
A Retrospective Cohort Study of Lung Cancer Incidences and Epidemiological Analysis in Saudi Arabian Population from 2006–2016


Abstract
:1. Introduction
2. Material and Methods
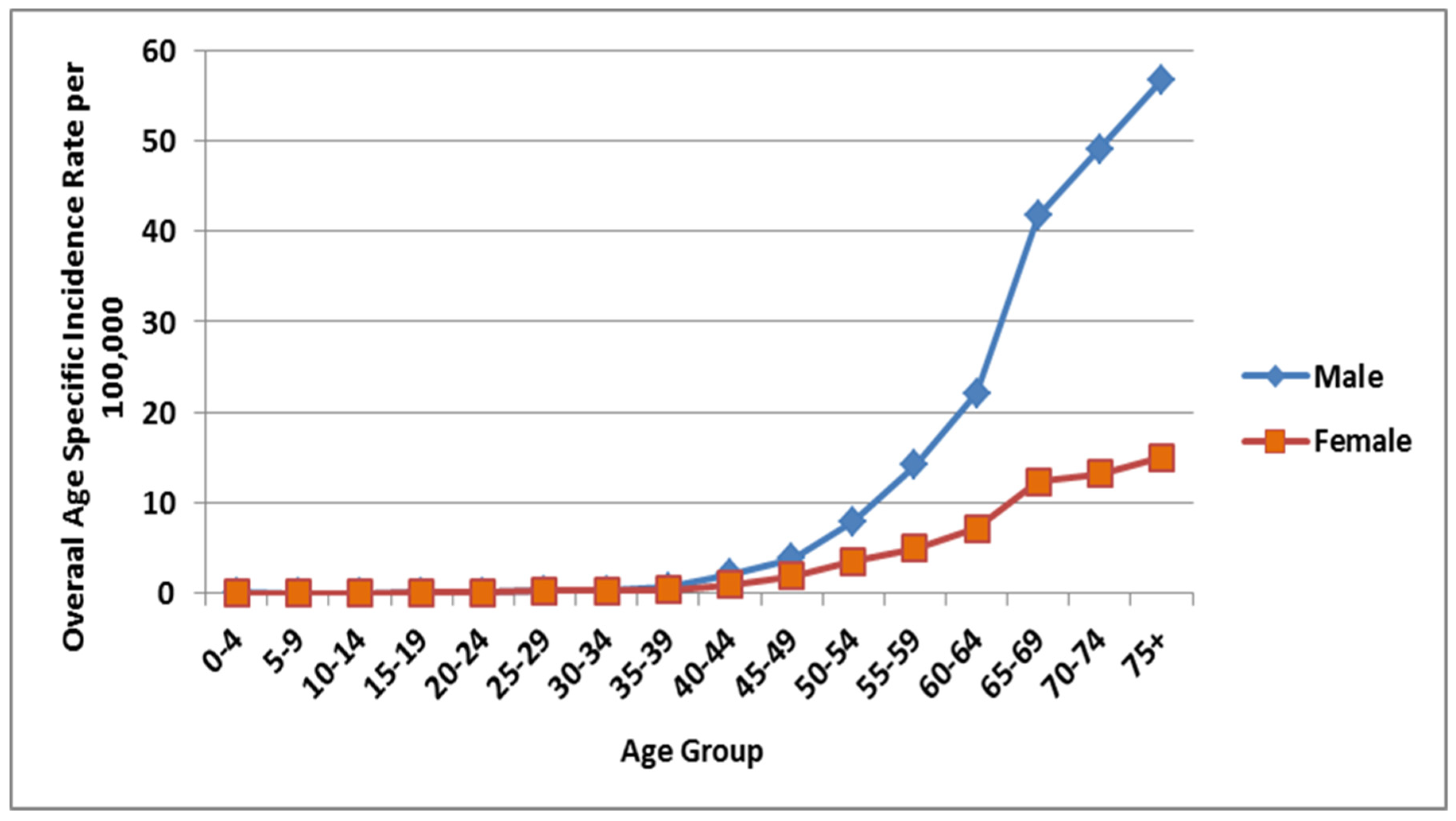
3. Incidences of Lung Cancer among Males
4. Incidences of Lung Cancer among Females
5. Lung Cancer: ASIR and CIR Incidences
6. CIR by Geographical Regions
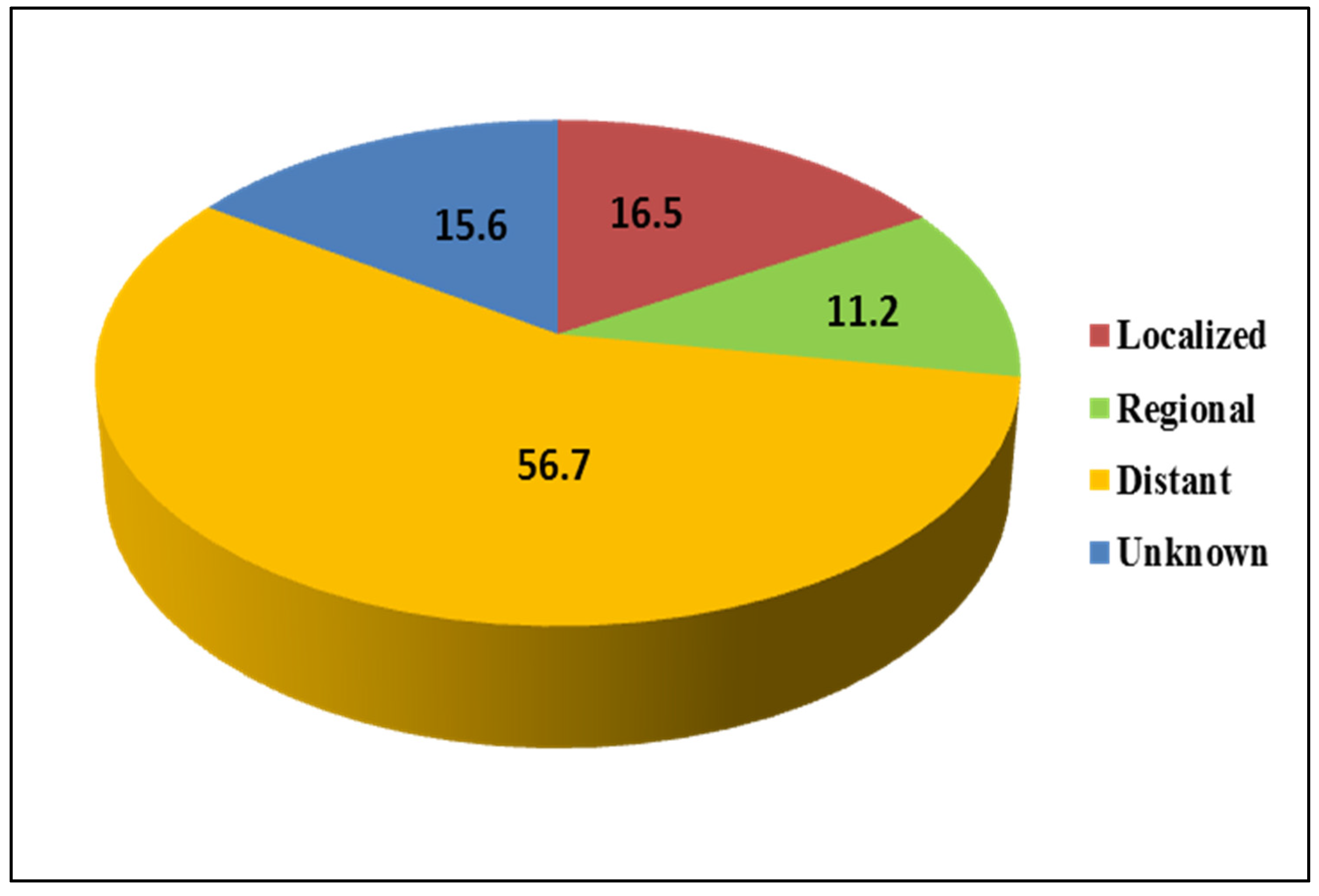
7. Lung Cancer: Stage Wise Distribution among Males and Females
8. Discussion
9. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CIR | Crude incidence rate |
| AIR | Age-specific incidence rate |
| ASIR | Age-standardized incidence rate |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Legato, M.J.; Bilezikian, J.P. (Eds.) Principles of Gender-Specific Medicine; Gulf Professional Publishing: Oxford, UK, 2004; Volume 2. [Google Scholar]
- Oglesby, I.K.; McElvaney, N.G.; Greene, C.M. MicroRNAs in inflammatory lung disease—Master regulators or target practice? Respir. Res. 2010, 11, 148. [Google Scholar] [CrossRef] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirsch, F.R.; Scagliotti, G.V.; Mulshine, J.L.; Kwon, R.; Curran, W.J.; Wu, Y.-L.; Paz-Ares, L. Lung cancer: Current therapies and new targeted treatments. Lancet 2017, 389, 299–311. [Google Scholar] [CrossRef]
- Scott, W.J.; Howington, J.; Feigenberg, S.; Movsas, B.; Pisters, K. Treatment of non-small cell lung cancer stage I and stage II: ACCP evidence-based clinical practice guidelines. Chest 2007, 132, 234S–242S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moyer, V.A. Screening for Lung Cancer: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2014, 160, 330–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosseini, M.; Naghan, P.A.; Karimi, S.; SeyedAlinaghi, S.; Bahadori, M.; Khodadad, K.; Mohammadi, F.; Keynama, K.; Masjedi, M.R. Environmental risk factors for lung cancer in Iran: A case-control study. Int. J. Epidemiol. 2009, 38, 989–996. [Google Scholar] [CrossRef] [Green Version]
- Althubiti, M.A.; Eldein, M.M.N. Trends in the incidence and mortality of cancer in Saudi Arabia. Saudi Med. J. 2018, 39, 1259–1262. [Google Scholar] [CrossRef]
- Ibrahim, E.; Bin Sadiq, B.M.; Banjar, L.; Awadalla, S.; Abomelha, M.S. Current and future cancer burden in Saudi Arabia: Meeting the challenge. Hematol. Stem Cell Ther. 2008, 1, 210–215. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Tao, S.; Shen, H.; Ma, J. Inhalation exposure to ambient polycyclic aromatic hydrocarbons and lung cancer risk of Chinese population. Proc. Natl. Acad. Sci. USA 2009, 106, 21063–21067. [Google Scholar] [CrossRef] [Green Version]
- Tammemägi, M.C.; Katki, H.A.; Hocking, W.G.; Church, T.R.; Caporaso, N.; Kvale, P.A.; Chaturvedi, A.K.; Silvestri, G.A.; Riley, T.L.; Commins, J.; et al. Selection Criteria for Lung-Cancer Screening. N. Engl. J. Med. 2013, 368, 728–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aggarwal, R.; Ranganathan, P. Study designs: Part 2—Descriptive studies. Perspect. Clin. Res. 2019, 10, 34. [Google Scholar] [CrossRef]
- Saudi Cancer Registry: Annual Reports. Available online: https://nhic.gov.sa/en/eServices/Pages/TumorRegistration.aspx (accessed on 20 January 2021).
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. (Eds.) AJCC Cancer Staging Manual; Springer International Publishing: Cham, Switzerland, 2017; ISBN 978-3-319-40617-6. [Google Scholar]
- Al-Ahmadi, K.; Al-Zahrani, A. NO2 and Cancer Incidence in Saudi Arabia. Int. J. Environ. Res. Public Health 2013, 10, 5844–5862. [Google Scholar] [CrossRef] [PubMed]
- Feldman, D.; Krishnan, A.V.; Swami, S.; Giovannucci, E.; Feldman, B.J. The role of vitamin D in reducing cancer risk and progression. Nat. Rev. Cancer 2014, 14, 342–357. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wang, S.; Che, X.; Liqun, Z. Vitamin D and Lung Cancer Risk: A Comprehensive Review and Meta-Analysis. Cell. Physiol. Biochem. 2015, 36, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.C.; Zhang, Z.L.; Wan, Z.; Wang, L.; Weber, P.; Eggersdorfer, M.; Qin, L.-Q.; Zhang, W. Circulating 25-hydroxyvitamin D and risk of lung cancer: A dose-response meta-analysis. Cancer Causes Control 2015, 26, 1719–1728. [Google Scholar] [CrossRef] [PubMed]
- Hussain, A.N.; Alkhenizan, A.H.; El Shaker, M.; Raef, H.; Gabr, A. Increasing trends and significance of hypovitaminosis D: A population-based study in the Kingdom of Saudi Arabia. Arch. Osteoporos. 2014, 9, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Al-Elq, A.H. The status of Vitamin D in medical students in the preclerkship years of a Saudi medical school. J. Fam. Community Med. 2012, 19, 100–104. [Google Scholar] [CrossRef] [Green Version]
- Bazarbashi, S.; Al-Eid, H.; Minguet, J. Cancer Incidence in Saudi Arabia: 2012 Data from the Saudi Cancer Registry. Asian Pac. J. Cancer Prev. APJCP 2017, 18, 2437–2444. [Google Scholar] [CrossRef]
- Lam, T.K.; Ruczinski, I.; Helzlsouer, K.J.; Shugart, Y.Y.; Caulfield, L.E.; Alberg, A.J. Cruciferous Vegetable Intake and Lung Cancer Risk: A Nested Case-Control Study Matched on Cigarette Smoking. Cancer Epidemiol. Prev. Biomark. 2010, 19, 2534–2540. [Google Scholar] [CrossRef] [Green Version]
- Büchner, F.L.; Bueno-De-Mesquita, H.B.; Ros, M.M.; Overvad, K.; Dahm, C.; Hansen, L.; Tjonneland, A.; Clavel-Chapelon, F.; Boutron-Ruault, M.-C.; Touillaud, M.; et al. Variety in Fruit and Vegetable Consumption and the Risk of Lung Cancer in the European Prospective Investigation into Cancer and Nutrition. Cancer Epidemiol. Prev. Biomark. 2010, 19, 2278–2286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahabir, S.; Forman, M.R.; Dong, Y.Q.; Park, Y.; Hollenbeck, A.R.; Schatzkin, A. Mineral Intake and Lung Cancer Risk in the NIH-American Association of Retired Persons Diet and Health Study. Cancer Epidemiol. Prev. Biomark. 2010, 19, 1976–1983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takata, Y.; Shu, X.-O.; Yang, G.; Li, H.; Dai, Q.; Gao, J.; Cai, Q.; Gao, Y.-T.; Zheng, W. Calcium Intake and Lung Cancer Risk Among Female Nonsmokers: A Report from the Shanghai Women’s Health Study. Cancer Epidemiol. Prev. Biomark. 2013, 22, 50–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansson, M.; Relton, C.; Ueland, P.M.; Vollset, S.E.; Midttun, Ø.; Nygård, O.; Slimani, N.; Boffetta, P.; Jenab, M.; Chapelon, F.C.; et al. Serum B Vitamin Levels and Risk of Lung Cancer. JAMA 2010, 303, 2377–2385. [Google Scholar] [CrossRef]
- Imai, H.; Kaira, K.; Mori, K.; Ono, A.; Akamatsu, H.; Matsumoto, S.; Taira, T.; Kenmotsu, H.; Harada, H.; Naito, T.; et al. Prognostic significance of diabetes mellitus in locally advanced non-small cell lung cancer. BMC Cancer 2015, 15, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Tseng, C.-H. Higher risk of mortality from lung cancer in Taiwanese people with diabetes. Diabetes Res. Clin. Pract. 2013, 102, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Bergamino, M.; Rullan, A.J.; Saigí, M.; Peiró, I.; Montanya, E.; Palmero, R.; Ruffinelli, J.C.; Navarro, A.; Arnaiz, M.D.; Brao, I.; et al. Fasting plasma glucose is an independent predictor of survival in patients with locally advanced non-small cell lung cancer treated with concurrent chemoradiotherapy. BMC Cancer 2019, 19, 165. [Google Scholar] [CrossRef] [PubMed]
- Alneami, Y.M.; Coleman, C.L. Risk Factors for and Barriers to Control Type-2 Diabetes among Saudi Population. Glob. J. Health Sci. 2016, 8, 10–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moradi-Lakeh, M.; Forouzanfar, M.H.; El Bcheraoui, C.; Daoud, F.; Afshin, A.; Hanson, S.W.; Vos, T.; Naghavi, M.; Murray, C.J.; Mokdad, A.H. High Fasting Plasma Glucose, Diabetes, and Its Risk Factors in the Eastern Mediterranean Region, 1990–2013: Findings From the Global Burden of Disease Study 2013. Diabetes Care 2016, 40, 22–29. [Google Scholar] [CrossRef] [Green Version]
- Sherif, S.; Sumpio, B.E. Economic development and diabetes prevalence in MENA countries: Egypt and Saudi Arabia comparison. World J. Diabetes 2015, 6, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Saudi Ministry of Health. Saudi Health Interview Survey (SHIS). 2013. Available online: http://www.healthdata.org/ksa/projects/saudihealth-interview-survey (accessed on 20 February 2021).
- Alghamdi, H.I.; Alshehri, A.; Farhat, G.N. An overview of mortality & predictors of small-cell and non-small cell lung cancer among Saudi patients. J. Epidemiol. Glob. Health 2017, 7, S1–S6. [Google Scholar] [CrossRef] [PubMed]
- Kingdom of Saudi Arabia Saudi Health Council Saudi Cancer Registry. Kingdom of Saudi Arabia Cancer Incidence Report 2014. Available online: https://nhic.gov.sa/eServices/Documents/2014.pdf (accessed on 16 February 2021).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Total Lung Cancer Incidences (All Ages in Males) | % | Total Incidences of Lung Cancer (All Ages in Females) | % |
|---|---|---|---|---|
| 2006 | 232 | 6.8 | 80 | 7 |
| 2007 | 323 | 9.5 | 89 | 7.8 |
| 2008 | 285 | 8.4 | 82 | 7.2 |
| 2009 | 276 | 8.1 | 103 | 9 |
| 2010 | 292 | 8.6 | 105 | 9.2 |
| 2011 | 343 | 10.1 | 109 | 9.5 |
| 2012 | 336 | 9.9 | 127 | 11.1 |
| 2013 | 326 | 9.6 | 109 | 9.5 |
| 2014 | 354 | 10.4 | 98 | 8.6 |
| 2015 | 324 | 9.6 | 92 | 8.1 |
| 2016 | 297 | 8.8 | 148 | 13 |
| Total | 3388 | 100 | 1142 | 100 |
| Overall | 308 | 9.1 | 104 | 9.1 |
| % | 100 | 100 |
| Region | Sex | CIR/ASIR | 2006 | 2016 | Difference |
|---|---|---|---|---|---|
| Asir | Male | CIR | 1.2 | 0.9 | −0.3 |
| ASIR | 1.8 | 1.1 | −0.7 | ||
| Female | CIR | 0.4 | 1.3 | 0.9 | |
| ASIR | 0.7 | 1.4 | 0.7 | ||
| Baha | Male | CIR | 2.5 | 2.2 | −0.3 |
| ASIR | 2.9 | 3.2 | 0.3 | ||
| Female | CIR | 0 | 0.5 | 0.5 | |
| ASIR | 0 | 0.6 | 0.6 | ||
| Madinah | Male | CIR | 2.7 | 2.1 | −0.6 |
| ASIR | 4.9 | 3.3 | −1.6 | ||
| Female | CIR | 1.3 | 0.4 | −0.9 | |
| ASIR | 2.4 | 0.5 | −1.9 | ||
| Jazan | Male | CIR | 1 | 0.5 | −0.5 |
| ASIR | 1.4 | 0.8 | −0.6 | ||
| Female | CIR | 0 | 0.3 | 0.3 | |
| ASIR | 0 | 0.4 | 0.4 | ||
| Qassim | Male | CIR | 1.2 | 1.6 | 0.4 |
| ASIR | 2 | 2.7 | 0.7 | ||
| Female | CIR | 0.9 | 0.6 | −0.3 | |
| ASIR | 1.3 | 1 | −0.3 | ||
| Hail | Male | CIR | 0 | 0.4 | 0.4 |
| ASIR | 0 | 0.5 | 0.5 | ||
| Female | CIR | 0 | 0.7 | 0.7 | |
| ASIR | 0 | 1 | 1 | ||
| Jouf | Male | CIR | 2.5 | 5.8 | 3.3 |
| ASIR | 5.1 | 10.1 | 5 | ||
| Female | CIR | 1.2 | 1.6 | 0.4 | |
| ASIR | 3.5 | 2.3 | −1.2 | ||
| Najran | Male | CIR | 1.1 | 0.5 | −0.6 |
| ASIR | 2.2 | 0.6 | −1.6 | ||
| Female | CIR | 0 | 0 | 0 | |
| ASIR | 0 | 0 | 0 | ||
| Riyadh | Male | CIR | 2.7 | 2.9 | 0.2 |
| ASIR | 6.3 | 4.6 | −1.7 | ||
| Female | CIR | 1.2 | 2.2 | 1 | |
| ASIR | 2.5 | 3.4 | 0.9 | ||
| Northern Region | Male | CIR | 1.6 | 2.1 | 0.5 |
| ASIR | 5.5 | 4.2 | −1.3 | ||
| Female | CIR | 1.6 | 2.1 | 0.5 | |
| ASIR | 4.4 | 4 | −0.4 | ||
| Makka | Male | CIR | 3.7 | 3.4 | −0.3 |
| ASIR | 6.6 | 4.5 | −2.1 | ||
| Female | CIR | 1.2 | 1.2 | 0 | |
| ASIR | 2 | 1.4 | −0.6 | ||
| Tabuk | Male | CIR | 2.8 | 3.8 | 1 |
| ASIR | 7.9 | 8 | 0.1 | ||
| Female | CIR | 0.3 | 2 | 1.7 | |
| ASIR | 1.1 | 4.1 | 3 | ||
| Eastern Province | Male | CIR | 3.7 | 5.1 | 1.4 |
| ASIR | 10.4 | 9.6 | −0.8 | ||
| Female | CIR | 1.1 | 2.5 | 1.4 | |
| ASIR | 2.4 | 3.7 | 1.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almatroudi, A. A Retrospective Cohort Study of Lung Cancer Incidences and Epidemiological Analysis in Saudi Arabian Population from 2006–2016. Int. J. Environ. Res. Public Health 2021, 18, 11827. https://doi.org/10.3390/ijerph182211827
Almatroudi A. A Retrospective Cohort Study of Lung Cancer Incidences and Epidemiological Analysis in Saudi Arabian Population from 2006–2016. International Journal of Environmental Research and Public Health. 2021; 18(22):11827. https://doi.org/10.3390/ijerph182211827
Chicago/Turabian StyleAlmatroudi, Ahmad. 2021. "A Retrospective Cohort Study of Lung Cancer Incidences and Epidemiological Analysis in Saudi Arabian Population from 2006–2016" International Journal of Environmental Research and Public Health 18, no. 22: 11827. https://doi.org/10.3390/ijerph182211827