
Transmission Dynamics of Schistosoma haematobium among School-Aged Children: A Cohort Study on Prevalence, Reinfection and Incidence after Mass Drug Administration in the White Nile State of Sudan

 and
and
Abstract
:1. Introduction
2. Materials and Methods
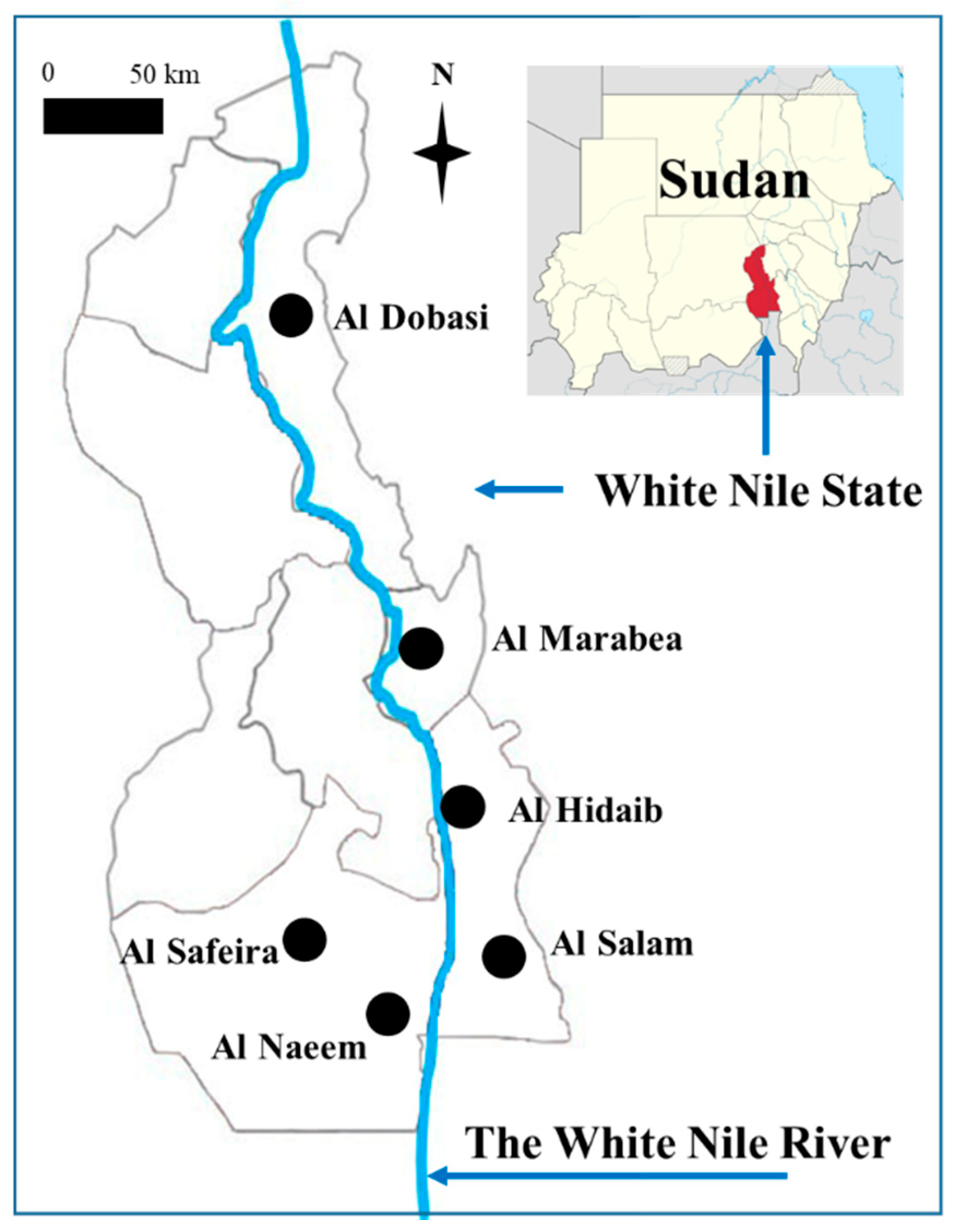
2.1. Study Area
2.2. Ethical Considerations
2.3. Sample Size Calculation
2.4. Urine Sample Collection and Examination
2.5. MDA with Praziquantel
2.6. Study Participants and Flow Diagram of the Cohort Study
2.7. Data Management and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gryseels, B. Schistosomiasis. Infect. Dis. Clin. N. Am. 2012, 26, 383–397. [Google Scholar] [CrossRef] [PubMed]
- Bustinduy, A.L.; Parraga, I.M.; Thomas, C.L.; Mungai, P.L.; Mutuku, F.; Muchiri, E.M.; Kitron, U.; King, C.H. Impact of polyparasitic infections on anemia and undernutrition among Kenyan children living in a Schistosoma haematobium-endemic area. Am. J. Trop. Med. Hyg. 2013, 88, 433–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, C.H.; Dangerfield-Cha, M. The unacknowledged impact of chronic schistosomiasis. Chronic Illn. 2008, 4, 65–79. [Google Scholar] [CrossRef]
- Ezeamama, A.E.; Bustinduy, A.L.; Nkwata, A.K.; Martinez, L.; Pabalan, N.; Boivin, M.J.; King, C.H. Cognitive deficits and educational loss in children with schistosome infection—A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2018, 12, e0005524. [Google Scholar] [CrossRef] [Green Version]
- Friedman, J.F.; Kanzaria, H.K.; Acosta, L.U.Z.P.; Langdon, G.C. Relationship between Schistosoma japonicum and nutritional status among children and young adults in Leyte, the Phillipines. Am. J. Trop. Med. Hyg. 2005, 72, 527–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Preventive Chemotherapy in Human Helminthiasis; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- World Health Organization. Schistosomiasis and soil transmitted helminthiases: Numbers of people treated in 2017. Wkly. Epidemiol. Rec. 2018, 93, 681–692. [Google Scholar]
- Wiegand, R.E.; Mwinzi, P.N.M.; Montgomery, S.P.; Chan, Y.L.; Andiego, K.; Omedo, M.; Muchiri, G.; Ogutu, M.O.; Rawago, F.; Odiere, M.R.; et al. A persistent hotspot of Schistosoma mansoni infection in a five-year randomized trial of praziquantel preventative chemotherapy strategies. J. Infect. Dis. 2017, 216, 1425–1433. [Google Scholar] [CrossRef] [Green Version]
- Lewis, F.A.; Tucker, M.S. Schistosomiasis. Adv. Exp. Med. Biol. 2014, 766, 47–75. [Google Scholar] [PubMed]
- Hotez, P.J.; Kamath, A. Neglected tropical diseases in sub-saharan Africa: Review of their prevalence, distribution, and disease burden. PLoS Negl. Trop. Dis. 2009, 3, e412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Schistosomiasis: Key Facts. World Health Organization, 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/schistosomiasis (accessed on 15 October 2021).
- World Health Organization. Prevention and Control of Schistosomiasis and Soil-Transmitted Helminthiaisis; WHO Tech Report Series, No.912; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Kabuyaya, M.; Chimbari, M.J.; Mukaratirwa, S. Efficacy of praziquantel treatment regimens in pre-school and school aged children infected with schistosomiasis in sub-Saharan Africa: A systematic review. Infect. Dis. Poverty 2018, 7, 73. [Google Scholar] [CrossRef] [Green Version]
- Zwang, J.; Olliaro, P. Efficacy and safety of praziquantel 40 mg/kg in preschool-aged and school-aged children: A meta-analysis. Parasit Vectors 2017, 10, 47. [Google Scholar] [CrossRef] [Green Version]
- Savioli, L.; Gabrielli, A.F.; Montresor, A.; Chitsulo, L.; Engels, D. Schistosomiasis control in Africa: 8 years after World Health Assembly Resolution 54.19. Parasitology 2009, 136, 1677–1681. [Google Scholar] [CrossRef] [Green Version]
- Cha, S.; Elhag, M.S.; Lee, Y.; Cho, D.; Ismail, H.A.H.A.; Hong, S. Epidemiological findings and policy implications from the nationwide schistosomiasis and intestinal helminthiasis survey in Sudan. Parasit Vectors 2019, 12, 429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cha, S.; Hong, S.T.; Lee, Y.H.; Lee, K.H.; Cho, D.S.; Lee, J.; Chai, J.Y.; Elhag, M.S.; Khaled, S.G.A.; Elnimeiri, M.K.M.; et al. Nationwide cross-sectional survey of schistosomiasis and soil-transmitted helminthiasis in Sudan: Study protocol. BMC Public Health 2017, 17, 703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Federal Ministry of Health. A Neglected Tropical Diseases Strategy; Federal Ministry of Health: Khartum, Sudan, 2021.
- Lee, Y.H.; Yeong, H.G.; Kong, W.H.; Lee, S.H.; Cho, H.I.; Nam, H.S.; Ismail, H.A.; Alla, G.N.; Oh, C.H.; Hong, S.T. Reduction of urogenital schistosomiasis with an integrated control project in Sudan. PLoS Negl. Trop. Dis. 2015, 9, e3423. [Google Scholar] [CrossRef] [Green Version]
- Cha, S.; Hong, S.T.; Lee, J.S.; Jeong, H.G.; Kwon, I.S.; Saed, A.A.W.; Elhag, M.S.; Ismail, H.A.H.A.; Amin, M.; Lee, Y.H. Comparison of the Change in the Prevalence and Intensity of Schistosoma haematobium Infection Between High and Low Prevalence Areas of White Nile State, Sudan. Korean J. Parasitol. 2020, 58, 421–430. [Google Scholar] [CrossRef]
- Tchuem Tchuenté, L.A.; Rollinson, D.; Stothard, J.R.; Molyneux, D. Moving from control to elimination of schistosomiasis in sub-Saharan Africa: Time to change and adapt strategies. Infect. Dis. Poverty 2017, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. A Global Strategy on Water, Sanitation and Hygiene to Combat Neglected Tropical Diseases 2021–2030; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. Ending the Neglect to Attain the Sustainable Development Goals A Road Map for Neglected Tropical Diseases 2021–2030; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Bizimana, P.; Ortu, G.; Van Geertruyden, J.P.; Nsabiyumva, F.; Nkeshimana, A.; Muhimpundu, E.; Polman, K. Integration of schistosomiasis control activities within the primary health care system: A critical review. Parasit Vectors 2019, 12, 393. [Google Scholar] [CrossRef] [Green Version]
- Casulli, A. New global targets for NTDs in the WHO roadmap 2021–2030. PLoS Negl. Trop. Dis. 2021, 15, e0009373. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.T.; Gu, Q.Y.; Limpanont, Y.; Song, L.G.; Wu, Z.D.; Okanurak, K.; Lv, Z.Y. Snail-borne parasitic diseases: An update on global epidemiological distribution, transmission interruption and control methods. Infect. Dis. Poverty 2018, 7, 28. [Google Scholar] [CrossRef] [Green Version]
- Molyneux, D.H.; Savioli, L.; Engels, D. Neglected tropical diseases: Progress towards addressing the chronic pandemic. Lancet 2017, 389, 312–325. [Google Scholar] [CrossRef]
- Zacharia, A.; Mushi, V.; Makene, T. A systematic review and meta-analysis on the rate of human schistosomiasis reinfection. PLoS ONE 2020, 15, e0243224. [Google Scholar] [CrossRef] [PubMed]
- Steinmann, P.; Keiser, J.; Bos, R.; Tanner, M.; Utzinger, J. Schistosomiasis and water resources development: Systematic review, meta-analysis, and estimates of people at risk. Lancet Infect. Dis. 2006, 6, 411–425. [Google Scholar] [CrossRef]
- El Gaddal, A.A. The Blue Nile Health Project: A comprehensive approach to the prevention and control of water associated diseases in irrigated schemes of the Sudan. J. Trop. Med. Hyg. 1985, 88, 47–56. [Google Scholar]
- Ismail, H.; Ahmed, R.M.; Lee, Y.-H.; Elhag, M.S.; Kim, Y.; Seungman, C.; Jin, C. Population Dynamics of Intermediate-Host Snails in the White Nile River, Sudan: A Year-Round Observational Descriptive Study. Korean J. Parasitol 2021, 59, 121–129. [Google Scholar] [CrossRef]
- World Health Organization. Sedimentation method. In Basic Laboratory Methods in Medical Parasitology; World Health Organization: Geneva, Switzerland, 1991. [Google Scholar]
- Landouré, A.; Dembélé, R.; Goita, S.; Kané, M.; Tuinsma, M.; Sacko, M.; Toubali, E.; French, M.D.; Keita, A.D.; Fenwick, A.; et al. Significantly Reduced Intensity of Infection but Persistent Prevalence of Schistosomiasis in a Highly Endemic Region in Mali after Repeated Treatment. PLoS Negl. Trop. Dis. 2012, 6, e1774. [Google Scholar] [CrossRef] [Green Version]
- Mduluza, T.; Ndhlovu, P.D.; Madziwa, T.M.; Midzi, N.; Zinyama, R.; Turner, C.M.; Chandiwana, S.K.; Nyazema, N.; Hagan, P. The impact of repeated treatment with praziquantel of schistosomiasis in children under six years of age living in an endemic area for Schistosoma haematobium infection. Mem. Inst. Oswaldo Cruz 2001, 96 (Suppl.), 157–164. [Google Scholar] [CrossRef] [Green Version]
- Mutsaka-Makuvaza, M.J.; Matsena-Zingoni, Z.; Tshuma, C.; Ray, S.; Zhou, X.-N.; Webster, B.; Midzi, N. Reinfection of urogenital schistosomiasis in pre-school children in a highly endemic district in Northern Zimbabwe: A 12 months compliance study. Infect. Dis. Poverty 2018, 7, 102. [Google Scholar] [CrossRef] [Green Version]
- Kabuyaya, M.; Chimbari, M.J.; Manyangadze, T.; Mukaratirwa, S. Efficacy of praziquantel on Schistosoma haematobium and re-infection rates among school-going children in the Ndumo area of uMkhanyakude district, KwaZulu-Natal, South Africa. Infect. Dis. Poverty 2017, 6, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houmsou, R.S.; Wama, B.E.; Agere, H.; Uniga, J.A.; Amuta, E.U.; Kela, S.L. High Efficacy of Praziquantel in Schistosoma haematobium-Infected Children in Taraba State, Northeast Nigeria: A follow-up study. Sultan Qaboos Univ. Med. J. 2018, 18, e304–e310. [Google Scholar] [CrossRef] [PubMed]
- Mutapi, F.; Ndhlovu, P.D.; Hagan, P.; Woolhouse, M.E.J. A comparison of re-infection rates with Schistosoma haematobium following chemotherapy in areas with high and low levels of infection. Parasite Immunol. 1999, 21, 253–259. [Google Scholar] [CrossRef]
- Bashir, M.; Bickle, Q.; Bushara, H.; Cook, L.; Shi, F.; He, D.; Huggins, M.; Lin, J.; Malik, K.; Moloney, A. Evaluation of defined antigen vaccines against Schistosoma bovis and S. japonicum in bovines. Trop. Geogr. Med. 1994, 46, 255–258. [Google Scholar]
- Yole, D.S.; Pemberton, R.; Reid, G.D.; Wilson, A.R. Protective immunity to Schistosoma mansoni induced in the olive baboon Papio anubis by the irradiated cercaria vaccine. Parasitology 1996, 112, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Mbanefo, E.C.; Huy, N.T.; Wadagni, A.A.; Eneanya, C.I.; Nwaorgu, O.; Hirayama, K. Host determinants of reinfection with schistosomes in humans: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2014, 8, e3164. [Google Scholar] [CrossRef] [Green Version]
- Olliaro, P.L.; Coulibaly, J.T.; Garba, A.; Halleux, C.; Keiser, J.; King, C.H.; N’Goran, E.K.; Raso, G.; Scherrer, A.U.; Figueiredo-Sousa, J.C.; et al. Efficacy and safety of single-dose 40 mg/kg oral praziquantel in the treatment of schistosomiasis in preschool-age versus school-age children: An individual participant data meta-analysis. PLoS Negl. Trop. Dis. 2020, 14, e0008277. [Google Scholar] [CrossRef] [PubMed]
- Farrell, S.H.; Truscott, J.E.; Anderson, R.M. The importance of patient compliance in repeated rounds of mass drug administration (MDA) for the elimination of intestinal helminth transmission. Parasit Vectors 2017, 10, 291. [Google Scholar] [CrossRef] [PubMed]
- Chai, J.Y. Praziquantel treatment in trematode and cestode infections: An update. Infect Chemother. 2013, 45, 32–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| School Name | Sample Size at Baseline | Mean Age (SD) in Years | Percentage of Boys (%) | Follow-up Rate (%) | |
|---|---|---|---|---|---|
| 2 Weeks | 6 Months | ||||
| Al Dobasi | 383 | 8.7 (2.0) | 100 | 90.1 | 73.9 |
| Al Hidaib | 285 | 8.8 (1.8) | 42 | 71.6 | 74.7 |
| Al Salam | 434 | 8.6 (2.0) | 45 | 75.3 | 49.5 |
| Al Naeem | 330 | 8.8 (2.0) | 100 | 91.2 | 75.2 |
| Al Sefeira | 519 | 8.4 (1.8) | 55 | 91.1 | 69.9 |
| Total | 1951 | 8.6 (1.9) | 67 | 84.6 | 67.8 |
| Baseline Survey | 2-Week Follow-Up Survey | 6-Month Follow-Up Survey | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. 1 | (+) | % | No. | (+) | % | Relative Risk | 95% CI | p-Value | No. | (+) | % | Relative Risk | 95% CI | p-Value | ||
| School | ||||||||||||||||
| Al Dobasi | 383 | 25 | 6.5 | 345 | 7 | 2 | 0.29 | 0.14–0.61 | 0.001 | 283 | 19 | 6.7 | 1.04 | 0.49–1.81 | 0.90 | |
| Al Hidaib | 285 | 117 | 41.1 | 204 | 24 | 11.8 | 0.24 | 0.17–0.36 | <0.001 | 213 | 22 | 10.3 | 0.26 | 0.18–0.38 | <0.001 | |
| Al Salam | 434 | 69 | 15.9 | 388 | 61 | 15.7 | 0.97 | 0.71–1.33 | 0.87 | 215 | 6 | 2.8 | 0.17 | 0.08–0.40 | <0.001 | |
| Al Naeem | 330 | 41 | 12.4 | 223 | 4 | 1.8 | 0.16 | 0.07–0.38 | <0.001 | 248 | 2 | 0.8 | 0.06 | 0.01–0.27 | <0.001 | |
| Al Sefeira | 519 | 17 | 3.3 | 490 | 13 | 2.7 | 0.81 | 0.41–1.63 | 0.56 | 362 | 6 | 1.7 | 0.52 | 0.22–1.23 | 0.13 | |
| Sex | ||||||||||||||||
| Boys | 1308 | 188 | 14.4 | 1079 | 62 | 5.7 | 0.48 | 0.29–0.79 | 0.004 | 897 | 43 | 4.88 | 0.44 | 0.26–0.77 | 0.004 | |
| Girls | 643 | 81 | 12.6 | 571 | 47 | 8.2 | 0.67 | 0.28–1.62 | 0.38 | 425 | 12 | 2.8 | 0.22 | 0.12–0.43 | <0.001 | |
| Total | 1951 | 269 | 13.8 | 1650 | 109 | 6.6 | 0.5 | 0.26–0.97 | 0.04 | 1322 | 55 | 4.2 | 0.33 | 0.18–0.58 | <0.001 | |
| Variables | Baseline Survey | 2-Week Follow-Up Survey | 6-Month Follow-Up Survey | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Positive No. 1 | GMI 2 | Positive No. | GMI 2 | Mean 3 Difference | 95% CI | p-Value | Positive No. | GMI 2 | Mean 3 Difference | 95% CI | p-Value | ||
| School | Al Dobasi | 25 | 7.2 | 7 | 4.7 | −1.2 | −11.5, 9.1 | 0.82 | 19 | 4.8 | −4.4 | −9.9,1.2 | 0.12 |
| Al Hidaib | 117 | 18.4 | 24 | 7.2 | −20.2 | −41.3, 1.0 | 0.06 | 22 | 6.8 | −26.1 | −47.7, −4.5 | 0.02 | |
| Al Salam | 69 | 9.6 | 61 | 4.3 | −7.1 | −14.6, 0.4 | 0.06 | 6 | 6.3 | −5.8 | −26.2, 14.5 | 0.57 | |
| Al Naeem | 41 | 19.8 | 4 | 6.4 | −15.1 | −70.2, 40.0 | 0.59 | 2 | 15.2 | −2.8 | −79.3, 73.7 | 0.94 | |
| Al Sefeira | 17 | 8.4 | 13 | 2.2 | −13 | −26.6, 0.6 | 0.06 | 6 | 6.4 | −7.9 | −27.9, 12.2 | 0.44 | |
| Sex | Boys | 188 | 13.8 | 62 | 4.9 | −12.5 | −25.4, 0.5 | 0.06 | 43 | 6.2 | −18.5 | −33.8, −3.2 | 0.02 |
| Girls | 81 | 13.5 | 47 | 4 | −12.9 | −21.8, −4.1 | 0.004 | 12 | 5.8 | −12.9 | −29.0, 3.3 | 0.12 | |
| Total | 269 | 13.7 | 109 | 4.5 | −12.6 | −21.5, −3.7 | 0.006 | 55 | 6.1 | −16.1 | −28.0, −4.2 | 0.008 | |
| Baseline | At 2 Weeks | At 6 Months | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| School | Positive No. 1 | GMI 2 | Negative No. 3 | F-U 4 | F-U Rate 5 | GMI 2 | Cure Rate | ERR 6 | Negative No. 3 | FU 4 | F-U Rate 5 | GMI 2 | Cure Rate | ERR 6 |
| Al Dobasi | 25 | 7.2 | 20 | 25 | 100.0% | 4.7 | 80.0% | 34.7% | 14 | 16 | 64.0% | 4.8 | 87.5% | 33.3% |
| Al Hidaib | 117 | 18.4 | 69 | 86 | 73.5% | 7.2 | 80.2% | 60.9% | 67 | 81 | 69.2% | 6.8 | 82.7% | 63.0% |
| Al Salam | 69 | 9.6 | 48 | 59 | 85.5% | 4.3 | 81.4% | 55.2% | 33 | 33 | 47.8% | 6.3 | 100.0% | 34.4% |
| Al Naeem | 41 | 19.8 | 20 | 22 | 53.7% | 6.4 | 90.9% | 67.7% | 24 | 24 | 58.5% | 15.2 | 100.0% | 23.2% |
| Al Sefeira | 17 | 8.4 | 14 | 15 | 88.2% | 2.2 | 93.3% | 73.8% | 9 | 10 | 58.8% | 6.4 | 90.0% | 23.8% |
| Sex | ||||||||||||||
| Boys | 188 | 13.8 | 115 | 140 | 74.5% | 4.9 | 82.1% | 64.5% | 94 | 108 | 57.4% | 6.2 | 87.0% | 55.1% |
| Girls | 81 | 13.5 | 56 | 67 | 82.7% | 4 | 83.6% | 70.4% | 53 | 56 | 69.1% | 5.8 | 94.6% | 57.0% |
| Total | 269 | 13.7 | 171 | 207 | 77.0% | 4.5 | 82.6% | 67.2% | 147 | 164 | 61.0% | 6.1 | 89.6% | 55.5% |
| Categories 2 | No. of Children by Sex | No. of Children by School | ||||||
|---|---|---|---|---|---|---|---|---|
| Total | Boys | Girls | Al Dobasi | Al Hidaib | Al Salam | Al Naeem | Al Sefeira | |
| + - ∙ | 102 | 67 | 35 | 13 | 46 | 23 | 11 | 9 |
| + - + | 10 | 9 | 1 | 0 | 9 | 0 | 0 | 1 |
| Reinfection rate (%) | 9.8 | 13.4 | 2.9 | 19.6 | 11.1 | |||
| 95% CI (%) | (0.5–17.4) | (7.1–24.0) | (0.4–18.0) | (10.4–33.7) | (1.5–50.6) | |||
| - ∙ ∙ | 1158 | 789 | 369 | 267 | 132 | 182 | 224 | 353 |
| - ∙ + | 38 | 29 | 9 | 17 | 8 | 6 | 2 | 5 |
| Incidence rate (%) | 3.3 | 3.7 | 2.4 | 6.4 | 6.1 | 3.3 | 0.9 | 1.4 |
| 95% CI (%) | (2.4–4.5) | (2.6–5.2) | (1.3–4.6) | (4.0–10.0) | (3.0–11.7) | (1.5–7.2) | (0.2–3.5) | (0.6–3.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, Y.; Lee, Y.-H.; Cha, S.; Choi, I.-U.; Ismail, H.A.H.A.; Elhag, M.S.; Hong, S.-T. Transmission Dynamics of Schistosoma haematobium among School-Aged Children: A Cohort Study on Prevalence, Reinfection and Incidence after Mass Drug Administration in the White Nile State of Sudan. Int. J. Environ. Res. Public Health 2021, 18, 11537. https://doi.org/10.3390/ijerph182111537
Jin Y, Lee Y-H, Cha S, Choi I-U, Ismail HAHA, Elhag MS, Hong S-T. Transmission Dynamics of Schistosoma haematobium among School-Aged Children: A Cohort Study on Prevalence, Reinfection and Incidence after Mass Drug Administration in the White Nile State of Sudan. International Journal of Environmental Research and Public Health. 2021; 18(21):11537. https://doi.org/10.3390/ijerph182111537
Chicago/Turabian StyleJin, Yan, Young-Ha Lee, Seungman Cha, In-Uk Choi, Hassan Ahmed Hassan Ahmed Ismail, Mousab Siddig Elhag, and Sung-Tae Hong. 2021. "Transmission Dynamics of Schistosoma haematobium among School-Aged Children: A Cohort Study on Prevalence, Reinfection and Incidence after Mass Drug Administration in the White Nile State of Sudan" International Journal of Environmental Research and Public Health 18, no. 21: 11537. https://doi.org/10.3390/ijerph182111537