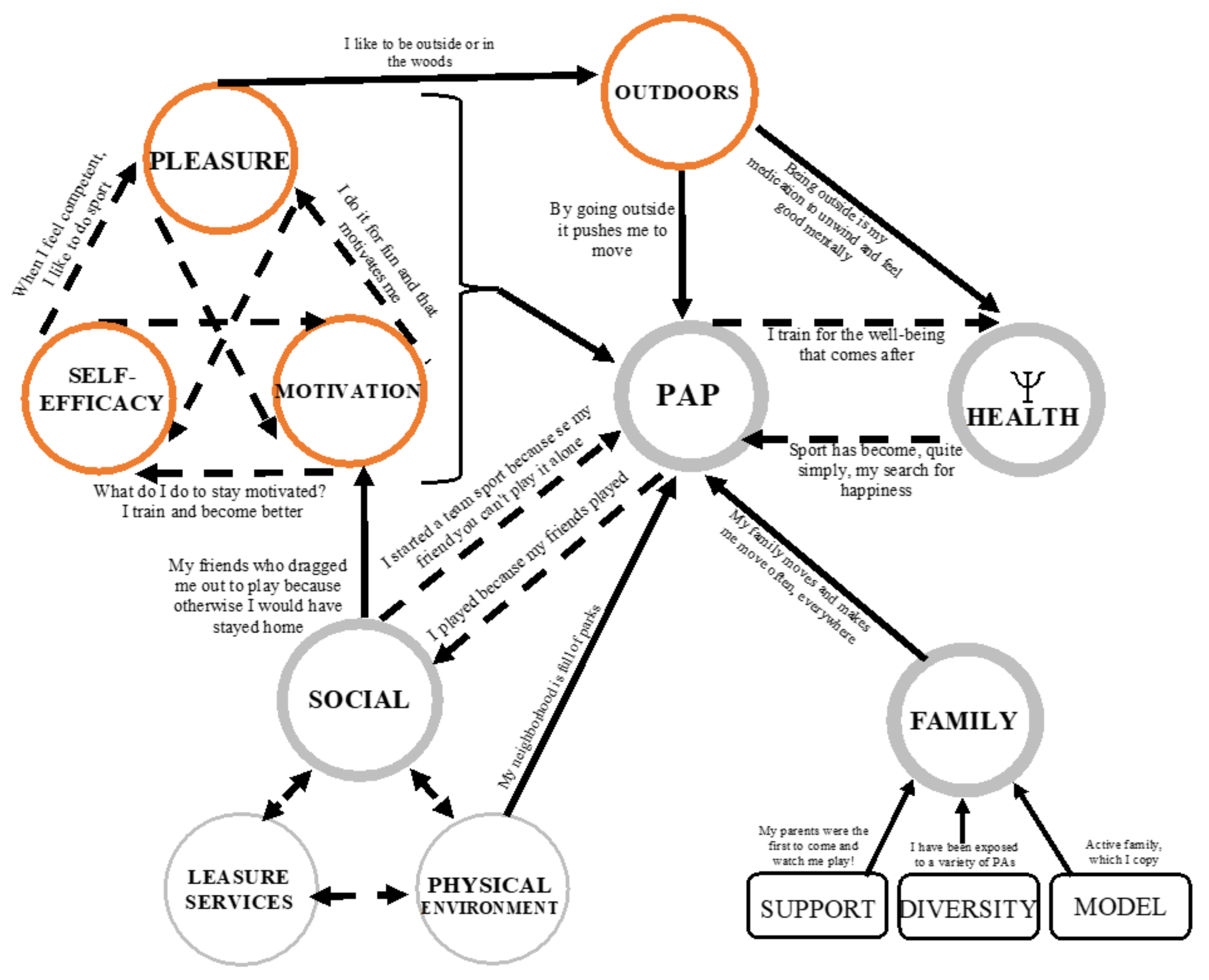
3.2. Diagram of the Winning Conditions for the Adoption and Maintenance of Healthy Lifestyle Habits
3.2.1. Blue Winning Conditions (Very Strong) and Their Links
A Strong Link between Physical Activity Participation and Psychological Health
YÉD2: I have always found over the years that I felt better and had better overall mental health when I exercised just a little bit, every day. This is something I discovered quite early on, but I confirm it [...]
MAK1: Sport has always been part of my life since I was little. So it’s something I do for fun, it’s a hobby, it’s a need to feel good. So it’s been integrated since I was really little.
The Family with Its Support, Diversity and Role Model as a Predominant Element in the Adoption of Healthy Lifestyle Habits
SÉD1: [...] Every weekend we did something new, especially in nature. We’d go hiking, we’d go mushroom picking, unusual things, fishing, hunting. Uh they signed me up for field hockey, soccer, baseball when I went to the States. Uh... I had a chance to try out a lot of sports [...]
ÉD2: [...] Of course I couldn’t do all the sports at the same time, I would have liked that, but they said, Perfect, we’ll support you. And I did other sports as well and every time they were behind me.
3.2.2. Green (Strong) Winning Condition and Its Links
The Social Environment as a Lever for the Physical Activity Participation
OÉD2: [...]… sometimes I was not motivated. Then my friends would tell me “oh, let’s go, let’s go do some sports” and I would go and finally I was happy to go but otherwise I wouldn’t have gone by myself.
NK1: And when you go outside, well, you find a lot of... I played baseball very quickly from the age of 5–6 at the local park and that made me want to play [...] Without the social infrastructure where people were outside, there might not have been as many hooks either.
Mk1: [...] Everyone is there at the same time: the arena, the baseball field, the park. So the kind of location creates a kind of excitement to go outside and play with our friends outside and then bike to our parks.
3.2.3. Orange (Medium Strength) Winning Conditions and Their Links
Pleasure, Motivation and Self-Efficacy Intimately Linked
AÉD2: It was also a need to... Not a need but actually I felt successful, I felt competent in what I was doing so I was just enjoying doing the sport by myself.
Integration of the Outdoors
MTK1: But what I found important to integrate is the outdoors, so to really have a contact with nature, that’s primordial and also mental health. I think that stress is such a major problem.
3.2.4. Yellow Winning Condition (Fairly Strong) and Its Links
Intrinsic Awareness of the Benefits of Physical Activity on Physical and Psychological Health
VIK1: It was just implanted, it was just natural, I didn’t really ask myself any questions. [...] And when I got to college, university, I just realized how important it was.
AK1: And at the university, with kin[esiology] it was not really my appearance, but it was more when I train, I have more energy, as I feel better, I have less headache. So it seems that my evolution was more external and now it seems more internal.
3.2.5. The Purple Winning Conditions (Strong Enough) and Their Links
Role of Routine, Balance (Physical-Psychological-Social)
GÉD1: [...] I changed that very habit. So I opened a little more time for my family, for my friends and to go towards new activities. And that, in my eyes, is a healthier way of life than what I had before, where I was focused on one thing and one thing only: sports. So, this is a turning point. [...] But I still keep in mind the learning that I did, so I always keep time for the other spheres of life.
3.2.6. Summary of the Winning Conditions for the Adoption and Maintenance of Healthy Lifestyle Habits
3.3. Summary of Findings
4. Discussion
4.1. Preliminary Model of Healthy Lifestyle Habit Adoption and Maintenance
4.2. Major Findings and Scientific Literature
4.2.1. Milestone 1: Family Environment as the First Pillar of Healthy Lifestyle Habit Adoption
4.2.2. Milestone 2: Social and Physical Environment as Facilitators to HLH Maintenance
4.2.3. Milestone 3: The Individual and His or Her Conscious Choices, Influenced by the Past and Dictated by the Desire to Be Physically and Mentally Healthy
4.2.4. Milestone 4: A Timeline Based on Autonomy and Environments in the Ideal HLH Pathway
4.3. Research Perspectives Based on the Results of the Study
4.4. Limits
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A. Key Features of Healthy Lifestyle Habit Adoption and Maintenance, Groups PE1 and PE2
Appendix B. Key Features of Healthy Lifestyle Habit Adoption and Maintenance, Group M1

Appendix C. Definitions and Precisions

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Themes | Definitions/Precisions | Extracts |
|---|---|---|
| Support | When the family environment is supportive and the youth feels a sense of involvement on their part. | JSÉD2: Super big support from parents [...] for any sport my parents were open: "you want to do sports, well you’re going to do it because it’s good for you". |
| Stability | A family setting where the environment offers the youth stability leading to the integration of healthy lifestyle habits. | EDG2: If you have a stable environment, and I’m speaking for myself, you have parents who are there to support you and who will always encourage you in what you are [...] that helps you a lot in your personal development as a person, in how you become. |
| Model | When a young person’s family culture is focused on healthy living and they want to replicate that in their own life. | AED2: My father is a great sportsman, he used to canoe. My mother was also a canoeist, so... I think it’s really the family culture that pushed me to develop healthy habits. JK1: Let’s say when I was a kid, I’m the last one in a family of 4, so I always learned by watching others and then my whole family did sports, like taekwado, field hockey, etc. [...] There was a lot of sport in my family. [...] There was my sister that I always copied a lot. |
| Diversity | Several possibilities are offered to the young person and he experiments with them. | SÉD1: I’ve had the chance to try several sports, so I find that I’m quite diversified as a person now, I have... That makes me want to discover more. CK1: [...]So at that time there was soccer with the city so go soccer, go gymnastics, go this, go that. |
| Choice | They can choose what they want to be involved in, such as what sport to play. | JPÉD2: Then I remember in elementary school that all my friends were playing hockey.I was maybe in third grade and I was bugging my parents and I was the one who said: "I want to play hockey" and that’s when it really changed my life because if I had continued with soccer I might have stopped. |
| Social environment | The social context that has an impact on healthy lifestyle habits, such as peers, the sports team, etc. | OÉD2: [...] sometimes I was not motivated. Well, my friends would say to me, "Oh, let’s go, let’s go play some sports," and I would go, and in the end I was happy to go, but otherwise I wouldn’t have gone alone. And then, team sports are not played alone, so you need peers to play team sports, so that helps too. |
| Routine | Organizing one’s schedule with a view to integrating healthy lifestyle habits. | NK1: I’ve been walking or biking to work every day for the past 3 years. [...] It’s a routine, it allows me to do 45 minutes of activity. FED1: [...] in the morning I often go and do a small, very simple weight training routine but at least I do it every day. |
| Balance | The global health which is based on the maintenance of a balance between several spheres of the life, in periphery and in complementarity with the practice of physical activity (social, psychological). | GÉD1: I have opened up a little more time for my family, for my friends, and for new activities. I think it’s a healthier lifestyle than what I had before, where I was focused on one thing and one thing only, sports. [...] I always keep time for the other spheres of life. CK1: I have found a physical activity that I enjoy and that fulfills me socially, physically and mentally. |
| Physical and psychological health | These two dimensions of health are linked in the sense that one leads to the other in a cyclical manner. | AED2: I went to train every day outside, in the sun. It allowed me to make decisions, it allowed me to regain my overall health, psychologically and everything. MAK1: Then today I think that I train in a way, I do a lot of hiking, I like to be in the woods, I do yoga and then running, then it’s really to manage my mood and then manage... That’s it, to be well. |
| Intrinsic awareness of benefits | Awareness of one’s choices in terms of HLH, which makes one realize the importance of one’s actions. This awareness was once influenced by external elements, such as family, and now comes from within. It can occur suddenly or after a prolonged break from PA (injury, independence, etc.) | CK1: I like couldn’t walk like the world for a year. [...] to have something taken away that you know is good for you pi that you know makes you feel good is like. I can’t wait for it to come back. So as a result of that I put even more...actually I kind of became aware of how important it is to take care of your body and everything really. JK1: After I went to university, when I left I discovered more...at university, yes, you become aware of "okay, it’s cool, I’m already moving", then you learn why it’s fun to move, then when I was in Toronto I really stopped moving, then I understood why it was important to move because I stopped for the first time in my life. So that made me start again, I didn’t feel well, I wasn’t sleeping. |
| Physical environment | The proximity and quality of outdoor and indoor facilities that support an active lifestyle. | Mk1: [...] Everyone is there at the same time; the arena, the baseball field, the park. So the kind of location creates a kind of excitement to go outside and play with our friends outside and then bike to our parks. JK1: In Toronto, for real, the bike paths and all that is really better developed, it’s fun to ride a bike, there’s a bike culture that is incredible. |
| Outdoors | Outdoor activity (sport practiced outdoors, in nature or not, camping, etc.). | AÉD2: For my psychological health, uh, a rather determining change that I had was this summer when I was in nature all summer, really in the forest. Access to water, to a lake etc. So that just made me realize again how important it is to be surrounded by nature and how it has psychological benefits. EDG1: Every weekend we did something new, especially in nature. We would go hiking, we would go mushroom picking, unusual things, fishing, hunting. |
Appendix D. Winning Conditions for Healthy Lifestyle Habit Adoption and Maintenance, Groups PE1 and PE2

Appendix E. Winning Conditions for Healthy Lifestyle Habit Adoption and Maintenance, Group M1

Appendix F. Questions for the Interviews and Focus Groups (French Version)
| QUESTION DE RECHERCHE : Quelles sont les conditions gagnantes de l’adoption et du maintien de saines habitudes de vie selon les parcours racontés et illustrés par des étudiants en éducation physique et à la santé et en sciences de l’activité physique? | ||
|---|---|---|
| OBJECTIFS DE RECHERCHES | THÈMES | QUESTIONS |
| Objectif 1: Décrire les parcours qui ont mené des étudiants en éducation physique et à la santé, en kinésiologie, en danse et en kinanthropologie à l’adoption et au maintien de saines habitudes de vie, et caractériser les formes du changement et du maintien de celles-ci. |
|
|
| Objectif 2: Repérer chez ces étudiants les types de conditions gagnantes d’adoption et de maintien et les caractériser (expériences cumulatives? Transformatrices ? Autres ?) |
|
|
| Objectif 3: Intégrer les conditions gagnantes des parcours dans un modèle préliminaire de l’adoption et du maintien de saines habitudes de vie. | ||
References
- Sapin, M.; Spini, D.; Widmer, E. Les Parcours de Vie: De L’Adolescence au Grand Age; Collection Le Savoir Suisse; Presses Polytechniques et Univer-Sitaires Romandes: Lausanne, Switzerland, 2007; Volume 39. [Google Scholar]
- Burton-Jeangros, C.; Cullati, S.; Sacker, A.; Blane, D. A Life Course Perspective on Health Trajectories and Transitions; Springer International Publishing: Midtown Manhattan, New York, NY, USA, 2015. [Google Scholar]
- Craigie, A.M.; Lake, A.; Kelly, S.; Adamson, A.; Mathers, J.C. Tracking of Obesity-Related Behaviours from Childhood to Adulthood: A Systematic Review. Maturitas 2011, 70, 266–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, A.S.; Mulder, C.; Twisk, J.W.R.; Van Mechelen, W.; Chinapaw, M.J.M. Tracking of Childhood Overweight into Adulthood: A Systematic Review of The Literature. Obes. Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Telama, R.; Yang, X.; Leskinen, E.; Kankaanpää, A.; Hirvensalo, M.; Tammelin, T.; Viikari, J.S.A.; Raitakari, O.T. Tracking of Physical Activity from Early Childhood through Youth into Adulthood. Med. Sci. Sports Exerc. 2014, 46, 955–962. [Google Scholar] [CrossRef] [PubMed]
- WHO. Report of the Commission on Ending Childhood Obesity; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Colley, R.C.; Carson, V.; Garriguet, D.; Janssen, I.; Roberts, K.C.; Tremblay, M.S. Activité Physique des Enfants et des Jeunes au Canada: Résultats D’accélérométrie de l’Enquête Canadienne Sur les Mesures de la Santé de 2007–2015. Rapp. Santé 2017, 28, 14–23. [Google Scholar]
- Gadais, T. Les Stratégies D’intervention Pour Aider Les Jeunes A Gérer Leur Pratique D’activité Physique. Une Revue De La Littérature. Staps 2015, 109, 57–77. [Google Scholar] [CrossRef]
- Gadais, T.; Rioux, M.-A.; Dionne, S.; Laurencelle, L.; Nadeau, L. Does Better Perception of Knowledge about Physical Activity Give Youth More Opportunities to be Active? Health Behav. Policy Rev. 2017, 4, 339–356. [Google Scholar] [CrossRef]
- Graham, H.; White, P. Social Determinants and Lifestyles: Integrating Environmental and Public Health Perspectives. Public Healh 2016, 141, 270–278. [Google Scholar] [CrossRef]
- Nolin, B. Niveau D’activite Physique de a Population Québécoise: Pas D’amélioration Depuis 2005. In Direction Du Sport, Du Loisir Et De L’activite Physique, Ministère De l’Éducation, De l’Enseignement Supérieur Et De La Recherche; Gouvernement du Québec: Québec, QC, Canada, 2015. [Google Scholar]
- Gourlan, M.; Bernard, P.; Bortolon, C.; Romain, A.J.; Lareyre, O.; Carayol, M.; Ninot, G.; Boiché, J. Efficacy of Theory-Based Interventions to Promote Physical Activity. A Meta-Analysis of Randomised Controlled Trials. Healh Psychol. Rev. 2015, 10, 50–66. [Google Scholar] [CrossRef]
- Ajzen, I. The Theory of Planned Behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Godin, G. Le Changement des Comportements de Santé. In Traité de Psychologie de la Santé; Dunod: Montréal, QC, Canada, 2002; pp. 375–388. [Google Scholar]
- Godin, G. Les comportements dans le domaine de la santé; Les presses de l’Université de Montréal: Montréal, QC, Canada, 2012. [Google Scholar]
- Deci, E.; Ryan, R.M. The General Causality Orientations Scale: Self-Determination in Personality. J. Res. Pers. 1985, 19, 109–134. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-Determination Theory and the Facilitation of Intrinsic Motivation, Social Development, and Well-Being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design. Am. Psychol. 1979, 32, 513–531. [Google Scholar] [CrossRef]
- Sallis, J.F.; Owen, N. Ecological Models of Health Behavior. In Health Behavior: Theory, Research, and Practice, 5th ed.; Jossey-Bass: San Franscico, CA, USA, 2015; pp. 43–64. [Google Scholar]
- Turcotte, S.; Gaudreau, L.; Otis, J. Démarche de Modélisation de L’intervention en Education a la Santé Incluse en Education Physique. Staps 2007, 3, 63–78. [Google Scholar] [CrossRef]
- Beaudoin, C.; Rivard, M.; Grenier, J.; Caty, D. Les enjeux de l’intégration de l’éducation à la santé à l’école primaire: L’apport de l’ÉPS au Québec, en Ontario et en France. In Coconstruire des Savoirs Les Métiers d’Intervenants dans les APS Besançon; Presses Universitaires de Franche-Comté: Besançon, France, 2008; pp. 317–333. [Google Scholar]
- Flynn, M.A.T.; McNeil, D.A.; Maloff, B.; Mutasingwa, D.; Wu, M.; Ford, C.; Tough, S.C. Reducing Obesity and Related Chronic Disease Risk in Children and Youth: A Synthesis of Evidence with ’Best Practice’ Recommendations. Obes. Rev. 2006, 7, 7–66. [Google Scholar] [CrossRef]
- Spinola e Castro, A.M. Interventions for Preventing Obesity in Children. Sao Paulo Med. J. 2014, 132, 128–129. [Google Scholar]
- Wolfenden, L.; Jones, J.; Williams, C.; Finch, M.; Wyse, R.; Kingsland, M.; Tzelepis, F.; Wiggers, J.H.; Williams, A.J.; Seward, K.; et al. Strategies to Improve the Implementation of Healthy Eating, Physical Activity and Obesity Prevention Policies, Practices or Programmes within Childcare Services. Cochrane Database Syst. Rev. 2016, 10, CD011779. [Google Scholar] [CrossRef]
- Dobbins, M.; Husson, H.; DeCorby, K.; LaRocca, R.L. School-Based Physical Activity Programs for Promoting Physical Activity and Fitness in Children and Adolescents Aged 6 To 18. Cochrane Database Syst. Rev. 2013, 2013, CD007651. [Google Scholar] [CrossRef]
- Giacomini, M.K.; Cook, D.J. Users’ Guides to the Medical Literature: XXIII. Qualitative Research in Health Care B. What Are the Results and How Do They Help Me Care for My Patients? Evidence-Based Medicine Working Group. JAMA 2000, 284, 478–482. [Google Scholar] [CrossRef]
- Hung, T.T.M.; Chiang, V.; Dawson, A.; Lee, R.L. Understanding of Factors that Enable Health Promoters in Implementing Health-Promoting Schools: A Systematic Review and Narrative Synthesis of Qualitative Evidence. PLoS ONE 2014, 9, e108284. [Google Scholar] [CrossRef]
- Kwasnicka, D.; Dombrowski, S.U.; White, M.; Sniehotta, F.F. Theoretical Explanations for Maintenance of Behaviour Change: A Systematic Review of Behaviour Theories. Health Psychol. Rev. 2015, 10, 277–296. [Google Scholar] [CrossRef]
- Tessier, C.; Comeau, L.; Institut National De Santé Publique du Québec. Direction du Développement des Individus et des C. In Le Développement des Enfants et des Adolescents Dans une Perspective de Promotion de la Santé et de Prévention en Contexte Scolaire; Institut National De Santé Publique Du Québec: Quebec City, QC, Canada, 2017; p. 55. [Google Scholar]
- Langford, R.; Bonell, C.; Jones, E.H.; Pouliou, T.; Murphy, S.; Waters, E.; Komro, A.K.; Gibbs, L.; Magnus, D.; Campbell, R. The World Health Organization’s Health Promoting Schools Framework: A Cochrane Systematic Review and Meta-Analysis. BMC Public Healh 2015, 15, 130. [Google Scholar] [CrossRef] [Green Version]
- McQueen, D.V.; Anderson, L.M. Données Probantes et Evaluation des Programmes en Promotion de la Santé. Ruptures Rev. Transdiscipl. En Santé 2000, 7, 79–98. [Google Scholar]
- Pluskota, A. The Application of Positive Psychology in the Practice of Education. SpringerPlus 2014, 3, 147. [Google Scholar] [CrossRef] [Green Version]
- Cooperrider, D.L.; Whitney, D. A Positive Revolution in Change: Appreciative Inquiry. In Handbook of Organizational Behavior, Revised and Expanded; Routledge: London, UK, 2001; pp. 611–630. [Google Scholar]
- Mishra, P.; Bhatnagar, J. Appreciative Inquiry: Models & Applications. Indian J. Ind. Relat. 2012, 47, 543–558. [Google Scholar]
- Chaubet, P.; Correa Molina, E.; Gervais, C.; Grenier, J.; Verret, C.; Trudelle, S. Vers une Démarche D’ingénierie Inverse pour Etudier la Réflexion Sur la Pratique et Ses Situations de Déclenchement. Illustration Sur Quatre Etudes. Approch. Inductives 2016, 3, 91–124. [Google Scholar] [CrossRef] [Green Version]
- Yin, R.K. Case Study Research: Design and Methods (Applied Social Research Methods); Sage Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Paillé, P.; Mucchielli, A. L’analyse thématique. In L’analyse Qualitative en Sciences Humaines et Sociales; Armand Colin: Paris, France, 2012. [Google Scholar] [CrossRef]
- Savoie-Zajc, L. Comment Peut-On Construire en Echantillonnage Scientifiquement Valide? Rech. Qual. 2007, 5, 99–111. [Google Scholar]
- Baribeau, C.; Royer, C. L’entretien Individuel en Recherche Qualitative: Usages et Modes de Présentation Dans la Revue Des Sciences de L’éducation. Rev. Ivoir. Sci. Educ. 2012, 38, 23–45. [Google Scholar]
- Paillé, P. L’analyse par Théorisation Ancrée. Cah. Rech. Sociol. 1994, 23, 147–181. [Google Scholar]
- Steinhardt, F.; Ullenhag, A.; Jahnsen, R.; Dolva, A.-S. Perceived Facilitators and Barriers for Participation in Leisure Activities in Children with Disabilities: Perspectives of Children, Parents and Professionals. Scand. J. Occup. Ther. 2019, 28, 121–135. [Google Scholar] [CrossRef]
- Bronikowski, M.; Bronikowska, M. Will They Stay Fit and Healthy? A Three-Year Follow-Up Evaluation of a Physical Activity and Health Intervention in Polish Youth. Scand. J. Public Heal. 2011, 39, 704–713. [Google Scholar] [CrossRef]
- Bergeron, P.; Reyburn, S. L’Impact de L’Environnement Bâti Sur L’activité Physique, L’Alimentation et le Poids; Institute National en Santé Publique, Direction du Développement des Individus et des Communautés: 2010. Available online: https://www.inspq.qc.ca/pdf/publications/1108_ImpactEnvironBati.pdf (accessed on 1 October 2021).
- Dagkas, S.; Stathi, A. Exploring Social and Environmental Factors Affecting Adolescents’ Participation in Physical Activity. Eur. Phys. Educ. Rev. 2007, 13, 369–384. [Google Scholar] [CrossRef]
- De Craemer, M.; De Decker, E.; De Bourdeaudhuij, I.; Deforche, B.; Vereecken, C.; Duvinage, K.; Grammatikaki, E.; Iotova, V.; Fernández-Alvira, J.M.; Zych, K.; et al. Physical Activity and Beverage Consumption in Preschoolers: Focus Groups with Parents and Teachers. BMC Public Health 2013, 13, 278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stenhammar, C.; Wells, M.; Åhman, A.; Wettergren, B.; Edlund, B.; Sarkadi, A. Children are Exposed to Temptation all the Time-Parents Lifestyle-Related Discussions in Focus Groups. Acta Paediatr. 2012, 101, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Carson, V.; Clark, M.; Berry, T.; Holt, N.L.; Latimer-Cheung, A.E. A Qualitative Examination of the Perceptions of Parents on the Canadian Sedentary Behaviour Guidelines for the Early Years. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 65. [Google Scholar] [CrossRef] [Green Version]
- Edwardson, C.L.; Gorely, T. Parental Influences on Different Types and Intensities of Physical Activity in Youth: A Systematic Review. Psychol. Sport Exerc. 2010, 11, 522–535. [Google Scholar] [CrossRef]
- Martin-Biggers, J.; Spaccarotella, K.; Hongu, N.; Alleman, G.; Worobey, J.; Byrd-Bredbenner, C. Translating It into Real Life: A Qualitative Study of the Cognitions, Barriers and Supports for Key Obesogenic Behaviors of Parents of Preschoolers. BMC Public Healh 2015, 15, 189. [Google Scholar] [CrossRef] [Green Version]
- Zahra, J.; Sebire, S.J.; Jago, R. “He’s Probably More Mr. Sport than Me”—A Qualitative Exploration of Mothers’ Perceptions of Fathers’ Role in their Children’s Physical Activity. BMC Pediatr. 2015, 15, 101. [Google Scholar] [CrossRef] [Green Version]
- Sallis, J.F.; Prochaska, J.J.; Taylor, W.C. A Review of Correlates of Physical Activity of Children and Adolescents. Med. Sci. Sports Exerc. 2000, 32, 963–975. [Google Scholar] [CrossRef]
- Hesketh, K.D.; Hinkley, T.; Campbell, K.J. Children′S Physical Activity and Screen Time: Qualitative Comparison of Views of Parents of Infants and Preschool Children. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 152. [Google Scholar] [CrossRef] [Green Version]
- Salvy, S.-J.; de la Haye, K.; Bowker, J.C.; Hermans, R.C. Influence of Peers and Friends on Children’s and Adolescents’ Eating and Activity Behaviors. Physiol. Behav. 2012, 106, 369–378. [Google Scholar] [CrossRef] [Green Version]
- Duncan, S.C.; Duncan, T.E.; Strycker, L.A. Sources and Types of Social Support in Youth Physical Activity. Health Psychol. 2005, 24, 3–10. [Google Scholar] [CrossRef]
- Abi Nader, P.; Hilberg, E.; Schuna, J.M.; John, D.H.; Gunter, K.B. Teacher-Level Factors, Classroom Physical Activity Opportunities, and Children’s Physical Activity Levels. J. Phys. Act. Health 2018, 15, 637–643. [Google Scholar] [CrossRef]
- Perlman, D. The Influence of the Social Context on Students In-Class Physical Activity. J. Teach. Phys. Educ. 2013, 32, 46–60. [Google Scholar] [CrossRef] [Green Version]
- Xu, F.; Chepyator-Thomson, J.; Liu, W.; Schmidlein, R. Association Between Social and Environmental Factors and Physical Activity Opportunities in Middle Schools. Eur. Phys. Educ. Rev. 2010, 16, 183–194. [Google Scholar] [CrossRef]
- Gadais, T.; Boulanger, M.; Trudeau, F.; Rivard, M.-C. Environments Favorable to Healthy Lifestyles: A Systematic Review of Initiatives in Canada. J. Sport Health Sci. 2017, 7, 7–18. [Google Scholar] [CrossRef]
- Cervero, R.; Kockelman, K. Travel Demand and the 3Ds: Density, Diversity, and Design. Transportation Research Part D: Transport and Environment. Transp. Res. Part D Transp. Environ. 1997, 2, 199–219. [Google Scholar] [CrossRef]
- Heath, G.W.; Brownson, R.C.; Kruger, J.; Miles, R.; Powell, K.E.; Ramsey, L.T. The Effectiveness of Urban Design and Land Use and Transport Policies and Practices to Increase Physical Activity: A Systematic Review. J. Phys. Act. Healh 2006, 3, S55–S76. [Google Scholar] [CrossRef]
- Loh, V.H.Y.; Veitch, J.; Salmon, J.; Cerin, E.; Thornton, L.; Mavoa, S.; Villanueva, K.; Timperio, A. Built Environment and Physical Activity Among Adolescents: The Moderating Effects of Neighborhood Safety and Social Support. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 132. [Google Scholar] [CrossRef] [Green Version]
- D’Angelo, H.; Fowler, S.L.; Nebeling, L.C.; Oh, A.Y. Adolescent Physical Activity: Moderation of Individual Factors by Neighborhood Environment. Am. J. Prev. Med. 2017, 52, 888–894. [Google Scholar] [CrossRef]
- Leriche, J.; Walczak, F. Les Obstacles a la Pratique Sportive des Cégépiens; Rapport de recherche PAREA, Bibliothèque et Archives Nationales du Québec. 2014. Available online: https://eduq.info/xmlui/bitstream/handle/11515/34118/033137-leriche-walczak-obstacles-pratique-sportive-cegepiens-sherbrooke-trois-rivieres-PAREA-2014.pdf?sequence=1 (accessed on 1 October 2021).
- Truelove, S.; Bruijns, B.A.; Vanderloo, L.M.; O’Brien, K.T.; Johnson, A.M.; Tucker, P. Physical Activity and Sedentary Time During Childcare Outdoor Play Sessions: A Systematic Review and Meta-Analysis. Prev. Med. 2018, 108, 74–85. [Google Scholar] [CrossRef]
- Donnelly, A.A.; MacIntyre, T.E. Physical Activity in Natural Settings: Green and Blue Exercise; Routledge: London, UK, 2019. [Google Scholar]
- Brunet, J.; Sabiston, C.M.; Chaiton, M.; Barnett, T.A.; O’Loughlin, E.; Low, N.C.; O’Loughlin, J.L. The Association Between Past and Current Physical Activity and Depressive Symptoms in Young Adults: A 10-Year Prospective Study. Ann. Epidemiol. 2013, 23, 25–30. [Google Scholar] [CrossRef]
- McNeill, L.H.; Kreuter, M.W.; Subramanian, S. Social Environment and Physical activity: A review of Concepts and Evidence. Soc. Sci. Med. 2006, 63, 1011–1022. [Google Scholar] [CrossRef]
- McPhie, M.L.; Rawana, J.S. Unravelling the Relation Between Physical Activity, Self-Esteem and Depressive Symptoms among Early and Late Adolescents: A Mediation Analysis. Ment. Heal. Phys. Act. 2012, 5, 43–49. [Google Scholar] [CrossRef]
- Aan het Rot, M.; Collins, K.A.; Fitterling, H.L. Physical Exercise and Depression. Mt. Sinai J. Med. 2009, 76, 204–214. [Google Scholar] [CrossRef]
- Poirel, E.B. Psychologiques de L’activité Physique Pour la Santé Mentale Optimale. St. Ment. Au Québec 2017, 42, 147–164. [Google Scholar] [CrossRef] [Green Version]
- Wankel, L.M. The Importance of Enjoyment to Adherence and Psychological Benefits from Physical Activity. Int. J. Sport Psychol. 1993, 24, 151–169. [Google Scholar]
- Schreiber, D.S. Guérir-Le Stress, L’anxiété et la Dépression sans Médica-Ments Ni Psychanalyse; Robert Laffont: Paris, France, 2003. [Google Scholar]
- Wipfli, B.; Landers, D.; Nagoshi, C.; Ringenbach, S. An Examination of Serotonin and Psychological Variables in the Relationship between Exercise and Mental Health. Scand. J. Med. Sci. Sports 2009, 21, 474–481. [Google Scholar] [CrossRef]
- Brown, P.; Roediger, H.; McDaniel, M.; Stick, M.I. The Science of Successful Learning; Belknap Press of Harvard University Press: Cambridge, MA, USA, 2014. [Google Scholar]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Couture-Wilhelmy, L.; Chaubet, P.; Gadais, T. Winning Conditions for the Adoption and Maintenance of Long-Term Healthy Lifestyles According to Physical Activity Students. Int. J. Environ. Res. Public Health 2021, 18, 11057. https://doi.org/10.3390/ijerph182111057
Couture-Wilhelmy L, Chaubet P, Gadais T. Winning Conditions for the Adoption and Maintenance of Long-Term Healthy Lifestyles According to Physical Activity Students. International Journal of Environmental Research and Public Health. 2021; 18(21):11057. https://doi.org/10.3390/ijerph182111057
Chicago/Turabian StyleCouture-Wilhelmy, Laurence, Philippe Chaubet, and Tegwen Gadais. 2021. "Winning Conditions for the Adoption and Maintenance of Long-Term Healthy Lifestyles According to Physical Activity Students" International Journal of Environmental Research and Public Health 18, no. 21: 11057. https://doi.org/10.3390/ijerph182111057