
Occupational Risks in Hospitals, Quality of Life, and Quality of Work Life: A Systematic Review

 , , , , ,
, , , , ,  ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search in Database
2.2. Selection of Studies, Extraction, and Data Analysis
2.3. Assessment of Methodological Quality and Risk of Bias
3. Results
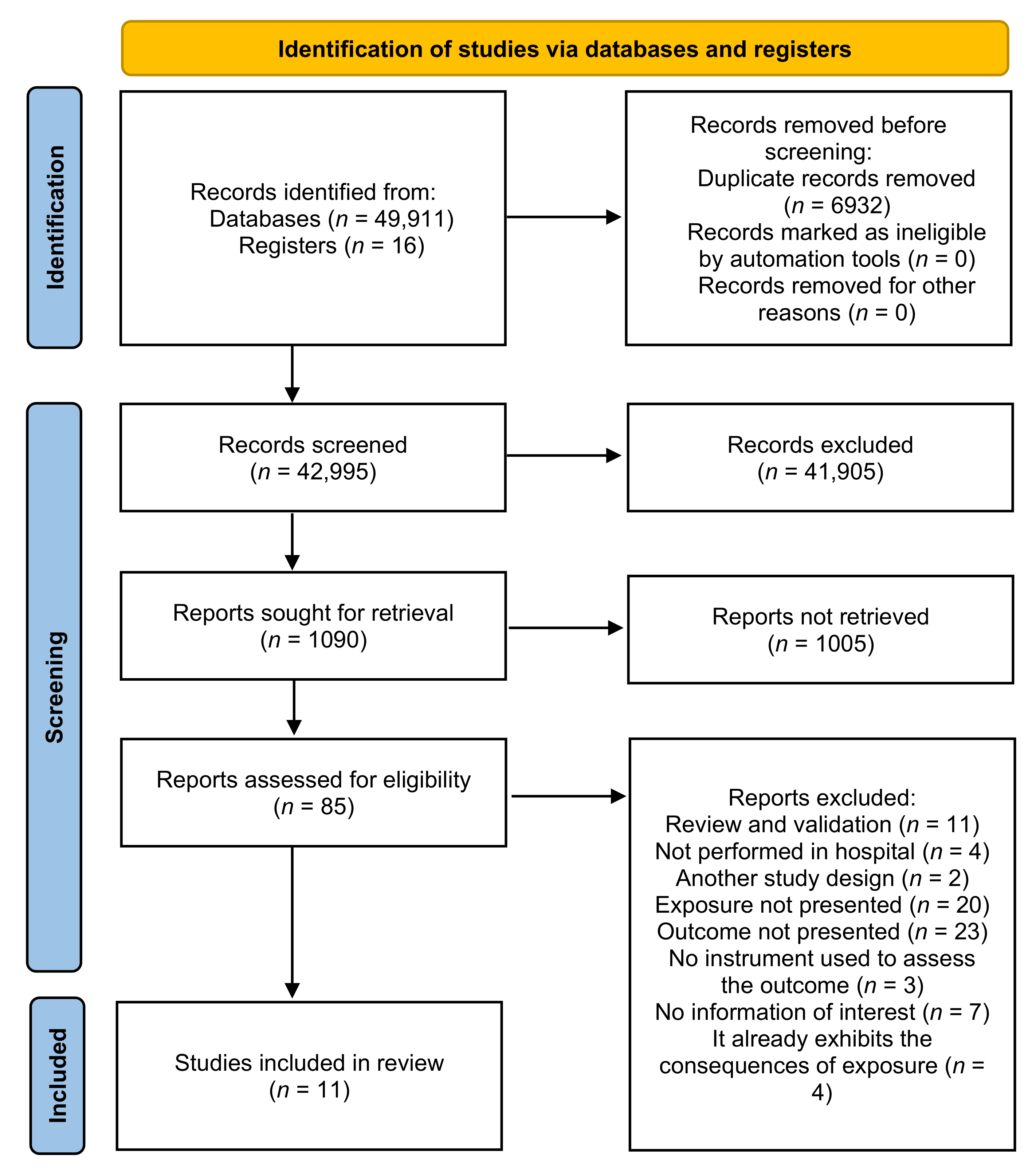
3.1. Selection and Characterization of the Studies
3.2. Description of the Results of Studies That Evaluated Occupational Risks with the Quality of Life (QL) of Workers
3.3. Description of the Results of Studies That Evaluated Occupational Risks with the Quality of Life at Work (QWL)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Study | Methodological Quality | Bias’ Risk | ||||||
|---|---|---|---|---|---|---|---|---|
| Selection | Comparability | Result | Total | Yes | No | Unclear | Result | |
| Almogbel, 2021 [30] | * * * * * | * * | * * | 9 | 7 | 1 | 3 | High risk |
| Azevedo, Nery and Cardoso, 2017 [33] | * * * * * | * * | * * | 9 | 5 | 2 | 4 | High risk |
| Foster et al., 2020 [34] | * * * * * | * | * * | 8 | 6 | 2 | 3 | High risk |
| Ghasemi et al., 2021 [31] | * * * * * | * | * * | 8 | 7 | 1 | 3 | High risk |
| Kalanlar, Akçay and Karabay, 2021 [32] | * * * * * | - | * * | 7 | 3 | 1 | 7 | High risk |
| Kim and Kim, 2017 [27] | * * * * * | * | * * | 8 | 4 | 3 | 4 | High risk |
| Lambert et al., 2004 [23] | * * * * * | * | * * | 8 | 6 | 3 | 2 | Moderate risk |
| Makabe et al., 2018 [29] | * * * * * | * | * | 7 | 7 | 2 | 2 | Moderate risk |
| Nowrouzi et al., 2015 [26,28] | * * * * * | * | * * * | 9 | 7 | 2 | 2 | Moderate risk |
| Silva, Luz and Gil, 2013 [35] | * * * * * | * | * * | 8 | 4 | 4 | 3 | High risk |
| Wu et al., 2010 [24] | * * * * * | * | * * | 8 | 6 | 2 | 3 | Moderate risk |
References
- Fontoura, F.P. Hospital laundry working and environment conditions: Workers’ perception. Rev. Bras. Saúde Ocup. 2016, 6369, 1–11. [Google Scholar]
- Assunção, A.Á. Condições de Trabalho e saúde dos Trabalhadores da saúde. Notes 2011, 8, 453–478. [Google Scholar]
- Antunes, R.; Praun, L. The society of illness at work. Serviço Soc. Soc. 2015, 123, 407–427. [Google Scholar] [CrossRef]
- Canales, M.; Valenzuela, S.; Paravic, T. Condiciones de trabajo de los profesionales de enfermería en Chile. Enfermería Univ. 2016, 13, 178–185. [Google Scholar] [CrossRef] [Green Version]
- Antunes, R.; Druck, G. A terceirização sem limites: A precarização do trabalho como regra. Soc. Questão 2015, 18, 19–40. [Google Scholar]
- Dos Santos, P.R. Saúde do Trabalhador no Trabalho Hospitalar: Metodologias Integradas de Avaliação de Experiências nos Espaços de Intervenção em Hospitais no Estado do Rio de Janeiro. Ph.D. Thesis, Rio de Janeiro, Brazil, 2010. [Google Scholar]
- Mendes, T.; Areosa, J. Acidentes de trabalho ocorridos em profissionais de saúde numa instituição hospitalar de Lisboa Accidents at work occurred in health care workers in a Lisbon hospital. Rev. Angolana Sociol. 2014, 13, 25–47. [Google Scholar] [CrossRef] [Green Version]
- Bayo, J.A.P.; Laina, M.S. Manual de Salud Laboral; Madri: Olalla, Spain, 1996; pp. 92–98. [Google Scholar]
- Sulzbacher, E.; Fontana, R.T. Concepções da equipe de enfermagem sobre a exposição a riscos físicos e químicos no ambiente hospitalar. Rev. Bras. Enferm. 2013, 66, 25–30. [Google Scholar] [CrossRef]
- Rai, R.; El-Zaemey, S.; Dorji, N.; Rai, B.D.; Fritschi, L. Exposure to Occupational Hazards among Health Care Workers in Low- and Middle-Income Countries: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 2603. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, L.S.; Valente, G.S.C. Riscos químicos hospitalares e gerenciamento dos agravos à saúde do trabalhador de enfermagem. Rev. Pesqui. Cuid. Fundam. Online 2012, 4, 21–24. [Google Scholar] [CrossRef]
- Rezende, M.P.; Robazzi, M.L.D.C.C.; Secco, I.A.d.O.; Suazo, S.V.V. Riscos físicos e sua identificação por auxiliares de enfermagem de Hospital de Ensino do Estado de Minas Gerais, Brasil. Rev. Enferm. UFPE Online 2009, 3, 588. [Google Scholar] [CrossRef] [Green Version]
- De Castro, D.M.B.; Pinto, E.R.; Coutinho, G.A.G.; Bugari, L.F.; De Jesus, M.S.B. Acidente de trabalho entre profissionaisde enfermagem de um hospital público dePorto Velho, Rondônia. Saúde Coletiva 2008, 5, 206–211. [Google Scholar]
- Tabeleão, V.P.; Tomasi, E.; Neves, S.F. Qualidade de vida e esgotamento profissional entre docentes da rede pública de Ensino Médio e Fundamental no Sul do Brasil. Cad. Saúde Pública 2011, 27, 2401–2408. [Google Scholar] [CrossRef]
- WHO-World Healthy Organization. WHO|The World Health Organization Quality of Life (WHOQOL); WHO: Geneva, Switzerland, 1995. [Google Scholar]
- Ferreira, M.C. Qualidade de Vida no Trabalho—Uma Abordagem Centrada no Olhar dos Trabalhadores; LPA Edições: Brasília, Brazil, 2011. [Google Scholar]
- Ferreira, M.C.; Brusiquese, R.G. Novas condições de trabalho e velhos modos de gestão: A qualidade de vida no trabalho em questão. Rev. Bras. Gestão Desenvolv. Reg. 2014, 10, 247–267. [Google Scholar]
- Constanza, I.; Pacheco, V.; Riaño-Casallas, M.I. Contribuciones de la salud y la seguridad en el trabajo a la calidad de la vida laboral: Una reflexión analítica. Cienc. Tecnol. Salud Vis. Ocul. 2017, 15, 85–94. [Google Scholar] [CrossRef] [Green Version]
- Roeder, M.A. Atividade Física, Saúde Mental e Qualidade de Vida; Shape: Rio de Janeiro, Brazil, 2003; p. 365. [Google Scholar]
- Nadler, D.A.; Lawler, E.E. Quality of work life: Perspectives and directions. Organ. Dyn. 1983, 11, 20–30. [Google Scholar] [CrossRef]
- Tachizawa, T.; Ferreira, V.C.P.; Fortuna, A.A.M. Gestão com Pessoas: Uma Abordagem Aplicada às Estratégias de Negócios; Editora FGV: Rio de Janeiro, Brazil, 2001. [Google Scholar]
- Fernandes, D.M.M.; Fernandes, S.B.; do Ferrazza, C.A.C. Gestão para a segurança e a qualidade de vida no trabalho em uma lavanderia hospitalar. Normas Publicação 2013, 22, 141–150. [Google Scholar]
- Aycan, Z.; Kanugo, R.N. Cross-cultural industrial and organizational psychology: A critical appraisal of the field and future directions. In Handbook of Industrial, Work and Organizational Psychology; Sage: London, UK, 2001; pp. 385–408. [Google Scholar]
- Guerreiro, I.; Monteiro, M. Qualidade de Vida no Ambiente Corporativo; Ipes Editorial: Campinas, Brazil, 2008; pp. 139–145. [Google Scholar]
- Freire, M.; Costa, E. Qualidade de vida dos profissionais de enfermagem no ambiente de trabalho. Rev. Enferm. Contemp. 2016, 5, 151–158. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372. [Google Scholar] [CrossRef]
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 2020, 368. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Hospital Research Institute: Otawa, ON, Canada.
- Bernardo, W.M. A revisão sistemática na prática clínica baseada em evidência. Femina 2008, 36, 335–344. [Google Scholar]
- Viswanathan, M.; Berkman, N.D. Development of the RTI item bank on risk of bias and precision of observational studies. J. Clin. Epidemiol. 2012, 65, 163–178. [Google Scholar] [CrossRef]
- Sedlar, N.; Lainscak, M.; Mårtensson, J.; Strömberg, A.; Jaarsma, T.; Farkas, J. Factors related to self-care behaviours in heart failure: A systematic review of European Heart Failure Self-Care Behaviour Scale studies. Eur. J. Cardiovasc. Nurs. 2017, 16, 272–282. [Google Scholar] [CrossRef] [Green Version]
- Lambert, V.; Lambert, C.; Itano, J.; Inouye, J.; Kim, S.; Kuniviktikul, W.; Sitthimongkol, Y.; Pongthavornkamol, K.; Gasemgitvattana, S.; Ito, M. Cross-cultural comparison of workplace stressors, ways of coping and demographic characteristics as predictors of physical and mental health among hospital nurses in Japan, Thailand, South Korea and the USA (Hawaii). Int. J. Nurs. Stud. 2004, 41, 671–684. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Zhu, W.; Li, H.; Tak-Sun Yu, I.; Lin, S.; Wang, X.; Yang, S. Quality of life and its influencing factors among medical professionals in China. Int. Arch. Occup. Environ. Health 2010, 83, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, M.C.; da Luz, V.B.; Gil, D. Ruído em hospital universitário: Impacto na qualidade de vida TT—Noise in the hospital setting: Impact on quality of life. Audiol. Commun. Res. 2013, 18, 109–119. [Google Scholar] [CrossRef] [Green Version]
- Nowrouzi, B.; Lightfoot, N.; Carter, L.; Lariviére, M.; Rukholm, E.; Schinke, R.; Belanger-Gardner, D. The relationship between quality of work life and location of cross-training among obstetric nurses in urban northeastern Ontario, Canada: A population-based cross sectional study. Int. J. Occup. Med. Environ. Health 2015, 28, 571–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.J.; Kim, H.Y. Emotional labor, job stress and professional quality of life among nurses in long-term care hospital. Korean J. Adult Nurs. 2017, 29, 290–301. [Google Scholar] [CrossRef]
- Nowrouzi, B.; Rukholm, E.; Larivière, M.; Carter, L.; Koren, I.; Mian, O.; Giddens, E. Work ability and work-related stress: A cross-sectional study of obstetrical nurses in urban northeastern Ontario. Work 2015, 54, 115–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makabe, S.; Kowitlawakul, Y.; Nurumal, M.S.; Wichaikhum, O.; Wangmo, N.; Yap, S.; Kunaviktikul, W.; Komatsu, J.; Shirakawa, H. Investigation of the key determinants of Asian nurses’ quality of life. Ind. Health 2018, 56, 212–219. [Google Scholar] [CrossRef] [Green Version]
- Almogbel, Y. The Effect of Occupational Stress on the Quality of Life of Pharmacists in Saudi Arabia. Risk Manag. Healthc. Policy 2021, 14, 643. [Google Scholar] [CrossRef]
- Ghasemi, F.; Rahmani, R.; Behmaneshpour, F.; Fazli, B. Quality of work life among surgeons and its association with musculoskeletal complaints. Cogent Psychol. 2021, 8, 1880256. [Google Scholar] [CrossRef]
- Kalanlar, B.; Akçay, D.; Karabay, İ. Assessing the correlation between the quality of working life and perceived stress in a rehabilitation hospital. Work. Older People 2020, 25, 1–10. [Google Scholar] [CrossRef]
- Azevedo, B.D.S.; Nery, A.A.; Cardoso, J.P. Estresse Ocupacional e Insatisfação com a Qualidade de Vida no Trabalho da Enfermagem. Texto Contexto Enferm. 2017, 26, 3940015. [Google Scholar] [CrossRef] [Green Version]
- Foster, K.; Roche, M.; Giandinoto, J.A.; Platania-Phung, C.; Furness, T. Mental health matters: A cross-sectional study of mental health nurses’ health-related quality of life and work-related stressors. Int. J. Ment. Health Nurs. 2021, 30, 624–634. [Google Scholar] [CrossRef]
- Ferraz, M. Qualidade de vida: Conceito e um breve histórico. Jovem Médico 1998, 4, 219–222. [Google Scholar]
- Flack, M. Problemas Conceituais em Qualidade de Vida. A Avaliação de Qualidade de Vida: Guia para Profissionais da Saúde; Artmed: Porto Alegre, Brazil, 2008. [Google Scholar]
- Pedroso, B.; Pilatti, L.; Reis, D. Cálculo dos escores e estatística descritiva do WHOQOL-100 utilizando o Microsoft Excel. Revista Brasileira Qualidade Vida 2008, 1, 23–32. [Google Scholar] [CrossRef]
- Alves, E. Qualidade de vida: Considerações sobre os indicadores e instrumentos de medida. Revista Brasileira Qualidade Vida 2011, 3, 16–23. [Google Scholar] [CrossRef] [Green Version]

| Author/Year | Country | Objective | Study’s Design | Instrument to Assess QoL | Instrument to Assess the Occupational Risk | Occupational Risk Assessed | Sample Size (Occupation) | Gender | Occupation Time (Years) |
|---|---|---|---|---|---|---|---|---|---|
| Almogbel, 2021 [39] | Saudi Arabia. | Evaluate the association between pharmacists’ Quality of life (QOL) and occupational stress in Saudi Arabia. | Cross-sectional | World Health Organization Quality of Life–Brief scale (WHOQOL-BREF). | Effort-Reward Imbalance (ERI). | Occupational stress. | 204 (pharmacists). | Male: 61.2%; Female: 38.8%. | Mean 8.1 (SD = 7.2). |
| Foster et al., 2020 [43] | Australia. | Identify the health-related Quality of life of mental health nurses (HR-QoL) and work-related stressors; associations between stressors and HR-QoL; and HR-QoL predictors. | Cross-sectional | Short Form SF-12v2-12-item. | Work-related stressor items were informed by literature and a prior pilot study. Work-related stressors were grouped in three categories comprising 23 different stressors: (1) Consumer/Carer stressors, (2) Collegial included staff behaviors and relationships in the multidisciplinary team and (3) Organizational included the nursing role and organizational resources. | Occupational stress. | 498 (nurses). | Male: (26%); Female: (74%); | <1–4 years (18%); 5–9 years (17%); 10–14 years (15%); >14 (50%). |
| Lambert et al., 2004 [32] | Japan, South Korea, Thailand, and the USA (Hawaii). | Culturally compare factors contributing to nursing shortages in countries that produced a limited number of research findings on stress in nurses. | Cross-sectional | SF-36 Health Survey (SF-36). | Nursing Stress Scale (NSS). | Occupational stress. | 1.554 (nurses). | Female: 93.2% (Japan); 98.7% (South Korea); 94.6% (Thailand); 93.4% (USA). | Average:11.8 (Japan); 8.01 (South Korea); 11.7 (Thailand); 13.4 (USA). |
| Makabe et al., 2018 [38] | Japan, Singapore, Malaysia, Thailand, and Bhutan. | Compare nurses’ Quality of life and investigate the main determinants among Asian countries with different economic statuses. | Cross-sectional | World Health Organization Quality of Life (WHOQOL-Bref). | NIOSH Questionnaire. | Occupational stress. | 1201 (nurses in Japan); 1040 (nurses in Singapore); 1001 (nurses in Malaysia); 418 (nurses in Thailand); 169 (nurses in Bhutan). | Female: 93% Japan; 93% Singapore; 94% Malaysia; 97% Thailand; 70% Bhutan. | Average: 15 (Japan); 08 (Singapore); 05 (Malaysia); 17 (Thailand); 08 (Bhutan). |
| Silva, Luz and Gil, 2013 [34] | Brazil. | Assess noise levels in different hospital environments and investigate the impact of this exposure on the Quality of life of professionals working in these environments. | Cross-sectional | World Health Organization Quality of Life (WHOQOL-Bref). | On-the-spot measurement of sound pressure levels, the minimum value is the weakest intensity, and the maximum as the strongest sound pressure intensity in each sector. | Occupational noise. | Seven sectors of the hospital and 35 workers (five from each sector). | Features only of sectors. | Features only of sectors |
| Wu et al., 2010 [33] | China. | Assess doctors’ quality of life and explore their main influencing factors, especially demographic characteristics, behavioral, occupational factors, and coping resources. | Cross-sectional | SF-36 Health Survey (SF-36) Chinese version. | Occupation Stress Inventory-Revised Edition (OSI-R) Chinese version. | Occupational stress. | 2721 (Physicians). | Male: 37.6%; Female: 62.4%. | No information. |
| Author/Year | Country | Objective | Study’s Design | Instrument to Assess QWL | Instrument to Assess the Occupational Risk | Occupational Risk Assessed | Sample Size (Occupation) | Gender | Occupation Time (Years) |
|---|---|---|---|---|---|---|---|---|---|
| Azevedo, Nery and Cardoso, 2017 [42] | Brazil. | Analyze the association between occupational stress, Quality of work life and associated factors among nursing workers | Cross-sectional | Total Quality of Work Life–TQWL-42. | Job Stress Scale (JSS). | Occupational stress. | 309 (nurses = 38.5%; nursing technician = 53.4%; nursing assistant = 8.1%). | Male: 11%; Female: 89%. | Mean 7.1. |
| Ghasemi et al., 2021 [40] | Iran. | Evaluate QWL among surgeons and investigate its association with musculoskeletal complaints. | Cross-sectional | Walton’s 35-item questionnaire. | Nordic Musculoskeletal Questionnaire (NMQ) and Rapid Entire Body Assessment (REBA). | Musculoskeletal complaints. | 74 (surgeons). | Male: 60.8%; Female: 39.2%. | Mean 7.00 (SD = 4.23). |
| Kalanlar, Akçay and Karabay, 2021 [41] | Turkey. | Examine the relationship between the Quality of working lives and the perceived stress of health personnel working in a hospital specialized. | Cross-sectional | Quality of Work Life Scale (QWLS). | Perceived Stress Scale (PSS). | Occupational stress (perceived Stress). | 80 (nurses, physicians, physiotherapists, psychologists and social workers). | Male: 31.3%; Female: 68.7%. | ≤10 years (23.7%); 11–20 years (43.8%); ≥21 years (32.5%). |
| Kim and Kim, 2017 [36] | South Korea. | Identify the emotional work, work stress, and QWL of hospital nurses; examine the correlation between them and analyze the factors that affect the Quality of professional life. | Cross-sectional. | Korean version of the Professional Quality of Life Scale (satisfaction of compassion/subscale Fatigue version 5). | Clinical tool developed by Ku and Kim (1984). | Occupational stress. | 136 (nurses). | No information. | Mean 10.71 (SD = 8.11). <5 years (30.1%); 5~10 years (21.3%); 11~20 years (30.9%); >20 years (17.6%). |
| Nowrouzi et al., 2015 [35,37] | Canada. | Examine the QWL of nurses working in midwifery wards at four hospitals in northeastern Ontario and explore factors that influence their QWL. | Cross-sectional | Work-Related Quality of Life Scale (WRQoL). | Nursing Stress Scale (NSS). | Occupational stress. | 111 (nurses). | Male: 5.4%; Female 94.6%. | Mean 11.6 (SD = 9.01). <35 years (24.4%); 35–44 years (35.3%); 45–54 years (23.2%); ≥55 years (17.1%). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Lira, C.R.N.; Akutsu, R.d.C.; Costa, P.R.d.F.; Leite, L.d.O.; da Silva, K.B.B.; Botelho, R.B.A.; Raposo, A.; Han, H.; Ariza-Montes, A.; Araya-Castillo, L.; et al. Occupational Risks in Hospitals, Quality of Life, and Quality of Work Life: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 11434. https://doi.org/10.3390/ijerph182111434
de Lira CRN, Akutsu RdC, Costa PRdF, Leite LdO, da Silva KBB, Botelho RBA, Raposo A, Han H, Ariza-Montes A, Araya-Castillo L, et al. Occupational Risks in Hospitals, Quality of Life, and Quality of Work Life: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(21):11434. https://doi.org/10.3390/ijerph182111434
Chicago/Turabian Stylede Lira, Carlos Rodrigo Nascimento, Rita de Cássia Akutsu, Priscila Ribas de Farias Costa, Luana de Oliveira Leite, Karine Brito Beck da Silva, Raquel B. A. Botelho, António Raposo, Heesup Han, Antonio Ariza-Montes, Luis Araya-Castillo, and et al. 2021. "Occupational Risks in Hospitals, Quality of Life, and Quality of Work Life: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 21: 11434. https://doi.org/10.3390/ijerph182111434
APA Stylede Lira, C. R. N., Akutsu, R. d. C., Costa, P. R. d. F., Leite, L. d. O., da Silva, K. B. B., Botelho, R. B. A., Raposo, A., Han, H., Ariza-Montes, A., Araya-Castillo, L., & Zandonadi, R. P. (2021). Occupational Risks in Hospitals, Quality of Life, and Quality of Work Life: A Systematic Review. International Journal of Environmental Research and Public Health, 18(21), 11434. https://doi.org/10.3390/ijerph182111434