
Factors Associated with Depression and Anxiety in Adults ≥60 Years Old during the COVID-19 Pandemic: A Systematic Review

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Evaluation of the Quality of the Studies
3. Results
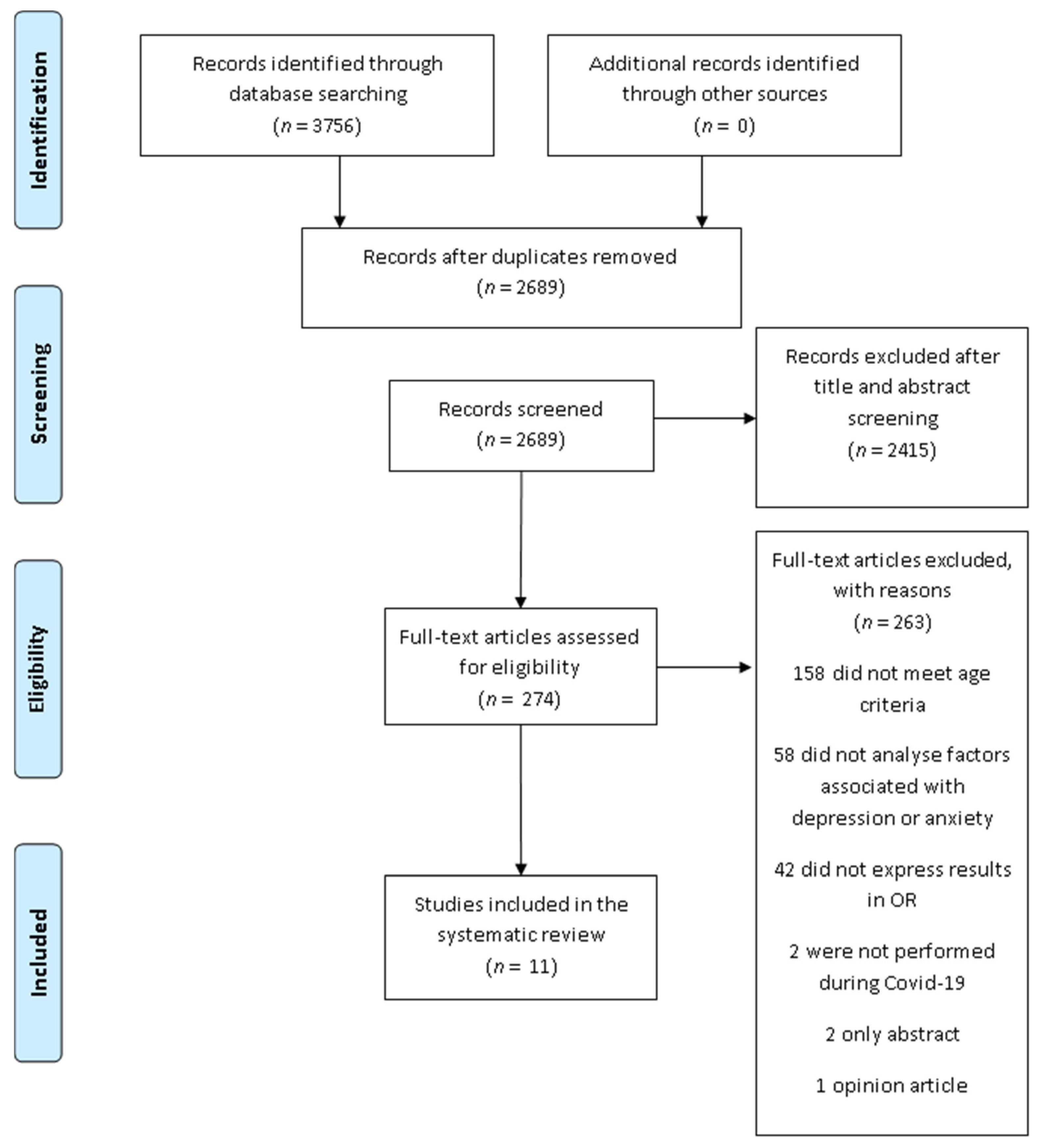
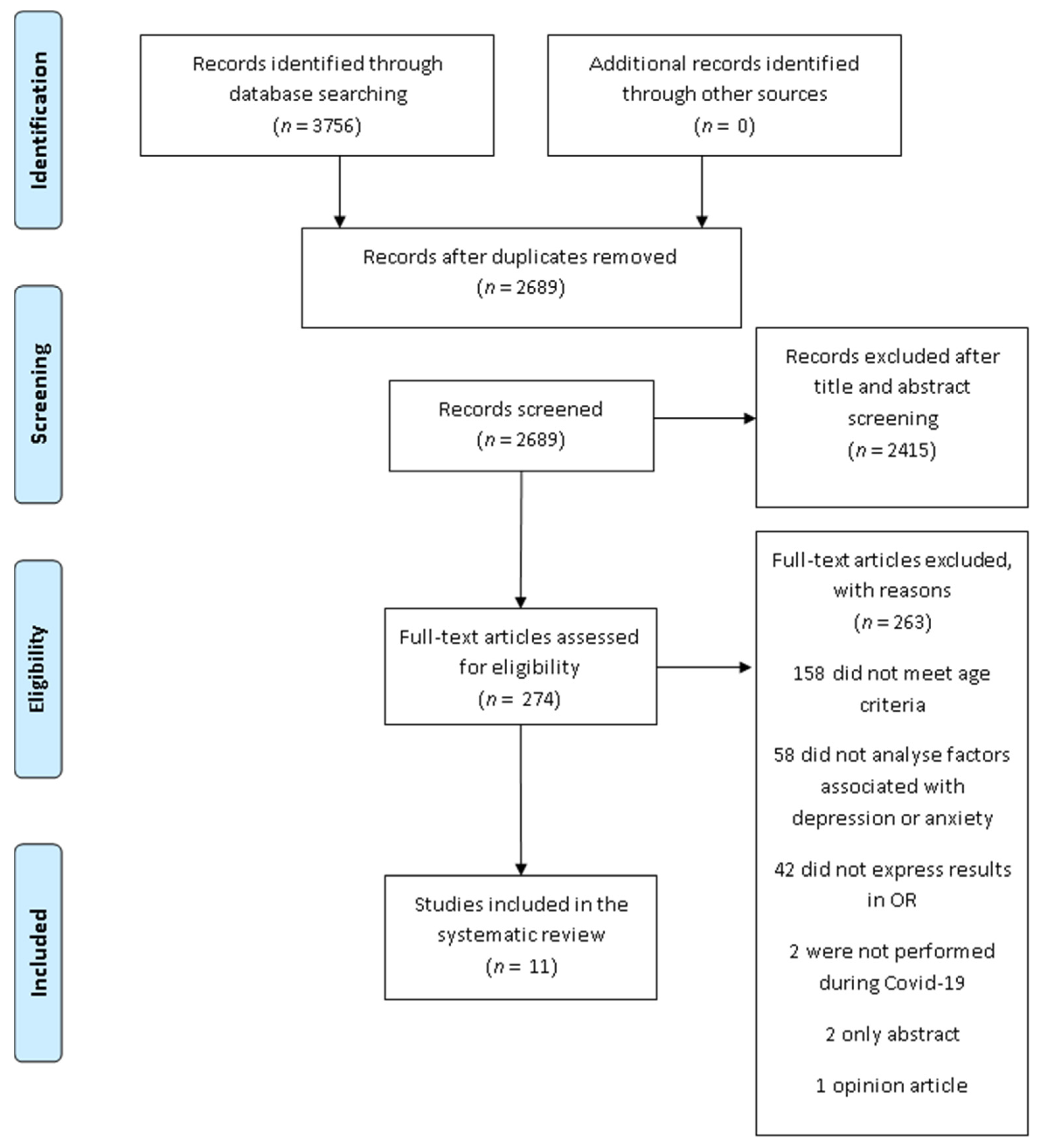
3.1. Study Selection
3.2. Study Characteristics
3.3. Gender
3.4. Age
3.5. Physical and Mental Conditions
3.6. Sleep Quality
3.7. Loneliness, Social Isolation and Personal Relationships
3.8. Other Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, L.; He, W.; Yu, X.; Hu, D.; Bao, M.; Liu, H.; Zhou, J.; Jiang, H. Coronavirus disease 2019 in elderly patients: Characteristics and prognostic factors based on 4-week follow-up. J. Infect. 2020, 80, 639–645. [Google Scholar] [CrossRef]
- Verity, R.; Okell, L.C.; Dorigatti, I.; Winskill, P.; Whittaker, C.; Imai, N.; Cuomo-Dannenburg, G.; Thompson, H.; Walker, P.G.T.; Fu, H.; et al. Estimates of the severity of coronavirus disease 2019: A model-based analysis. Lancet Infect. Dis. 2020, 20, 669–677. [Google Scholar] [CrossRef]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef] [Green Version]
- Xiang, G.; Xie, L.; Chen, Z.; Hao, S.; Fu, C.; Wu, Q.; Liu, X.; Li, S. Clinical risk factors for mortality of hospitalized patients with COVID-19: Systematic review and meta-analysis. Ann. Palliat. Med. 2021, 10, 2723–2735. [Google Scholar] [CrossRef]
- Chu, I.Y.-H.; Alam, P.; Larson, H.J.; Lin, L. Social consequences of mass quarantine during epidemics: A systematic review with implications for the COVID-19 response. J. Travel Med. 2020, 27, taaa192. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Kala, M.P.; Jafar, T.H. Factors associated with psychological distress during the coronavirus disease 2019 (COVID-19) pandemic on the predominantly general population: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0244630. [Google Scholar] [CrossRef]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Marcén-Román, Y.; Gasch-Gallen, A.; de la Mota, I.V.M.; Calatayud, E.; Gómez-Soria, I.; Rodríguez-Roca, B. Stress Perceived by University Health Sciences Students, 1 Year after COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 5233. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, R.; Burns, A.; Leavey, G.; Leroi, I.; Burholt, V.; Lubben, J.; Holt-Lunstad, J.; Victor, C.; Lawlor, B.; Vilar-Compte, M.; et al. Impact of the COVID-19 Pandemic on Loneliness and Social Isolation: A Multi-Country Study. Int. J. Environ. Res. Public Health 2021, 18, 9982. [Google Scholar] [CrossRef] [PubMed]
- Lahiri, A.; Jha, S.S.; Bhattacharya, S.; Ray, S.; Chakraborty, A. Effectiveness of preventive measures against COVID-19: A systematic review of In Silico modeling studies in indian context. Indian J. Public Health 2020, 64, S156–S167. [Google Scholar] [CrossRef]
- Shankar, A.; McMunn, A.; Demakakos, P.; Hamer, M.; Steptoe, A. Social isolation and loneliness: Prospective associations with functional status in older adults. Health Psychol. 2017, 36, 179–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grolli, R.E.; Mingoti, M.E.D.; Bertollo, A.G.; Luzardo, A.R.; Quevedo, J.; Réus, G.Z.; Ignácio, Z.M. Impact of COVID-19 in the Mental Health in Elderly: Psychological and Biological Updates. Mol. Neurobiol. 2021, 58, 1905–1916. [Google Scholar] [CrossRef]
- Maggi, G.; Baldassarre, I.; Barbaro, A.; Cavallo, N.D.; Cropano, M.; Nappo, R.; Santangelo, G. Mental health status of Italian elderly subjects during and after quarantine for the COVID-19 pandemic: A cross-sectional and longitudinal study. Psychogeriatrics 2021, 21, 540–551. [Google Scholar] [CrossRef] [PubMed]
- Levkovich, I.; Shinan-Altman, S.; Schvartz, N.E.; Alperin, M. Depression and Health-Related Quality of Life Among Elderly Patients during the COVID-19 Pandemic in Israel: A Cross-sectional Study. J. Prim. Care Community Health 2021, 12, 2150132721995448. [Google Scholar] [CrossRef]
- Gorrochategi, M.P.; Munitis, A.E.; Santamaria, M.D.; Etxebarria, N.O. Stress, Anxiety, and Depression in People Aged Over 60 in the COVID-19 Outbreak in a Sample Collected in Northern Spain. Am. J. Geriatr. Psychiatry 2020, 28, 993–998. [Google Scholar] [CrossRef]
- De Pue, S.; Gillebert, C.; Dierckx, E.; Vanderhasselt, M.-A.; De Raedt, R.; Bussche, E.V.D. The impact of the COVID-19 pandemic on wellbeing and cognitive functioning of older adults. Sci. Rep. 2021, 11, 1–11. [Google Scholar] [CrossRef]
- Briggs, R.; McDowell, C.P.; De Looze, C.; Kenny, R.A.; Ward, M. Depressive Symptoms Among Older Adults Pre– and Post–COVID-19 Pandemic. J. Am. Med. Dir. Assoc. 2021, 22, 2251–2257. [Google Scholar] [CrossRef]
- Lee, A.T.C.; Mo, F.Y.M.; Lam, L.C.W. Higher psychogeriatric admissions in COVID-19 than in severe acute respiratory syndrome. Int. J. Geriatr. Psychiatry 2020, 35, 1449–1457. [Google Scholar] [CrossRef]
- Maier, A.; Riedel-Heller, S.G.; Pabst, A.; Luppa, M. Risk factors and protective factors of depression in older people 65+. A systematic review. PLoS ONE 2021, 16, e0251326. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bobes-Bascarán, T.; Sáiz, P.A.; Velasco, A.; Martínez-Cao, C.; Pedrosa, C.; Portilla, A.; de la Fuente-Tomas, L.; García-Alvarez, L.; García-Portilla, M.P.; Bobes, J. Early Psychological Correlates Associated With COVID-19 in A Spanish Older Adult Sample. Am. J. Geriatr. Psychiatry 2020, 28, 1287–1298. [Google Scholar] [CrossRef] [PubMed]
- Carlos, A.F.; Poloni, T.E.; Caridi, M.; Pozzolini, M.; Vaccaro, R.; Rolandi, E.; Cirrincione, A.; Pettinato, L.; Vitali, S.F.; Tronconi, L.; et al. Life during COVID-19 lockdown in Italy: The influence of cognitive state on psychosocial, behavioral and lifestyle profiles of older adults. Aging Ment. Health 2021, 1–10. [Google Scholar] [CrossRef]
- Robb, C.E.; De Jager, C.A.; Ahmadi-Abhari, S.; Giannakopoulou, P.; Udeh-Momoh, C.; McKeand, J.; Price, G.; Car, J.; Majeed, A.; Ward, H.; et al. Associations of Social Isolation with Anxiety and Depression During the Early COVID-19 Pandemic: A Survey of Older Adults in London, UK. Front. Psychiatry 2020, 11, 591120. [Google Scholar] [CrossRef] [PubMed]
- Di Santo, S.G.; Franchini, F.; Filiputti, B.; Martone, A.; Sannino, S. The Effects of COVID-19 and Quarantine Measures on the Lifestyles and Mental Health of People Over 60 at Increased Risk of Dementia. Front. Psychiatry 2020, 11, 578628. [Google Scholar] [CrossRef] [PubMed]
- Do, B.N.; Nguyen, P.-A.; Pham, K.M.; Nguyen, H.C.; Nguyen, M.H.; Tran, C.Q.; Nguyen, T.T.P.; Tran, T.V.; Pham, L.V.; Tran, K.V.; et al. Determinants of Health Literacy and Its Associations with Health-Related Behaviors, Depression Among the Older People With and Without Suspected COVID-19 Symptoms: A Multi-Institutional Study. Front. Public Health 2020, 8, 581746. [Google Scholar] [CrossRef]
- Li, W.; Zhao, N.; Yan, X.; Zou, S.; Wang, H.; Li, Y.; Xu, X.; Du, X.; Zhang, L.; Zhang, Q.; et al. The prevalence of depressive and anxiety symptoms and their associations with quality of life among clinically stable older patients with psychiatric disorders during the COVID-19 pandemic. Transl. Psychiatry 2021, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kitani-Morii, F.; Kasai, T.; Horiguchi, G.; Teramukai, S.; Ohmichi, T.; Shinomoto, M.; Fujino, Y.; Mizuno, T. Risk factors for neuropsychiatric symptoms in patients with Parkinson’s disease during COVID-19 pandemic in Japan. PLoS ONE 2021, 16, e0245864. [Google Scholar] [CrossRef] [PubMed]
- McArthur, C.; Saari, M.; Heckman, G.A.; Wellens, N.; Weir, J.; Hebert, P.; Turcotte, L.; Jbilou, J.; Hirdes, J.P. Evaluating the Effect of COVID-19 Pandemic Lockdown on Long-Term Care Residents’ Mental Health: A Data-Driven Approach in New Brunswick. J. Am. Med. Dir. Assoc. 2021, 22, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Piskorz, D.; Barragán, A.P.; Santi, R.L.; Vázquez, G.; Ortiz, G.S.; Zambrano, L.R.; Castillo, M.M.; Roa, C.; Baños, M.; Ramos, M.G.; et al. Psychological Impact of the Pandemic on Ambulatory Cardiometabolic Patients Without Evidence of SARS-CoV-2 Infection. The CorCOVID Latam Psy Study. Curr. Probl. Cardiol. 2021, 46, 100737. [Google Scholar] [CrossRef] [PubMed]
- Cigiloglu, A.; Ozturk, Z.A.; Efendioglu, E.M. How have older adults reacted to coronavirus disease 2019? Psychogeriatrics 2021, 21, 112–117. [Google Scholar] [CrossRef]
- Bérard, E.; Kai, S.H.Y.; Coley, N.; Bongard, V.; Ferrières, J. Lockdown-related factors associated with the worsening of cardiovascular risk and anxiety or depression during the COVID-19 pandemic. Prev. Med. Rep. 2021, 21, 101300. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Sears, K.; Sfetcu, R.; Currie, M.; Lisy, K.; Tufanaru, C.; Qureshi, R.; Mattis, P.; & Mu, P. Conducting systematic reviews of association (etiology): The Joanna Briggs Institute’s approach. Int. J. Evid. 2015, 13, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Kisely, S.; Warren, N.; McMahon, L.; Dalais, C.; Henry, I.; Siskind, D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: Rapid review and meta-analysis. BMJ 2020, 369, m1642. [Google Scholar] [CrossRef] [PubMed]
- Swendeman, D.; Fehrenbacher, A.E.; Roy, S.; Das, R.; Ray, P.; Sumstine, S.; Ghose, T.; Jana, S. Gender disparities in depression severity and coping among people living with HIV/AIDS in Kolkata, India. PLoS ONE 2018, 13, e0207055. [Google Scholar] [CrossRef]
- Assariparambil, A.R.; Noronha, J.A.; Kamath, A.; Adhikari, P.; Nayak, B.S.; Shankar, R.; George, A. Depression among older adults: A systematic review of South Asian countries. Psychogeriatrics 2021, 21, 201–219. [Google Scholar] [CrossRef]
- Acciai, F.; Hardy, M. Depression in later life: A closer look at the gender gap. Soc. Sci. Res. 2017, 68, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Q.-W.; Qian, S.; Li, J.-Y.; Jia, R.-X.; Wang, Y.-Q.; Xu, Y. Risk factors for depressive symptoms among older Chinese adults: A meta-analysis. J. Affect. Disord. 2020, 277, 341–346. [Google Scholar] [CrossRef]
- Kuehner, C. Gender differences in unipolar depression: An update of epidemiological findings and possible explanations. Acta Psychiatr. Scand. 2003, 108, 163–174. [Google Scholar] [CrossRef]
- Lee, A.M.W.S.; Wong, J.G.; McAlonan, G.M.; Cheung, V.; Cheung, C.; Sham, P.C.; Chu, C.-M.; Wong, P.-C.; Tsang, K.W.; Chua, S.E. Stress and Psychological Distress among SARS Survivors 1 Year after the Outbreak. Can. J. Psychiatry 2007, 52, 233–240. [Google Scholar] [CrossRef] [Green Version]
- Bryant, C.; Jackson, H.; Ames, D. The prevalence of anxiety in older adults: Methodological issues and a review of the literature. J. Affect. Disord. 2008, 109, 233–250. [Google Scholar] [CrossRef]
- Zhao, Y.-J.; Jin, Y.; Rao, W.-W.; Li, W.; Zhao, N.; Cheung, T.; Ng, C.H.; Wang, Y.-Y.; Zhang, Q.-E.; Xiang, Y.-T. The prevalence of psychiatric comorbidities during the SARS and COVID-19 epidemics: A systematic review and meta-analysis of observa-tional studies. J. Affect. Disord. 2021, 287, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Bishwajit, G.; O’Leary, D.P.; Ghosh, S.; Yaya, S.; Shangfeng, T.; Feng, Z. Physical inactivity and self-reported depression among middle- and older-aged population in South Asia: World health survey. BMC Geriatr. 2017, 17, 100. [Google Scholar] [CrossRef] [PubMed]
- Zasadzka, E.; Pieczyńska, A.; Trzmiel, T.; Kleka, P.; Pawlaczyk, M. Correlation between Handgrip Strength and Depression in Older Adults—A Systematic Review and a Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4823. [Google Scholar] [CrossRef] [PubMed]
- Tsutsumimoto, K.; Doi, T.; Shimada, H.; Makizako, H.; Hotta, R.; Nakakubo, S.; Suzuki, T. Combined Effect of Slow Gait Speed and Depressive Symptoms on Incident Disability in Older Adults. J. Am. Med. Dir. Assoc. 2016, 17, 123–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Author and Year | Study Design | Time of the Study and Country | Participants Information | N | Age | Gender (%) | Depression Outcome Measure | Cutoff Score | Results (OR [95%CI]) | Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| Bobes-Bascarán et al. 2020 [21] | Cross-sectional | Between 19 and 26 March 2020, during the lockdown, in Spain. | Adults ≥ 60 recruited during the lockdown. | 2194 | Mean: 65.62 ± 5.05 | 54.6% Female | DASS-21 depression subscale | >4 points in the subscale | Multivariate Logistic Regression: female 2.004 (1.559–2.575), never married 0.665 (0.456–0.970); civil servant 0.530 (0.293–0.957); retired 0.539 (0.311–0.934); able to enjoy free time 0.268 (0.148–0.488); family/friends infected with COVID-19 1.631 (1.247–2.132); past mental disorders 1.810 (1.352–2.423); current mental disorders 3.132 (2.043–4.803). | 8 |
| Carlos et al. 2020 [22] | Cross-sectional | Between 9 April 2020, one month after the imple- mentation of lockdown, and 4 May 2020, the day of transition to “phase 2”, in Italy. | Adults ≥ 65, stratified by level of neurocognitive deficit. | 204 | Median: 82 | 57.4% Female | GDS-5 | ≥2 | Logistic regression model after controlling for other factors (age, dementia, new hobbies, digital literacy): sleep disturbances 2.29 (1.06–4.93); general health problems 2.45 (1.16–5.16); exercise 0.30 (0.12–0.72). | 7 |
| Robb et al. 2020 [23] | Cross-sectional | Between 30 April and 8 July 2020, in the United Kingdom. | Adults ≥ 50 from Cognitive Health in Ageing Register for Interventional and Observation Trials (CHARIOT). | 7127 | Mean: 70.6 ± 7.4 | 54.1% Female | Worsening or improving depression. Measured with the HADS-depression, with questions added to each ítem to self-report change from the beginning of COVID-19 restrictions. | ≥4 answers for positive or negative change for considering depression worsening or improvement. | Multivariable model adjusted for age, sex, hypertension, hypercholesterolemia, type 2 diabetes, chronic obstructive pulmonary disease, cardiovascular disease and mental health conditions before lockdown: Worsened: women 2.46 (2.10–2.89); age 0.81 (0.77–0.85); single/widow/divorced 1.37 (1.17–1.59); smoker 1.41 (0.97–2.04); alcohol consumption (units p/w) 1.01 (1.00–1.01); poor sleep < once per week 2.00 (1.51–2.65); poor sleep 1–2 times per week 2.84 (2.13–3.79); poor sleep ≥3 times per week 6.91 (5.21–9.15); feeling lonely rarely 2.72 (2.16–3.43); feeling lonely sometimes 7.14 (5.78–8.82); feeling lonely often 17.24 (13.20–22.50); live alone 1.32 (1.12–1.55); friend/family social media contact 2–6 times per week 1.05 (0.90–1.23); friend/family social media contact, ≤once per week 0.99 (0.77–1.27). Improved: women 1.14 (0.77–1.69); age 0.89 (0.78–1.02); single/widow/divorced 0.65 (0.41–1.03); smoker 2.07 (0.94–4.57); alcohol consumption (units p/w) 0.97 (0.95–0.99); poor sleep < once per week 0.72 (0.44–1.18); poor sleep 1–2 times per week 0.78 (0.45–1.35); poor sleep ≥3 times per week 0.75 (0.40–1.42); feeling lonely rarely 0.62 (0.37–1.02); feeling lonely sometimes 0.49 (0.26–0.91); feeling lonely often 0.77 (0.30–1.99); live alone 0.62 (0.37–1.02); friend/family social media contact 2–6 times per week 0.72 (0.47–1.11); friend/family social media contact, ≤once per week 0.69 (0.35–1.36). | 7 |
| Di Santo et al. 2020 [24] | Cross-sectional | From 21 April to 7 May 2020, in Italy. | Adults ≥ 60 with mild cognitive impairment, part of a clinical trial. | 128 | Mean: 74.29 ± 6.51 | 81% Female | GDS-5 | ≥2 | Multivariable logistic regression analysis: alone or poor relation with cohabitants 2.79 (1.20–6.49); poor sleep quality 1.85 (0.80–4.29); no pets 0.16 (0.02–1.20). | 8 |
| Do et al. 2020 [25] | Cross-sectional | Between 14 February and 2 March 2020, in Vietnam. | Adults aged 60–85. | 928 | Mean: 68.2 ± 6.51 | 56.3% Female | PHQ-9 | ≥10 | Logistic regression model adjusted for age, marital status (in the group without COVID-19), education and social status: health literacy in subjects without COVID-19 1.02 (0.96–1.09); health literacy in subjects with COVID-19 0.91 (0.87–0.94). | 8 |
| Li et al. 2021 [26] | Cross-sectional | Between 22 May and 15 July 2020, in China. | Adults ≥ 50 with psychiatric disorders. | 1063 | Mean: 62.8 ± 9.4 | 67.4% Female | PHQ-9 | ≥5 depression; ≥10 moderate to severe depression. | Binary logistic regression analysis: Depression: rural area 1.29 (0.88–1.89); having severe physical diseases 1.35 (0.85–2.15); poor treatment adherence 1.25 (0.88–1.78); difficulty attending psychiatric hospital 1.38 (0.95–1.99); schizophrenia 0.95 (0.51–1.77); organic mental disorder 0.57 (0.28–1.16); other psychiatric diseases 0.50 (0.35–0.71); education years 0.99 (0.94–1.03); insomnia (ISI score) 1.29 (1.24–1.34); pain score 1.14 (1.03–1.25). Combined depression and anxiety: rural area 1.36 (0.95–1.93); having severe physical diseases 1.49 (0.98–2.26); poor treatment adherence 1.42 (1.03–1.95); difficulty attending psychiatric hospital 1.37 (0.97–1.91); schizophrenia 0.50 (0.26–0.97); organic mental disorder 0.66 (0.34–1.29); other psychiatric diseases 0.53 (0.38–0.73); education years 0.98 (0.94–1.03); insomnia (ISI score) 1.19 (1.16–1.23); pain score 1.15 (1.06–1.25). | 8 |
| Kitani-Morii et al. 2021 [27] | Cross-sectional | From 22 April to 15 May 2020 during the state of emergency in Japan. | Adults with Parkinson’s disease and control group. | 71 (39 Parkinson; 32 control) | Mean: 72.3 ± 10.9 (Parkinson); 66.4 ± 13.8 (control) | 35% Female (Parkinson); 84% Female (Control) | PHQ-9 | ≥10 | Multivariate logistic regression analyses in patients with Parkinson’s disease: male 5.66 (0.51–62.47); aged between 70 and 79 0.61 (0.05–0.08); aged ≥80 0.19 (0.01–3.93); disease duration ≥5 years 1.01 (0.13–7.78); HY stage 3,4 10.17 (0.57–182.91); MDS-UPDRS part 2 1.31 (1.04–1.66); L-dopa ≥600 mg 1.39 (0.13–15.26); dopamine agonist 9.33 (0.85–102.72). | 8 |
| McArthurt et al. 2021 [28] | Longitudinal Retrospective | Assessments from January 2017 to June 2020, in Canada. | Long-term care homes residents. | 765 | Mean: 81.4 ± 11.5 | 59.5% Female | DRS | ≥3 | Longitudinal Multivariate Model: age 1.00 (0.98–1.01); female 2.11 (1.47–3.04); lockdown 0.86 (0.66–1.11); being in the reference home “facility X” 0.45 (0.27–0.74); Alzheimer’s and other dementias 0.69 (0.48–0.99); CPS 1.55 (1.18–2.04); CPS 2 measure 0.92 (0.88–0.96); CHESS 1.17 (1.07–1.29); ABS 1.28 (1.22–1.34); ADL Hierarchy 1.11 (1.00–1.24). | 10 |
| Piskorz et al. 2021 [29] | Cross-sectional | From 15 June to 15 July 2020, in Mexico, Guatemala, El Salvador, Costa Rica, Cuba, the Dominican Republic, Venezuela, Colombia, Ecuador, Peru, Paraguay, Chile, and Argentina. | Adults with cardiometabolic disease were recruited during the lockdown. | 4216 | Mean: 60.35 ± 15.39 | 49.07% Female | DSM-5 | 1 positive answer to the main questions or 3 or more positive answers to the additional questions. | Multivariate logistic regression: female 1.72 (1.40–2.11); consuming ≥5 medications/day 1.29 (1.00–1.66); physical activity less than 100 minutes per week 1.36 (1.10–1.67); low fruits and vegetables consumption 1.46 (1.05–2.03); poor treatment adherence 1.43 (1.10–1.85); reduced food intake 2.10 (1.68–2.62). | 7 |
| Cigiloglu et al. 2021 [30] | Cross-sectional | 40 days after the detection of the first national COVID-19 case and 30 days after curfew was declared in Turkey. | Adults ≥ 65 who had to remain at home during the pandemic. | 104 | Stratified by age group: 65–74, 72.1%; 75–84, 17.3%; ≥85, 10.6%. | 41.3% Female | GDS-15 | ≥5 | Multivariate logistic regression analysis: female 2.25 (0.89–5.64); age 1.53 (0.78–2.98); monthly income medium vs low 0.34 (0.08–1.46); monthly income high vs low 0.13 (0.04–0.44); number of chronic diseases 1.08 (0.71–1.65). | 7 |
| Bérard et al. 2021 [31] | Cross-sectional | From 17 April to 10 May 2020, with mean time (±standard deviation) in lockdown before interviews of 44 days (±6 days), in France. | Adults aged between 50–89 during lockdown were recruited from a previous population-based study (PSYCOV-CV). | 536 (489 analysis of the factors associated with depression or anxiety) | Median: 67 | 52% Female | PHQ-9 | >4 | Multivariate logistic regression analysis: Depression or Anxiety: female gender 1.98 (1.23–3.20); home with balcony or terrace 0.21 (0.04–1.04); home with garden 0.29 (0.06–1.26); not in total agreement with the effectiveness of preventive measures 2.46 (1.42–4.27); feeling socially isolated during lockdown 1.68 (1.05–2.67); worsening relationship with a partner since the beginning of lockdown 5.24 (2.11–13.0); pre-lockdown diet quality score > median 0.51 (0.31–0.85); history of anxiety 7.34 (4.45–12.1). | 3 |
| Author and Year | Study Design | Time of the Study and Country | Participants Information | N | Age | Gender (%) | Anxiety Outcome Measure | Cutoff Score | Results (OR [95%CI]) | Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| Bobes-Bascarán et al. 2020 [21] | Cross-sectional | Between 19 March and 26 March 2020, during the lockdown, in Spain. | Adults ≥ 60 recruited during the lockdown. | 2194 | Mean: 65.62 ± 5.05 | 54.6% Female | DASS-21 anxiety subscale | >4 points in the subscale | Multivariate logistic regression: age 0.876 (0.800–0.960); female 3.320 (1.511–7.294); able to enjoy free time 0.103 (0.047–0.227); more than 14 days with COVID-19 symptoms 7.584 (1.398–41.146); current mental disorders 6.202 (3.005–12.799). | 8 |
| Robb et al. 2020 [23] | Cross-sectional | Between 30 April and 8 July 2020, in the United Kingdom. | Adults ≥ 50 from Cognitive Health in Ageing Register for Interventional and Observation Trials (CHARIOT). | 7127 | Mean: 70.6 ± 7.4 | 54.1% Female | Worsening or improving anxiety. Measured with the HADS-anxiety, with questions added to each ítem in order to self-report change from the beginning of COVID-19 restrictions. | ≥4 answers for positive or negative change for considering anxiety worsening or improvement | Multivariable model adjusted for age, sex, hypertension, hypercholesterolemia, type 2 diabetes, chronic obstructive pulmonary disease, cardiovascular disease and mental health conditions before lockdown: Worsened: women 2.42 (2.06–2.85), age 0.78 (0.75–0.83); single/widow/divorced 1.17 (1.00–1.37); smoker 1.16 (0.79–1.72); alcohol consumption (units p/w) 1.00 (1.00–1.01); poor sleep < once per week 1.81 (1.34–2.45); poor sleep 1–2 times per week 3.50 (2.59–4.73); poor sleep ≥3 times per week 7.67 (5.69–10.33); feeling lonely rarely 1.65 (1.32–2.07); feeling lonely sometimes 4.73 (3.87–5.77); feeling lonely often 10.85 (8.39–14.03); live alone 1.15 (0.98–1.36); friend/family social media contact 2–6 times per week 0.81 (0.68–0.95); friend/family social media contact, ≤ once per week 0.77 (0.59–1.00). Improved: women 1.7 (1.36–2.16); age 0.97 (0.89–1.04); single/widow/divorced 1.30 (1.03–1.64); smoker 1.36 (0.78–2.38); alcohol consumption (units p/w) 1.00 (0.99–1.01); poor sleep < once per week 0.53 (0.41–0.69); poor sleep 1–2 times per week 0.43 (0.31–0.60); poor sleep ≥3 times per week 0.41 (0.28–0.61); feeling lonely rarely 0.72 (0.56–0.96); feeling lonely sometimes 0.62 (0.45–0.86); feeling lonely often 0.53 (0.28–0.99); live alone 1.05 (0.82–1.35); friend/family social media contact 2–6 times per week 0.74 (0.57–0.94); friend/family social media contact, ≤ once per week 0.76 (0.51–1.11). | 7 |
| Di Santo et al. 2020 [24] | Cross-sectional | From 21 April to 7 May 2020, in Italy. | Adults ≥ 60 with mild cognitive impairment, part of a clinical trial. | 128 | Mean: 74.29 ± 6.51 | 81% Female | GAD-7 | ≥10 | Multiple logistic models: subjective cognitive disorder 4.39 (1.03–18.69); cold/flu symptoms 4.01 (1.13–14.24); reduction in productive activities 4.42 (1.10–17.76); time spent searching information 2.45 (0.71–8.45). | 8 |
| Li et al. 2021 [26] | Cross-sectional | Between 22 May and 15 July 2020, in China. | Adults ≥ 50 with psychiatric disorders. | 1063 | Mean: 62.8 ± 9.4 | 67.4% Female | GAD-7 | ≥5 anxiety; ≥10 moderate to severe anxiety. | Binary logistic regression analysis: Anxiety: rural area 1.20 (0.86–1.68); having severe physical diseases 1.57 (1.05–2.35); poor treatment adherence 1.50 (1.11–2.03); difficulty attending psychiatric hospital 1.33 (0.96–1.84); schizophrenia 0.67 (0.37–1.22); organic mental disorder 0.78 (0.41–1.47); other psychiatric diseases 0.74 (0.54–1.01); education years 0.97 (0.93–1.01); insomnia (ISI score) 1.15 (1.12–1.18); pain score 1.11 (1.02–1.20). Combined depression and anxiety: rural area 1.36 (0.95–1.93); having severe physical diseases 1.49 (0.98–2.26); poor treatment adherence 1.42 (1.03–1.95); difficulty attending psychiatric hospital 1.37 (0.97–1.91); schizophrenia 0.50 (0.26–0.97); organic mental disorder 0.66 (0.34–1.29); other psychiatric diseases 0.53 (0.38–0.73); education years 0.98 (0.94–1.03); insomnia (ISI score) 1.19 (1.16–1.23); pain score 1.15 (1.06–1.25). | 8 |
| Kitani-Morii et al. 2021 [27] | Cross-sectional | From 22 April to 15 May 2020, during the state of emergency, in Japan. | Adults with Parkinson’s disease and control group. | 71 (39 Parkinson; 32 control) | Mean: 72.3 ± 10.9 (Parkinson); 66.4 ± 13.8 (control) | 35% Female (Parkinson); 84% Female (Control) | GAD-7 | ≥7 | Multivariate logistic regression analysis in patients with Parkinson’s disease: male 17.12 (1.13–257.27); aged between 70 and 79 0.55 (0.04–7.69); aged ≥ 80 0.16 (0.01–3.08); disease duration ≥5 years 0.35 (0.04–3.08); HY stage 3,4 8.19 (0.52–128.74); MDS-UPDRS part 2 1.36 (1.07–1.72); dopamine agonist 13.07 (0.81–210.16). | 6 |
| Cigiloglu et al. 2021 [30] | Cross-sectional | 40 days after the detection of the first national COVID-19 case and 30 days after curfew was declared, in Turkey. | Adults ≥ 65 who had to remain at home during the pandemic. | 104 | Stratified by age group: 65–74, 72.1%; 75–84, 17.3%; ≥85, 10.6%. | 41.3% Female | GAI | 8/9 | Multivariate logistic regression analysis: female 3.25 (1.22–8.70); age 0.89 (0.45–1.75); monthly income medium vs low 0.21 (0.04–1.19); monthly income high vs low 0.07 (0.02–0.35); number of chronic diseases 1.18 (0.75–1.86). | 7 |
| Bérard et al. 2021 [31] | Cross-sectional | From 17 April to 10 May 2020, with mean time (±standard deviation) in lockdown before interviews of 44 days (±6 days), in France. | Adults aged between 50 and 89 during lockdown were recruited from a previous population-based study (PSYCOV-CV). | 536 (489 for the analysis of the factors associated with depression or anxiety) | Median: 67 | 52% Female | GAD-7 | >4 | Multivariate logistic regression analysis: Depression or Anxiety: female gender 1.98 (1.23–3.20); home with balcony or terrace 0.21 (0.04–1.04); home with garden 0.29 (0.06–1.26); not in total agreement with the effectiveness of preventive measures 2.46 (1.42–4.27); feeling socially isolated during lockdown 1.68 (1.05–2.67); worsening relationship with a partner since the beginning of lockdown 5.24 (2.11–13.0); pre-lockdown diet quality score > median 0.51 (0.31–0.85); history of anxiety 7.34 (4.45–12.1). | 3 |
| Cross-Sectional Studies | Inclusion Criteria | Participants and Setting | Exposition | Measurement of the Condition | Identify Confounding Factors | Deal with Confounding Factors | Outcomes | Statistical Analysis | Total |
|---|---|---|---|---|---|---|---|---|---|
| Author and Year | |||||||||
| Bobes-Bascarán et al. 2020s | + | + | + | + | + | + | + | + | 8 |
| Carlos et al. 2020 | + | + | + | + | - | + | + | + | 7 |
| Robb et al. 2020 | + | + | + | + | + | + | - | + | 7 |
| Di Santo et al. 2020 | + | + | + | + | + | + | + | + | 8 |
| Do et al. 2020 | + | + | + | + | + | + | + | + | 8 |
| Li et al. 2021 | + | + | + | + | + | + | + | + | 8 |
| Kitani-Morii et al. 2021 | + | + | + | + | - | - | + | + | 6 |
| Piskorz et al. 2021 | + | + | + | + | + | ? | + | + | 7 |
| Cigiloglu et al. 2021 | + | ? | + | + | + | + | + | + | 7 |
| Bérard et al. 2021 | ? | - | ? | + | - | - | + | + | 3 |
| Cohort Studies | Group Recruitment | Group Exposure | Exposure Measurement | Identify Confounding Factors | Deal with Confounding Factors | Not Exposure Previous the Study | Outcomes | Follow Up Time | Follow Up Complete | Strategies to Address Incomplete Follow up | Statistical Analysis | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author and Year | ||||||||||||
| McArthur et al. 2021 | + | + | + | + | + | - | + | + | + | - | + | 10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciuffreda, G.; Cabanillas-Barea, S.; Carrasco-Uribarren, A.; Albarova-Corral, M.I.; Argüello-Espinosa, M.I.; Marcén-Román, Y. Factors Associated with Depression and Anxiety in Adults ≥60 Years Old during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 11859. https://doi.org/10.3390/ijerph182211859
Ciuffreda G, Cabanillas-Barea S, Carrasco-Uribarren A, Albarova-Corral MI, Argüello-Espinosa MI, Marcén-Román Y. Factors Associated with Depression and Anxiety in Adults ≥60 Years Old during the COVID-19 Pandemic: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(22):11859. https://doi.org/10.3390/ijerph182211859
Chicago/Turabian StyleCiuffreda, Gianluca, Sara Cabanillas-Barea, Andoni Carrasco-Uribarren, María Isabel Albarova-Corral, María Irache Argüello-Espinosa, and Yolanda Marcén-Román. 2021. "Factors Associated with Depression and Anxiety in Adults ≥60 Years Old during the COVID-19 Pandemic: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 22: 11859. https://doi.org/10.3390/ijerph182211859
APA StyleCiuffreda, G., Cabanillas-Barea, S., Carrasco-Uribarren, A., Albarova-Corral, M. I., Argüello-Espinosa, M. I., & Marcén-Román, Y. (2021). Factors Associated with Depression and Anxiety in Adults ≥60 Years Old during the COVID-19 Pandemic: A Systematic Review. International Journal of Environmental Research and Public Health, 18(22), 11859. https://doi.org/10.3390/ijerph182211859